
Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
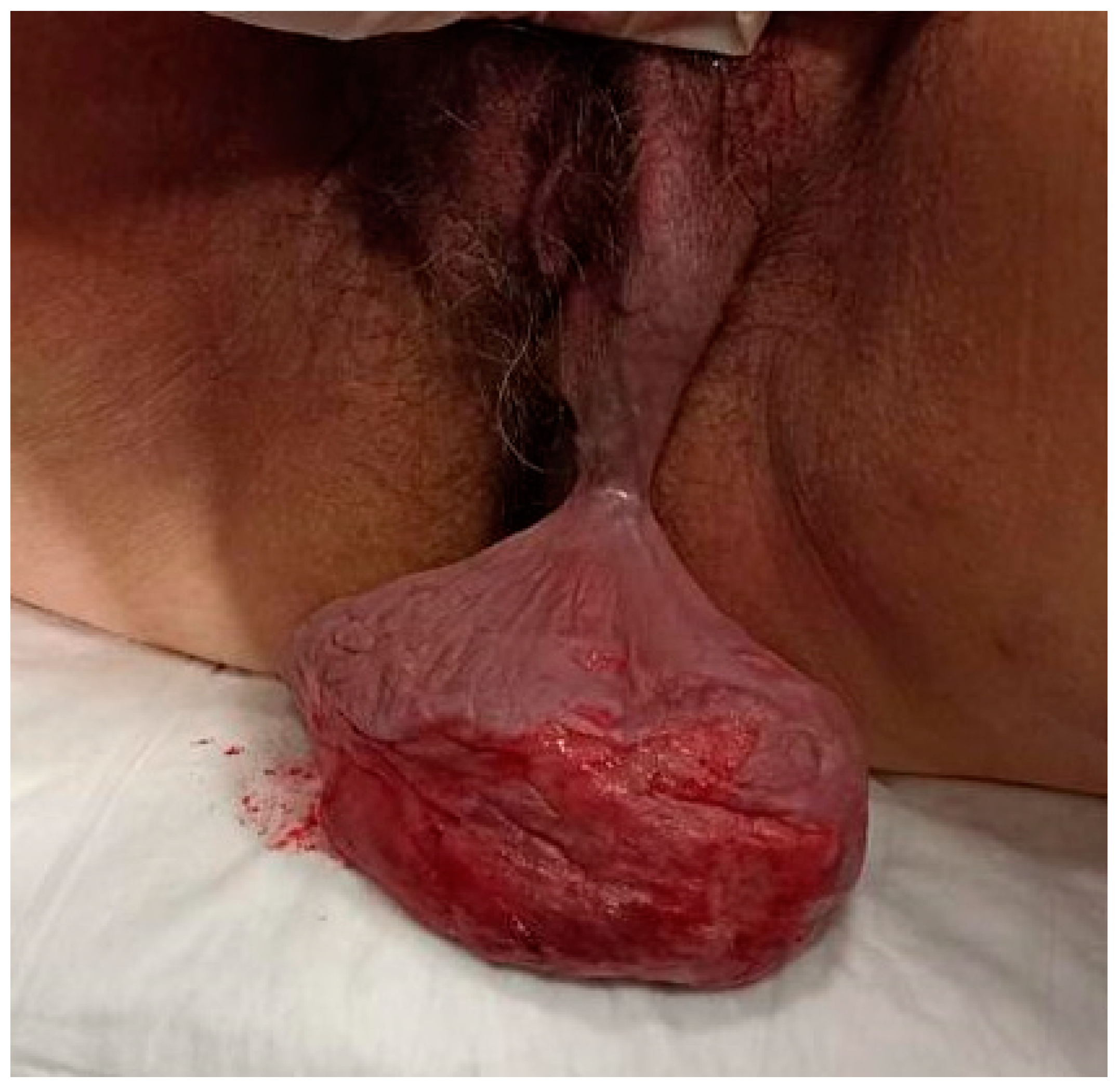
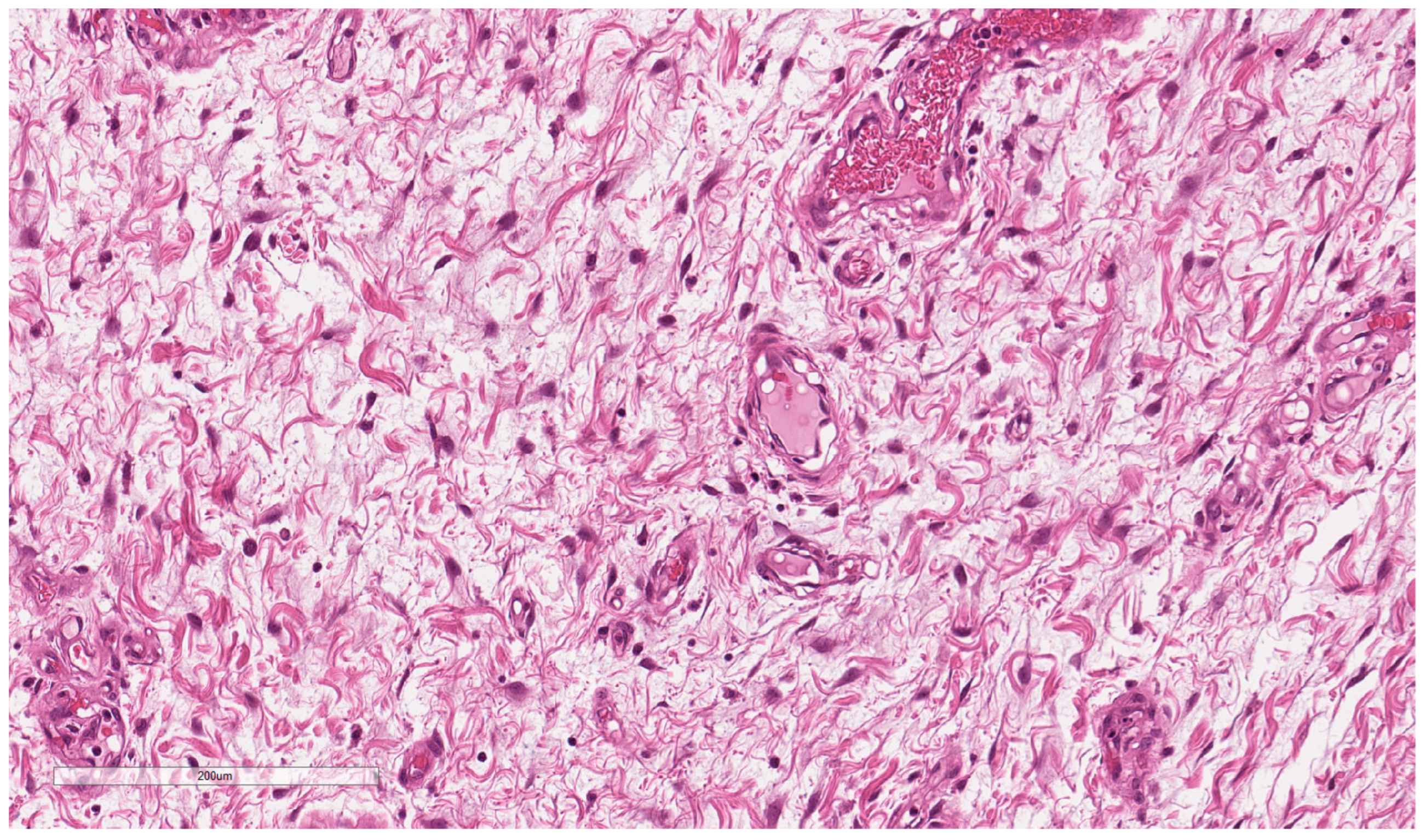
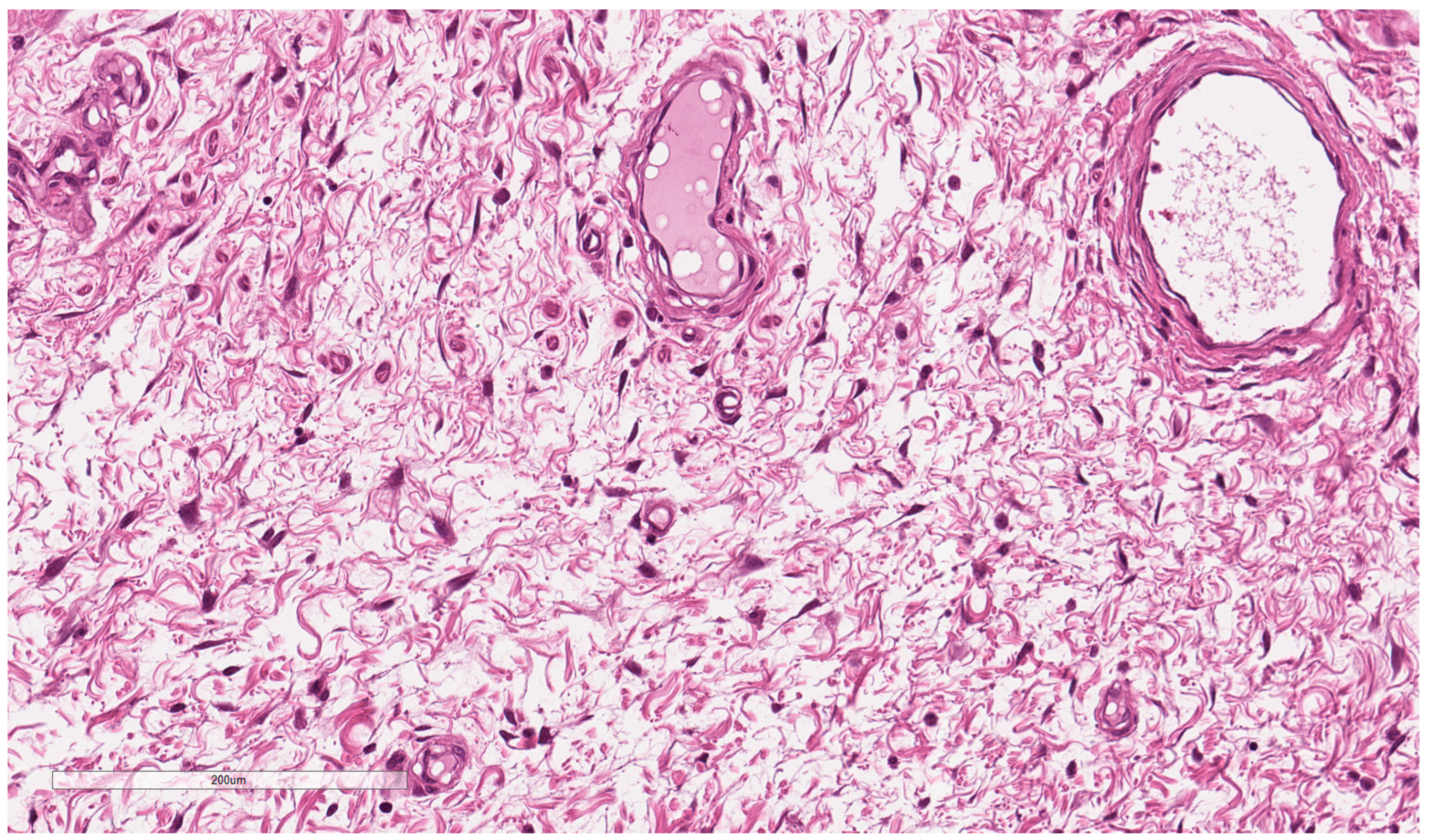
2.1. Case Report
2.2. Review of Literature
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Srivastava, V.; Jha, P.K.; Kumar Verma, A.; Ahmad Ansari, M. Vulvar aggressive angiomyxoma: A surgical challenge. BMJ Case Rep. 2021, 14, e240687. [Google Scholar] [CrossRef] [PubMed]
- Smirniotis, V.; Kondi-Pafiti, A.I.; Theodoraki, K.; Kostopanagiotou, G.; Liapis, A.; Kourias, E. Aggressive angiomyxoma of the pelvis: A clinopathologic study of a case. Clin. Exp. Obstet. Gynecol. 1997, 24, 209–211. [Google Scholar] [PubMed]
- Mehrotra, K.; Bhandari, M.; Khullar, G.; Sharma, S. Large Superficial Angiomyxoma of the Vulva-report of Two Cases with Varied Clinical Presentation. Indian Dermatol. Online J. 2021, 12, 605–607. [Google Scholar] [PubMed]
- Steeper, T.A.; Rosai, J. Aggressive angiomyxoma of the female pelvis and perineum. Report of nine cases of a distinctive type of gynecologic soft-tissue neoplasm. Am. J. Surg. Path. 1983, 7, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.C.; Kuzey, G.M.; Dogan, N.U.; Yuce, K. Aggressive angiomyxoma of vulva recurring 8 years after initial diagnosis. Arch. Gynecol. Obstet. 2009, 280, 485–487. [Google Scholar] [CrossRef]
- Aguilar-Frasco, J.; Ruben-Castillo, C.; Rodríguez-Quintero, J.H.; Medina-Franco, H. Aggressive angiomyxoma: Giant recurrence successfully treated with wide excision and adjuvant therapy with GnRH analogue. BMJ Case Rep. 2018, 11, e226973. [Google Scholar] [CrossRef] [Green Version]
- Brzezinska, B.N.; Clements, A.E.; Rath, K.S.; Reid, G.C. A persistent mass: A case of aggressive Angiomyxoma of the vulva. Gynecol. Oncol. Rep. 2018, 24, 15–17. [Google Scholar] [CrossRef]
