
Sleep Quality Disturbances Are Associated with White Matter Alterations in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury

 , , , , , , , , add
Show full author list
, , , , , , , , add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Diagnostic and Clinical Assessment
2.2.1. Assessment of PTSD
2.2.2. Assessment of mTBI
2.2.3. Assessment of Sleep Quality
2.2.4. Assessment of Comorbid Psychiatric Disorders
2.2.5. Assessment of Warzone-Related Stress
2.3. Magnetic Resonance Imaging
2.3.1. Image Acquisition
2.3.2. Image Pre-Processing
2.3.3. WM Fiber Clustering
2.3.4. Diffusion Parameter Extraction
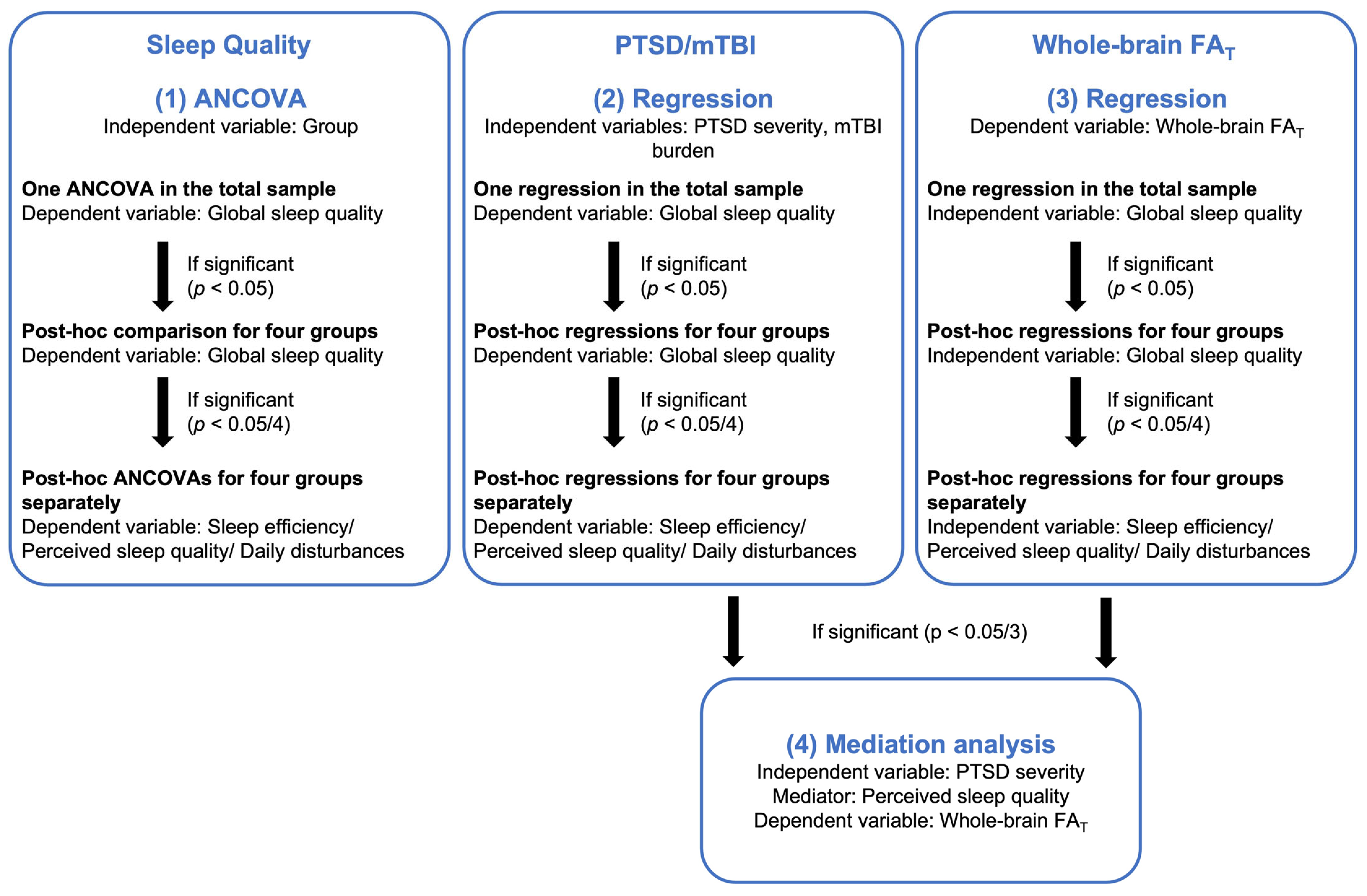
2.4. Statistical Analysis
2.4.1. Group Differences in Sleep Quality
2.4.2. PTSD, mTBI, and Sleep Quality
2.4.3. Sleep Quality and WM Microstructure
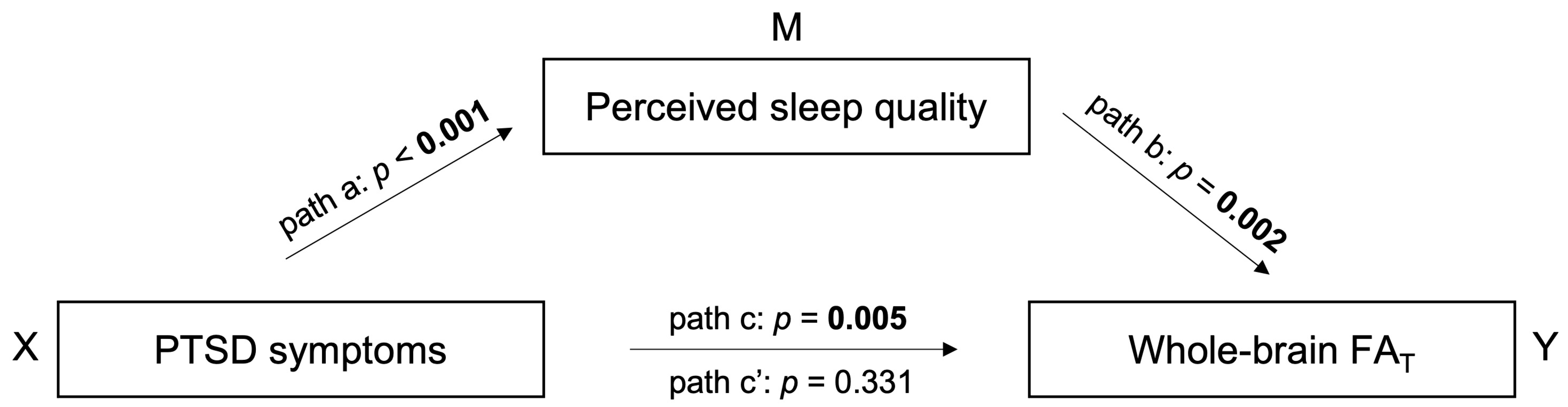
2.4.4. Sleep Quality as a Mediator between PTSD Symptom Severity and WM Microstructure
3. Results
3.1. Group Differences in Sleep Quality
3.2. PTSD, mTBI, and Sleep Quality
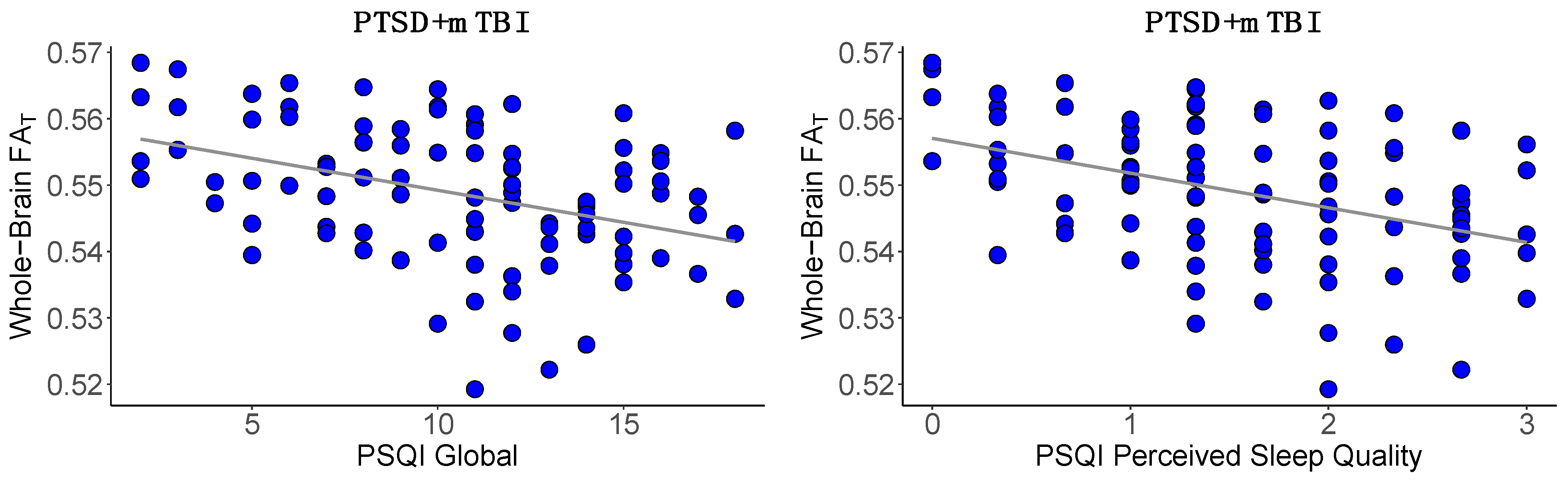
3.3. Sleep Quality and WM Microstructure
3.4. Sleep Quality Mediates the Association between PTSD Symptom Severity and WM Microstructure
4. Discussion
4.1. Group Differences in Sleep Quality
4.2. PTSD, mTBI, and Sleep Quality
4.3. Sleep Quality and WM Microstructure
4.4. Sleep Quality Mediates the Association between PTSD Symptom Severity and WM Microstructure
4.5. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fulton, J.J.; Calhoun, P.S.; Wagner, H.R.; Schry, A.R.; Hair, L.P.; Feeling, N.; Elbogen, E.; Beckham, J.C. The Prevalence of Posttraumatic Stress Disorder in Operation Enduring Freedom/Operation Iraqi FreDevelopment of a Clinician-Administered edom (OEF/OIF) Veterans: A Meta-Analysis. J. Anxiety Disord. 2015, 31, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, R.B.; Post, E.P.; Sun, H.; Pomerantz, A.; Saxon, A.J.; Piette, J.D.; Maynard, C.; Arnow, B.; Curtis, I.; Fihn, S.D.; et al. Prevalence, Comorbidity, and Prognosis of Mental Health among US Veterans. Am. J. Public Health 2015, 105, 2564–2569. [Google Scholar] [CrossRef] [PubMed]
- Schneiderman, A.I.; Braver, E.R.; Kang, H.K. Understanding Sequelae of Injury Mechanisms and Mild Traumatic Brain Injury Incurred during the Conflicts in Iraq and Afghanistan: Persistent Postconcussive Symptoms and Posttraumatic Stress Disorder. Am. J. Epidemiol. 2008, 167, 1446–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindquist, L.K.; Love, H.C.; Elbogen, E.B. Traumatic Brain Injury in Iraq and Afghanistan Veterans: New Results from a National Random Sample Study. J. Neuropsychiatry Clin. Neurosci. 2017, 29, 254–259. [Google Scholar] [CrossRef]
- Combs, H.L.; Berry, D.T.R.; Pape, T.; Babcock-Parziale, J.; Smith, B.; Schleenbaker, R.; Shandera-Ochsner, A.; Harp, J.P.; High, W.M. The Effects of Mild Traumatic Brain Injury, Post-Traumatic Stress Disorder, and Combined Mild Traumatic Brain Injury/Post-Traumatic Stress Disorder on Returning Veterans. J. Neurotrauma 2015, 32, 956–966. [Google Scholar] [CrossRef] [Green Version]
- Vasterling, J.J.; Aslan, M.; Lee, L.O.; Proctor, S.P.; Ko, J.; Jacob, S.; Concato, J. Longitudinal Associations among Posttraumatic Stress Disorder Symptoms, Traumatic Brain Injury, and Neurocognitive Functioning in Army Soldiers Deployed to the Iraq War. J. Int. Neuropsychol. Soc. 2018, 24, 311–323. [Google Scholar] [CrossRef]
- Lagarde, E.; Salmi, L.-R.; Holm, L.W.; Contrand, B.; Masson, F.; Ribéreau-Gayon, R.; Laborey, M.; Cassidy, J.D. Association of Symptoms Following Mild Traumatic Brain Injury with Posttraumatic Stress Disorder vs. Postconcussion Syndrome. JAMA Psychiatry 2014, 71, 1032–1040. [Google Scholar] [CrossRef] [Green Version]
- Seelig, A.D.; Jacobson, I.G.; Smith, B.; Hooper, T.I.; Boyko, E.J.; Gackstetter, G.D.; Gehrman, P.; Macera, C.A.; Smith, T.C. Sleep Patterns before, during, and after Deployment to Iraq and Afghanistan. Sleep 2010, 33, 1615–1622. [Google Scholar] [CrossRef] [Green Version]
- Germain, A. Sleep Disturbances as the Hallmark of PTSD: Where Are We Now? Am. J. Psychiatry 2013, 170, 372–382. [Google Scholar] [CrossRef]
- Khazaie, H. Sleep Disturbances in Veterans with Chronic War-Induced PTSD. J. Inj. Violence Res. 2016, 8, 99–107. [Google Scholar] [CrossRef]
- Grima, N.; Ponsford, J.; Rajaratnam, S.M.; Mansfield, D.; Pase, M.P. Sleep Disturbances in Traumatic Brain Injury: A Meta-Analysis. J. Clin. Sleep Med. 2016, 12, 419–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathias, J.L.; Alvaro, P.K. Prevalence of Sleep Disturbances, Disorders, and Problems Following Traumatic Brain Injury: A Meta-Analysis. Sleep Med. 2012, 13, 898–905. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, K.S.; Kark, S.M.; Gehrman, P.; Bogdanova, Y. Sleep Disturbances, TBI and PTSD: Implications for Treatment and Recovery. Clin. Psychol. Rev. 2015, 40, 195–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maher, M.J.; Rego, S.A.; Asnis, G.M. Sleep Disturbances in Patients with Post-Traumatic Stress Disorder: Epidemiology, Impact and Approaches to Management. CNS Drugs 2006, 20, 567–590. [Google Scholar] [CrossRef]
- Lavie, P.; Hefez, A.; Halperin, G.; Enoch, D. Long-Term Effects of Traumatic War-Related Events on Sleep. Am. J. Psychiatry 1979, 136, 175–178. [Google Scholar] [CrossRef]
- McCarthy, E.; DeViva, J.C.; Norman, S.B.; Southwick, S.M.; Pietrzak, R.H. Self-Assessed Sleep Quality Partially Mediates the Relationship between PTSD Symptoms and Functioning and Quality of Life in U.S. Veterans: Results from the National Health and Resilience in Veterans Study. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 869–876. [Google Scholar] [CrossRef]
- Colvonen, P.J.; Ellison, J.; Haller, M.; Norman, S.B. Examining Insomnia and PTSD over Time in Veterans in Residential Treatment for Substance Use Disorders and PTSD. Behav. Sleep Med. 2019, 17, 524–535. [Google Scholar] [CrossRef]
- Spoormaker, V.I.; Montgomery, P. Disturbed Sleep in Post-Traumatic Stress Disorder: Secondary Symptom or Core Feature? Sleep Med. Rev. 2008, 12, 169–184. [Google Scholar] [CrossRef]
- Eugene, A.R.; Masiak, J. The Neuroprotective Aspects of Sleep. MEDtube Sci. 2015, 3, 35–40. [Google Scholar]
- De Vivo, L.; Bellesi, M. The Role of Sleep and Wakefulness in Myelin Plasticity. Glia 2019, 67, 2142–2152. [Google Scholar] [CrossRef] [Green Version]
- Babu Henry Samuel, I.; Pollin, K.U.; Breneman, C.B. Lower Cortical Volume Is Associated with Poor Sleep Quality after Traumatic Brain Injury. Brain Imaging Behav. 2022, 16, 1362–1371. [Google Scholar] [CrossRef] [PubMed]
- Chao, L.L.; Mohlenhoff, B.S.; Weiner, M.W.; Neylan, T.C. Associations between Subjective Sleep Quality and Brain Volume in Gulf War Veterans. Sleep 2014, 37, 445–452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Cornelissen-Guillaume, G.G.; He, J.; Kastin, A.J.; Harrison, L.M.; Pan, W. Circadian Rhythm of Autophagy Proteins in Hippocampus Is Blunted by Sleep Fragmentation. Chronobiol. Int. 2016, 33, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C.; Gillin, J.C.; Buchsbaum, M.S.; Hershey, T.; Hazlett, E.; Sicotte, N.; Bunney, W.E. The Effect of Sleep Deprivation on Cerebral Glucose Metabolic Rate in Normal Humans Assessed with Positron Emission Tomography. Sleep 1991, 14, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Shenton, M.E.; Hamoda, H.M.; Schneiderman, J.S.; Bouix, S.; Pasternak, O.; Rathi, Y.; Vu, M.-A.; Purohit, M.P.; Helmer, K.; Koerte, I.; et al. A Review of Magnetic Resonance Imaging and Diffusion Tensor Imaging Findings in Mild Traumatic Brain Injury. Brain Imaging Behav. 2012, 6, 137–192. [Google Scholar] [CrossRef]
