
Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Natural In Vitro Maturation Cycle
2.3. Controlled Ovarian Stimulation (COS) IVF and Switching to IVM Cycle
2.4. Collection, Culture and Maturation of Oocytes
2.5. Embryo Morphology Assessment and ET
2.6. Luteal Phase Supplementation
2.7. Variables and Outcome Measures
2.8. Statistical Analysis
3. Results
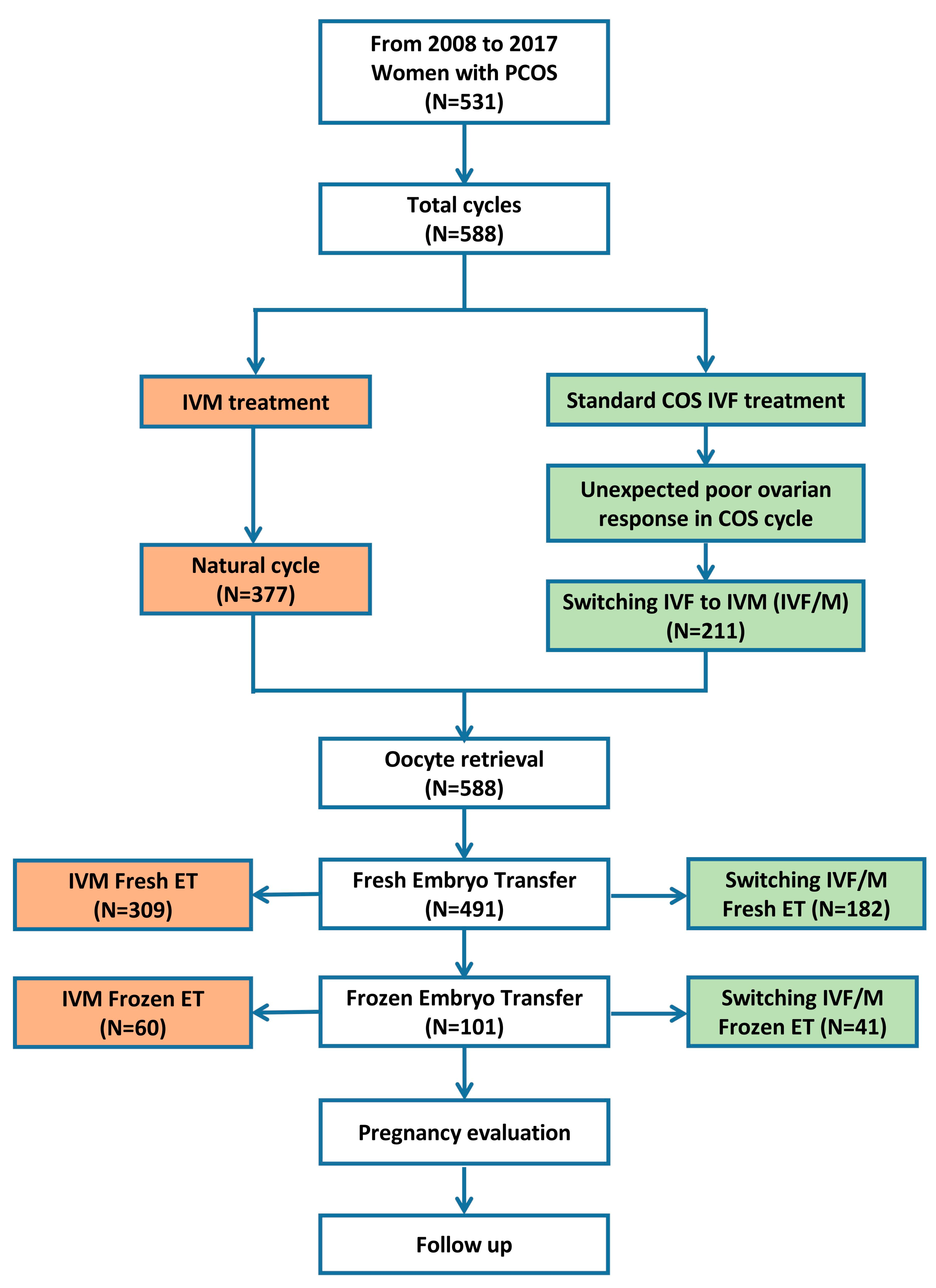
3.1. Participants
3.2. Demographic and Clinical Characteristics
3.3. Treatment and Laboratory Measures
3.4. Pregnancy and Neonatal Outcomes
3.5. Factors Associated with Live Birth after IVM
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Practice Committees of the American Society for Reproductive Medicine; the Society for Assisted Reproductive Technology. In vitro maturation: A committee opinion. Fertil. Steril. 2013, 99, 663–666. [Google Scholar] [CrossRef] [PubMed]
- Practice Committees of the American Society for Reproductive Medicine tSoRB, Technologists; the Society for Assisted Reproductive Technology. Electronic address jao. In vitro maturation: A committee opinion. Fertil. Steril. 2021, 115, 298–304. [Google Scholar] [CrossRef]
- Lin, Y.; Zheng, X.; Ma, C.; Li, X.; Zhang, X.; Yang, P.; Xu, J.; Zhu, J. Human Chorionic Gonadotropin Priming Does Not Improve Pregnancy Outcomes of PCOS-IVM Cycles. Front. Endocrinol. 2020, 11, 279. [Google Scholar] [CrossRef] [PubMed]
- De Vos, M.; Grynberg, M.; Ho, T.M.; Yuan, Y.; Albertini, D.F.; Gilchrist, R.B. Perspectives on the development and future of oocyte IVM in clinical practice. J. Assist. Reprod. Genet. 2021, 38, 1265–1280. [Google Scholar] [CrossRef] [PubMed]
- Gong, X.; Li, H.; Zhao, Y. The Improvement and Clinical Application of Human Oocyte In Vitro Maturation (IVM). Reprod. Sci. 2021, 29, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Sauerbrun-Cutler, M.T.; Vega, M.; Keltz, M.; McGovern, P.G. In vitro maturation and its role in clinical assisted reproductive technology. Obstet. Gynecol. Surv. 2015, 70, 45–57. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [Green Version]
- Vuong, L.N.; Braam, S.C.; Pham, T.D.; Mol, B.W.; Vuong, L.N. The effectiveness and safety of in vitro maturation of oocytes versus in vitro fertilization in women with a high antral follicle count. Hum. Reprod. 2019, 34, 1055–1064. [Google Scholar]
- Vuong, L.N.; Le, A.H.; Ho, V.N.A.; Pham, T.D.; Sanchez, F.; Romero, S.; De Vos, M.; Ho, T.M.; Gilchrist, R.B.; Smitz, J. Live births after oocyte in vitro maturation with a prematuration step in women with polycystic ovary syndrome. J. Assist. Reprod. Genet. 2020, 37, 347–357. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Guo, W.; Zeng, L.; Zheng, D.; Yang, S.; Wang, L.; Wang, R.; Mol, B.W.; Li, R.; Qiao, J. Live birth after in vitro maturation versus standard in vitro fertilisation for women with polycystic ovary syndrome: Protocol for a non-inferiority randomised clinical trial. BMJ Open 2020, 10, e035334. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Huang, C.; Zhang, T.; Gong, W.; Deng, X.; Liu, H.; Liu, J.; Guo, Y. The effects of statins on hyperandrogenism in women with polycystic ovary syndrome: A systematic review and meta-analysis of randomized controlled trials. Reprod. Biol. Endocrinol. 2021, 19, 189. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Zhang, Q.; Yang, D.; Li, S.; Lu, S.; Wu, X.; Wei, Z.; Song, X.; Wang, X.; Fu, S.; et al. Prevalence of polycystic ovary syndrome in women in China: A large community-based study. Hum. Reprod. 2013, 28, 2562–2569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Hu, W.H.; Wan, Q.; Li, T.; Qian, Y.; Chen, M.X.; Tang, X.J.; Feng, Q.; Meng, X.Q.; Adu-Gyamfi, E.A.; et al. Effect of artificial cycle with or without GnRH-a pretreatment on pregnancy and neonatal outcomes in women with PCOS after frozen embryo transfer: A propensity score matching study. Reprod. Biol. Endocrinol. 2022, 20, 56. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.K.; Maheshwari, A.; Felix, N.; Campbell, S.; Nargund, G. Mild versus conventional ovarian stimulation for IVF in poor, normal and hyper-responders: A systematic review and meta-analysis. Hum. Reprod. Update 2021, 27, 229–253. [Google Scholar] [CrossRef]
- Xu, B.; Zhou, M.; Cheng, M.; Zhang, D.; Wu, X.; Si, C.; Xia, L.; Xu, H.; Li, J.; Chang, H.M.; et al. Transvaginal ovarian drilling followed by controlled ovarian stimulation from the next day improves ovarian response for the poor responders with polycystic ovary syndrome during IVF treatment: A pilot study. Reprod. Biol. Endocrinol. 2020, 18, 7. [Google Scholar] [CrossRef]
- Conforti, A.; Esteves, S.C.; Cimadomo, D.; Vaiarelli, A.; Di Rella, F.; Ubaldi, F.M.; Zullo, F.; De Placido, G.; Alviggi, C. Management of Women With an Unexpected Low Ovarian Response to Gonadotropin. Front. Endocrinol. 2019, 10, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chian, R.C.; Buckett, W.M.; Abdul Jalil, A.K.; Son, W.Y.; Sylvestre, C.; Rao, D.; Tan, S.L. Natural-cycle in vitro fertilization combined with in vitro maturation of immature oocytes is a potential approach in infertility treatment. Fertil. Steril. 2004, 82, 1675–1678. [Google Scholar] [CrossRef]
- Zhao, F.; Lu, X.; Gong, C.; Xi, H.; Liu, X.; Zhao, J. The feasibility of switching from IVF to IVM combined with all-blastocyst-culture and transfer for patients with ovarian hyperstimulation syndrome tendency. Int. J. Gynaecol. Obstet. 2022, 159, 453–487. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar] [CrossRef]
- Alpha Scientists in Reproductive Medicine; ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum. Reprod 2011, 26, 1270–1283. [Google Scholar] [CrossRef] [Green Version]
