
Emotional Exhaustion, a Proxy for Burnout, Is Associated with Sleep Health in French Healthcare Workers without Anxiety or Depressive Symptoms: A Cross-Sectional Study


 , ,
, ,  , ,
, ,  , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Characteristics of the Study Population
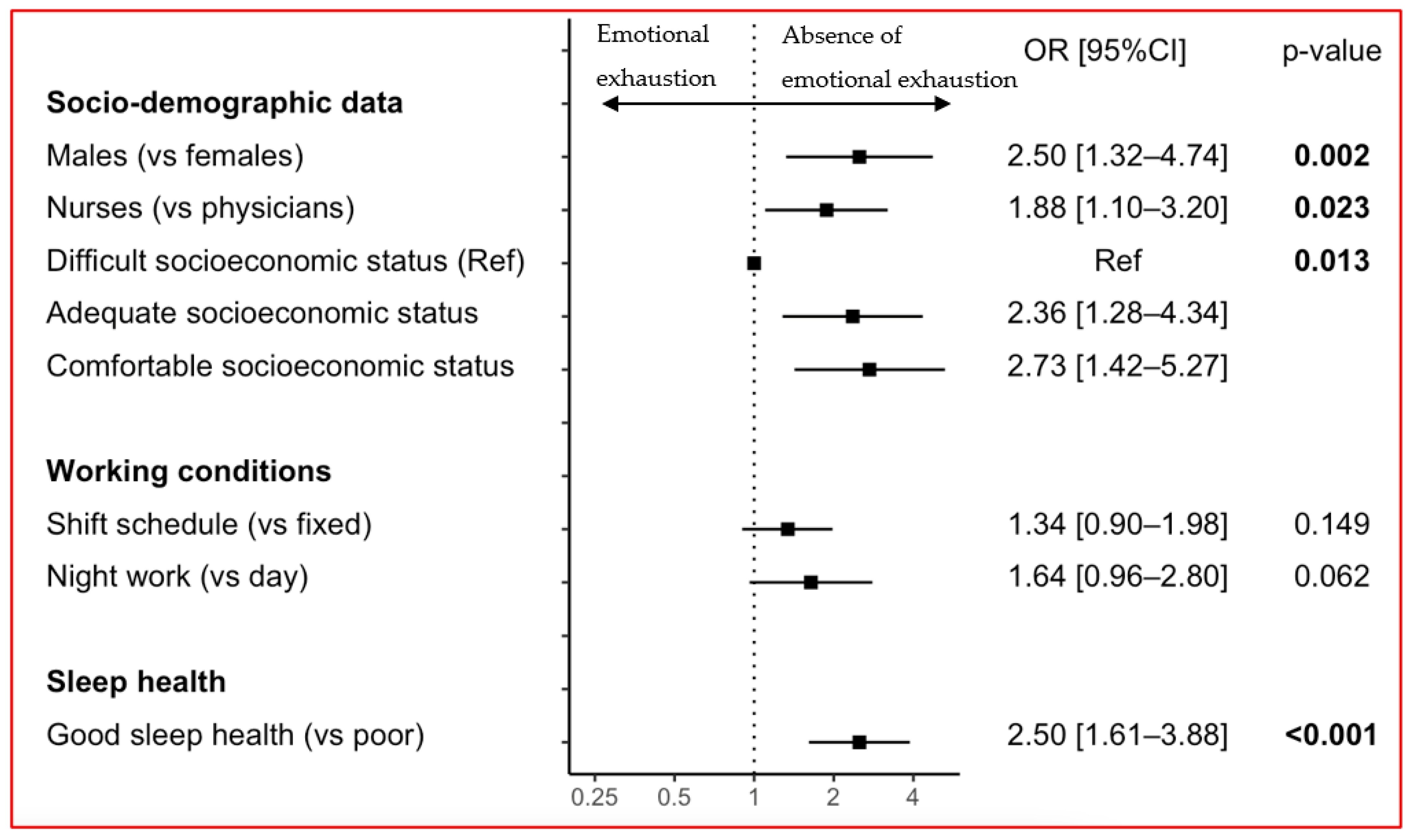
3.2. Association between EE and Sleep Health
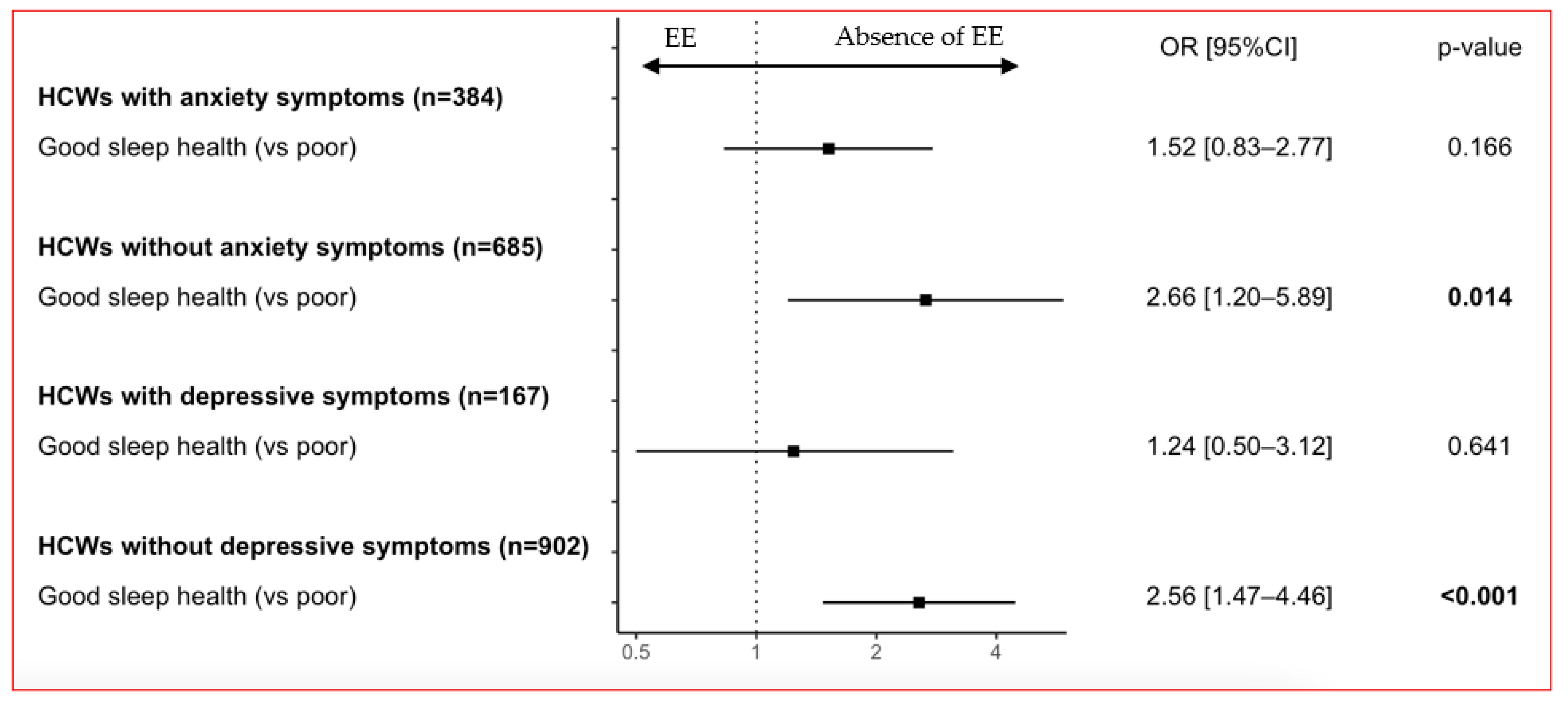
3.3. Association between EE and Sleep Health According to ANXIETY and Depressive Symptoms
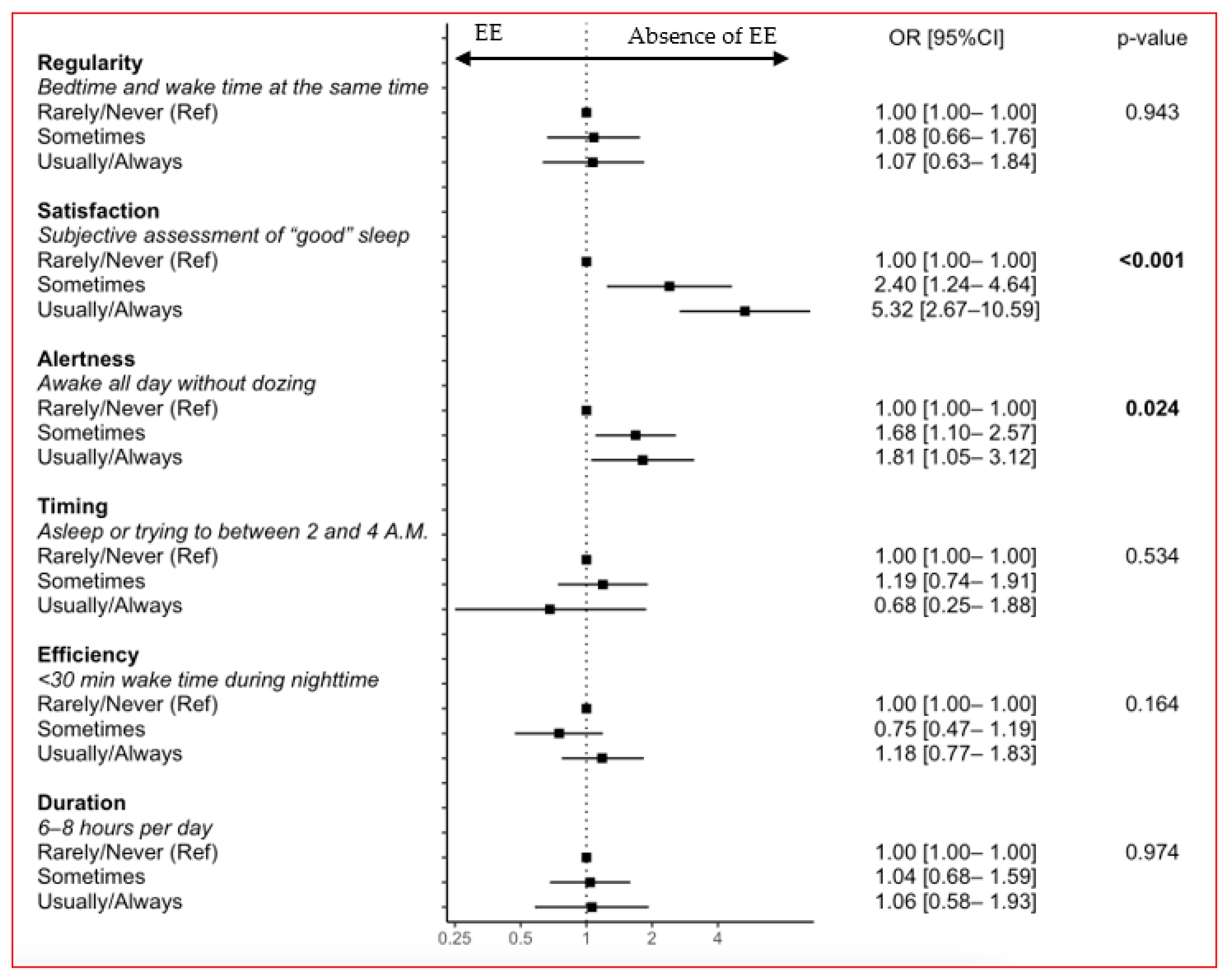
3.4. Associations between EE and Sleep Health Dimensions
4. Discussion
4.1. Key Results
4.2. Interpretation
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Maslach, C.; Jackson, S.E.; Leiter, M.P. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Menlo Park, CA, USA, 1996; ISBN 978-99963-45-77-7. [Google Scholar]
- Bayes, A.; Tavella, G.; Parker, G. The Biology of Burnout: Causes and Consequences. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2021, 22, 686–698. [Google Scholar] [CrossRef] [PubMed]
- De Hert, S. Burnout in Healthcare Workers: Prevalence, Impact and Preventative Strategies. Local Reg. Anesth. 2020, 13, 171–183. [Google Scholar] [CrossRef] [PubMed]
- Woo, T.; Ho, R.; Tang, A.; Tam, W. Global Prevalence of Burnout Symptoms among Nurses: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2020, 123, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Karuna, C.; Palmer, V.; Scott, A.; Gunn, J. Prevalence of Burnout among GPs: A Systematic Review and Meta-Analysis. Br. J. Gen. Pract. 2022, 72, e316–e324. [Google Scholar] [CrossRef]
- Gómez-Urquiza, J.L.; Aneas-López, A.B.; Fuente-Solana, E.I.; Albendín-García, L.; Díaz-Rodríguez, L.; Fuente, G.A. Prevalence, Risk Factors, and Levels of Burnout Among Oncology Nurses: A Systematic Review. Oncol. Nurs. Forum 2016, 43, E104–E120. [Google Scholar] [CrossRef]
- Lucas, G.; Colson, S.; Boyer, L.; Gentile, S.; Fond, G. Work Environment and Mental Health in Nurse Assistants, Nurses and Health Executives: Results from the AMADEUS Study. J. Nurs. Manag. 2022, 30, 2268–2277. [Google Scholar] [CrossRef]