- Schuff, N.; Zhang, Y.; Zhan, W.; Lenoci, M.; Ching, C.; Boreta, L.; Mueller, S.G.; Wang, Z.; Marmar, C.R.; Weiner, M.W.; et al. Patterns of Altered Cortical Perfusion and Diminished Subcortical Integrity in Posttraumatic Stress Disorder: An MRI Study. Neuroimage 2011, 54, S62–S68. [Google Scholar] [CrossRef] [Green Version]
- Aschbacher, K.; Mellon, S.H.; Wolkowitz, O.M.; Henn-Haase, C.; Yehuda, R.; Flory, J.D.; Bierer, L.M.; Abu-Amara, D.; Marmar, C.R.; Mueller, S.G. Posttraumatic Stress Disorder, Symptoms, and White Matter Abnormalities among Combat-Exposed Veterans. Brain Imaging Behav. 2018, 12, 989–999. [Google Scholar] [CrossRef]
- Ju, Y.; Ou, W.; Su, J.; Averill, C.L.; Liu, J.; Wang, M.; Wang, Z.; Zhang, Y.; Liu, B.; Li, L.; et al. White Matter Microstructural Alterations in Posttraumatic Stress Disorder: An ROI and Whole-Brain Based Meta-Analysis. J. Affect. Disord. 2020, 266, 655–670. [Google Scholar] [CrossRef]
- O’Doherty, D.C.M.; Ryder, W.; Paquola, C.; Tickell, A.; Chan, C.; Hermens, D.F.; Bennett, M.R.; Lagopoulos, J. White Matter Integrity Alterations in Post-Traumatic Stress Disorder. Hum. Brain Mapp. 2018, 39, 1327–1338. [Google Scholar] [CrossRef]
- Siehl, S.; King, J.A.; Burgess, N.; Flor, H.; Nees, F. Structural White Matter Changes in Adults and Children with Posttraumatic Stress Disorder: A Systematic Review and Meta-Analysis. NeuroImage Clin. 2018, 19, 581–598. [Google Scholar] [CrossRef]
- Graziano, R.; Bruce, S.; Paul, R. The Corpus Callosum and PTSD Severity. J. Interpers. Violence 2021, 36, 7480–7494. [Google Scholar] [CrossRef]
- Olson, E.A.; Cui, J.; Fukunaga, R.; Nickerson, L.D.; Rauch, S.L.; Rosso, I.M. Disruption of White Matter Structural Integrity and Connectivity in Posttraumatic Stress Disorder: A TBSS and Tractography Study. Depress. Anxiety 2017, 34, 437–445. [Google Scholar] [CrossRef] [Green Version]
- Averill, C.L.; Averill, L.A.; Wrocklage, K.M.; Scott, J.C.; Akiki, T.J.; Schweinsburg, B.; Southwick, S.M.; Krystal, J.H.; Abdallah, C.G. Altered White Matter Diffusivity of the Cingulum Angular Bundle in Posttraumatic Stress Disorder. Complex Psychiatry 2018, 4, 75–82. [Google Scholar] [CrossRef]
- Koch, S.B.J.; Van Zuiden, M.; Nawijn, L.; Frijling, J.L.; Veltman, D.J.; Olff, M. Decreased Uncinate Fasciculus Tract Integrity in Male and Female Patients with PTSD: A Diffusion Tensor Imaging Study. J. Psychiatry Neurosci. 2017, 42, 331–342. [Google Scholar] [CrossRef] [Green Version]
- McCunn, P.; Richardson, J.D.; Jetly, R.; Dunkley, B. Diffusion Tensor Imaging Reveals White Matter Differences in Military Personnel Exposed to Trauma with and without Post-Traumatic Stress Disorder. Psychiatry Res. 2021, 298, 113797. [Google Scholar] [CrossRef]
- Dennis, E.L.; Disner, S.G.; Fani, N.; Salminen, L.E.; Logue, M.; Clarke, E.K.; Haswell, C.C.; Averill, C.L.; Baugh, L.A.; Bomyea, J.; et al. Altered White Matter Microstructural Organization in Posttraumatic Stress Disorder across 3047 Adults: Results from the PGC-ENIGMA PTSD Consortium. Mol. Psychiatry 2021, 26, 4315–4330. [Google Scholar] [CrossRef]
- Bierer, L.M.; Ivanov, I.; Carpenter, D.M.; Wong, E.W.; Golier, J.A.; Tang, C.Y.; Yehuda, R. White Matter Abnormalities in Gulf War Veterans with Posttraumatic Stress Disorder: A Pilot Study. Psychoneuroendocrinology 2015, 51, 567–576. [Google Scholar] [CrossRef]
- Sanjuan, P.M.; Thoma, R.; Claus, E.D.; Mays, N.; Caprihan, A. Reduced White Matter Integrity in the Cingulum and Anterior Corona Radiata in Posttraumatic Stress Disorder in Male Combat Veterans: A Diffusion Tensor Imaging Study. Psychiatry Res. Neuroimaging 2013, 214, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Kennis, M.; van Rooij, S.J.H.; Tromp, D.P.M.; Fox, A.S.; Rademaker, A.R.; Kahn, R.S.; Kalin, N.H.; Geuze, E. Treatment Outcome-Related White Matter Differences in Veterans with Posttraumatic Stress Disorder. Neuropsychopharmacology 2015, 40, 2434–2442. [Google Scholar] [CrossRef] [Green Version]
- Hedges, D.W.; Thatcher, G.W.; Bennett, P.J.; Sood, S.; Paulson, D.; Creem-Regehr, S.; Brown, B.L.; Allen, S.; Johnson, J.; Froelich, B.; et al. Brain Integrity and Cerebral Atrophy in Vietnam Combat Veterans with and without Posttraumatic Stress Disorder. Neurocase 2007, 13, 402–410. [Google Scholar] [CrossRef]
- Daniels, J.K.; Lamke, J.P.; Gaebler, M.; Walter, H.; Scheel, M. White Matter Integrity and Its Relationship to PTSD and Childhood Trauma—A Systematic Review and Meta-Analysis. Depress. Anxiety 2013, 30, 207–216. [Google Scholar] [CrossRef]
- Abe, O.; Yamasue, H.; Kasai, K.; Yamada, H.; Aoki, S.; Iwanami, A.; Ohtani, T.; Masutani, Y.; Kato, N.; Ohtomo, K. Voxel-Based Diffusion Tensor Analysis Reveals Aberrant Anterior Cingulum Integrity in Posttraumatic Stress Disorder Due to Terrorism. Psychiatry Res. Neuroimaging 2006, 146, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Harnett, N.G.; Goodman, A.M.; Knight, D.C. PTSD-Related Neuroimaging Abnormalities in Brain Function, Structure, and Biochemistry. Exp. Neurol. 2020, 330, 113331. [Google Scholar] [CrossRef] [PubMed]
- Dailey, N.S.; Smith, R.; Bajaj, S.; Alkozei, A.; Gottschlich, M.K.; Raikes, A.C.; Satterfield, B.C.; Killgore, W.D.S. Elevated Aggression and Reduced White Matter Integrity in Mild Traumatic Brain Injury: A DTI Study. Front. Behav. Neurosci. 2018, 12, 118. [Google Scholar] [CrossRef]
- Nakayama, N.; Okumura, A.; Shinoda, J.; Yasokawa, Y.-T.; Miwa, K.; Yoshimura, S.-I. Evidence for White Matter Disruption in Traumatic Brain Injury without Macroscopic Lesions. J. Neurol. Neurosurg. Psychiatry 2006, 77, 850–855. [Google Scholar] [CrossRef] [Green Version]
- Petrie, E.C.; Cross, D.J.; Yarnykh, V.L.; Richards, T.; Martin, N.M.; Pagulayan, K.; Hoff, D.; Hart, K.; Mayer, C.; Tarabochia, M.; et al. Neuroimaging, Behavioral, and Psychological Sequelae of Repetitive Combined Blast/Impact Mild Traumatic Brain Injury in Iraq and Afghanistan War Veterans. J. Neurotrauma 2014, 31, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Rutgers, D.R.; Fillard, P.; Paradot, G.; Tadié, M.; Lasjaunias, P.; Ducreux, D. Diffusion Tensor Imaging Characteristics of the Corpus Callosum in Mild, Moderate, and Severe Traumatic Brain Injury. Am. J. Neuroradiol. 2008, 29, 1730–1735. [Google Scholar] [CrossRef] [Green Version]
- Mu, W.; Catenaccio, E.; Lipton, M.L. Neuroimaging in Blast-Related Mild Traumatic Brain Injury. J. Head Trauma Rehabil. 2017, 32, 55–69. [Google Scholar] [CrossRef]
- Wallace, E.J.; Mathias, J.L.; Ward, L. Diffusion Tensor Imaging Changes Following Mild, Moderate and Severe Adult Traumatic Brain Injury: A Meta-Analysis. Brain Imaging Behav. 2018, 12, 1607–1621. [Google Scholar] [CrossRef]