- Zamani, M.; Mollabashi, M.; Mehrabi, N.; Alizadeh, S. Aggressive angiomyxoma of vulva in 28-years old patient: A case report of second recurrence. Ann. Med. Surg. 2021, 69, 102706. [Google Scholar] [CrossRef]
- Xie, Y.; Qian, Y.; Zou, B. A giant aggressive angiomyxoma of vulva in a young woman: A case report. Medicine 2019, 98, e13860. [Google Scholar] [CrossRef]
- Muskan, V.; Adhikari, P.; Thapa, B.D.; Shrestha, R. Vulval Aggressive Angiomyxoma in a 19 year teenager: A case report. BMC Women’s Health 2022, 22, 382. [Google Scholar] [CrossRef]
- Goyal, L.D.; Garg, P.; Badyal, R.; Bhalla, S. Aggressive (deep) angiomyxoma of the vulva: A case report. J. Med. Case Rep. 2022, 16, 71. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.Y.; Su, N.; Jiang, Y.X.; Yang, M. Application of ultrasound in aggressive angiomyxoma: Eight case reports and review of literature. World J. Clin. Cases 2018, 6, 811–819. [Google Scholar] [CrossRef] [PubMed]
- Fatušić, J.; Hudić, I.; Fatušić, Z.; Čičkušić, E.; Šarkanović, G. Giant aggressive angiomyxoma of the vulva: Case Report. Acta Clin. Croat 2015, 54, 220–222. [Google Scholar]
- Ribeiro, J.C.; Vieira, S.C.; Silva, B.B.; Santos, L.G.; Costa, P.V.; Fonsêca, L.A. Aggressive angiomyxoma of the vulva: Case report. Einstein 2015, 13, 276–278. [Google Scholar] [CrossRef] [Green Version]
- Tariq, R.; Hasnain, S.; Siddiqui, M.T.; Ahmed, R. Aggressive angiomyxoma: Swirled configuration on ultrasound and MR imaging. J. Pak. Med. Assoc. 2014, 64, 345–348. [Google Scholar] [PubMed]
- Narayama, C.; Ikeda, M.; Yasaka, M.; Sagara, Y.; Kan-No, Y.; Hayashi, I.; Narita, A.; Asai, S.; Tajima, T.; Shida, M.; et al. Aggressive Angiomyxoma of the Vulva with No Recurrence on a 5-year Follow up: A Case Report. Tokai. J. Exp. Clin. Med. 2016, 41, 42–45. [Google Scholar] [PubMed]
- Amin, A.; El Badawy, S.; Bull, A. Aggressive angiomyxoma of the vulva. J. Obstet. Gynaecol. 2013, 33, 325–326. [Google Scholar] [CrossRef] [PubMed]