- Gardner, D.K.; Schoolcraft, W.B. In vitro culture of human blastocyst. In Towards Reproductive Certainty: Infertility and Genetics Beyond 1999; Janson, R., Mortimer, D., Eds.; Parthenon Press: Carnforth, UK, 1999; pp. 378–388. [Google Scholar]
- Cela, V.; Obino, M.E.R.; Alberga, Y.; Pinelli, S.; Sergiampietri, C.; Casarosa, E.; Simi, G.; Papini, F.; Artini, P.G. Ovarian response to controlled ovarian stimulation in women with different polycystic ovary syndrome phenotypes. Gynecol. Endocrinol. 2018, 34, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Delbos, L.; Parot-Schinkel, E.; El Hachem, H.; Legendre, G.; Descamps, P.; Boucret, L.; Ferre-L’Hotellier, V.; Jeanneteau, P.; Dreux, C.; Moriniere, C.; et al. ConFIRM trial—Conversion of in vitro fertilization cycles to intrauterine inseminations in patients with a poor ovarian response to stimulation: A protocol for a multicentric, prospective randomized trial. Trials 2018, 19, 565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleming, R.; Seifer, D.B.; Frattarelli, J.L.; Ruman, J. Assessing ovarian response: Antral follicle count versus anti-Mullerian hormone. Reprod. Biomed. Online 2015, 31, 486–496. [Google Scholar] [CrossRef] [Green Version]
- Thakre, N.; Homburg, R. A review of IVF in PCOS patients at risk of ovarian hyperstimulation syndrome. Expert Rev. Endocrinol. Metab. 2019, 14, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Al-Shawaf, A.T.; Zosmer, S.; Hussain, A.; Tozer, N.; Panay, C.; Wilson, A.M.; Lower, J.G. Grudzinskas, Prevention of severe ovarian hyperstimulation syndrome in IVF with or without ICSI and embryo transfer: A modified coasting strategy based on ultrasound for identification of high-risk patients. Hum. Reprod 2001, 26, 24–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Z.; Chen, L.; Wu, H.; Zheng, D.; Li, R.; Mol, B.W.; Qiao, J. Assisted reproductive technology in Beijing, 2013–2015. Reprod. Biomed. Online 2018, 37, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.; Tarlatzis, B.; Nargund, G.; Gianaroli, L. Definition EwgoPOR. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamazou, F.; Fuchs, F.; Grynberg, M.; Gallot, V.; Herzog, E.; Fanchin, R.; Frydman, N.; Frydman, R. Cancellation of IVF-ET cycles: Poor prognosis, poor responder, or variability of the response to controlled ovarian hyperstimulation? An analysis of 142 cancellations. J. Gynecol. Obstet. Biol. Reprod. 2012, 41, 41–47. [Google Scholar] [CrossRef]
- Shohieb, A.; Mostafa, M.; El-Khayat, W. Conversion of ICSI cycles to IUI in poor responders to controlled ovarian hyperstimulation. Middle East Fertil. Soc. J. 2012, 17, 42–46. [Google Scholar] [CrossRef]
- Younis, J.S.; Ben-Ami, M.; Ben-Shlomo, I. The Bologna criteria for poor ovarian response: A contemporary critical appraisal. J. Ovarian Res. 2015, 8, 76. [Google Scholar] [CrossRef] [Green Version]
