Increasing Number of Cases Due to Candida auris in North Italy, July 2019–December 2022

 , ,
, ,  add
Show full author list
add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Notification of Cases
3.2. Characteristics of Cases Colonised or Infected by C. auris
3.3. Laboratory Testing
3.4. Environmental Investigation
3.5. Control Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanyaolu, A.; Okorie, C.; Marinkovic, A.; Abbasi, A.F.; Prakash, S.; Mangat, J.; Hosein, Z.; Haider, N.; Chan, J. Candida auris: An Overview of the Emerging Drug-Resistant Fungal Infection. Infect. Chemother. 2022, 54, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Tracking Candida Auris. Available online: https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html (accessed on 1 December 2022).
- Ahmad, S.; Alfouzan, W. Candida auris: Epidemiology, Diagnosis, Pathogenesis, Antifungal Susceptibility, and Infection Control Measures to Combat the Spread of Infections in Healthcare Facilities. Microorganisms 2021, 9, 807. [Google Scholar] [CrossRef] [PubMed]
- Pruden, A.; Vikesland, P.J.; Davis, B.C.; de Roda Husman Ana, M. Seizing the moment: Now is the time for integrated global surveillance of antimicrobial resistance in wastewater environments. Curr. Opin. Microbiol. 2021, 64, 91–99. [Google Scholar] [CrossRef] [PubMed]
- OECD; ECDC; EFSA; EMA. Antimicrobial Resistance in the EU/EEA: A One Health Response. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/antimicrobial-resistance-policy-brief-2022.pdf (accessed on 1 December 2022).
- Eze, N.; Cecchini, M.; Hashiguchi, T.O. Antimicrobial Resistance in Long-Term Care Facilities; OECD Health Working Papers; No. 136; OECD Publishing: Paris, France, 2022. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID-19: U.S. Impact on Antimicrobial Resistance, Special Report 2022. 2022. Available online: https://stacks.cdc.gov/view/cdc/117915 (accessed on 1 December 2022).
- Lee, W.G.; Shin, J.H.; Uh, Y.; Kang, M.G.; Kim, S.H.; Park, K.H.; Jang, H.-C. First three reported cases of nosocomial fungemia caused by Candida auris. J. Clin. Microbiol. 2011, 49, 3139–3142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, K.; Makimura, K.; Hasumi, Y.; Nishiyama, Y.; Uchida, K.; Yamaguchi, H. Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol. Immunol. 2009, 53, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Desnos-Ollivier, M.; Fekkar, A.; Bretagne, S. Earliest case of Candida auris infection imported in 2007 in Europe from India prior to the 2009 description in Japan. J. Mycol. Med. 2021, 31, 101139. [Google Scholar] [CrossRef]
- Kohlenberg, A.; Struelens, M.J.; Monnet, D.L.; Plachouras, D.; Candida auris survey collaborative group. Candida auris: Epidemiological situation, laboratory capacity and preparedness in European Union and European Economic Area countries, 2013 to 2017. Euro. Surveill. 2018, 23, 18–00136. [Google Scholar] [CrossRef] [Green Version]
- Plachouras, D.; Lotsch, F.; Kohlenberg, A.; Monnet, D.L.; Candida auris survey collaborative group. Candida auris: Epidemiological situation, laboratory capacity and preparedness in the European Union and European Economic Area*, January 2018 to May 2019. Euro. Surveill. 2020, 25, 2000240. [Google Scholar] [CrossRef] [Green Version]
- Rossi, A.; Chavez, J.; Iverson, T.; Hergert, J.; Oakeson, K.; LaCross, N.; Njoku, C.; Gorzalski, A.; Gerrity, D. Candida auris Discovery through Community Wastewater Surveillance during Healthcare Outbreak, Nevada, USA, 2022. Emerg. Infect. Dis. 2023, 29, 422–425. [Google Scholar] [CrossRef]