- Geoffroy, P.A.; Le Goanvic, V.; Sabbagh, O.; Richoux, C.; Weinstein, A.; Dufayet, G.; Lejoyeux, M. Psychological Support System for Hospital Workers during the COVID-19 Outbreak: Rapid Design and Implementation of the Covid-Psy Hotline. Front. Psychiatry 2020, 11, 511. [Google Scholar] [CrossRef]
- Kancherla, B.S.; Upender, R.; Collen, J.F.; Rishi, M.A.; Sullivan, S.S.; Ahmed, O.; Berneking, M.; Flynn-Evans, E.E.; Peters, B.R.; Gurubhagavatula, I. What Is the Role of Sleep in Physician Burnout? J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2020, 16, 807–810. [Google Scholar] [CrossRef]
- Stewart, N.H.; Koza, A.; Dhaon, S.; Shoushtari, C.; Martinez, M.; Arora, V.M. Sleep Disturbances in Frontline Health Care Workers during the COVID-19 Pandemic: Social Media Survey Study. J. Med. Internet Res. 2021, 23, e27331. [Google Scholar] [CrossRef]
- Jahrami, H.; BaHammam, A.S.; Bragazzi, N.L.; Saif, Z.; Faris, M.; Vitiello, M.V. Sleep Problems during the COVID-19 Pandemic by Population: A Systematic Review and Meta-Analysis. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2021, 17, 299–313. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of Depression, Anxiety, and Insomnia among Healthcare Workers during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Brain. Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Ghahramani, S.; Lankarani, K.B.; Yousefi, M.; Heydari, K.; Shahabi, S.; Azmand, S. A Systematic Review and Meta-Analysis of Burnout Among Healthcare Workers During COVID-19. Front. Psychiatry 2021, 12, 758849. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep Health: Can We Define It? Does It Matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Ravyts, S.G.; Dzierzewski, J.M.; Perez, E.; Donovan, E.K.; Dautovich, N.D. Sleep Health as Measured by RU SATED: A Psychometric Evaluation. Behav. Sleep Med. 2019, 19, 48–56. [Google Scholar] [CrossRef]
- Brandolim Becker, N.; Martins, R.I.S.; Jesus, S.d.N.; Chiodelli, R.; Rieber, S.M. Sleep Health Assessment: A Scale Validation. Psychiatry Res. 2018, 259, 51–55. [Google Scholar] [CrossRef]
