

Application of an Intraoperative Limb Positioner for Adjustable Traction in Both-Column Fractures of the Acetabulum: A Technical Note with Clinical Outcome

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
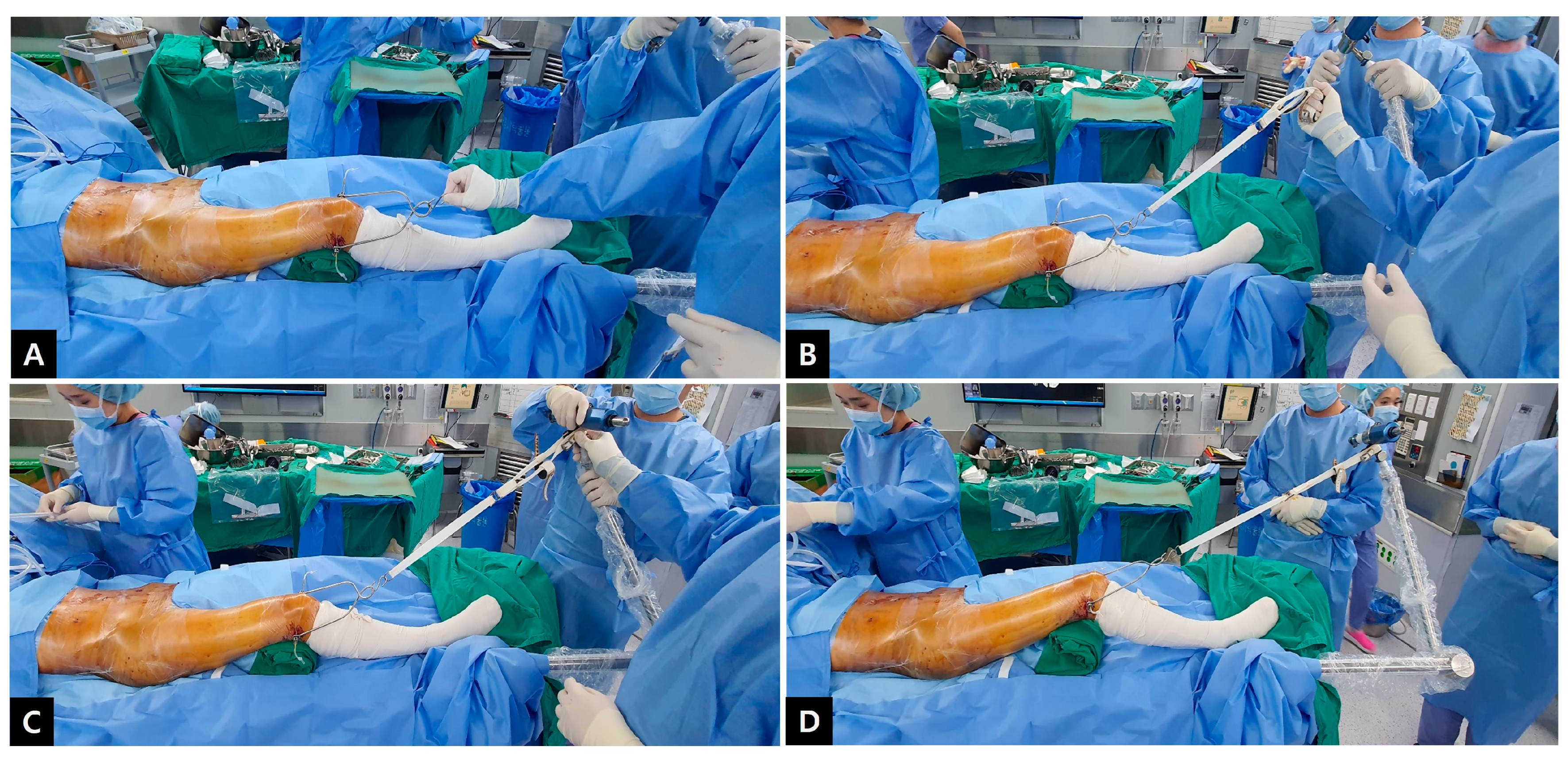
2.1. Operative Technique
- Preparation
- 2.