- Xiong, K.; Zhu, Y.; Zhang, Y.; Yin, Z.; Zhang, J.; Qiu, M.; Zhang, W. White Matter Integrity and Cognition in Mild Traumatic Brain Injury Following Motor Vehicle Accident. Brain Res. 2014, 1591, 86–92. [Google Scholar] [CrossRef]
- Davenport, N.D.; Lamberty, G.J.; Nelson, N.W.; Lim, K.O.; Armstrong, M.T.; Sponheim, S.R. PTSD Confounds Detection of Compromised Cerebral White Matter Integrity in Military Veterans Reporting a History of Mild Traumatic Brain Injury. Brain Inj. 2016, 30, 1491–1500. [Google Scholar] [CrossRef]
- Lepage, C.; Pasternak, O.; Bouix, S.; Shenton, M.E.; Zafonte, R.D.; Coleman, M.J.; McAllister, T.W.; Flashman, L.A.; George, M.S.; Morey, R.A.; et al. White Matter Abnormalities in Mild Traumatic Brain Injury with and without Post-Traumatic Stress Disorder: A Subject-Specific Diffusion Tensor Imaging Study. Brain Imaging Behav. 2017, 12, 870–881. [Google Scholar] [CrossRef] [PubMed]
- Santhanam, P.; Teslovich, T.; Wilson, S.H.; Yeh, P.-H.; Oakes, T.R.; Weaver, L.K. Decreases in White Matter Integrity of Ventro-Limbic Pathway Linked to Post-Traumatic Stress Disorder in Mild Traumatic Brain Injury. J. Neurotrauma 2019, 36, 1093–1098. [Google Scholar] [CrossRef]
- Lopez, K.C.; Leary, J.B.; Pham, D.L.; Chou, Y.-Y.; Dsurney, J.; Chan, L. Brain Volume, Connectivity, and Neuropsychological Performance in Mild Traumatic Brain Injury: The Impact of Post-Traumatic Stress Disorder Symptoms. J. Neurotrauma 2017, 34, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Bresser, T.; Foster-Dingley, J.C.; Wassing, R.; Leerssen, J.; Ramautar, J.R.; Stoffers, D.; Lakbila-Kamal, O.; van den Heuvel, M.; van Someren, E.J.W. Consistent Altered Internal Capsule White Matter Microstructure in Insomnia Disorder. Sleep 2020, 43, zsaa031. [Google Scholar] [CrossRef]
- Sexton, C.E.; Zsoldos, E.; Filippini, N.; Griffanti, L.; Winkler, A.; Mahmood, A.; Allan, C.L.; Topiwala, A.; Kyle, S.D.; Spiegelhalder, K.; et al. Associations between Self-Reported Sleep Quality and White Matter in Community-Dwelling Older Adults: A Prospective Cohort Study. Hum. Brain Mapp. 2017, 38, 5465–5473. [Google Scholar] [CrossRef] [Green Version]
- Khalsa, S.; Hale, J.R.; Goldstone, A.; Wilson, R.S.; Mayhew, S.D.; Bagary, M.; Bagshaw, A.P. Habitual Sleep Durations and Subjective Sleep Quality Predict White Matter Differences in the Human Brain. Neurobiol. Sleep Circadian Rhythm. 2017, 3, 17–25. [Google Scholar] [CrossRef]
- Spiegelhalder, K.; Regen, W.; Prem, M.; Baglioni, C.; Nissen, C.; Feige, B.; Schnell, S.; Kiselev, V.G.; Hennig, J.; Riemann, D. Reduced Anterior Internal Capsule White Matter Integrity in Primary Insomnia. Hum. Brain Mapp. 2014, 35, 3431–3438. [Google Scholar] [CrossRef]
- Li, S.; Tian, J.; Bauer, A.; Huang, R.; Wen, H.; Li, M.; Wang, T.; Xia, L.; Jiang, G. Reduced Integrity of Right Lateralized White Matter in Patients with Primary Insomnia: A Diffusion-Tensor Imaging Study. Radiology 2016, 280, 520–528. [Google Scholar] [CrossRef]
- Kang, J.M.; Joo, S.W.; Son, Y.D.; Kim, H.; Ko, K.P.; Lee, J.S.; Kang, S.G. Low White-Matter Integrity between the Left Thalamus and Inferior Frontal Gyrus in Patients with Insomnia Disorder. J. Psychiatry Neurosci. 2018, 43, 366–374. [Google Scholar] [CrossRef] [Green Version]
- Cai, W.; Zhao, M.; Liu, J.; Liu, B.; Yu, D.; Yuan, K. Right Arcuate Fasciculus and Superior Longitudinal Fasciculus Abnormalities in Primary Insomnia. Brain Imaging Behav. 2019, 13, 1746–1755. [Google Scholar] [CrossRef]
- Kocevska, D.; Tiemeier, H.; Lysen, T.S.; de Groot, M.; Muetzel, R.L.; Van Someren, E.J.W.; Ikram, M.A.; Vernooij, M.W.; Luik, A.I. The Prospective Association of Objectively Measured Sleep and Cerebral White Matter Microstructure in Middle-Aged and Older Persons. Sleep 2019, 42, zsz140. [Google Scholar] [CrossRef]
- Lu, F.-M.; Dai, J.; Couto, T.A.; Liu, C.-H.; Chen, H.; Lu, S.-L.; Tang, L.-R.; Tie, C.-L.; Chen, H.-F.; He, M.-X.; et al. Diffusion Tensor Imaging Tractography Reveals Disrupted White Matter Structural Connectivity Network in Healthy Adults with Insomnia Symptoms. Front. Hum. Neurosci. 2017, 11, 583. [Google Scholar] [CrossRef] [Green Version]
- Grau-Rivera, O.; Operto, G.; Falcón, C.; Sánchez-Benavides, G.; Cacciaglia, R.; Brugulat-Serrat, A.; Gramunt, N.; Salvadó, G.; Suárez-Calvet, M.; Minguillon, C.; et al. Association between Insomnia and Cognitive Performance, Gray Matter Volume, and White Matter Microstructure in Cognitively Unimpaired Adults. Alzheimers Res. Ther. 2020, 12, 4. [Google Scholar] [CrossRef] [Green Version]
- Yaffe, K.; Nasrallah, I.; Hoang, T.D.; Lauderdale, D.S.; Knutson, K.L.; Carnethon, M.R.; Launer, L.J.; Lewis, C.E.; Sidney, S. Sleep Duration and White Matter Quality in Middle-Aged Adults. Sleep 2016, 39, 1743–1747. [Google Scholar] [CrossRef] [Green Version]
- Bottari, S.A.; Lamb, D.G.; Murphy, A.J.; Porges, E.C.; Rieke, J.D.; Harciarek, M.; Datta, S.; Williamson, J.B. Hyperarousal Symptoms and Decreased Right Hemispheric Frontolimbic White Matter Integrity Predict Poorer Sleep Quality in Combat-Exposed Veterans. Brain Inj. 2021, 35, 922–933. [Google Scholar] [CrossRef]
- Fakhran, S.; Yaeger, K.; Alhilali, L. Symptomatic White Matter Changes in Mild Traumatic Brain Injury Resemble Pathologic Features of Early Alzheimer Dementia. Radiology 2013, 269, 249–257. [Google Scholar] [CrossRef] [Green Version]
- Raikes, A.C.; Bajaj, S.; Dailey, N.S.; Smith, R.S.; Alkozei, A.; Satterfield, B.C.; Killgore, W.D.S. Diffusion Tensor Imaging (DTI) Correlates of Self-Reported Sleep Quality and Depression Following Mild Traumatic Brain Injury. Front. Neurol. 2018, 9, 468. [Google Scholar] [CrossRef]
- DeGutis, J.; Chiu, C.; Thai, M.; Esterman, M.; Milberg, W.; McGlinchey, R. Trauma Sequelae Are Uniquely Associated with Components of Self-Reported Sleep Dysfunction in OEF/OIF/OND Veterans. Behav. Sleep Med. 2018, 16, 38–63. [Google Scholar] [CrossRef]
- McGlinchey, R.E.; Milberg, W.P.; Fonda, J.R.; Fortier, C.B. A Methodology for Assessing Deployment Trauma and Its Consequences in OEF/OIF/OND Veterans: The TRACTS Longitudinal Prospective Cohort Study. Int. J. Methods Psychiatr. Res. 2017, 26, e1556. [Google Scholar] [CrossRef] [Green Version]
- Kinzel, P.; Marx, C.E.; Sollmann, N.; Hartl, E.; Guenette, J.P.; Kaufmann, D.; Bouix, S.; Pasternak, O.; Rathi, Y.; Coleman, M.J.; et al. Serum Neurosteroid Levels Are Associated With Cortical Thickness in Individuals Diagnosed with Posttraumatic Stress Disorder and History of Mild Traumatic Brain Injury. Clin. EEG Neurosci. 2020, 51, 285–299. [Google Scholar] [CrossRef] [PubMed]
- Lindemer, E.R.; Salat, D.H.; Leritz, E.C.; McGlinchey, R.E.; Milberg, W.P. Reduced Cortical Thickness with Increased Lifetime Burden of PTSD in OEF/OIF Veterans and the Impact of Comorbid TBI. NeuroImage Clin. 2013, 2, 601–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The Development of a Clinician-Administered PTSD Scale. J. Trauma. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Bovin, M.J.; Lee, D.J.; Sloan, D.M.; Schnurr, P.P.; Kaloupek, D.G.; Keane, T.M.; Marx, B.P. The Clinician-Administered PTSD Scale for DSM–5 (CAPS-5): Development and Initial Psychometric Evaluation in Military Veterans. Psychol. Assess. 2018, 30, 383–395. [Google Scholar] [CrossRef]