- Benítez, I.; Roure, N.; Pinilla, L.; Sapiña-Beltran, E.; Buysse, D.J.; Barbé, F.; de Batlle, J. Validation of the Satisfaction Alertness Timing Efficiency and Duration (SATED) Questionnaire for Sleep Health Measurement. Ann. Am. Thorac. Soc. 2020, 17, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Coelho, J.; Lopez, R.; Richaud, A.; Buysse, D.J.; Wallace, M.L.; Philip, P.; Micoulaud-Franchi, J.-A. Toward a Multi-Lingual Diagnostic Tool for the Worldwide Problem of Sleep Health: The French RU-SATED Validation. J. Psychiatr. Res. 2021, 143, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Furihata, R.; Tateyama, Y.; Nakagami, Y.; Akahoshi, T.; Itani, O.; Kaneita, Y.; Buysse, D.J. The Validity and Reliability of the Japanese Version of RU-SATED. Sleep Med. 2022, 91, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Buxton, O.M.; Lee, S.; Marino, M.; Beverly, C.; Almeida, D.M.; Berkman, L. Sleep Health and Predicted Cardiometabolic Risk Scores in Employed Adults from Two Industries. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2018, 14, 371–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubala, A.G.; Buysse, D.J.; Brindle, R.C.; Krafty, R.T.; Thayer, J.F.; Hall, M.H.; Kline, C.E. The Association between Physical Activity and a Composite Measure of Sleep Health. Sleep Breath. Schlaf Atm. 2020, 24, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Furihata, R.; Hall, M.H.; Stone, K.L.; Ancoli-Israel, S.; Smagula, S.F.; Cauley, J.A.; Kaneita, Y.; Uchiyama, M.; Buysse, D.J. Study of Osteoporotic Fractures (SOF) Research Group An Aggregate Measure of Sleep Health Is Associated with Prevalent and Incident Clinically Significant Depression Symptoms among Community-Dwelling Older Women. Sleep 2017, 40, zsw075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalmases, M.; Benítez, I.; Sapiña-Beltran, E.; Garcia-Codina, O.; Medina-Bustos, A.; Escarrabill, J.; Saltó, E.; Buysse, D.J.; Plana, R.E.; Sánchez-de-la-Torre, M.; et al. Impact of Sleep Health on Self-Perceived Health Status. Sci. Rep. 2019, 9, 7284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koutsimani, P.; Montgomery, A.; Georganta, K. The Relationship Between Burnout, Depression, and Anxiety: A Systematic Review and Meta-Analysis. Front. Psychol. 