- Hu, S.; Zhu, F.; Jiang, W.; Wang, Y.; Quan, Y.; Zhang, G.; Gu, F.; Yang, Y. Retrospective Analysis of the Clinical Characteristics of Candida auris Infection Worldwide From 2009 to 2020. Front. Microbiol. 2021, 12, 658329. [Google Scholar] [CrossRef]
- Rossow, J.; Ostrowsky, B.; Adams, E.; Greenko, J.; McDonald, R.; Vallabhaneni, S.; Forsberg, K.; Perez, S.; Lucas, T.; Alroy, K.A.; et al. Factors Associated With Candida auris Colonization and Transmission in Skilled Nursing Facilities With Ventilator Units, New York, 2016–2018. Clin. Infect. Dis. 2021, 72, e753–e760. [Google Scholar] [CrossRef] [PubMed]
- Giacobbe, D.R.; Magnasco, L.; Sepulcri, C.; Mikulska, M.; Koehler, P.; Cornely, O.A.; Bassetti, M. Recent advances and future perspectives in the pharmacological treatment of Candida auris infections. Expert Rev. Clin. Pharmacol. 2021, 14, 1205–1220. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Candida Auris in Healthcare-Settings—Europe, First Update; ECDC: Stockholm, Sweden, 2018. [Google Scholar]
- Vinayagamoorthy, K.; Pentapati, K.C.; Prakash, H. Prevalence, risk factors, treatment and outcome of multidrug resistance Candida auris infections in Coronavirus disease (COVID-19) patients: A systematic review. Mycoses 2022, 65, 613–624. [Google Scholar] [CrossRef]
- Thoma, R.; Seneghini, M.; Seiffert, S.N.; Vuichard Gysin, D.; Scanferla, G.; Haller, S.; Flury, D.; Boggian, K.; Kleger, G.-R.; Filipovic, M.; et al. The challenge of preventing and containing outbreaks of multidrug-resistant organisms and Candida auris during the coronavirus disease 2019 pandemic: Report of a carbapenem-resistant Acinetobacter baumannii outbreak and a systematic review of the literature. Antimicrob. Resist Infect. Control. 2022, 11, 12. [Google Scholar]
- Welsh, R.M.; Bentz, M.L.; Shams, A.; Houston, H.; Lyons, A.; Rose, L.J.; Litvintseva, A.P. Survival, Persistence, and Isolation of the Emerging Multidrug-Resistant Pathogenic Yeast Candida auris on a Plastic Health Care Surface. J. Clin. Microbiol. 2017, 55, 2996–3005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kean, R.; McKloud, E.; Townsend, E.M.; Sherry, L.; Delaney, C.; Jones, B.L.; Williams, C.; Ramage, G. The comparative efficacy of antiseptics against Candida auris biofilms. Int. J. Antimicrob. Agents 2018, 52, 673–677. [Google Scholar] [CrossRef] [Green Version]
- Keighley, C.; Garnham, K.; Harch, S.A.J.; Robertson, M.; Chaw, K.; Teng, J.C.; Chen, S.C.-A. Candida auris: Diagnostic Challenges and Emerging Opportunities for the Clinical Microbiology Laboratory. Curr. Fungal. Infect. Rep. 2021, 15, 116–126. [Google Scholar] [CrossRef]
- Dennis, E.K.; Chaturvedi, S.; Chaturvedi, V. So Many Diagnostic Tests, So Little Time: Review and Preview of Candida auris Testing in Clinical and Public Health Laboratories. Front. Microbiol. 2021, 12, 757835. [Google Scholar] [CrossRef]
- Council of State and Territorial Epidemiologists. Standardized Case Definition for Candida Auris Causing Clinical Infection and Colonization in People; (17-ID-03); Council of State and Territorial Epidemiologists: Atlanta, GA, USA, 2018. [Google Scholar]
- Centers for Disease Control and Prevention. Candida Auris. Available online: https://www.cdc.gov/fungal/candida-auris/index.html (accessed on 1 December 2022).