- Elkattah, R.; Sarkodie, O.; Otteno, H.; Fletcher, A. Aggressive angiomyxoma of the vulva: A précis for primary care providers. Case Rep. Obstet. Gynecol. 2013, 2013, 183725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zizi-Sermpetzoglou, A.; Myoteri, D.; Koulia, K.; Kontostolis, V.; Moschouris, H.; Dellaportas, D. Aggressive angiomyxoma of the vulva: A bizarre perineal lesion. Case Rep. Oncol. Med. 2015, 2015, 292304. [Google Scholar] [CrossRef]
- Sengupta, S.K.; Bhattacharyya, S.K.; Saha, S.P.; Roy, H.; Sarkar, A.N. Recurrent aggressive angiomyxoma of the vulva—A rare presentation. J. Clin. Diagn. Res. 2014, 8, OD01-2. [Google Scholar]
- Narang, S.; Kohli, S.; Kumar, V.; Chandoke, R. Aggressive angiomyxoma with perineal herniation. J. Clin. Imaging Sci. 2014, 4, 23. [Google Scholar] [CrossRef] [PubMed]
- Das, B.P.; Baruah, D.; Medhi, K.B.; Talukder, B. An aggressive angiomyxoma of vulva—A rare entity—A case report. J. Midlife Health 2016, 7, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, P.E.; Hui, P.; McCarthy, S. Hormonal therapy for aggressive angiomyxoma: A case report and proposed management algorithm. J. Low. Genit. Tract Dis. 2014, 18, E55–E61. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.C.; Sheu, C.Y.; Chen, T.Y.; Yang, Y.C. Aggressive angiomyxoma: A small palpable vulvar lesion with a huge mass in the pelvis. J. Low. Genit. Tract Dis. 2013, 17, 75–78. [Google Scholar] [CrossRef]
- Kiran, G.; Yancar, S.; Sayar, H.; Kiran, H.; Coskun, A.; Arikan, D.C. Late recurrence of aggressive angiomyxoma of the vulva. J. Low. Genit. Tract Dis 2013, 17, 85–87. [Google Scholar] [CrossRef]
- Lee, K.A.; Seo, J.W.; Yoon, N.R.; Lee, J.W.; Kim, B.G.; Bae, D.S. Aggressive angiomyxoma of the vulva: A case report. Obstet. Gynecol. Sci. 2014, 57, 164–167. [Google Scholar] [CrossRef]