2019, 10, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alvaro, P.K.; Roberts, R.M.; Harris, J.K. A Systematic Review Assessing Bidirectionality between Sleep Disturbances, Anxiety, and Depression. Sleep 2013, 36, 1059–1068. [Google Scholar] [CrossRef]
- Wolkow, A.P.; Barger, L.K.; O’Brien, C.S.; Sullivan, J.P.; Qadri, S.; Lockley, S.W.; Czeisler, C.A.; Rajaratnam, S.M.W. Associations between Sleep Disturbances, Mental Health Outcomes and Burnout in Firefighters, and the Mediating Role of Sleep during Overnight Work: A Cross-Sectional Study. J. Sleep Res. 2019, 28, e12869. [Google Scholar] [CrossRef]
- Thielmann, B.; Schierholz, R.S.; Böckelmann, I. Subjective and Objective Consequences of Stress in Subjects with Subjectively Different Sleep Quality—A Cross-Sectional Study. Int. J. Environ. Res. Public. Health 2021, 18, 9990. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. Lond. Engl. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Leger, D.; Esquirol, Y.; Gronfier, C.; Metlaine, A. Le travail posté et de nuit et ses conséquences sur la santé: État des lieux et recommandations. Presse Médicale 2018, 47, 991–999. [Google Scholar] [CrossRef]
- Cox, B.; van Oyen, H.; Cambois, E.; Jagger, C.; le Roy, S.; Robine, J.-M.; Romieu, I. The Reliability of the Minimum European Health Module. Int. J. Public Health 2009, 54, 55–60. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. An Ultra-Brief Screening Scale for Anxiety and Depression: The PHQ-4. Psychosomatics 2009, 50, 613–621. [Google Scholar] [CrossRef] [Green Version]
- Yuksel, D.; McKee, G.B.; Perrin, P.B.; Alzueta, E.; Caffarra, S.; Ramos-Usuga, D.; Arango-Lasprilla, J.C.; Baker, F.C. Sleeping When the World Locks down: Correlates of Sleep Health during the COVID-19 Pandemic across 59 Countries. Sleep Health 2021, 7, 134–142. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Sloan, J.A.; Shanafelt, T.D. Single Item Measures of Emotional Exhaustion and Depersonalization Are Useful for Assessing Burnout in Medical Professionals. J. Gen. Intern. Med. 2009, 24, 1318–1321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, C.P.; Dyrbye, L.N.; Satele, D.V.; Sloan, J.A.; Shanafelt, T.D. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J. Gen. Intern. Med. 2012, 27, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Flickinger, T.E.; Kon, R.H.; Jacobsen, R.; Owens, J.; Schorling, J.; Plews-Ogan, M. Single-Item Burnout Measure Correlates Well with Emotional Exhaustion Domain of Burnout but Not Depersonalization among Medical Students. J. Gen. Intern. Med. 2020, 35, 3383–3385. [Google Scholar] [CrossRef] [PubMed]
- Lim, N.; Kim, E.K.; Kim, H.; Yang, E.; Lee, S.M. Individual and Work-Related Factors Influencing Burnout of Mental Health Professionals: A Meta-Analysis. J. Employ. Couns. 2010, 47, 86–96. [Google Scholar] [CrossRef]
- Demir Zencirci, A.; Arslan, S. Morning-Evening Type and Burnout Level as Factors Influencing Sleep Quality of Shift Nurses: A Questionnaire Study. Croat. Med. J. 2011, 52, 527–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demir, A.; Ulusoy, M.; Ulusoy, M.F. Investigation of Factors Influencing Burnout Levels in the Professional and Private Lives of Nurses. Int. J. Nurs. Stud. 2003, 40, 807–827. [Google Scholar] [CrossRef]
- Royston, P.; Ambler, G.; Sauerbrei, W. The Use of Fractional Polynomials to Model Continuous Risk Variables in Epidemiology. Int. J. Epidemiol. 1999, 28, 964–974. [Google Scholar] [CrossRef] [Green Version]
- Selvin, S. Statistical Analysis of Epidemiologic Data, 2nd ed.; Oxford University Press: New York, NY, USA, 1996; ISBN 978-0-19-509760-3. [Google Scholar]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Burnout-Depression Overlap: A Review. Clin. Psychol. Rev. 2015, 36, 28–41. [Google Scholar] [CrossRef] [Green Version]
- Grandner, M.A. Sleep and Health, 1st ed.; Academic Press Inc.: Cambridge, MA, USA, 2019. [Google Scholar]