- Crea, F.; Codda, G.; Orsi, A.; Battaglini, A.; Giacobbe, D.R.; Delfino, E.; Ungaro, R.; Marchese, A. Isolation of Candida auris from invasive and non-invasive samples of a patient suffering from vascular disease, Italy, July 2019. Euro. Surveill. 2019, 24, 1900549. [Google Scholar] [CrossRef] [Green Version]
- Mikulska, M.; Magnasco, L.; Signori, A.; Sepulcri, C.; Dettori, S.; Tutino, S.; Vena, A.; Miletich, F.; Ullah, N.; Morici, P.; et al. Sensitivity of Serum Beta-D-Glucan in Candidemia According to Candida Species Epidemiology in Critically Ill Patients Admitted to the Intensive Care Unit. J. Fungi 2022, 8, 921. [Google Scholar] [CrossRef]
- Briano, F.; Magnasco, L.; Sepulcri, C.; Dettori, S.; Dentone, C.; Mikulska, M.; Ball, L.; Vena, A.; Robba, C.; Patroniti, N.; et al. Candida auris Candidemia in Critically Ill, Colonized Patients: Cumulative Incidence and Risk Factors. Infect. Dis. Ther. 2022, 11, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs for Antifungal agents, Version 10.0. 2020. Available online: http://www.eucast.org/astoffungi/clinicalbreakpointsforantifungals/ (accessed on 1 December 2022).
- Magnasco, L.; Mikulska, M.; Giacobbe, D.R.; Taramasso, L.; Vena, A.; Dentone, C.; Dettori, S.; Tutino, S.; Labate, L.; Di Pilato, V.; et al. Spread of Carbapenem-Resistant Gram-Negatives and Candida auris during the COVID-19 Pandemic in Critically Ill Patients: One Step Back in Antimicrobial Stewardship? Microorganisms 2021, 9, 95. [Google Scholar] [CrossRef] [PubMed]
- Di Pilato, L.; Codda, G.; Ball, L.; Giacobbe, D.R.; Willison, E.; Mikulska, M.; Magnasco, L.; Crea, F.; Vena, A.; Pelosi, P.; et al. Molecular Epidemiological Investigation of a Nosocomial Cluster of C. auris: Evidence of Recent Emergence in Italy and Ease of Transmission during the COVID-19 Pandemic. J. Fungi 2021, 7, 140. [Google Scholar] [CrossRef] [PubMed]
- Piatti, G.; Sartini, M.; Cusato, C.; Schito, A.M. Colonization by Candida auris in critically ill patients: Role of cutaneous and rectal localization during an outbreak. J. Hosp. Infect. 2022, 120, 85–89. [Google Scholar] [CrossRef]