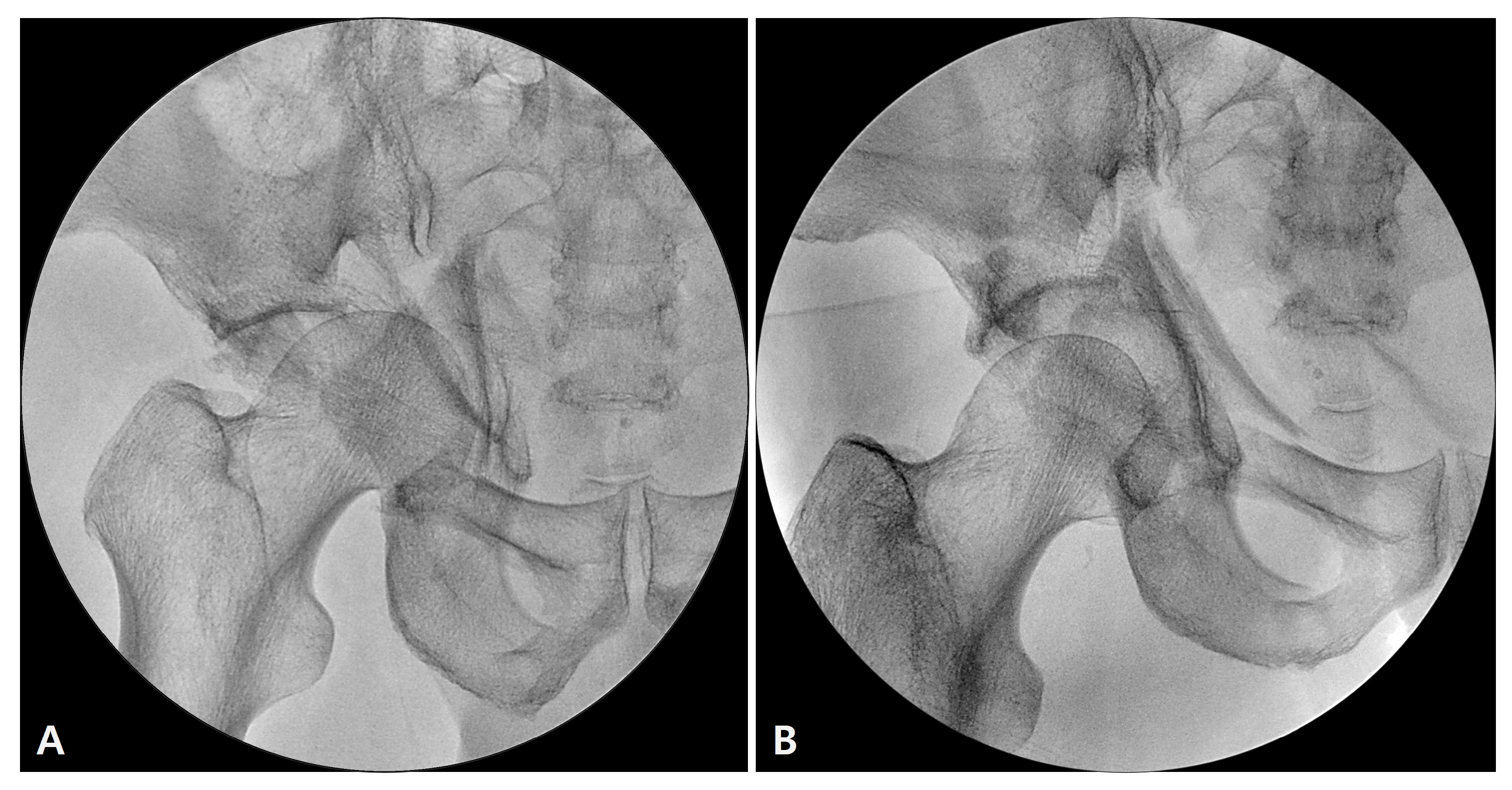
- Traction with a limb positioner
- 3.
