
Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Population
2.3. Evaluation of Choroidal Thickness by WF-OCT
2.4. Classification of the Choroidal Map Patterns
2.5. Verification of Reproducibility of Choroidal Map Image Classification
2.6. Statistical Analysis
3. Results
3.1. Background Characteristics of Healthy Eyes
3.2. Relationship of CCT to SE, Ocular Axis Length, and Age
3.3. Classification of the Context Map Patterns
3.4. Relationship between the Choroidal Map Patterns and Biomarkers
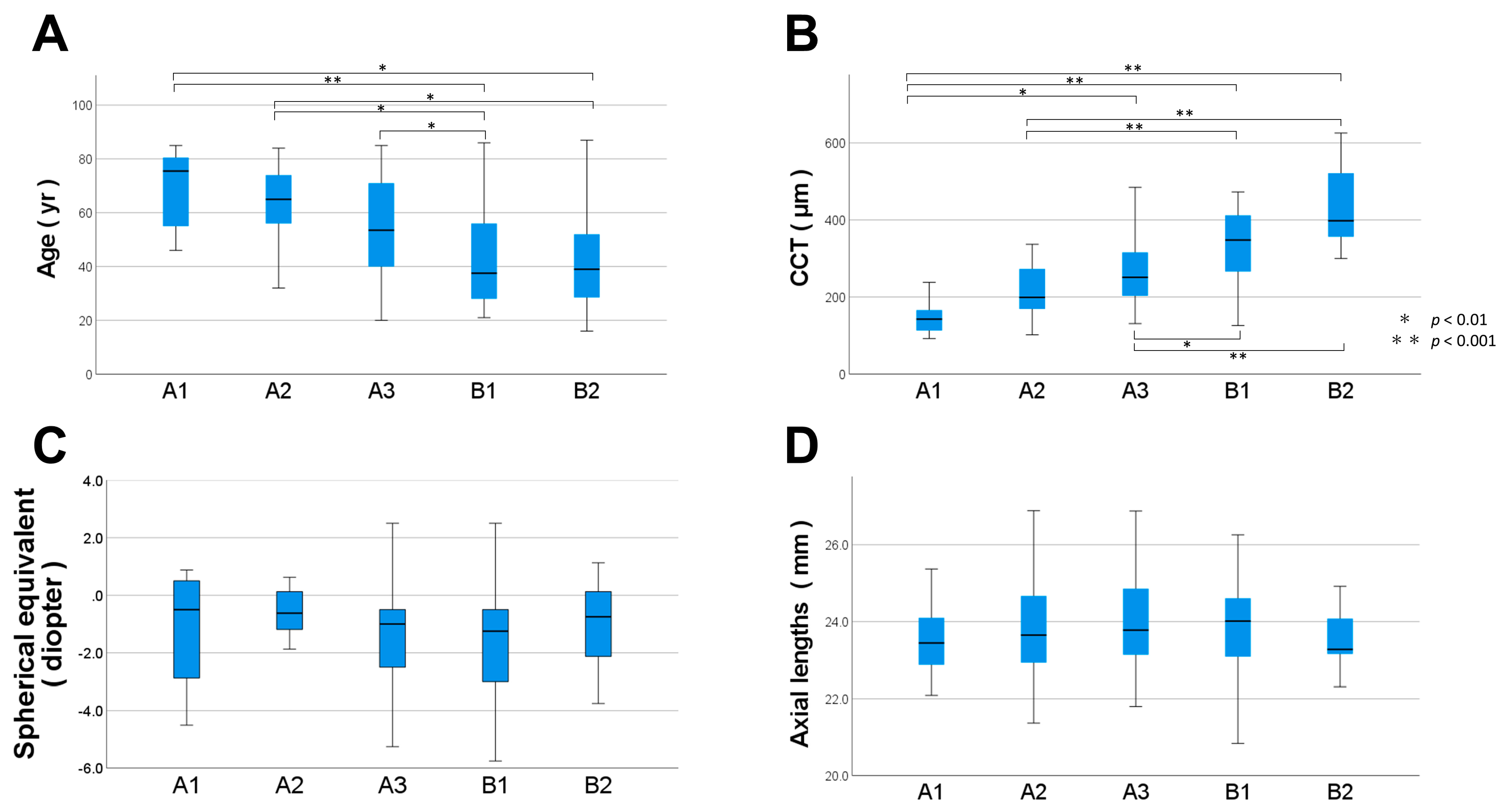
3.5. Differences in the Choroidal Thickness Map Patterns by Sex and Age Group
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kur, J.; Newman, E.A.; Chan-Ling, T. Cellular and physiological mechanisms underlying blood flow regulation in the retina and choroid in health and disease. Prog. Retin. Eye Res. 2012, 31, 377–406. [Google Scholar] [CrossRef] [PubMed]
- Cheung, C.M.G.; Lee, W.K.; Koizumi, H.; Dansingani, K.; Lai, T.Y.Y.; Freund, K.B. Pachychoroid disease. Eye 2019, 33, 14–33. [Google Scholar] [CrossRef]
- Savastano, M.C.; Dansingani, K.K.; Rispoli, M.; Virgili, G.; Savastano, A.; Freund, K.B.; Lumbroso, B. Classification of haller vessel arrangements in acute and chronic central serous chorioretinopathy imaged with en face optical coherence tomography. Retina 2018, 38, 1211–1215. [Google Scholar] [CrossRef]
- Spaide, R.F.; Ledesma-Gil, G.; Cheung, C.M.G. Intervortex venous anastomosis in pachychoroid-related disorders. Retina 2021, 41, 997–1004. [Google Scholar] [CrossRef] [PubMed]
- Kishi, S.; Matsumoto, H. A new insight into pachychoroid diseases: Remodeling of choroidal vasculature. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 260, 3405–3417. [Google Scholar] [CrossRef]
- Spaide, R.F.; Ngo, W.K.; Barbazetto, I.; Sorenson, J.A. Sausaging and Bulbosities of the Choroidal Veins in Central Serous Chorioretinopathy. Retina 2022, 42, 1638–1644. [Google Scholar] [CrossRef]
- Matsumoto, H.; Hoshino, J.; Mukai, R.; Nakamura, K.; Kikuchi, Y.; Kishi, S.; Akiyama, H. Vortex Vein Anastomosis at the Watershed in Pachychoroid Spectrum Diseases. Ophthalmol. Retin. 2020, 4, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Pang, C.E.; Shah, V.P.; Sarraf, D.; Freund, K.B. Ultra-widefield imaging with autofluorescence and indocyanine green angiography in central serous chorioretinopathy. Am. J. Ophthalmol. 2014, 158, 362–371.e2. [Google Scholar] [CrossRef]
- Gao, J.; Rao, C.-H.; Li, F.; Liu, L.; Liu, K.-J. Ultra-Widefield Swept-Source Optical Coherence Tomography Angiography in the Assessment of Choroidal Changes in Young Adults with Myopia. Transl. Vis. Sci. Technol. 2022, 11, 14. [Google Scholar] [CrossRef]