- Koehler, P.; Arendrup, M.C.; Arikan-Akdagli, S.; Bassetti, M.; Bretagne, S.; Klingspor, L.; Lagrou, K.; Meis, J.F.; Rautemaa-Richardson, R.; Schelenz, S.; et al. ECMM CandiReg-A ready to use platform for outbreaks and epidemiological studies. Mycoses 2019, 62, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberg, A.; Monnet, D.L.; Plachouras, D.; Candida auris survey collaborative group; Candida auris survey collaborative group. Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA, 2020 to 2021. Euro. Surveill. 2022, 27, 2200846. [Google Scholar] [CrossRef]
- Saris, K.; Meis, J.F.; Bano, J.R.; Tacconelli, E.; van de Belt Tom, H.; Voss, A. Does Online Search Behavior Coincide with Candida auris Cases? An Exploratory Study. J. Fungi 2019, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Du, H.; Bing, J.; Nobile, C.J.; Huang, G. Candida auris infections in China. Virulence 2022, 13, 589–591. [Google Scholar] [CrossRef]
- Okoye, C.A.; Nweze, E.; Ibe, C. Invasive candidiasis in Africa, what is the current picture? Pathog. Dis. 2022, 80, ftac012. [Google Scholar] [CrossRef]
- Zerrouki, H.; Ibrahim, A.; Rebiahi, S.; Elhabiri, Y.; Benhaddouche, D.; de Groot, T.; Meis, J.F.; Rolain, J.; Bittar, F. Emergence of Candida auris in intensive care units in Algeria. Mycoses 2022, 65, 753–759. [Google Scholar] [CrossRef]
- Vaseghi, N.; Sharifisooraki, J.; Khodadadi, H.; Nami, S.; Safari, F.; Ahangarkani, F.; Meis, J.F.; Badali, H.; Morovati, H. Global prevalence and subgroup analyses of coronavirus disease (COVID-19) associated Candida auris infections (CACa): A systematic review and meta-analysis. Mycoses 2022, 65, 683–703. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xu, J. Population genomic analyses reveal evidence for limited recombination in the superbug Candida auris in nature. Comput. Struct. Biotechnol. J. 2022, 20, 3030–3040. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.E.; Jacobs, J.L.; Dennis, E.K.; Taimur, S.; Rana, M.; Patel, D.; Gitman, M.; Patel, G.; Schaefer, S.; Iyer, K.; et al. Candida auris Pan-Drug-Resistant to Four Classes of Antifungal Agents. Antimicrob. Agents Chemother. 2022, 66, e0005322. [Google Scholar] [CrossRef]