- Reduction and fixation
2.2. Postoperative Management and Assessment
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelly, J.; Ladurner, A.; Rickman, M. Surgical management of acetabular fractures—A contemporary literature review. Injury 2020, 51, 2267–2271. [Google Scholar] [CrossRef] [PubMed]
- Gänsslen, A.; Frink, M.; Hildebrand, F.; Krettek, C. Both column fractures of the acetabulum: Epidemiology, operative management and long-term-results. Acta Chir. Orthop. Traumatol. Cech. 2012, 79, 107–113. [Google Scholar] [PubMed]
- Tannast, M.; Najibi, S.; Matta, J.M. Two to twenty-year survivorship of the hip in 810 patients with operatively treated acetabular fractures. J. Bone Jt. Surg. Am. 2012, 94, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Calafi, L.A.; Routt, M.L. Direct hip joint distraction during acetabular fracture surgery using the AO universal manipulator. J. Trauma Inj. Infect. Crit. Care 2010, 68, 481–484. [Google Scholar] [CrossRef] [PubMed]
- Lefaivre, K.A.; Starr, A.J.; Barker, B.P.; Overturf, S.; Reinert, C.M. Early experience with reduction of displaced disruption of the pelvic ring using a pelvic reduction frame. J. Bone Jt. Surg. Br. 2009, 91, 1201–1207. [Google Scholar] [CrossRef]
- Romanelli, F.; Boe, E.; Sun, L.; Keller, D.M.; Yoon, R.S.; Liporace, F.A. Temporary external fixation to table as a traction reduction aide in the treatment of unstable pelvic ring injuries: A technical note. Hip Pelvis 2020, 32, 214–222. [Google Scholar] [CrossRef]
- Goodnough, L.H.; Olsen, T.; Hidden, K.; DeBaun, M.R.; Kleweno, C.P. Use of an intraoperative limb positioner for adjustable distraction in acetabulum fractures with femoral head protrusion: A case report. JBJS Case Connect. 2021, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Henderson, E.R.; Prioreschi, B.; Mata-Fink, A.; Bell, J.E. Use of the spider limb positioner in oncologic lower extremity surgery. Expert Rev. Med. Devices 2014, 11, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Matta, J. Fractures of the acetabulum: Accuracy of reduction and clinical results of fractures operated within three weeks after the injury. J. Bone Jt. Surg. Am. 1996, 78, 1632–1645. [Google Scholar] [CrossRef]
- Rommens, P.M. Ilioinguinal approach for acetabular fractures. Orthop. Traumatol. 2002, 10, 179–189. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Grotz, M.R.; Papakostidis, C.; Dinopoulos, H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J. Bone Jt. Surg. Br. 2005, 87, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Tile, M.; Helfet, D.; Kellam, J. Fractures of the Pelvis and the Acetabulum, 3rd ed.; Lippincott Williams & Wilkins: New York, NY, USA, 2003. [Google Scholar]
- Harris, A.M.; Althausen, P.; Kellam, J.F.; Bosse, M.J. Simultaneous anterior and posterior approaches for complex acetabular fractures. J. Orthop. Trauma 2008, 22, 494–497. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Chiu, E.; Lo, W.; Chung, T. Cerclage wiring in displaced both column fractures of the acetabulum. Injury 2001, 32, 391–394. [Google Scholar] [CrossRef] [PubMed]