- Choi, H.; Park, C.; Ji, Y.I. Alternative surgical approaches for aggressive angiomyxoma at different sites in the pelvic cavity. Obstet. Gynecol. Sci. 2015, 58, 525–529. [Google Scholar] [CrossRef]
- Lourenço, C.; Oliveira, N.; Ramos, F.; Ferreira, I.; Oliveira, M. Aggressive angiomyxoma of the vagina: A case report. Rev. Bras. Ginecol. Obstet. 2013, 35, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Foust-Wright, C.; Allen, A.; Shobeiri, S.A. Periurethral aggressive angiomyxoma: A case report. Int. Urogynecol. J. 2013, 24, 877–880. [Google Scholar] [CrossRef]
- Ota, H.; Otsuki, K.; Ichihara, M.; Ishikawa, T.; Okai, T. A case of aggressive angiomyxoma of the vulva. J. Med. Ultrason. 2013, 40, 283–287. [Google Scholar] [CrossRef]
- Dahiya, K.; Jain, S.; Duhan, N.; Nanda, S.; Kundu, P. Aggressive angiomyxoma of vulva and vagina: A series of three cases and review of literature. Arch. Gynecol. Obstet. 2011, 283, 1145–1148. [Google Scholar] [CrossRef]
- Nucci, M.R.; Fletchr, C.D. Vulvovaginal soft tissue tumors: Update and review. Histopathology 2000, 36, 97–108. [Google Scholar] [CrossRef]
- Kondo, T. Aggressive angiomyxoma in the inguinal region: A case report. J. Med. Case Rep. 2010, 4, 396. [Google Scholar] [CrossRef] [Green Version]
- Htwe, M.; Deppisch, L.M.; Saint-Julien, J.S. Hormone-dependent, aggressive angiomyxoma of the vulva. Obstet. Gynecol. 1995, 86, 697–699. [Google Scholar] [CrossRef]
- Bhakti Dattatraya Deshmukh, M.P.K.; Momin Yasmin, A.; Sulhyan Kalpana, R. Aggressive angiomyxoma of vulva: A Case report and review of literature. Arch. Med. Health Sci. 2015, 3, 88–90. [Google Scholar] [CrossRef]
- Xu, H.; Sun, P.; Xu, R.; Wang, L.; Shi, Y. Aggressive angiomyxoma in pregnancy: A case report and literature review. J. Int. Med. Res. 2020, 48, 300060520936414. [Google Scholar] [CrossRef]
- Sun, N.X.; Li, W. Aggressive angiomyxoma of the vulva: Case report and literature review. J. Int. Med. Res. 2010, 38, 1547–1552. [Google Scholar] [CrossRef]