- Fortier, C.B.; Amick, M.M.; Grande, L.; McGlynn, S.; Kenna, A.; Morra, L.; Clark, A.; Milberg, W.P.; McGlinchey, R.E. The Boston Assessment of Traumatic Brain Injury–Lifetime (BAT-L) Semistructured Interview: Evidence of Research Utility and Validity. J. Head Trauma Rehabil. 2014, 29, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Cole, J.C.; Motivala, S.J.; Buysse, D.J.; Oxman, M.N.; Levin, M.J.; Irwin, M.R. Validation of a 3-Factor Scoring Model for the Pittsburgh Sleep Quality Index in Older Adults. Sleep 2006, 29, 112–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- First, M.B.; Gibbon, M.; Spitzer, R.L.; Williams, J.B.W. Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I); American Psychiatric Press: Washington, DC, USA, 1997. [Google Scholar]
- Vogt, D.S.; Smith, B.N.; King, L.A.; King, D.W.; Knight, J.A.; Vasterling, J.J. Deployment Risk and Resilience Inventory-2 (DRRI-2): An Updated Tool for Assessing Psychosocial Risk and Resilience Factors among Service Members and Veterans. J. Trauma. Stress 2013, 26, 710–717. [Google Scholar] [CrossRef]
- Greve, D.N.; Fischl, B. Accurate and Robust Brain Image Alignment Using Boundary-Based Registration. Neuroimage 2009, 48, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Jenkinson, M.; Bannister, P.; Brady, M.; Smith, S. Improved Optimization for the Robust and Accurate Linear Registration and Motion Correction of Brain Images. Neuroimage 2002, 17, 825–841. [Google Scholar] [CrossRef]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Noh, T.; Juvekar, P.; Frisken, S.F.; Rigolo, L.; Norton, I.; Kapur, T.; Pujol, S.; Wells, W.; Yarmarkovich, A.; et al. SlicerDMRI: Diffusion MRI and Tractography Research Software for Brain Cancer Surgery Planning and Visualization. JCO Clin. Cancer Inform. 2020, 299–309. [Google Scholar] [CrossRef]
- Norton, I.; Essayed, W.I.; Zhang, F.; Pujol, S.; Yarmarkovich, A.; Golby, A.J.; Kindlmann, G.; Wasserman, D.; Estepar, R.S.J.; Rathi, Y.; et al. SlicerDMRI: Open Source Diffusion MRI Software for Brain Cancer Research. Cancer Res. 2017, 77, e101–e103. [Google Scholar] [CrossRef] [Green Version]
- Levitt, J.J.; Zhang, F.; Vangel, M.; Nestor, P.G.; Rathi, Y.; Kubicki, M.; Shenton, M.E.; O’Donnell, L.J. The Organization of Frontostriatal Brain Wiring in Healthy Subjects Using a Novel Diffusion Imaging Fiber Cluster Analysis. Cereb. Cortex 2021, 31, 5308–5318. [Google Scholar] [CrossRef]
- Kochsiek, J.; O’Donnell, L.J.; Zhang, F.; Bonke, E.M.; Sollmann, N.; Tripodis, Y.; Wiegand, T.L.T.; Kaufmann, D.; Umminger, L.; Di Biase, M.A.; et al. Exposure to Repetitive Head Impacts Is Associated with Corpus Callosum Microstructure and Plasma Total Tau in Former Professional American Football Players. J. Magn. Reson. Imaging 2021, 54, 1819–1829. [Google Scholar] [CrossRef]
- Irimia, A.; Fan, D.; Chaudhari, N.N.; Ngo, V.; Zhang, F.; Joshi, S.H.; O’Donnell, L.J. Mapping Cerebral Connectivity Changes after Mild Traumatic Brain Injury in Older Adults Using Diffusion Tensor Imaging and Riemannian Matching of Elastic Curves. In Proceedings of the 2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), Iowa City, IA, USA, 3–7 April 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 1690–1693. [Google Scholar]
- Gong, S.; Zhang, F.; Norton, I.; Essayed, W.I.; Unadkat, P.; Rigolo, L.; Pasternak, O.; Rathi, Y.; Hou, L.; Golby, A.J.; et al. Free Water Modeling of Peritumoral Edema Using Multi-Fiber Tractography: Application to Tracking the Arcuate Fasciculus for Neurosurgical Planning. PLoS ONE 2018, 13, e197056. [Google Scholar] [CrossRef] [Green Version]
- Zekelman, L.R.; Zhang, F.; Makris, N.; He, J.; Chen, Y.; Xue, T.; Liera, D.; Drane, D.L.; Rathi, Y.; Golby, A.J.; et al. White Matter Association Tracts Underlying Language and Theory of Mind: An Investigation of 809 Brains from the Human Connectome Project. Neuroimage 2022, 246, 118739. [Google Scholar] [CrossRef]
- Robles, D.J.; Dharani, A.; Rostowsky, K.A.; Chaudhari, N.N.; Ngo, V.; Zhang, F.; O’Donnell, L.J.; Green, L.; Sheikh-Bahaei, N.; Chui, H.C.; et al. Older Age, Male Sex, and Cerebral Microbleeds Predict White Matter Loss after Traumatic Brain Injury. GeroScience 2022, 44, 83–102. [Google Scholar] [CrossRef]
- Zhang, F.; Karayumak, S.C.; Pieper, S.; O’Donnell, L.J. Consistent White Matter Parcellation in Adolescent Brain Cognitive Development (ABCD). In Proceedings of the Annual Meeting of the International Society for Magnetic Resonance in Medicine (ISMRM), London, UK, 7–12 May 2022; ISMRM: Concord, CA, USA, 2022. [Google Scholar]
- He, H.; Zhang, F.; Pieper, S.; Makris, N.; Rathi, Y.; Wells, W.; O’Donnell, L.J. Model and Predict Age and Sex in Healthy Subjects Using Brain White Matter Features: A Deep Learning Approach. In Proceedings of the 2022 IEEE 19th International Symposium on Biomedical Imaging (ISBI), Kolkata, India, 28–31 March 2022. [Google Scholar] [CrossRef]
- Wang, J.; Zhang, F.; Zhao, C.; Zeng, Q.; He, J.; O’Donnell, L.J.; Feng, Y. Investigation of Local White Matter Abnormality in Parkinson’s Disease by Using an Automatic Fiber Tract Parcellation. Behav. Brain Res. 2020, 394, 112805. [Google Scholar] [CrossRef]
- Sydnor, V.J.; Rivas-Grajales, A.M.; Lyall, A.E.; Zhang, F.; Bouix, S.; Karmacharya, S.; Shenton, M.E.; Westin, C.-F.; Makris, N.; Wassermann, D.; et al. A Comparison of Three Fiber Tract Delineation Methods and Their Impact on White Matter Analysis. Neuroimage 2018, 178, 318–331. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Wu, Y.; Norton, I.; Rathi, Y.; Golby, A.J.; O’Donnell, L.J. Test–Retest Reproducibility of White Matter Parcellation Using Diffusion MRI Tractography Fiber Clustering. Hum. Brain Mapp. 2019, 40, 3041–3057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, L.J.; Suter, Y.; Rigolo, L.; Kahali, P.; Zhang, F.; Norton, I.; Albi, A.; Olubiyi, O.; Meola, A.; Essayed, W.I.; et al. Automated White Matter Fiber Tract Identification in Patients with Brain Tumors. NeuroImage Clin. 2017, 13, 138–153. [Google Scholar] [CrossRef]
- Lienhard, S.; Malcolm, J.G.; Westin, C.-F.; Rathi, Y. A Full Bi-Tensor Neural Tractography Algorithm Using the Unscented Kalman Filter. EURASIP J. Adv. Signal Process. 2011, 2011, 77. [Google Scholar] [CrossRef] [Green Version]
- Malcolm, J.G.; Shenton, M.E.; Rathi, Y. Filtered Multitensor Tractography. IEEE Trans. Med. Imaging 2010, 29, 1664–1675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vos, S.B.; Viergever, M.A.; Leemans, A. Multi-Fiber Tractography Visualizations for Diffusion MRI Data. PLoS ONE 2013, 8, e81453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farquharson, S.; Tournier, J.-D.; Calamante, F.; Fabinyi, G.; Schneider-Kolsky, M.; Jackson, G.D.; Connelly, A. White Matter Fiber Tractography: Why We Need to Move beyond DTI. J. Neurosurg. 2013, 118, 1367–1377. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Wu, Y.; Norton, I.; Rigolo, L.; Rathi, Y.; Makris, N.; O’Donnell, L.J. An Anatomically Curated Fiber Clustering White Matter Atlas for Consistent White Matter Tract Parcellation across the Lifespan. Neuroimage 2018, 179, 429–447. [Google Scholar] [CrossRef]