- Masahiro, S.; Kensei, N.; Kensuke, S.; Kunihiko, T.; Takanobu, A.; Toshiya, E.; Kmanabu, K.; Masabumi, I.; Toyama, U. Operative treatment of both column fractures in the acetabulum. Orthop. Traumatol. 2002, 51, 162–167. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| No. | Age | Sex | Injury Mechanism | Side | CDFH | Operation Time (Minutes) | Reduction Status (by Matta) | Union Time (Months) | Follow-Up Duration (Months) | Merle d’Aubigné Score | Complication |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 35 | M | Driver accident | L | Yes | 150 | Excellent | 16 | 40 | 15 | |
| 2 | 66 | M | Pedestrian accident | R | Yes | 240 | Excellent | 18 | 50 | 18 | |
| 3 | 89 | F | Fall down | L | No | 200 | Good | 17 | 30 | 18 | |
| 4 | 85 | M | Motorcycle accident | R | Yes | 180 | Good | 18 | 12 | 15 | |
| 5 | 60 | F | Pedestrian accident | R | No | 240 | Excellent | 16 | 32 | 15 | |
| 6 | 50 | F | Pedestrian accident | R | No | 190 | Excellent | 20 | 19 | 18 | |
| 7 | 55 | M | Pedestrian accident | R | Yes | 200 | Good | 20 | 60 | 15 | |
| 8 | 47 | M | Pedestrian accident | L | Yes | 250 | Excellent | 18 | 49 | 16 | |
| 9 | 21 | F | Motorcycle accident | R | Yes | 240 | Excellent | 15 | 29 | 15 | |
| 10 | 55 | M | Fall down | L | No | 180 | Good | 20 | 30 | 17 | |
| 11 | 58 | M | Fall down | L | No | 220 | Excellent | 18 | 24 | 16 | |
| 12 | 56 | M | Pedestrian accident | R | Yes | 240 | Good | 18 | 28 | 16 | |
| 13 | 71 | F | Pedestrian accident | R | No | 200 | Good | 16 | 23 | 15 | ONFH |
| 14 | 50 | M | Fall down | R | Yes | 155 | Excellent | 16 | 23 | 18 | |
| 15 | 25 | F | Fall down | R | Yes | 180 | Excellent | 18 | 30 | 18 | |
| 16 | 60 | F | Driver accident | L | No | 170 | Good | 18 | 26 | 18 | |
| 17 | 31 | M | Fall down | R | Yes | 240 | Excellent | 16 | 34 | 18 | |
| 18 | 64 | F | Pedestrian accident | R | Yes | 290 | Poor | 18 | 17 | 15 | |
| 19 | 44 | F | Pedestrian accident | R | No | 200 | Good | 13 | 24 | 18 | Traumatic OA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-W.; Oh, C.-W.; Park, K.-H.; Hong, W.-K.; Yoon, S.-H.; Lee, G.-S.; Oh, J.-K. Application of an Intraoperative Limb Positioner for Adjustable Traction in Both-Column Fractures of the Acetabulum: A Technical Note with Clinical Outcome. J. Clin. Med. 2023, 12, 1682. https://doi.org/10.3390/jcm12041682
Kim J-W, Oh C-W, Park K-H, Hong W-K, Yoon S-H, Lee G-S, Oh J-K. Application of an Intraoperative Limb Positioner for Adjustable Traction in Both-Column Fractures of the Acetabulum: A Technical Note with Clinical Outcome. Journal of Clinical Medicine. 2023; 12(4):1682. https://doi.org/10.3390/jcm12041682
Chicago/Turabian StyleKim, Joon-Woo, Chang-Wug Oh, Kyeong-Hyeon Park, Won-Ki Hong, Sung-Hyuk Yoon, Gwang-Sub Lee, and Jong-Keon Oh. 2023. "Application of an Intraoperative Limb Positioner for Adjustable Traction in Both-Column Fractures of the Acetabulum: A Technical Note with Clinical Outcome" Journal of Clinical Medicine 12, no. 4: 1682. https://doi.org/10.3390/jcm12041682
APA StyleKim, J. -W., Oh, C. -W., Park, K. -H., Hong, W. -K., Yoon, S. -H., Lee, G. -S., & Oh, J. -K. (2023). Application of an Intraoperative Limb Positioner for Adjustable Traction in Both-Column Fractures of the Acetabulum: A Technical Note with Clinical Outcome. Journal of Clinical Medicine, 12(4), 1682. https://doi.org/10.3390/jcm12041682