- Vuong, L.N.; Ho, V.N.A.; Ho, T.M.; Dang, V.Q.; Phung, T.H.; Giang, N.H.; Le, A.H.; Pham, T.D.; Wang, R.; Smitz, J.; et al. In-vitro maturation of oocytes versus conventional IVF in women with infertility and a high antral follicle count: A randomized non-inferiority controlled trial. Hum. Reprod. 2020, 35, 2537–2547. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Guo, W.; Zeng, L.; Zheng, D.; Yang, S.; Xu, Y.; Wang, L.; Wang, R.; Mol, B.W.; Li, R.; et al. In vitro maturation without gonadotropins versus in vitro fertilization with hyperstimulation in women with polycystic ovary syndrome: A non-inferiority randomized controlled trial. Hum. Reprod. 2022, 37, 242–253. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.Y.; Chian, R.C. Development of in vitro maturation techniques for clinical applications. Fertil. Steril. 2017, 108, 577–584. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| No. of Cycles | Percentages (%) | |
|---|---|---|
| Total numbers | 588 | 100.00 |
| Year | ||
| 2008 | 29 | 4.9 |
| 2009 | 76 | 12.9 |
| 2010 | 54 | 9.2 |
| 2011 | 84 | 14.3 |
| 2012 | 43 | 7.3 |
| 2013 | 72 | 12.2 |
| 2014 | 89 | 15.1 |
| 2015 | 52 | 8.8 |
| 2016 | 56 | 9.5 |
| 2017 | 33 | 5.6 |
| Type of infertility | ||
| Primary infertility | 151 | 25.7 |
| Secondary infertility | 437 | 74.3 |
| PCOS for single cause for infertility | 197 | 33.5 |
| PCOS combined causes for infertility | ||
| Male factors | 211 | 35.9 |
| Tubal disorder | 160 | 27.2 |
| Previous poor ovarian response | 16 | 2.7 |
| Endometriosis | 4 | 0.7 |
| Type of ART cycle | ||
| Natural cycle | 377 | 64.1 |
| Hyper-stimulation cycle | 198 | 33.7 |
| GnRH-a protocol | 128 | 64.6 |
| Short GnRH—a protocol | 22 | 17.2 |
| Long GnRH—a protocol | 78 | 60.9 |
| Super long GnRH-a protocol | 28 | 21.9 |
| GnRH-ant protocol | 70 | 35.4 |
| Mini-stimulation cycle | 13 | 2.2 |
| Total (n = 588) | Type of Cycle | p-Value | ||
|---|---|---|---|---|
| IVF/M Cycle (n = 211) | IVM Cycle (n = 377) | |||
| Age | ||||
| Mean (SD)—years | 30.1 (3.9) | 29.6 (3.8) | 30.4 (3.9) | 0.01 |
| Distribution—no. (%) | ||||
| <35 years | 503 (85.5) | 185 (87.7) | 318 (84.4) | 0.27 |
| ≥35 years | 85 (14.5) | 26 (12.3) | 59 (15.6) | |
| BMI a (median, IQR)—kg/m2 | 25.3 (22.4–28.4) | 26.2 (23.1–28.9) | 24.8 (22.3–28.2) | 0.01 |
| Fertility history | ||||
| Duration of attempt to conceive (median, IQR)—year | 4.0 (2.0–6.0) | 4.0 (2.0–6.0) | 4.0 (3.0–6.0) | 0.15 |
| Previous conception—no. (%) | 151 (25.7) | 53 (25.1) | 98 (26.0) | 0.45 |
| Indications for IVF—no. (%) | ||||
| Male factors | 211 (35.9) | 91 (43.1) | 120 (31.8) | 0.01 |
| Tubal disorder | 160 (27.2) | 68 (32.2) | 92 (24.4) | 0.04 |
| Previous poor ovarian response | 16 (2.7) | 4 (1.9) | 12 (3.2) | 0.36 |
| Endometriosis | 4 (0.7) | 0 (0.0) | 4 (1.1) | 0.13 |
| Number of IVF attempt | ||||
| Median (IQR) | 1.0 (1.0–2.0) | 1.0 (1.0–1.0) | 1.0 (1.0–2.0) | 0.99 |
| Distribution-no. (%) | ||||
| 1 | 423 (71.9) | 177 (83.9) | 246 (65.3) | <0.01 |