- Baumgartner, C.; Michailovich, O.; Levitt, J.; Pasternak, O.; Bouix, S.; Westin, C.-F.; Rathi, Y. A Unified Tractography Framework for Comparing Diffusion Models on Clinical Scans. In Proceedings of the International Conference on Medical Image Computing and Computer Assisted Intervention (MICCAI’12)—Computational Diffusion MRI Workshop, Nice, France, 1–5 October 2012; pp. 27–32. [Google Scholar]
- Chen, Z.; Tie, Y.; Olubiyi, O.; Rigolo, L.; Mehrtash, A.; Norton, I.; Pasternak, O.; Rathi, Y.; Golby, A.J.; O’Donnell, L.J. Reconstruction of the Arcuate Fasciculus for Surgical Planning in the Setting of Peritumoral Edema Using Two-Tensor Unscented Kalman Filter Tractography. NeuroImage Clin. 2015, 7, 815–822. [Google Scholar] [CrossRef] [Green Version]
- Liao, R.; Ning, L.; Chen, Z.; Rigolo, L.; Gong, S.; Pasternak, O.; Golby, A.J.; Rathi, Y.; O’Donnell, L.J. Performance of Unscented Kalman Filter Tractography in Edema: Analysis of the Two-Tensor Model. NeuroImage Clin. 2017, 15, 819–831. [Google Scholar] [CrossRef]
- O’Donnell, L.J.; Wells, W.M.; Golby, A.J.; Westin, C.-F. Unbiased Groupwise Registration of White Matter Tractography. Med. Image Comput. Comput. Assist. Interv. 2012, 15, 123–130. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, L.J.; Westin, C.F. Automatic Tractography Segmentation Using a High-Dimensional White Matter Atlas. IEEE Trans. Med. Imaging 2007, 26, 1562–1575. [Google Scholar] [CrossRef] [PubMed]
- Maier-Hein, K.H.; Neher, P.F.; Houde, J.-C.; Côté, M.-A.; Garyfallidis, E.; Zhong, J.; Chamberland, M.; Yeh, F.-C.; Lin, Y.-C.; Ji, Q.; et al. The Challenge of Mapping the Human Connectome Based on Diffusion Tractography. Nat. Commun. 2017, 8, 1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xue, T.; Zhang, F.; Zhang, C.; Chen, Y.; Song, Y.; Makris, N.; Rathi, Y.; Cai, W.; O’Donnell, L.J. Supwma: Consistent and Efficient Tractography Parcellation of Superficial White Matter with Deep Learning. In Proceedings of the 2022 IEEE 19th International Symposium on Biomedical Imaging (ISBI), Kolkata, India, 28–31 March 2022; IEEE: New York, NY, USA; pp. 1–5. [Google Scholar]
- Steinmann, S.; Lyall, A.E.; Langhein, M.; Nägele, F.L.; Rauh, J.; Cetin-Karayumak, S.; Zhang, F.; Mussmann, M.; Billah, T.; Makris, N.; et al. Sex-Related Differences in White Matter Asymmetry and Its Implications for Verbal Working Memory in Psychosis High-Risk State. Front. Psychiatry 2021, 12, 686967. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Cetin Karayumak, S.; Hoffmann, N.; Rathi, Y.; Golby, A.J.; O’Donnell, L.J. Deep White Matter Analysis (DeepWMA): Fast and Consistent Tractography Segmentation. Med. Image Anal. 2020, 65, 101761. [Google Scholar] [CrossRef]
- Hong, Y.; O’Donnell, L.J.; Savadjiev, P.; Zhang, F.; Wassermann, D.; Pasternak, O.; Johnson, H.; Paulsen, J.; Vonsattel, J.P.; Makris, N.; et al. Genetic Load Determines Atrophy in Hand Cortico-Striatal Pathways in Presymptomatic Huntington’s Disease. Hum. Brain Mapp. 2018, 39, 3871–3883. [Google Scholar] [CrossRef]
- Pasternak, O.; Sochen, N.; Gur, Y.; Intrator, N.; Assaf, Y. Free Water Elimination and Mapping from Diffusion MRI. Magn. Reson. Med. 2009, 62, 717–730. [Google Scholar] [CrossRef]
- Metzler-Baddeley, C.; O’Sullivan, M.J.; Bells, S.; Pasternak, O.; Jones, D.K. How and How Not to Correct for CSF-Contamination in Diffusion MRI. Neuroimage 2012, 59, 1394–1403. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis—A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Isaac, L.; Main, K.L.; Soman, S.; Gotlib, I.H.; Furst, A.J.; Kinoshita, L.M.; Fairchild, J.K.; Yesavage, J.A.; Ashford, J.W.; Bayley, P.J.; et al. The Impact of Depression on Veterans with PTSD and Traumatic Brain Injury: A Diffusion Tensor Imaging Study. Biol. Psychol. 2015, 105, 20–28. [Google Scholar] [CrossRef]
- Espinoza Oyarce, D.A.; Shaw, M.E.; Alateeq, K.; Cherbuin, N. Volumetric Brain Differences in Clinical Depression in Association with Anxiety: A Systematic Review with Meta-Analysis. J. Psychiatry Neurosci. 2020, 45, 406–429. [Google Scholar] [CrossRef]
- Davey, D.K.; Jurick, S.M.; Crocker, L.D.; Hoffman, S.N.; Sanderson-Cimino, M.; Tate, D.F.; Velez, C.S.; Delano-Wood, L.; Jak, A.J. White Matter Integrity, Suicidal Ideation, and Cognitive Dysfunction in Combat-Exposed Iraq and Afghanistan Veterans. Psychiatry Res. Neuroimaging 2021, 317, 111389. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.F.; Peng, W.; Sweeney, J.A.; Jia, Z.Y.; Gong, Q.Y. Brain Structure Alterations in Depression: Psychoradiological Evidence. CNS Neurosci. Ther. 2018, 24, 994–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Velzen, L.S.; Kelly, S.; Isaev, D.; Aleman, A.; Aftanas, L.I.; Bauer, J.; Baune, B.T.; Brak, I.V.; Carballedo, A.; Connolly, C.G.; et al. White Matter Disturbances in Major Depressive Disorder: A Coordinated Analysis across 20 International Cohorts in the ENIGMA MDD Working Group. Mol. Psychiatry 2020, 25, 1511–1525. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.S.; Lee, S.H. White Matter-Based Structural Brain Network of Anxiety. Adv. Exp. Med. Biol. 2020, 1191, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Zhong, Y.; Ma, Z.; Lu, X.; Zhang, N.; Fox, P.T.; Wang, C. Gray Matter Changes in Panic Disorder: A Voxel-Based Meta-Analysis and Meta-Analytic Connectivity Modeling. Psychiatry Res. Neuroimaging 2018, 282, 82–89. [Google Scholar] [CrossRef]
- Harrewijn, A.; Cardinale, E.M.; Groenewold, N.A.; Bas-Hoogendam, J.M.; Aghajani, M.; Hilbert, K.; Cardoner, N.; Porta-Casteràs, D.; Gosnell, S.; Salas, R.; et al. Cortical and Subcortical Brain Structure in Generalized Anxiety Disorder: Findings from 28 Research Sites in the ENIGMA-Anxiety Working Group. Transl. Psychiatry 2021, 11, 502. [Google Scholar] [CrossRef]
- Pando-Naude, V.; Toxto, S.; Fernandez-Lozano, S.; Parsons, C.E.; Alcauter, S.; Garza-Villarreal, E.A. Gray and White Matter Morphology in Substance Use Disorders: A Neuroimaging Systematic Review and Meta-Analysis. Transl. Psychiatry 2021, 11, 29. [Google Scholar] [CrossRef]
- Navarri, X.; Afzali, M.H.; Lavoie, J.; Sinha, R.; Stein, D.J.; Momenan, R.; Veltman, D.J.; Korucuoglu, O.; Sjoerds, Z.; van Holst, R.J.; et al. How Do Substance Use Disorders Compare to Other Psychiatric Conditions on Structural Brain Abnormalities? A Cross-Disorder Meta-Analytic Comparison Using the ENIGMA Consortium Findings. Hum. Brain Mapp. 2022, 43, 399–413. [Google Scholar] [CrossRef]
- Kuo, J.R.; Kaloupek, D.G.; Woodward, S.H. Amygdala Volume in Combat-Exposed Veterans with and without Posttraumatic Stress Disorder: A Cross-Sectional Study. Arch. Gen. Psychiatry 2012, 69, 1080–1086. [Google Scholar] [CrossRef]
- Aupperle, R.L.; Connolly, C.G.; Stillman, A.N.; May, A.C.; Paulus, M.P. Deployment and Post-Deployment Experiences in OEF/OIF Veterans: Relationship to Gray Matter Volume. PLoS ONE 2013, 8, e75880. [Google Scholar] [CrossRef]