- Yadav, A.; Jain, K.; Wang, Y.; Pawar, K.; Kaur, H.; Sharma, K.K.; Tripathy, V.; Singh, A.; Xu, J.; Chowdhary, A. Candida auris on Apples: Diversity and Clinical Significance. mBio 2022, 13, e0051822-22. [Google Scholar] [CrossRef] [PubMed]
- Aldejohann, A.M.; Wiese-Posselt, M.; Gastmeier, P.; Kurzai, O. Expert recommendations for prevention and management of Candida auris transmission. Mycoses 2022, 65, 590–598. [Google Scholar] [CrossRef]
- de Jong, A.W.; van den Ende, B.G.; Hagen, F. Molecular Tools for Candida auris Identification and Typing. Methods Mol. Biol. 2022, 2517, 33–41. [Google Scholar]
- Johnson, E.M.; Borman, A.M. Susceptibility Testing of Candida auris Isolates. Methods Mol. Biol. 2022, 2517, 55–71. [Google Scholar]
- Izadi, A.; Aghaei Gharehbolagh, S.; Sadeghi, F.; Talebi, M.; Darmiani, K.; Zarrinnia, A.; Zarei, F.; Peymaeei, F.; Khojasteh, S.; Borman, A.M.; et al. Drug repurposing against Candida auris: A systematic review. Mycoses 2022, 65, 784–793. [Google Scholar] [CrossRef]
- Bandara, H.M.H.N.; Samaranayake, L.P. Emerging strategies for environmental decontamination of the nosocomial fungal pathogen Candida auris. J. Med. Microbiol. 2022, 71, 001548. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients’ Characteristics (%) | Liguria N = 297 | Piedmont N = 48 | Emilia-Romagna N = 15 | Total N = 360 |
|---|---|---|---|---|
| Median age (years, range) | N = 295 64 (0–91) | N = 48 64 (22–82) | N = 15 61.5 (47–87) | N = 358 64 (0–91) |
| Gender | N = 297 | N = 48 | N = 12 | N = 357 |
| Males | 195 (65.7) | 32 (66.7) | 10 (83.3) | 237 (66.3) |
| Females | 102 (34.3) | 16 (33.3) | 2 (16.7) | 120 (33.6) |
| Sample type | N = 294 | N = 48 | N = 15 | N = 357 |
| Blood | 25 (8.5) | 2 (4.2) | 3 (20) | 30 (8.4) |