| 2 | 94 (16.0) | 21 (10.0) | 73 (19.4) | |
| 3 | 35 (6.0) | 8 (3.8) | 27 (7.2) | |
| 4 | 21 (3.6) | 3 (1.4) | 18 (4.8) | |
| ≥5 | 15 (2.5) | 2 (1.0) | 13 (3.5) | |
| Ultrasonographic findings | ||||
| AFC in both ovaries—no. (%) | ||||
| <12 | 84 (16.5) | 52 (25.1) | 32 (10.6) | <0.01 |
| 12–20 | 375 (73.5) | 144 (69.6) | 231 (76.2) | |
| >20 | 51 (10.0) | 11 (5.3) | 40 (13.2) | |
| Endometrial thickness b (Mean, SD)—mm | 8.2 (1.7) | 8.9 (1.7) | 7.7 (1.6) | <0.01 |
| Laboratory tests | ||||
| FSH c (median, IQR)—mIU/mL | 5.8 (4.8–7.0) | 5.9 (4.9–7.3) | 5.6 (4.6–6.8) | 0.67 |
| LH d (median, IQR)—mIU/mL | 7.0 (4.2–10.7) | 6.7 (3.5–10.3) | 7.1 (4.4–11.0) | 0.76 |
| Ratio of LH to FSH e (median, IQR) | 1.2 (0.7–1.8) | 1.1 (0.6–1.7) | 1.3 (0.7–1.9) | 0.07 |
| Estradiol f (median, IQR)—pmol/L | 168.5 (122.0–220.0) | 154.0 (119.5–218.5) | 171.0 (124.0–221.0) | 0.48 |
| Androgen g (median, IQR)—pmol/liter | 11.8 (8.1–17.2) | 11.2 (7.8–15.8) | 12.1 (8.1–18.9) | 0.27 |
| Total (n = 588) | Type of Cycle | p-Value | ||
|---|---|---|---|---|
| IVF/M Cycle (n = 211) | IVM Cycle (n = 377) | |||
| Duration of follicular phase a (median, IQR)—days | 0.0 (0.0–7.0) | 9.0 (6.0–12.0) | 0.0 (0.0–0.0) | <0.01 |
| Total gonadotropin dose b (median, IQR)—IU | 0.0 (0.0–900.0) | 1200.0 (750.0–1950.0) | 0.0 (0.0–0.0) | <0.01 |
| Estradiol level on hCG trigger day c (median, IQR)—pmol/L | 374.0 (190.0–852.5) | 749.0 (355.0–2061.8) | 220.0 (164.0–418.0) | <0.01 |
| Progesterone level on hCG trigger day d (median, IQR)—nmol/L | 0.9 (0.6–1.4) | 0.9 (0.6–1.4) | 0.9 (0.6–1.4) | 0.62 |
| LH level on hCG trigger day e (median, IQR)—mIU/mL | 5.5 (1.3–9.4) | 1.3 (0.4–3.6) | 8.4 (5.9–13.0) | <0.01 |
| No. of oocytes retrieved f | ||||
| Total number | 8779 | 2786 | 5993 | <0.01 |
| Median (IQR) | 13.0 (8.0–20.0) | 12.0 (7.0–17.0) | 13.5 (8.0–21.0) | |
| Method of fertilization—no. (%) | ||||
| Conventional IVF | 11 (1.9) | 8 (3.8) | 3 (0.8) | 0.01 |
| ICSI | 570 (96.9) | 198 (93.8) | 372 (98.7) | |
| Half-ICSI | 7 (1.2) | 5 (2.4) | 2 (0.5) | |
| No. of mature oocytes | ||||
| Total number | 4184 | 1573 | 2611 | 0.40 |
| Median (IQR) | 6.0 (4.0–10.0) | 6.0 (4.0–10.0) | 6.0 (4.0–10.0) | |
| No. of 2 pronuclear zygotes | ||||
| Total number | 2580 | 957 | 1623 | 0.45 |
| Median (IQR) | 4.0 (2.0–6.0) | 4.0 (2.0–6.0) | 3.0 (1.0–6.0) | |
| No. of available embryos | ||||
| Total number | 1515 | 522 | 993 | 0.46 |
| Median (IQR) | 2.0 (1.0–3.0) | 2.0 (2.0–3.0) | 2.0 (1.0–3.0) | |
| No. of good quality embryos | ||||
| Total number | 1241 | 432 | 809 | 0.64 |
| Median (IQR) | 2.0 (0.0–3.0) | 2.0 (0.0–3.0) | 2.0 (0.0–3.0) | |
| Patients undergoing the first fresh embryo transfer—no. (%) | ||||
| Day 3 | 485 (98.8%) | 179 (98.4%) | 306 (99.0%) | 0.5 |
| Day 5 | 6 (1.2%) | 3 (1.6%) | 3(0.1%) | |
| No. of embryo transferred (the first Fresh ET cycle) | ||||
| Total number | 975 | 356 | 619 | |