- Clausen, A.N.; Billinger, S.A.; Sisante, J.-F.V.; Suzuki, H.; Aupperle, R.L. Preliminary Evidence for the Impact of Combat Experiences on Gray Matter Volume of the Posterior Insula. Front. Psychol. 2017, 8, 2151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, O.; Adolf, J.; Gleich, T.; Willmund, G.; Zimmermann, P.; Lindenberger, U.; Gallinat, J.; Kühn, S. Military Deployment Correlates with Smaller Prefrontal Gray Matter Volume and Psychological Symptoms in a Subclinical Population. Transl. Psychiatry 2017, 7, e1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McWhinney, S.R.; Abé, C.; Alda, M.; Benedetti, F.; Bøen, E.; del Mar Bonnin, C.; Borgers, T.; Brosch, K.; Canales-Rodríguez, E.J.; Cannon, D.M.; et al. Association between Body Mass Index and Subcortical Brain Volumes in Bipolar Disorders–ENIGMA Study in 2735 Individuals. Mol. Psychiatry 2021, 26, 6806–6819. [Google Scholar] [CrossRef] [PubMed]
- Medic, N.; Ziauddeen, H.; Ersche, K.D.; Farooqi, I.S.; Bullmore, E.T.; Nathan, P.J.; Ronan, L.; Fletcher, P.C. Increased Body Mass Index Is Associated with Specific Regional Alterations in Brain Structure. Int. J. Obes. 2016, 40, 1177–1182. [Google Scholar] [CrossRef] [Green Version]
- Steegers, C.; Blok, E.; Lamballais, S.; Jaddoe, V.; Bernardoni, F.; Vernooij, M.; van der Ende, J.; Hillegers, M.; Micali, N.; Ehrlich, S.; et al. The Association between Body Mass Index and Brain Morphology in Children: A Population-Based Study. Brain Struct. Funct. 2021, 226, 787–800. [Google Scholar] [CrossRef]
- Bolzenius, J.D.; Laidlaw, D.H.; Cabeen, R.P.; Conturo, T.E.; McMichael, A.R.; Lane, E.M.; Heaps, J.M.; Salminen, L.E.; Baker, L.M.; Scott, S.E.; et al. Brain Structure and Cognitive Correlates of Body Mass Index in Healthy Older Adults. Behav. Brain Res. 2015, 278, 342–347. [Google Scholar] [CrossRef] [Green Version]
- Gunstad, J.; Paul, R.H.; Cohen, R.A.; Tate, D.F.; Spitznagel, M.B.; Grieve, S.; Gordon, E. Relationship between Body Mass Index and Brain Volume in Healthy Adults. Int. J. Neurosci. 2008, 118, 1582–1593. [Google Scholar] [CrossRef]
- Alosco, M.L.; Stanek, K.M.; Galioto, R.; Korgaonkar, M.S.; Grieve, S.M.; Brickman, A.M.; Spitznagel, M.B.; Gunstad, J. Body Mass Index and Brain Structure in Healthy Children and Adolescents. Int. J. Neurosci. 2014, 124, 49–55. [Google Scholar] [CrossRef]
- Thomaes, K.; Dorrepaal, E.; Draijer, N.; Jansma, E.P.; Veltman, D.J.; van Balkom, A.J. Can Pharmacological and Psychological Treatment Change Brain Structure and Function in PTSD? A Systematic Review. J. Psychiatr. Res. 2014, 50, 1–15. [Google Scholar] [CrossRef]
- Scherk, H.; Falkai, P. Changes in Brain Structure Caused by Neuroleptic Medication. Nervenarzt 2004, 75, 1112–1117. [Google Scholar] [CrossRef]
- Seiger, R.; Gryglewski, G.; Klöbl, M.; Kautzky, A.; Godbersen, G.M.; Rischka, L.; Vanicek, T.; Hienert, M.; Unterholzner, J.; Silberbauer, L.R.; et al. The Influence of Acute SSRI Administration on White Matter Microstructure in Patients Suffering from Major Depressive Disorder and Healthy Controls. Int. J. Neuropsychopharmacol. 2021, 24, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Dusi, N.; Barlati, S.; Vita, A.; Brambilla, P. Brain Structural Effects of Antidepressant Treatment in Major Depression. Curr. Neuropharmacol. 2015, 13, 458–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira, R.; Coelho, A.; Reis, J.; Portugal-Nunes, C.; Magalhães, R.; Ferreira, S.; Moreira, P.S.; Sousa, N.; Bessa, J.M. White Matter Microstructure Alterations Associated with Paroxetine Treatment Response in Major Depression. Front. Behav. Neurosci. 2021, 15, 693109. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xu, X.; Luo, Q.; Luo, Y.; Chen, Y.; Lui, S.; Wu, M.; Zhu, H.; Kemp, G.J.; Gong, Q. Brain Grey Matter Volume Alterations Associated with Antidepressant Response in Major Depressive Disorder. Sci. Rep. 2017, 7, 10464. [Google Scholar] [CrossRef] [Green Version]
- Fani, N.; Harnett, N.G.; Bradley, B.; Mekawi, Y.; Powers, A.; Stevens, J.S.; Ressler, K.J.; Carter, S.E. Racial Discrimination and White Matter Microstructure in Trauma-Exposed Black Women. Biol. Psychiatry 2022, 91, 254–261. [Google Scholar] [CrossRef]
- Noble, K.G.; Korgaonkar, M.S.; Grieve, S.M.; Brickman, A.M. Higher Education Is an Age-Independent Predictor of White Matter Integrity and Cognitive Control in Late Adolescence. Dev. Sci. 2013, 16, 653–664. [Google Scholar] [CrossRef]
- Tummala, S.; Roy, B.; Park, B.; Kang, D.W.; Woo, M.A.; Harper, R.M.; Kumar, R. Associations between Brain White Matter Integrity and Disease Severity in Obstructive Sleep Apnea. J. Neurosci. Res. 2016, 94, 915–923. [Google Scholar] [CrossRef] [Green Version]
- Balba, N.M.; Elliott, J.E.; Weymann, K.B.; Opel, R.A.; Duke, J.W.; Oken, B.S.; Morasco, B.J.; Heinricher, M.M.; Lim, M.M. Increased Sleep Disturbances and Pain in Veterans with Comorbid Traumatic Brain Injury and Posttraumatic Stress Disorder. J. Clin. Sleep Med. 2018, 14, 1865–1878. [Google Scholar] [CrossRef] [Green Version]
- Martindale, S.L.; Farrell-Carnahan, L.V.; Ulmer, C.S.; Kimbrel, N.A.; McDonald, S.D.; Rowland, J.A. Sleep Quality in Returning Veterans: The Influence of Mild Traumatic Brain Injury. Rehabil. Psychol. 2017, 62, 563–570. [Google Scholar] [CrossRef]
- Selassie, A.W.; Zaloshnja, E.; Langlois, J.A.; Miller, T.; Jones, P.; Steiner, C. Incidence of Long-Term Disability Following Traumatic Brain Injury Hospitalization, United States, 2003. J. Head Trauma Rehabil. 2008, 23, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, J.D.; Cancelliere, C.; Carroll, L.J.; Côté, P.; Hincapié, C.A.; Holm, L.W.; Hartvigsen, J.; Donovan, J.; Nygren-De Boussard, C.; Kristman, V.L.; et al. Systematic Review of Self-Reported Prognosis in Adults after Mild Traumatic Brain Injury: Results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch. Phys. Med. Rehabil. 2014, 95, 132–151. [Google Scholar] [CrossRef] [PubMed]
- Gonschorek, A.S.; Schwenkreis, P.; Guthke, T. Psychische Störungen Nach Leichtem Schädel-Hirn-Trauma. Nervenarzt 2016, 87, 567–579. [Google Scholar] [CrossRef] [PubMed]
- Martindale, S.L.; Konst, M.J.; Bateman, J.R.; Arena, A.; Rowland, J.A. The Role of PTSD and TBI in Post-Deployment Sleep Outcomes. Mil. Psychol. 2020, 32, 212–221. [Google Scholar] [CrossRef]
- Jessen, N.A.; Munk, A.S.F.; Lundgaard, I.; Nedergaard, M. The Glymphatic System: A Beginner’s Guide. Neurochem. Res. 2015, 40, 2583–2599. [Google Scholar] [CrossRef] [Green Version]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep Drives Metabolite Clearance from the Adult Brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [Green Version]
- Piantino, J.; Schwartz, D.L.; Luther, M.; Newgard, C.; Silbert, L.; Raskind, M.; Pagulayan, K.; Kleinhans, N.; Iliff, J.; Peskind, E. Link between Mild Traumatic Brain Injury, Poor Sleep, and Magnetic Resonance Imaging: Visible Perivascular Spaces in Veterans. J. Neurotrauma 2021, 38, 2391–2399. [Google Scholar] [CrossRef]
- Mohamed, A.Z.; Cumming, P.; Nasrallah, F.A.; Department of Defense Alzheimer’s Disease Neuroimaging Initiative. White Matter Alterations Are Associated with Cognitive Dysfunction Decades after Moderate-to-Severe Traumatic Brain Injury and/or Posttraumatic Stress Disorder. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2021, 6, 1100–1109. [Google Scholar] [CrossRef]