| BAL/bronchial aspirate | 40 (13.6) | 3 (6.3) | 6 (40) | 49 (13.7) |
| CVC | 0 | 1 (2.1) | 1 (6.7) | 2 (0.6) |
| Sputum | 1 (0.3) | 0 | 0 | 1 (0.3) |
| Surgical wound | 1 (0.3) | 0 | 0 | 1 (0.3) |
| Swab (inguinal/axillary and/or rectal) | 217 (73.8) | 40 (83.3) | 3 (20) | 260 (72.8) |
| Urine | 10 (3.4) | 2 (4.2) | 2 (13.3) | 14 (3.9) |
| Hospital ward | N = 296 | N = 48 | N = 15 | N = 359 |
| Emergency room | 6 (2) | 0 | 0 | 6 (1.7) |
| Geriatrics | 0 | 0 | 2 (13.3) | 2 (0.6) |
| ICU | 228 (77.0) | 46 (95.8) | 10 (66.7) | 284 (79.1) |
| Internal medicine | 31 (10.5) | 1 (2.1) | 0 | 32 (8.9) |
| Rehabilitation unit | 2 (0.7) | 0 | 3 (20) | 5 (1.4) |
| Surgery | 29 (9.8) | 1 (2.1) | 0 | 30 (8.4) |
| Main comorbidity/medical issue | N = 289 | N = 48 | N = 5 | N = 342 |
| No symptoms due to C. auris | 54 (18.7) | 48 (100) | 14 (93.3) | 116 (33.9) |
| Acute respiratory disease | 19 (6.6) | 5 (10.4) | 2 (40.0) | 26 (7.6) |
| Bacteraemia | 9 (3.0) | 2 (4.2) | 2 (40.0) | 13 (3.8) |
| Chronic respiratory disease | 4 (1.4) | 1 (2.1) | 0 | 5 (1.5) |
| Cardiac disease | 21 (7.3) | 5 (10.4) | 0 | 26 (7.6) |
| SARS-CoV-2 positive/COVID-19 | 89 (30.8) | 14 (29.2) | 0 | 103 (30.1) |
| Diabetes | 3 (1.0) | 2 (4.2) | 0 | 5 (1.5) |
| Immunosuppressive disorder/Cancer | 4 (1.4) | 6 (12.5) | 0 | 10 (2.9) |
| Intestinal/renal/mediastinal disorder | 0 | 10 (20.8) | 0 | 10 (2.9) |
| Neurologic disorder | 62 (21.5) | 2 (4.2) | 1 (20.0) | 65 (19.0) |
| Sepsis/septic shock | 32 (11.1) | 0 | 0 | 32 (9.4) |
| Surgery | 38 (13.1) | 0 | 0 | 38 (11.1) |
| Trauma | 14 (4.8) | 1 (2.1) | 0 | 15 (4.4) |
| Median time between diagnosis and death (days) | 6.0 * | 10.0 § | n.a. | n.a. |
| In-hospital lethality | 119 (40.1) | 20 (41.7) | 6 (50.0) | N = 145 (40.3) |
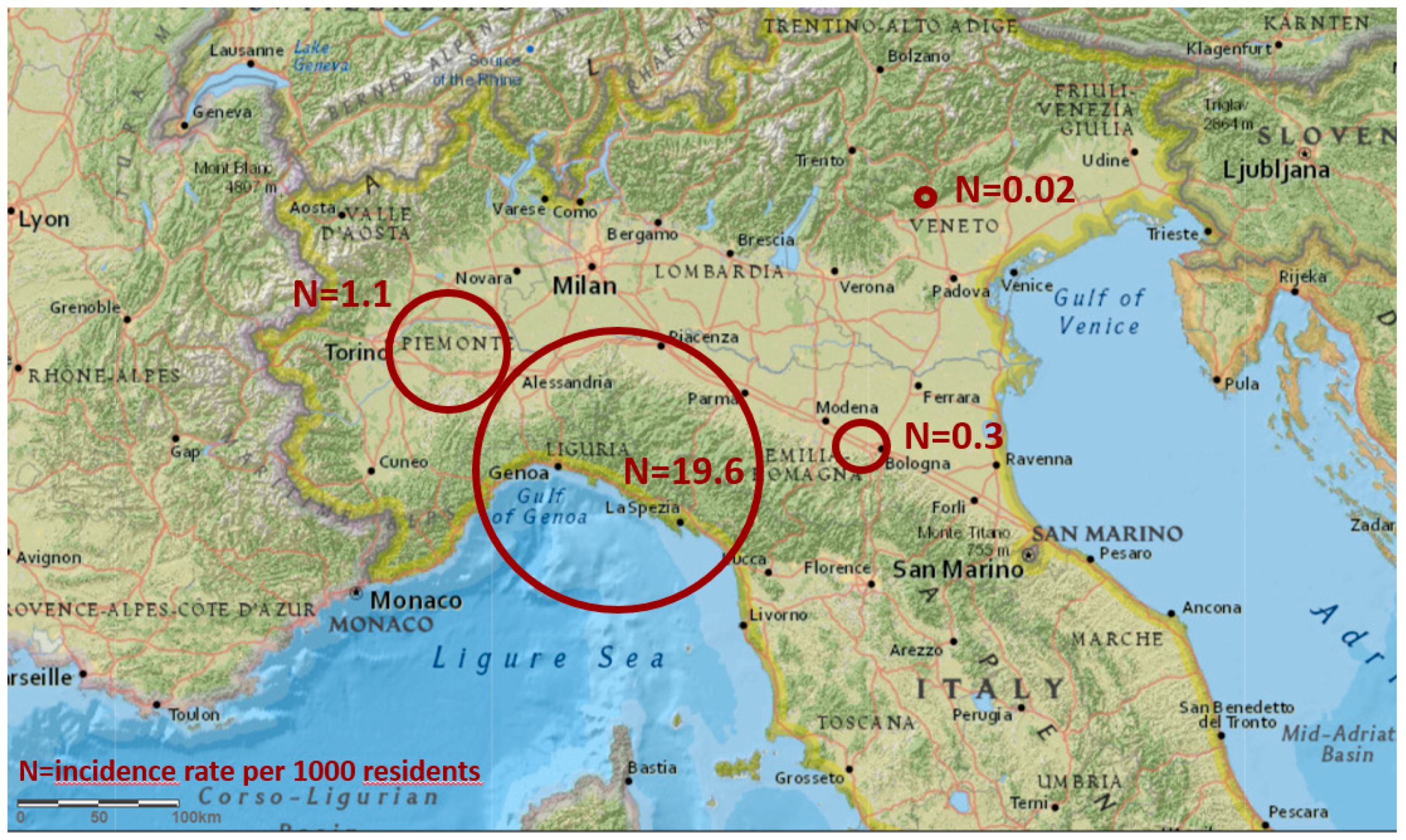
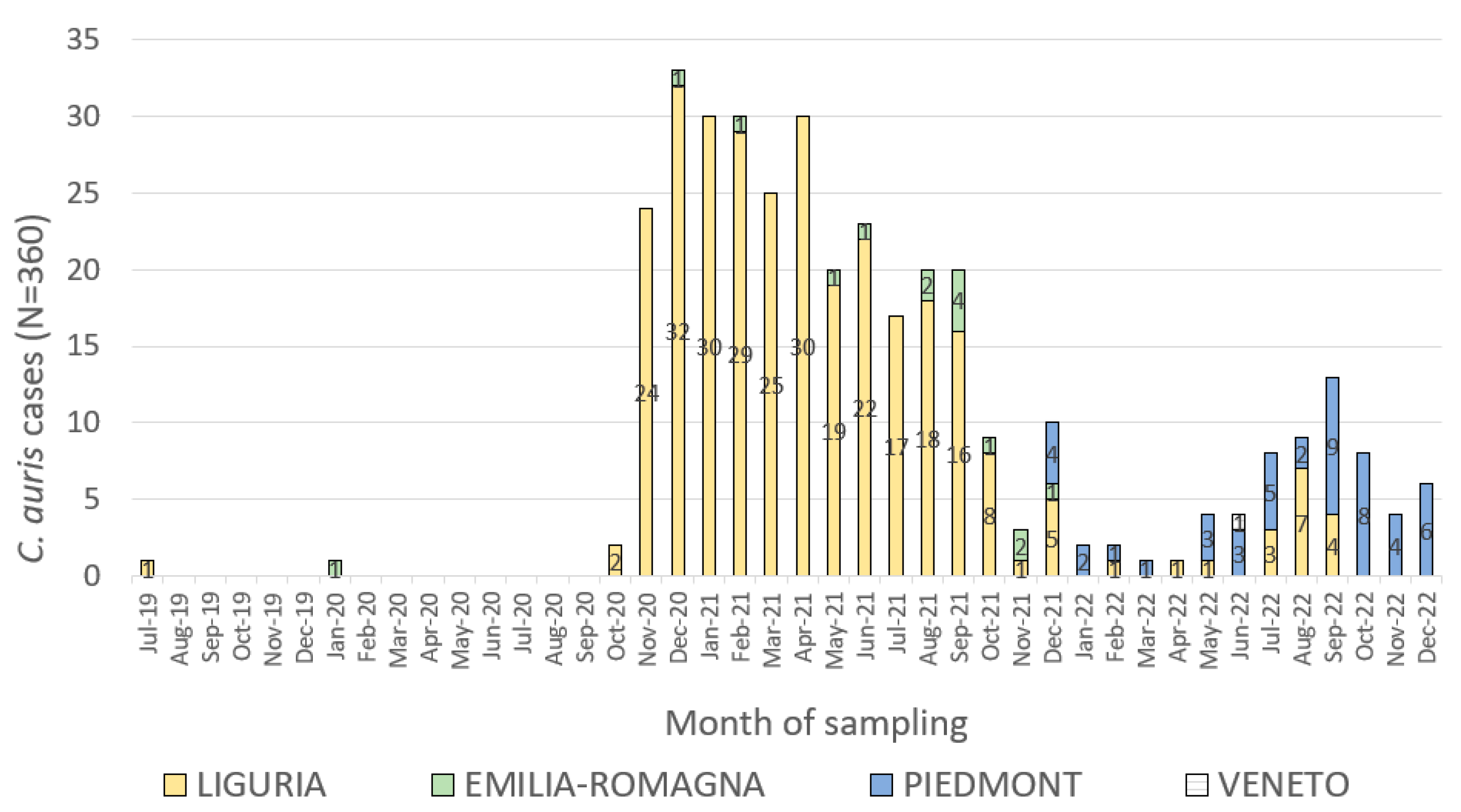
| Region | N. of Cases | Incidence per 1000 Residents | N. of Residents (1 Jan 2021) | N. of Hospital/Healthcare Beds (1 Jan 2019) |
|---|---|---|---|---|
| Liguria | 297 | 19.6 | 1,518,495 | 5723 |