| Mean (SD) | 1.7 (0.9) | 1.7 (0.8) | 1.6 (0.9) | 0.53 |
| Distribution—no. (%) | ||||
| 1 | 71 (12.1) | 24 (11.4) | 47 (12.5) | 0.06 |
| 2 | 356 (60.5) | 142 (67.3) | 214 (56.8) | |
| 3 | 64 (10.9) | 16 (7.6) | 48 (12.7) | |
| No. of embryo transferred (the cumulative ET after one complete cycle) | ||||
| Total number | 1167 | 432 | 735 | |
| Mean (SD) | 2.0 (0.5) | 2.0 (0.6) | 1.9 (0.3) | 0.73 |
| Distribution—no. (%) | ||||
| 1 | 94 (16.0) | 36 (17.1) | 58 (15.4) | 0.188 |
| 2 | 411 (70.0) | 163 (77.3) | 249 (66.0) | |
| 3 | 83 (14.1) | 24 (11.4) | 59 (15.7) | |
| Total (n = 588) | Type of Cycle | p-Value | ||
|---|---|---|---|---|
| IVF/M Cycle (n = 211) | IVM Cycle (n = 377) | |||
| Number of transferred cycles—(the first fresh ET cycle) | 491 | 182 | 309 | |
| Number of embryos transferred | 975 | 356 | 619 | |
| Positive β-hCG—no./total no. (%) | 198/491 (40.3) | 63/182 (34.6) | 135/309 (43.7) | 0.05 |
| Clinical pregnancy-no./total no. (%) | 161/491 (32.8) | 48/182 (26.4) | 113/309 (36.6) | 0.02 |
| Ectopic pregnancy | 7/161 (4.3) | 3/48 (6.3) | 4/113 (3.5) | 0.44 |
| Uterine pregnancy | 154/161 (95.7) | 45/48 (93.8) | 109/113 (96.5) | 0.14 |
| Number of ET embryos | 0.49 | |||
| 1 | 37/154 (24.0) | 12/45 (26.7) | 25/109 (22.9) | |
| 2 | 114/154 (74.0) | 33/45 (73.3) | 81/109 (74.3) | |
| 3 | 3/154 (1.9) | 0/45 (0.0) | 3/109 (2.8) | |
| Implantation (per embryo)—no./total no. (%) | 161/975 (16.5) | 48/356 (13.5) | 113/619 (18.3) | 0.05 |
| Pregnancy loss—no/total no. (%) | ||||
| Among biochemical pregnancy | 37/198 (18.7) | 15/63 (23.8) | 22/135 (16.3) | 0.21 |
| Among clinical pregnancy | 48/161 (29.8) | 14/48 (29.2) | 34/113 (30.1) | 0.91 |
| First trimester | 37/161 (23.0) | 11/48 (22.9) | 26/113 (23.0) | |
| Second trimester | 11/161 (6.8) | 3/48 (6.3) | 8/113 (7.1) | |
| Live birth rate(after 28 weeks gestation)-no./total no. (%) | 105/491 (21.4) | 30/182 (16.4) | 75/309 (24.3) | 0.04 |
| Number of transferred cycles—(the cumulative ET after one complete cycle) | 592 | 223 | 369 | |
| Number of embryos transferred | 1167 | 432 | 735 | |
| Positive β-hCG—no./total no. (%) | 231/592 (39.0) | 73/223 (32.7) | 158/369 (42.8) | 0.01 |
| Clinical pregnancy-no./total no. (%) | 191/592 (32.3) | 58/223 (26.0) | 133/369 (36.0) | 0.01 |
| Ectopic pregnancy | 8/191 (4.2) | 3/58 (5.2) | 5/133 (3.8) | 0.65 |
| Uterine pregnancy | 185/191 (96.9) | 55/58 (94.8) | 130/133 (97.7) | 0.29 |
| Number of ET embryos | ||||
| 1 | 51/185 (27.6) | 14/55 (25.5) | 37/130 (28.5) | 0.89 |
| 2 | 126/185 (79.7) | 39/55 (70.9) | 87/130 (66.9) | |
| 3 | 8/185 (4.3) | 2/55 (3.6) | 6/130 (4.6) | |
| Implantation (per embryo)—no./total no. (%) | 191/1167(16.4) | 58/ 432(13.4) | 133/735 (18.1) | 0.03 |
| Pregnancy loss—no/total no. (%) | ||||
| Among biochemical pregnancy | 40/231 (17.3) | 15/73 (20.5) | 25/158 (15.8) | 0.38 |