- Faraj, W.; Houjeij, M.; Haydar, A.; Nassar, H.; Nounou, G.; Khalife, M. Aggressive angiomyxoma presenting with back and perineal bulge; a complex surgical approach: A case report. Int. J. Surg. Case Rep. 2016, 24, 211–214. [Google Scholar] [CrossRef] [Green Version]
- Wiser, A.; Korach, J.; Gotlieb, W.H.; Fridman, E.; Apter, S.; Ben-Baruch, G. Importance of accurate preoperative diagnosis in the management of aggressive angiomyxoma: Report of three cases and review of the literature. Abdom. Imaging 2006, 31, 383–386. [Google Scholar] [CrossRef]
- Blandamura, S.; Cruz, J.; Faure Vergara, L. Aggressive angiomyxoma: A second case of metastasis with patient’s death. Hum. Pathol. 2003, 34, 1072–1074. [Google Scholar] [CrossRef]
- Ayati, E.; Pesikhani, M.D.; Karamali, M.; Borhan, A.; Pourali, L. A deep giant aggressive angiomyxoma of the labia majora: A case report. Int. J. Surg. Case Rep. 2022, 96, 107313. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year | Clinical Aspects | History | Symptoms | Site | Treatment | Follow-up |
|---|---|---|---|---|---|---|
| Aguilar-Frasco et al., 2018 [6] | 39 yrs; bulky, soft, and mobile bilobulated tumour with dimensions of 28.1 × 10.4 cm | R After 1 year | Tumour | Right labium majus | Surgical excision | GnRH-analogue therapy > 3 months |
| Brzezinska et al., 2018 [7] | 47 yrs; bulky, soft, and mobile tumour with dimensions of 4.3 × 3.6 cm | P | Tumour | Right labium majus | Surgical excision | Observation |
| Zamani et al., 2021 [8] | 28 yrs; bulky, soft pedunculated tumour with dimensions of 20 × 15 × 10 cm. | R After 2 years | Tumour | Vulva and pubis | Surgical excision | GnRH-analogue therapy for 3 months |
| Xie et al., 2019 [9] | 22 yrs; bulky, soft, pedunculated, and ulcerated tumour with dimensions of 30 cm × 20 cm | P | Tumour, pruritus | Left vulva | Surgical excision | Observation |