- Funatsu, R.; Sonoda, S.; Terasaki, H.; Shiihara, H.; Mihara, N.; Horie, J.; Sakamoto, T. Choroidal morphologic features in central serous chorioretinopathy using ultra-widefield optical coherence tomography. Graefe’s Arch. Clin. Exp. Ophthalmol. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.H.; Yuan, M.Z.; Zhao, X.Y.; Yu, W.H.; Chen, Y.X. Wide-field swept source optical coherence tomography evaluation of posterior segment changes in highly myopic eyes. Eur. J. Ophthalmol. 2022, 32, 2777–2788. [Google Scholar] [CrossRef] [PubMed]
- Hirata, M.; Tsujikawa, A.; Matsumoto, A.; Hangai, M.; Ooto, S.; Yamashiro, K.; Akiba, M.; Yoshimura, N. Macular choroidal thickness and volume in normal subjects measured by swept-source optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4971–4978. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Miyake, M.; Hosoda, Y.; Uji, A.; Nakano, E.; Takahashi, A.; Muraoka, Y.; Miyata, M.; Tamura, H.; Ooto, S.; et al. Distribution of Choroidal Thickness and Choroidal Vessel Dilation in Healthy Japanese Individuals. Ophthalmol. Sci. 2021, 1, 100033. [Google Scholar] [CrossRef]
- Hayreh, S.S. In vivo choroidal circulation and its watershed zones. Eye 1990, 4 Pt 2, 273–289. [Google Scholar] [CrossRef]
- Kakiuchi, N.; Terasaki, H.; Sonoda, S.; Shiihara, H.; Yamashita, T.; Tomita, M.; Shinohara, Y.; Sakoguchi, T.; Iwata, K.; Sakamoto, T. Regional Differences of Choroidal Structure Determined by Wide-Field Optical Coherence Tomography. Investig. Ophthalmol. Vis. Sci. 2019, 60, 2614. [Google Scholar] [CrossRef]
- Ho, J.; Branchini, L.; Regatieri, C.; Krishnan, C.; Fujimoto, J.G.; Duker, J.S. Analysis of normal peripapillary choroidal thickness via spectral domain optical coherence tomography. Ophthalmology 2011, 118, 2001–2007. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Jirarattanasopa, P.; Ooto, S.; Tsujikawa, A.; Yamashiro, K.; Hangai, M.; Hirata, M.; Matsumoto, A.; Yoshimura, N. Assessment of macular choroidal thickness by optical coherence tomography and angiographic changes in central serous chorioretinopathy. Ophthalmology 2012, 119, 1666–1678. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Q.; Larsen, M.; Munch, I.C. Subfoveal choroidal thickness in relation to sex and axial length in 93 Danish university students. Investig. Ophthalmol. Vis. Sci. 2011, 52, 8438–8441. [Google Scholar] [CrossRef]
- Funatsu, R.; Terasaki, H.; Shiihara, H.; Kawano, S.; Hirokawa, M.; Tanabe, Y.; Fujiwara, T.; Mitamura, Y.; Sakamoto, T.; Sonoda, S. Quantitative evaluations of vortex vein ampullae by adjusted 3D reverse projection model of ultra-widefield fundus images. Sci. Rep. 2021, 11, 8916. [Google Scholar] [CrossRef]
- Ding, X.; Li, J.; Zeng, J.; Kawano, S.; Hirokawa, M.; Tanabe, Y.; Fujiwara, T.; Mitamura, Y.; Sakamoto, T.; Sonoda, S. Choroidal Thickness in Healthy Chinese Subjects. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9555. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Medrano, J.; Flores-Moreno, I.; Pena-Garcia, P.; Montero, J.A.; Duker, J.S.; Ruiz-Moreno, J.M. Macular choroidal thickness profile in a healthy population measured by swept-source optical coherence tomography. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3532–3542. [Google Scholar] [CrossRef]