| Among clinical pregnancy | 59/191 (30.9) | 16/58 (27.6) | 43/133 (32.3) | 0.51 |
| First trimester | 47/191 (24.6) | 13/58 (22.4) | 34/133 (25.6) | |
| Second trimester | 12/191 (6.3) | 3/58 (5.2) | 9/133 (6.9) | |
| Live birth rate (after 28 weeks of gestation)-no./total no. (%) | 125/592 (21.1) | 38/223 (17.4) | 87/369 (23.6) | 0.05 |
| Pregnancy complication-no./total no. (%) | ||||
| Hypertensive disorders | 3/185 (1.62) | 0/55 (0.0) | 3/130 (2.31) | 0.26 |
| Premature rupture of membranes | 2/85 (2.35) | 0/55 (0.0) | 2/130 (1.54) | 0.36 |
| Gestational diabetes mellitus | 1/185 (0.54) | 0/55 (0.0) | 1/130 (0.77) | 0.51 |
| Anemia | 1/185 (0.54) | 0/55 (0.0) | 1/130 (0.77) | 0.51 |
| Intrauterine infection | 1/185 (0.54) | 1/55 (1.82) | 0/130 (0.0) | 0.12 |
| Delivery a—no./total no. (%) | 115/582 (19.8) | 35/220(15.9) | 80/362 (22.1) | 0.07 |
| Number of neonates b | 125 | 38 | 87 | |
| Live birth | 124/125 (99.0) | 37/38 (97.4) | 87/87 (100.0) | 0.13 |
| Singleton | 102/124 (98.1) | 31/37 (83.8) | 69/87 (79.3) | 0.56 |
| Twin | 22/124 (17.7) | 6/37 (16.2) | 18/87 (20.7) | 0.56 |
| Stillbirth | 1/125 (1.0) | 1/38 (2.6) | 0/87 (0.0) | 0.19 |
| Sex | ||||
| Male | 65/125 (52.0) | 20/38 (52.6) | 45/87 (51.7) | 0.92 |
| Female | 60/125 (48.0) | 18/38 (47.4) | 42/87 (48.3) | |
| Gestational age on delivery (weeks) | ||||
| Medianc (IQR)—weeks | 38.0 (37.0–39.0) | 38.0 (35.8–39.0) | 38.0 (37.0–39.0) | 0.99 |
| Distribution-no./total no. (%) c | ||||
| Preterm labor (28–36 + 6 weeks) | 21/111(18.9) | 5/35 (14.3) | 16/76 (21.1) | 0.39 |
| Term labor (≥37 weeks) | 90/111 (81.1) | 30/35 (85.7) | 60/76 (78.9) | 0.40 |
| Mode of delivery-no./total no. (%) | ||||
| Cesarean section | 89/114 (78.1) | 26/34 (76.5) | 63/80 (78.8) | 0.78 |
| Natural delivery | 25/114 (21.9) | 8/34 (23.5) | 17/80 (21.2) | 0.57 |
| Advanced neonatal outcome-no./total no. (%) | ||||
| Birth defect | 3/185 (1.6) | 0/55 (0.0) | 3/130 (2.3) | 0.26 |
| Neonatal asphyxia | 0/185 (0.0) | 0/55 (0.0) | 0/130 (0.0) | |
| Neonatal death | 0/185 (0.0) | 0/55 (0.0) | 0/130 (0.0) | |
| Birth weight—g | ||||
| Singleton d | 3155.6 (723.0) | 3089.6 (800.5) | 3242.2 (688.3) | 0.78 |
| Twin | 2707.3 (521.2) | 2701.3 (534.9) | 3112.3 (593.1) | 0.81 |
| Live Birth (N = 104) | No Live Birth (N = 377) | Unadjusted Model | Adjusted Model A | |||
|---|---|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |||
| Age—year | 30.4 (3.7) | 29.8 (3.8) | 1.04 (0.98–1.10) | 0.23 | - | - |
| BMI a—kg/m2 | 25.3 (4.1) | 25.8 (4.2) | 0.97 (0.92–1.03) | 0.28 | - | - |
| Duration of attempt to conceive—year | 4.6 (2.8) | 4.6 (2.9) | 1.00 (0.93–1.08) | 0.98 | - | - |
| Previous conception—no. (%) | 28 (29.5) | 99 (25.0) | - | - | ||
| Indications for PCOS IVF—no. (%) | - | - | ||||
| Tubal disorder | 27 (28.4) | 106 (26.8) | 0.92 (0.56–1.52) | 0.75 | - | - |
| POR | 0 (0.0) | 9 (2.3) | - | - | - | - |