- Wooten, D.W.; Ortiz-Terán, L.; Zubcevik, N.; Zhang, X.; Huang, C.; Sepulcre, J.; Atassi, N.; Johnson, K.A.; Zafonte, R.D.; El Fakhri, G. Multi-Modal Signatures of Tau Pathology, Neuronal Fiber Integrity, and Functional Connectivity in Traumatic Brain Injury. J. Neurotrauma 2019, 36, 3233–3243. [Google Scholar] [CrossRef]
- Santhanam, P.; Wilson, S.H.; Oakes, T.R.; Weaver, L.K. Effects of Mild Traumatic Brain Injury and Post-Traumatic Stress Disorder on Resting-State Default Mode Network Connectivity. Brain Res. 2019, 1711, 77–82. [Google Scholar] [CrossRef]
- Sydnor, V.J.; Bouix, S.; Pasternak, O.; Hartl, E.; Levin-Gleba, L.; Reid, B.; Tripodis, Y.; Guenette, J.P.; Kaufmann, D.; Makris, N.; et al. Mild Traumatic Brain Injury Impacts Associations between Limbic System Microstructure and Post-Traumatic Stress Disorder Symptomatology. NeuroImage Clin. 2020, 26, 102190. [Google Scholar] [CrossRef]
- Rezaie, L.; Fobian, A.D.; McCall, W.V.; Khazaie, H. Paradoxical Insomnia and Subjective–Objective Sleep Discrepancy: A Review. Sleep Med. Rev. 2018, 40, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Mysliwiec, V.; McGraw, L.; Pierce, R.; Smith, P.; Trapp, B.; Roth, B.J. Sleep Disorders and Associated Medical Comorbidities in Active Duty Military Personnel. Sleep 2013, 36, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghadami, M.R.; Khaledi-Paveh, B.; Nasoori, M.; Khazaie, H. PTSD-Related Paradoxical Insomnia: An Actigraphic Study among Veterans with Chronic PTSD. J. Inj. Violence Res. 2015, 7, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werner, K.B.; Griffin, M.G.; Galovski, T.E. Objective and Subjective Measurement of Sleep Disturbance in Female Trauma Survivors with Posttraumatic Stress Disorder. Psychiatry Res. 2016, 240, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Lewis, C.; Lewis, K.; Kitchiner, N.; Isaac, S.; Jones, I.; Bisson, J.I. Sleep Disturbance in Post-Traumatic Stress Disorder (PTSD): A Systematic Review and Meta-Analysis of Actigraphy Studies. Eur. J. Psychotraumatol. 2020, 11, 1767349. [Google Scholar] [CrossRef] [PubMed]
- Kram Mendelsohn, A.; Daffre, C.; Oliver, K.I.; Seo, J.; Lasko, N.B.; Pace-Schott, E.F. 1071 Subjective Measures of Hyperarousal Predict Subjective Longitudinal and Retrospective Measures of Sleep Quality in Individuals Exposed to Trauma. Sleep 2020, 43, A408. [Google Scholar] [CrossRef]
- Parrino, L.; Milioli, G.; De Paolis, F.; Grassi, A.; Terzano, M.G. Paradoxical Insomnia: The Role of CAP and Arousals in Sleep Misperception. Sleep Med. 2009, 10, 1139–1145. [Google Scholar] [CrossRef]
- Johnson, D.A.; Javaheri, S.; Guo, N.; Champion, C.L.; Sims, J.F.; Brock, M.P.; Sims, M.; Patel, S.R.; Williams, D.R.; Wilson, J.G.; et al. Objective Measures of Sleep Apnea and Actigraphy-Based Sleep Characteristics as Correlates of Subjective Sleep Quality in an Epidemiologic Study: The Jackson Heart Sleep Study. Psychosom. Med. 2020, 82, 324–330. [Google Scholar] [CrossRef]
- Moshkani Farahani, D.; Tavallaie, A.; Vahedi, E.; Rezaiemaram, P.; Naderi, Z.; Talaie, A. The Relationship between Perceived Sleep Quality, Polysomnographic Measures and Depressive Symptoms in Chemically-Injured Veterans: A Pilot Study. Iran. J. Psychiatry 2014, 9, 169–174. [Google Scholar]
- Strasshofer, D.R.; Pacella, M.L.; Irish, L.A.; Palmieri, P.A.; Johnson, D.M.; Delahanty, D.L. The Role of Perceived Sleep Quality in the Relationship between PTSD Symptoms and General Mental Health. Ment. Health Prev. 2017, 5, 27–32. [Google Scholar] [CrossRef]
- Fernandez-Mendoza, J.; Calhoun, S.L.; Bixler, E.O.; Karataraki, M.; Liao, D.; Vela-Bueno, A.; Jose Ramos-Platon, M.; Sauder, K.A.; Basta, M.; Vgontzas, A.N. Sleep Misperception and Chronic Insomnia in the General Population: Role of Objective Sleep Duration and Psychological Profiles. Psychosom. Med. 2011, 73, 88–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.E.; Campbell-Sills, L.; Kessler, R.C.; Sun, X.; Heeringa, S.G.; Nock, M.K.; Ursano, R.J.; Jain, S.; Stein, M.B. Pre-Deployment Insomnia Is Associated with Post-Deployment Post-Traumatic Stress Disorder and Suicidal Ideation in US Army Soldiers. Sleep 2019, 42, zsy229. [Google Scholar] [CrossRef] [Green Version]
- Pace-Schott, E.F.; Milad, M.R.; Orr, S.P.; Rauch, S.L.; Stickgold, R.; Pitman, R.K. Sleep Promotes Generalization of Extinction of Conditioned Fear. Sleep 2009, 32, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Zuj, D.V.; Palmer, M.A.; Hsu, C.-M.K.; Nicholson, E.L.; Cushing, P.J.; Gray, K.E.; Felmingham, K.L. Impaired Fear Extinction Associated with PTSD Increased with Hours since Waking. Depress. Anxiety 2016, 33, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.P.; van der Helm, E. Overnight Therapy? The Role of Sleep in Emotional Brain Processing. Psychol. Bull. 2009, 135, 731–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merritt, V.C.; Jurick, S.M.; Crocker, L.D.; Sullan, M.J.; Sakamoto, M.S.; Davey, D.K.; Hoffman, S.N.; Keller, A.V.; Jak, A.J. Associations between Multiple Remote Mild TBIs and Objective Neuropsychological Functioning and Subjective Symptoms in Combat-Exposed Veterans. Arch. Clin. Neuropsychol. 2020, 35, 491–505. [Google Scholar] [CrossRef] [Green Version]
- Foster, S.N.; Hansen, S.L.; Capener, D.C.; Matsangas, P.; Mysliwiec, V. Gender Differences in Sleep Disorders in the US Military. Sleep Health 2017, 3, 336–341. [Google Scholar] [CrossRef]
- Seitz, J.; Cetin-Karayumak, S.; Lyall, A.; Pasternak, O.; Baxi, M.; Vangel, M.; Pearlson, G.; Tamminga, C.; Sweeney, J.; Clementz, B.; et al. Investigating Sexual Dimorphism of Human White Matter in a Harmonized, Multisite Diffusion Magnetic Resonance Imaging Study. Cereb. Cortex 2021, 31, 201–212. [Google Scholar] [CrossRef]
- Koffel, E.; Polusny, M.A.; Arbisi, P.A.; Erbes, C.R. Pre-Deployment Daytime and Nighttime Sleep Complaints as Predictors of Post-Deployment PTSD and Depression in National Guard Troops. J. Anxiety Disord. 2013, 27, 512–519. [Google Scholar] [CrossRef]
- Acheson, D.T.; Kwan, B.; Maihofer, A.X.; Risbrough, V.B.; Nievergelt, C.M.; Clark, J.W.; Tu, X.M.; Irwin, M.R.; Baker, D.G. Sleep Disturbance at Pre-Deployment Is a Significant Predictor of Post-Deployment Re-Experiencing Symptoms. Eur. J. Psychotraumatol. 2019, 10, 1679964. [Google Scholar] [CrossRef] [Green Version]
- Van Liempt, S.; Van Zuiden, M.; Westenberg, H.; Super, A.; Vermetten, E. Impact of Impaired Sleep on the Development of PTSD Symptoms in Combat Veterans: A Prospective Longitudinal Cohort Study. Depress. Anxiety 2013, 30, 469–474. [Google Scholar] [CrossRef] [PubMed]
- van den Heuvel, M.P.; Mandl, R.C.W.; Kahn, R.S.; Hulshoff Pol, H.E. Functionally Linked Resting-State Networks Reflect the Underlying Structural Connectivity Architecture of the Human Brain. Hum. Brain Mapp. 2009, 30, 3127–3141. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Sample (N = 180) | PTSD (n = 38) | mTBI (n = 25) | Comorbid PTSD+mTBI (n = 94) | No History of PTSD or mTBI (n = 23) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | ||