- Taillard, J.; Sagaspe, P.; Philip, P.; Bioulac, S. Sleep Timing, Chronotype and Social Jetlag: Impact on Cognitive Abilities and Psychiatric Disorders. Biochem. Pharmacol. 2021, 191, 114438. [Google Scholar] [CrossRef]
- Karasek, R.; Brisson, C.; Kawakami, N.; Houtman, I.; Bongers, P.; Amick, B. The Job Content Questionnaire (JCQ): An Instrument for Internationally Comparative Assessments of Psychosocial Job Characteristics. J. Occup. Health Psychol. 1998, 3, 322–355. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A Systematic Review Including Meta-Analysis of Work Environment and Burnout Symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, C.M.; Morris, N.J.; Nock, N.L. Structural Equation Modeling. Methods Mol. Biol. Clifton NJ 2012, 850, 495–512. [Google Scholar] [CrossRef]
- Barham, W.T.; Buysse, D.J.; Kline, C.E.; Kubala, A.G.; Brindle, R.C. Sleep Health Mediates the Relationship between Physical Activity and Depression Symptoms. Sleep Breath. Schlaf Atm. 2021, 26, 1341–1349. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.L.; Yu, L.; Buysse, D.J.; Stone, K.L.; Redline, S.; Smagula, S.F.; Stefanick, M.L.; Kritz-Silverstein, D.; Hall, M.H. Multidimensional Sleep Health Domains in Older Men and Women: An Actigraphy Factor Analysis. Sleep 2018, 44, zsaa181. [Google Scholar] [CrossRef] [PubMed]
- Wallace, M.L.; Stone, K.; Smagula, S.F.; Hall, M.H.; Simsek, B.; Kado, D.M.; Redline, S.; Vo, T.N.; Buysse, D.J. Osteoporotic Fractures in Men (MrOS) Study Research Group Which Sleep Health Characteristics Predict All-Cause Mortality in Older Men? An Application of Flexible Multivariable Approaches. Sleep 2018, 41, zsx189. [Google Scholar] [CrossRef] [PubMed]
- Albakri, U.; Drotos, E.; Meertens, R. Sleep Health Promotion Interventions and Their Effectiveness: An Umbrella Review. Int. J. Environ. Res. Public. Health 2021, 18, 5533. [Google Scholar] [CrossRef]
- Karasek, R. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- De Sousa, G.M.; de Oliveira Tavares, V.D.; de Meiroz Grilo, M.L.P.; Coelho, M.L.G.; de Lima-Araújo, G.L.; Schuch, F.B.; Galvão-Coelho, N.L. Mental Health in COVID-19 Pandemic: A Meta-Review of Prevalence Meta-Analyses. Front. Psychol. 2021, 12, 703838. [Google Scholar] [CrossRef]