- Burger, H.G. The endocrinology of the menopause. J. Steroid. Biochem. Mol. Biol. 1999, 69, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Barton, M. Cholesterol and atherosclerosis: Modulation by oestrogen. Curr. Opin. Lipidol. 2013, 24, 214–220. [Google Scholar] [CrossRef]
- Brislane, Á.; Low, D.A.; Carter, S.E.; Holder, S.M.; Jones, H.; Hopkins, N.D. Cerebral and peripheral vascular differences between pre- and postmenopausal women. Menopause 2020, 27, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Kavroulaki, D.; Gugleta, K.; Kochkorov, A.; Katamay, R.; Flammer, J.; Orgul, S. Influence of gender and menopausal status on peripheral and choroidal circulation. Acta Ophthalmol. 2010, 88, 850–853. [Google Scholar] [CrossRef] [PubMed]
- Çiloğlu, E.; Unal, F.; Dogan, N.C. The relationship between the central serous chorioretinopathy, choroidal thickness, and serum hormone levels. Graefe’s Arch. Clin. Exp. Ophthalmol. 2018, 256, 1111–1116. [Google Scholar] [CrossRef]
- Schmetterer, L.; Polak, K. Role of nitric oxide in the control of ocular blood flow. Prog. Retin. Eye Res. 2001, 20, 823–847. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | Male | Female | p Value (M vs. F) |
|---|---|---|---|---|
| (N = 63) | (N = 83) | |||
| Sex | Male 63 (43.2%) | |||
| Age years, mean (SD) | 52.3 ± 19.8 | 51.14 ± 19.18 | 53.10 ± 20.34 | 0.588 |
| Axial lengths mm, mean (SD) | 23.80 ± 1.18 | 24.18 ± 1.12 | 23.52 ± 1.15 | 0.02 |
| Spherical equivalent diopter mean (SD) | −1.13 ± 1.81 | −1.13 ± 1.81 | −1.32 ± 1.91 | 0.891 |
| CCT mm, mean (SD) | 287.9 ± 113.8 | 296.05 ± 112.15 | 281.73 ± 115.28 | 0.337 |
| Factor | Multiple Regression Analysis (Corrected R2 = 0.213) | |
|---|---|---|
| β Standardized Regression Coefficient | p | |
| Age (year) | −0.52 | <0.01 |
| Axial lengths (mm) | −0.29 | <0.01 |
| Spherical equivalent (diopter) | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mihara, N.; Sonoda, S.; Terasaki, H.; Shiihara, H.; Sakono, T.; Funatsu, R.; Sakamoto, T. Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes. J. Clin. Med. 2023, 12, 1505. https://doi.org/10.3390/jcm12041505
Mihara N, Sonoda S, Terasaki H, Shiihara H, Sakono T, Funatsu R, Sakamoto T. Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes. Journal of Clinical Medicine. 2023; 12(4):1505. https://doi.org/10.3390/jcm12041505
Chicago/Turabian StyleMihara, Naohisa, Shozo Sonoda, Hiroto Terasaki, Hideki Shiihara, Takato Sakono, Ryoh Funatsu, and Taiji Sakamoto. 2023. "Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes" Journal of Clinical Medicine 12, no. 4: 1505. https://doi.org/10.3390/jcm12041505
APA StyleMihara, N., Sonoda, S., Terasaki, H., Shiihara, H., Sakono, T., Funatsu, R., & Sakamoto, T. (2023). Sex- and Age-Dependent Wide-Field Choroidal Thickness Differences in Healthy Eyes. Journal of Clinical Medicine, 12(4), 1505. https://doi.org/10.3390/jcm12041505