| Piedmont | 48 | 1.1 | 4,274,945 | 16,513 |
| Emilia-Romagna | 15 | 0.3 | 4,438,937 | 17,308 |
| Veneto | 1 | 0.02 | 4,869,830 | 17,472 |
| Total | 361 | 0.024 | 15,102,207 | 57,016 |
| Antifungal Drugs | MIC Range (mcg/mL) |
|---|---|
| Triazoles | |
| Fluconazole | ≤0.0019–8 |
| Itraconazole | ≤0.0312–1 |
| Posaconazole | ≤0.0078–0.25 |
| Voriconazole (and other 2° generation azoles) | ≤0.0078–2 |
| Polyenes | |
| Amphotericin B | ≤0.0312–2 |
| Anidulafungin | ≤0.0019–0.125 |
| Caspofungin | 0.0156–0.25 |
| Micafungin | ≤0.0019–0.12 |
| Flucytosine | ≤0.0625–0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sticchi, C.; Raso, R.; Ferrara, L.; Vecchi, E.; Ferrero, L.; Filippi, D.; Finotto, G.; Frassinelli, E.; Silvestre, C.; Zozzoli, S.; et al. Increasing Number of Cases Due to Candida auris in North Italy, July 2019–December 2022. J. Clin. Med. 2023, 12, 1912. https://doi.org/10.3390/jcm12051912
Sticchi C, Raso R, Ferrara L, Vecchi E, Ferrero L, Filippi D, Finotto G, Frassinelli E, Silvestre C, Zozzoli S, et al. Increasing Number of Cases Due to Candida auris in North Italy, July 2019–December 2022. Journal of Clinical Medicine. 2023; 12(5):1912. https://doi.org/10.3390/jcm12051912
Chicago/Turabian StyleSticchi, Camilla, Roberto Raso, Lorenza Ferrara, Elena Vecchi, Loredana Ferrero, Daniela Filippi, Giuseppe Finotto, Elena Frassinelli, Carlo Silvestre, Susanna Zozzoli, and et al. 2023. "Increasing Number of Cases Due to Candida auris in North Italy, July 2019–December 2022" Journal of Clinical Medicine 12, no. 5: 1912. https://doi.org/10.3390/jcm12051912
APA StyleSticchi, C., Raso, R., Ferrara, L., Vecchi, E., Ferrero, L., Filippi, D., Finotto, G., Frassinelli, E., Silvestre, C., Zozzoli, S., Ambretti, S., Diegoli, G., Gagliotti, C., Moro, M. L., Ricchizzi, E., Tumietto, F., Russo, F., Tonon, M., Maraglino, F., ... Sabbatucci, M. (2023). Increasing Number of Cases Due to Candida auris in North Italy, July 2019–December 2022. Journal of Clinical Medicine, 12(5), 1912. https://doi.org/10.3390/jcm12051912