- Rothman, K.J.; Gallacher, J.E.; Hatch, E.E. Why Representativeness Should Be Avoided. Int. J. Epidemiol. 2013, 42, 1012–1014. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Total n = 1069 | Sleep Health a | Emotional Exhaustion b | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Good n = 474 | Poor n = 595 | Statistic | p-Value | Yes n = 143 | No n = 926 | Statistic | p-Value | ||
| Age (years) | 39.2 ± 11.3 | 39.8 ± 10.8 | 39.8 ± 11.7 | t = 1.41 | 0.159 | 40.4 ± 10.8 | 39.1 ± 11.4 | t = 1.39 | 0.167 |
Sex
| 169 (15.8%) 900 (84.2%) | 80 (16.9%) 394 (83.1%) | 89 (15.0%) 506 (85.0%) | X2 = 0.593 | 0.393 | 12 (8.4%) 131 (91.6%) | 157 (17.0%) 769 (83.0%) | X2 = 6.20 | 0.009 |
Job category
| 866 (81.0%) 203 (19.0%) | 332 (70.0%) 142 (30.0%) | 534 (89.8%) 61 (10.2%) | X2 = 65.3 | <0.001 | 116 (81.1%) 27 (18.9%) | 750 (81.0%) 176 (19.0%) | X2 < 0.001 | 0.972 |
Perceived socioeconomic status
| 501 (46.9%) 501 (46.9%) 67 (6.3%) | 287 (60.6%) 172 (36.3%) 15 (3.2%) | 214 (36.0%) 329 (55.3%) 52 (8.7%) | X2 = 67.4 | <0.001 | 56 (39.2%) 67 (46.9%) 20 (14.0%) | 445 (48.1%) 434 (46.9%) 47 (5.1%) | X2 = 17.8 | <0.001 |
Work schedule:
| 514 (48.1%) 555 (51.9%) | 192 (40.5%) 282 (59.5%) | 322 (54.1%) 273 (45.9%) | X2 = 19.0 | <0.001 | 67 (46.9%) 76 (53.2%) | 447 (48.3%) 479 (51.7%) | X2 = 0.051 | 0.821 |
Night work:
| 199 (18.6%) 870 (81.4%) | 50 (10.6%) 424 (89.4%) | 149 (25.0%) 446 (75.0%) | X2 = 35.6 | <0.001 | 22 (15.4%) 121 (84.6%) | 177 (19.1%) 749 (80.9%) | X2 = 0.905 | 0.342 |
| Telecommuting: Yes | 168 (15.7%) | 81 (17.1%) | 87 (14.6%) | X2 = 1.03 | 0.271 | 24 (16.8%) | 144 (15.6%) | X2 = 0.064 | 0.706 |
| Work in a COVID-19 unit: Yes | 234 (21.9%) | 90 (19.0%) | 144 (24.2%) | X2 = 3.90 | 0.041 | 30 (21.0%) | 204 (22.0%) | X2 = 0.030 | 0.777 |
| Self-perceived health: Poor | 163 (15.3%) | 32 (6.8%) | 131 (22.0%) | X2 = 46.4 | <0.001 | 44 (30.8%) | 119 (12.9%) | X2 = 29.4 | <0.001 |
| Anxiety symptoms: Yes | 384 (35.9%) | 98 (20.7%) | 286 (48.1%) | X2 = 84.8 | <0.001 | 110 (76.9%) | 274 (29.6%) | X2 = 119 | <0.001 |