| Muskan et al., 2022 [10] | 19 yrs; bulky, soft tumour with dimensions of 10 cm × 10 cm | P | Tumour | Left vulva | Surgical excision | Observation |
| Goyal et al., 2022 [11] | 40 yrs; bulky, soft pedunculated and ulcerated tumour 8 × 8 cm | P | Tumour, serosanguinous discharge from the ulceration | Left labium majus | Surgical excision | GnRH-analogue therapy for 3 months |
| Zhao et al., 2018 [12] | (1) 40 yrs; bulky, soft tumour (2) 38 yrs; bulky soft tumour with dimensions of 7.2 × 5.6 × 14.6 cm (3) 40 yrs; bulky, soft tumour with dimensions of 17.1 × 10.6 × 8.9 cm (4) 35 yrs; bulky, soft tumour with dimensions of 16.2 × 6.9 × 7.4 cm (5) 38 yrs; bulky, soft tumour (6) 45 yrs; bulky, soft tumour with dimensions of 12.3 × 8.8 × 6.3 cm (7) 34 yrs; bulky, soft tumour measuring 11 cm | (1) P (2) R After 2 years (3) P (4) P (5) R After 3 years (6) P (7) P | (1) Tumour (2) Tumour (3) Tumour (4) Tumour (5) Tumour (6) Tumour (7) Tumour | (1) Left vulva (2) Right vulva (3) Left labium majus (4) Left labium majus (5) Left vulva (6) Left vulva (7) Left vulva | (1) Surgical excision (2) Surgical excision (3) Surgical excision (4) Surgical excision (5) Surgical excision (6) Surgical excision (7) Surgical excision | (1) Observation (2) Observation (3) Observation (4) GnRH-analogue therapy (5) Observation (6) Observation (7) Observation |
| Fatušić et al., 2015 [13] | 57 yrs; bulky, soft ulcerated tumour | P | Tumour | Left vulva | Surgical excision | Observation |
| Ribeiro et al., 2015 [14] | 42 yrs; bulky, soft tumour | P | Tumour, difficulty in urinating | Vulva | Surgical excision | Observation |
| Tariq et al., 2014 [15] | 40 yrs; bulky, soft tumour | P | Tumour, pain | Lower-left pelvic-perineal and medial gluteal region | Surgical excision | Observation |
| Narayama et al., 2016 [16] | 49 yrs; bulky, soft tumour with dimensions of 15 × 9.5 × 9 cm | P | Tumour | Left vulva | Surgical excision | Observation |