| Male factors | 35 (36.8) | 141 (35.6) | 0.95 (0.50–1.51) | 0.82 | - | - |
| Endometriosis | 0 (0.0) | 2 (0.5) | - | - | - | - |
| Type of stimulation protocol—no. (%) | - | - | ||||
| IVM | 68 (71.6) | 241 (60.9) | 0.62 (0.38–1.01) | 0.05 | - | - |
| IVF/M | 27 (28.4) | 155 (39.1) | Ref | ref | - | - |
| Number of IVF attempt | 1.4 (0.7) | 1.5 (1.1) | 0.90 (0.71–1.15) | 0.41 | - | - |
| AFC in both ovaries | 30.0 (11.5) | 29.4 (12.5) | 1.00 (0.98–1.02) | 0.89 | - | - |
| Endometrial thickness b—mm | 8.2 (1.8) | 8.3 (1.6) | 0.98 (0.85–1.13) | 0.73 | - | - |
| FSH c—mIU/mL | 6.2 (2.3) | 6.7 (7.8) | 0.99 (0.95–1.03) | 0.60 | - | - |
| LH d—mIU/mL | 8.4 (5.0) | 8.2 (6.3) | 1.01 (0.97–1.04) | 0.77 | - | - |
| Estradiol e—pmol/L | 171.5 (75.8) | 181.6 (121.4) | 1.00 (0.99–1.00) | 0.45 | - | - |
| Androgen f—pmol/liter | 14.4 (14.5) | 13.3 (7.0) | 1.00 (0.99–1.04) | 0.37 | 1.02 (0.99–1.05) | 0.24 |
| Duration of follicular phase g—days | 2.6 (4.7) | 3.6 (5.2) | 0.96 (0.92–1.01) | 0.12 | 0.94 (0.88–1.01) | 0.07 |
| Total gonadotropin dose h (SD)—IU | 389.8 (775.4) | 538.1 (875.9) | 1.00 (0.99–1.00) | 0.14 | - | - |
| Estradiol level on hCG trigger day i (SD)—pmol/L | 948.9 (2077.7) | 1406.9 (3438.5) | 1.00 (1.00–1.00) | 0.29 | - | - |
| Progesterone level on hCG trigger day j (SD)—nmol/L | 1.1 (0.7) | 1.2 (1.0) | 0.91 (0.67–1.23) | 0.54 | - | - |
| LH level on hCG trigger day k—mIU/mL | 11.2 (24.4) | 7/0 (12.4) | 1.01 (1.00–1.03) | 0.90 | - | - |
| Number of oocytes retrieved l (SD) | 16.3 (10.0) | 16.1 (10.5) | 1.00 (0.98–1.02) | 0.89 | 0.96 (0.92–1.00) | 0.05 |
| Number of embryos transferred-no./total no. (%) | ||||||
| 1 | 2 (2.1) | 69 (17.4) | ref | ref | ref | ref |
| 2 | 76 (80.0) | 280 (70.7) | 0.08 (0.02–0.36) | <0.01 | 0.07 (0.01–0.59) | 0.02 |
| 3 | 17 (17.9) | 47 (11.9) | 0.75 (0.41–1.38) | 0.36 | 0.60 (0.24–1.49) | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, W.; Zheng, X.; Zheng, D.; Yang, Z.; Yang, S.; Yang, R.; Li, R.; Qiao, J. Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients. J. Clin. Med. 2023, 12, 1978. https://doi.org/10.3390/jcm12051978
Guo W, Zheng X, Zheng D, Yang Z, Yang S, Yang R, Li R, Qiao J. Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients. Journal of Clinical Medicine. 2023; 12(5):1978. https://doi.org/10.3390/jcm12051978
Chicago/Turabian StyleGuo, Wei, Xiaoying Zheng, Danni Zheng, Zi Yang, Shuo Yang, Rui Yang, Rong Li, and Jie Qiao. 2023. "Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients" Journal of Clinical Medicine 12, no. 5: 1978. https://doi.org/10.3390/jcm12051978
APA StyleGuo, W., Zheng, X., Zheng, D., Yang, Z., Yang, S., Yang, R., Li, R., & Qiao, J. (2023). Effectiveness, Flexibility and Safety of Switching IVF to IVM as a Rescue Strategy in Unexpected Poor Ovarian Response for PCOS Infertility Patients. Journal of Clinical Medicine, 12(5), 1978. https://doi.org/10.3390/jcm12051978