| Depressive symptoms: Yes | 167 (15.6%) | 34 (7.2%) | 133 (22.4%) | X2 = 45.0 | <0.001 | 65 (45.5%) | 102 (11.0%) | X2 = 109 | <0.001 |
| Sleep health: Good | 474 (44.3%) | 38 (26.6%) | 436 (47.1%) | X2 = 20.3 | <0.001 | ||||
| Emotional exhaustion: Yes | 143 (13.4%) | 38 (8.0%) | 105 (17.7%) | X2 = 20.3 | <0.001 | <0.001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coelho, J.; Taillard, J.; Bernard, A.; Lopez, R.; Fond, G.; Boyer, L.; Lucas, G.; Alla, F.; Buysse, D.J.; Wallace, M.L.; et al. Emotional Exhaustion, a Proxy for Burnout, Is Associated with Sleep Health in French Healthcare Workers without Anxiety or Depressive Symptoms: A Cross-Sectional Study. J. Clin. Med. 2023, 12, 1895. https://doi.org/10.3390/jcm12051895
Coelho J, Taillard J, Bernard A, Lopez R, Fond G, Boyer L, Lucas G, Alla F, Buysse DJ, Wallace ML, et al. Emotional Exhaustion, a Proxy for Burnout, Is Associated with Sleep Health in French Healthcare Workers without Anxiety or Depressive Symptoms: A Cross-Sectional Study. Journal of Clinical Medicine. 2023; 12(5):1895. https://doi.org/10.3390/jcm12051895
Chicago/Turabian StyleCoelho, Julien, Jacques Taillard, Adèle Bernard, Régis Lopez, Guillaume Fond, Laurent Boyer, Guillaume Lucas, François Alla, Daniel J. Buysse, Meredith L. Wallace, and et al. 2023. "Emotional Exhaustion, a Proxy for Burnout, Is Associated with Sleep Health in French Healthcare Workers without Anxiety or Depressive Symptoms: A Cross-Sectional Study" Journal of Clinical Medicine 12, no. 5: 1895. https://doi.org/10.3390/jcm12051895
APA StyleCoelho, J., Taillard, J., Bernard, A., Lopez, R., Fond, G., Boyer, L., Lucas, G., Alla, F., Buysse, D. J., Wallace, M. L., Verdun-Esquer, C., Geoffroy, P. -A., d’Incau, E., Philip, P., & Micoulaud-Franchi, J. -A. (2023). Emotional Exhaustion, a Proxy for Burnout, Is Associated with Sleep Health in French Healthcare Workers without Anxiety or Depressive Symptoms: A Cross-Sectional Study. Journal of Clinical Medicine, 12(5), 1895. https://doi.org/10.3390/jcm12051895