| Amin et al., 2013 [17] | 89 yrs; bulky, pedunculated tumour with dimensions of 12 × 7 × 6 cm | P | Tumour | Left labium majus | Surgical excision | Observation |
| R. Elkattah et al., 2013 [18] | 38 yrs; bulky, soft tumour with dimensions of 12 × 6 × 4 cm | P | Tumour, dyspareunia | Left labium majus | Surgical excision | Observation |
| Zizi-Sermpetzoglou et al., 2015 [19] | 47 yrs; bulky, soft tumour with dimensions of 25 × 20 × 6 cm | P | Tumour | Right labium majus | Surgical excision | Reoperation 18 months later for recurrence |
| Sengupta et al., 2014 [20] | 34 yrs; bulky, soft tumour with dimensions of 5 × 4 cm | R After 2 years | Tumour | Left labium majus | Surgical excision | Observation |
| Narang et al., 2014 [21] | 40 yrs; bulky, soft tumour with dimensions of 15 × 12 cm | R After 16 months | Tumour | Perineum | Surgical excision | Observation |
| Das et al., 2016 [22] | 40 yrs; bulky, soft tumour with dimensions of 18 × 10 cm | P | Tumour | Right labium majus | Surgical excision | Observation |
| Schwartz et al., 2014 [23] | 32 yrs; bulky, soft tumour with dimensions of 4 × 2.5 cm | R A lot of recurrence during 16 years | Tumour | Left labium majus | Surgical excision | GnRH-analogue therapy for 5 years |
| Huang et al., 2013 [24] | 44 yrs; bulky, soft tumour with dimensions of 12 × 9 × 5 cm | P | Tumour | Left vulva | Surgical excision | Observation |
| Kiran et al., 2013 [25] | 57 yrs; bulky, soft tumour with dimensions of 25 × 30 cm | R After 20 years | Tumour | Left vulva | Surgical excision | Observation |
| Lee et al., 2014 [26] | 35 yrs; bulky, soft tumour with dimensions of 10 × 7 cm | P | Tumour | Right labium majus | Surgical excision | Observation |