| Age (years) | 31.49 ± 7.60 | 20–55 | 31.18 ± 6.79 | 22–48 | 32.60 ± 9.82 | 21–55 | 31.22 ± 7.18 | 20–53 | 31.87 ± 8.24 | 23–53 | |
| Education (years) | 13.89 ± 1.96 | 12–20 | 13.34 ± 1.60 | 12–17 | 14.36 ± 1.78 | 12–18 | 13.84 ± 2.03 | 12–20 | 14.48 ± 2.19 | 12–19 | |
| Number of OEF/OIF deployments | 1.40 ± 0.69 | 1–5 | 1.39 ± 0.79 | 1–4 | 1.40 ± 0.65 | 1–3 | 1.41 ± 0.71 | 1–5 | 1.35 ± 4.87 | 1–2 | |
| Number of other stressful deployments | 0.39 ± 0.77 | 0–5 | 0.37 ± 0.63 | 0–3 | 0.24 ± 0.44 | 0–3 | 0.49 ± 0.89 | 0–5 | 0.22 ± 0.52 | 0–2 | |
| Total duration of OEF/OIF deployments (months) | 13.64 ± 8.37 | 3–53 | 13.84 ± 9.75 | 5–53 | 14.72 ± 7.89 | 3–31 | 13.49 ± 8.36 | 3–52 | 13.87 ± 6.81 | 4–28 | |
| Total duration of other deployments (months) | 2.84 ± 6.21 | 0–49 | 3.03 ± 5.22 | 0–17 | 1.36 ± 3.87 | 0–16 | 3.41 ± 7.24 | 0–49 | 1.83 ± 4.93 | 0–18 | |
| Number of lifetime mTBIs | 1.39 ± 2.18 | 0–18 | 0.00 ± 0.00 | 0–0 | 1.56 ± 0.96 | 1–5 | 2.24 ± 2.62 | 1–18 | 0.00 ± 0.00 | 0–0 | |
| Lifetime mTBI burden | 2.22 ± 3.42 | 0–31 | 0.00 ± 0.00 | 0–0 | 2.40 ± 1.47 | 1–6 | 3.61 ± 4.10 | 1–31 | 0.00 ± 0.00 | 0–0 | |
| Total CAPS | 45.84 ± 27.14 | 0–104 | 39.79 ± 21.15 | 6–88 | 15.84 ± 13.73 | 0–41 | 51.80 ± 18.65 | 2–92 | 12.65 ± 10.60 | 0–39 | |
| n | % * | n | % * | n | % * | n | % * | n | % * | ||
| Ethnicity | American Indian or Alaska Native | 1 | 0.56 | 0 | 0.00 | 0 | 0.00 | 1 | 1.06 | 0 | 0.00 |
| Asian | 2 | 1.11 | 1 | 2.63 | 0 | 0.00 | 1 | 1.06 | 0 | 0.00 | |
| Black | 13 | 7.22 | 4 | 10.53 | 3 | 12.00 | 6 | 6.38 | 0 | 0.00 | |
| Hispanic or Latino | 26 | 14.44 | 6 | 15.79 | 5 | 20.00 | 13 | 13.83 | 2 | 8.70 | |
| Native Hawaiian or Pacific Islander | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | |
| White | 138 | 76.67 | 26 | 68.42 | 17 | 68.00 | 74 | 78.72 | 21 | 91.30 | |
| Unknown | 1 | 0.56 | 1 | 2.63 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | |
| Service branch | Army | 33 | 18.33 | 4 | 10.53 | 6 | 24.00 | 21 | 22.34 | 2 | 8.70 |
| Army National Guard | 62 | 34.44 | 15 | 39.47 | 10 | 40.00 | 26 | 27.66 | 11 | 47.83 | |
| Air Force | 9 | 5.00 | 1 | 2.63 | 2 | 8.00 | 5 | 5.32 | 1 | 4.35 | |
| Air Force National Guard | 7 | 3.89 | 2 | 5.26 | 1 | 4.00 | 3 | 3.19 | 1 | 4.35 | |
| Coast Guard | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | 0 | 0.00 | |
| Navy | 7 | 3.89 | 1 | 2.63 | 1 | 4.00 | 5 | 5.32 | 0 | 0.00 | |
| Marines | 38 | 21.11 | 5 | 13.16 | 4 | 16.00 | 27 | 28.72 | 2 | 8.70 | |
| Reserves | 25 | 13.89 | 10 | 26.32 | 2 | 8.00 | 9 | 9.57 | 4 | 17.39 | |
| National Guard, branch unknown | 6 | 3.33 | 1 | 2.63 | 0 | 0.00 | 3 | 3.19 | 2 | 8.70 | |
| Psychiatric diagnoses | Lifetime PTSD | 132 | 73.33 | 38 | 100.00 | 0 | 0.00 | 94 | 100.00 | 0 | 0.00 |
| Lifetime substance use disorder | 118 | 65.56 | 23 | 60.53 | 13 | 52.00 | 72 | 76.60 | 10 | 43.48 | |
| Lifetime mood disorder | 63 | 35.00 | 14 | 36.84 | 4 | 16.00 | 42 | 44.68 | 3 | 13.04 | |
| Lifetime anxiety disorder | 30 | 16.67 | 9 | 23.68 | 3 | 12.00 | 15 | 15.96 | 3 | 13.04 | |
| Psychiatric medication | Antidepressants | 37 | 20.55 | 8 | 21.05 | 1 | 4.00 | 28 | 29.79 | 0 | 0.00 |
| Antiseizure medication | 12 | 6.67 | 2 | 5.26 | 0 | 0.00 | 10 | 10.64 | 0 | 0.00 | |
| Sedatives | 13 | 7.22 | 5 | 13.16 | 1 | 4.00 | 7 | 7.45 | 0 | 0.00 | |
| Pain medication | 61 | 33.89 | 10 | 26.32 | 10 | 40.00 | 38 | 40.43 | 3 | 13.04 | |
| Prazosin | 5 | 2.78 | 0 | 0.00 | 0 | 0.00 | 5 | 5.32 | 0 | 0.00 | |
| mTBI | Military mTBI | 64 | 35.56 | 0 | 0.00 | 7 | 28.00 | 57 | 60.64 | 0 | 0.00 |
| Lifetime mTBI | 119 | 66.11 | 0 | 0.00 | 25 | 100.00 | 94 | 100.00 | 0 | 0.00 | |
| Total Sample | PTSD | mTBI | Comorbid PTSD+mTBI | No History of PTSD or mTBI | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean ± SD | Range | n | Range | Mean ± SD | n | Range | Mean ± SD | n | Range | Mean ± SD | n | Range | Mean ± SD | ||
| PSQI Global | 178 | 8.97 ± 4.46 | 0–20 | 38 | 8.71 ± 4.43 | 0–20 | 25 | 6.68 ± 3.61 | 1–18 | 92 | 10.49 ± 4.23 | 2–18 | 23 | 5.78 ± 3.48 | 0–14 | |
| PSQI 3-factor structure | Sleep efficiency | 179 | 1.23 ± 0.99 | 0–3 | 38 | 1.13 ± 0.98 | 0–3 | 25 | 0.86 ± 0.99 | 0–3 | 93 | 1.46 ± 0.94 | 0–3 | 23 | 0.89 ± 1.07 | 0–3 |
| Perceived sleep quality | 180 | 1.31 ± 0.80 | 0–3 | 38 | 1.30 ± 0.73 | 0–3 | 25 | 0.99 ± 0.64 | 0–2.67 | 94 | 1.54 ± 0.82 | 0–3 | 23 | 0.72 ± 0.52 | 0–2 | |
| Daily disturbances | 179 | 1.32 ± 0.62 | 0–3 | 38 | 1.28 ± 0.59 | 0–2.5 | 25 | 1.00 ± 0.48 | 0–2 | 93 | 1.53 ± 0.61 | 0–3 | 23 | 0.91 ± 0.47 | 0–2 | |
| PTSD vs. mTBI vs. Comorbid PTSD+mTBI vs. No history of PTSD or mTBI | Post-hoc PTSD vs. mTBI | Post-hoc PTSD vs. Comorbid PTSD+mTBI | Post-hoc mTBI vs. Comorbid PTSD+mTBI | Post-hoc PTSD vs. No history of PTSD or mTBI | Post-hoc mTBI vs. No history of PTSD or mTBI | Post-hoc Comorbid PTSD+mTBI vs. No history of PTSD or mTBI | ||||||||||
| ANCOVA | ||||||||||||||||
| F(df), | p | η2 | p * | |||||||||||||
| PSQI Global | 11.430(3, 173) | <0.001 | 0.17 | 0.055 | 0.026 | <0.001 | 0.008 | 0.457 | <0.001 | |||||||
| PSQI 3-factor structure | Sleep efficiency | 4.16(3, 174) | 0.007 | 0.07 | 0.259 | 0.078 | 0.006 | 0.339 | 0.894 | 0.012 | ||||||
| Perceived sleep quality | 9.20(3, 175) | <0.001 | 0.14 | 0.112 | 0.091 | 0.001 | 0.004 | 0.224 | <0.001 | |||||||
| Daily disturbances | 10.66(3, 174) | <0.001 | 0.16 | 0.057 | 0.025 | <0.001 | 0.017 | 0.618 | <0.001 | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rojczyk, P.; Seitz-Holland, J.; Kaufmann, E.; Sydnor, V.J.; Kim, C.L.; Umminger, L.F.; Wiegand, T.L.T.; Guenette, J.P.; Zhang, F.; Rathi, Y.; et al. Sleep Quality Disturbances Are Associated with White Matter Alterations in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury. J. Clin. Med. 2023, 12, 2079. https://doi.org/10.3390/jcm12052079
Rojczyk P, Seitz-Holland J, Kaufmann E, Sydnor VJ, Kim CL, Umminger LF, Wiegand TLT, Guenette JP, Zhang F, Rathi Y, et al. Sleep Quality Disturbances Are Associated with White Matter Alterations in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury. Journal of Clinical Medicine. 2023; 12(5):2079. https://doi.org/10.3390/jcm12052079
Chicago/Turabian StyleRojczyk, Philine, Johanna Seitz-Holland, Elisabeth Kaufmann, Valerie J. Sydnor, Cara L. Kim, Lisa F. Umminger, Tim L. T. Wiegand, Jeffrey P. Guenette, Fan Zhang, Yogesh Rathi, and et al. 2023. "Sleep Quality Disturbances Are Associated with White Matter Alterations in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury" Journal of Clinical Medicine 12, no. 5: 2079. https://doi.org/10.3390/jcm12052079
APA StyleRojczyk, P., Seitz-Holland, J., Kaufmann, E., Sydnor, V. J., Kim, C. L., Umminger, L. F., Wiegand, T. L. T., Guenette, J. P., Zhang, F., Rathi, Y., Bouix, S., Pasternak, O., Fortier, C. B., Salat, D., Hinds, S. R., Heinen, F., O’Donnell, L. J., Milberg, W. P., McGlinchey, R. E., ... Koerte, I. K. (2023). Sleep Quality Disturbances Are Associated with White Matter Alterations in Veterans with Post-Traumatic Stress Disorder and Mild Traumatic Brain Injury. Journal of Clinical Medicine, 12(5), 2079. https://doi.org/10.3390/jcm12052079