| Choi et al., 2015 [27] | (1) 49 yrs; bulky, soft tumour with dimensions of 19 × 19 cm (2) 31 yrs; mixed echogenic mass of the pelvic cavity with dimensions of 18 × 15 × 8 cm (3) 36 yrs; bulky, soft tumour with dimensions of 15 × 10 × 6 cm | (1) P (2) P (3) P | (1) Tumour (2) Abdominal distension and lower abdominal swelling. (3) Tumour | (1) Left labium majus (2) Pelvis (3) Left buttock | (1) Surgical excision (2) Surgical excision (3) Surgical excision | (1) Observation (2) Observation (3) Observation |
| Lourenço et al., 2013 [28] | 47 yrs; bulky, soft tumour with dimensions of 9 × 7 cm | P | Tumour | Left labium majus | Surgial excision | Observation |
| Foust-Wright et al., 2012 [29] | 19 yrs; soft tumour measuring 3.4 cm | P | Tumour, dysuria | Periurethral mass extending beyond the hymen | Surgical excision | Observation |
| Ota et al., 2013 [30] | 28 yrs; bulky, soft tumour with dimensions of 4.8 × 4 cm | P | Tumour, dysuria | Left labium majus | Surgical excision | Observation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gulino, F.A.; Gulisano, M.; Ettore, C.; Giorlandino, A.; Russo, E.; Ettore, G. Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years. J. Clin. Med. 2023, 12, 1726. https://doi.org/10.3390/jcm12051726
Gulino FA, Gulisano M, Ettore C, Giorlandino A, Russo E, Ettore G. Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years. Journal of Clinical Medicine. 2023; 12(5):1726. https://doi.org/10.3390/jcm12051726
Chicago/Turabian StyleGulino, Ferdinando Antonio, Marianna Gulisano, Carla Ettore, Alexandra Giorlandino, Emanuele Russo, and Giuseppe Ettore. 2023. "Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years" Journal of Clinical Medicine 12, no. 5: 1726. https://doi.org/10.3390/jcm12051726
APA StyleGulino, F. A., Gulisano, M., Ettore, C., Giorlandino, A., Russo, E., & Ettore, G. (2023). Aggressive Angiomyxoma of the Vulva: Which Is the Best Management Strategy? Description of a Case Report and Review of Literature of the Last Ten Years. Journal of Clinical Medicine, 12(5), 1726. https://doi.org/10.3390/jcm12051726