
Validation of an Automated Artificial Intelligence Algorithm for the Quantification of Major OCT Parameters in Diabetic Macular Edema


 ,
,  , , , , ,
, , , , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Dataset
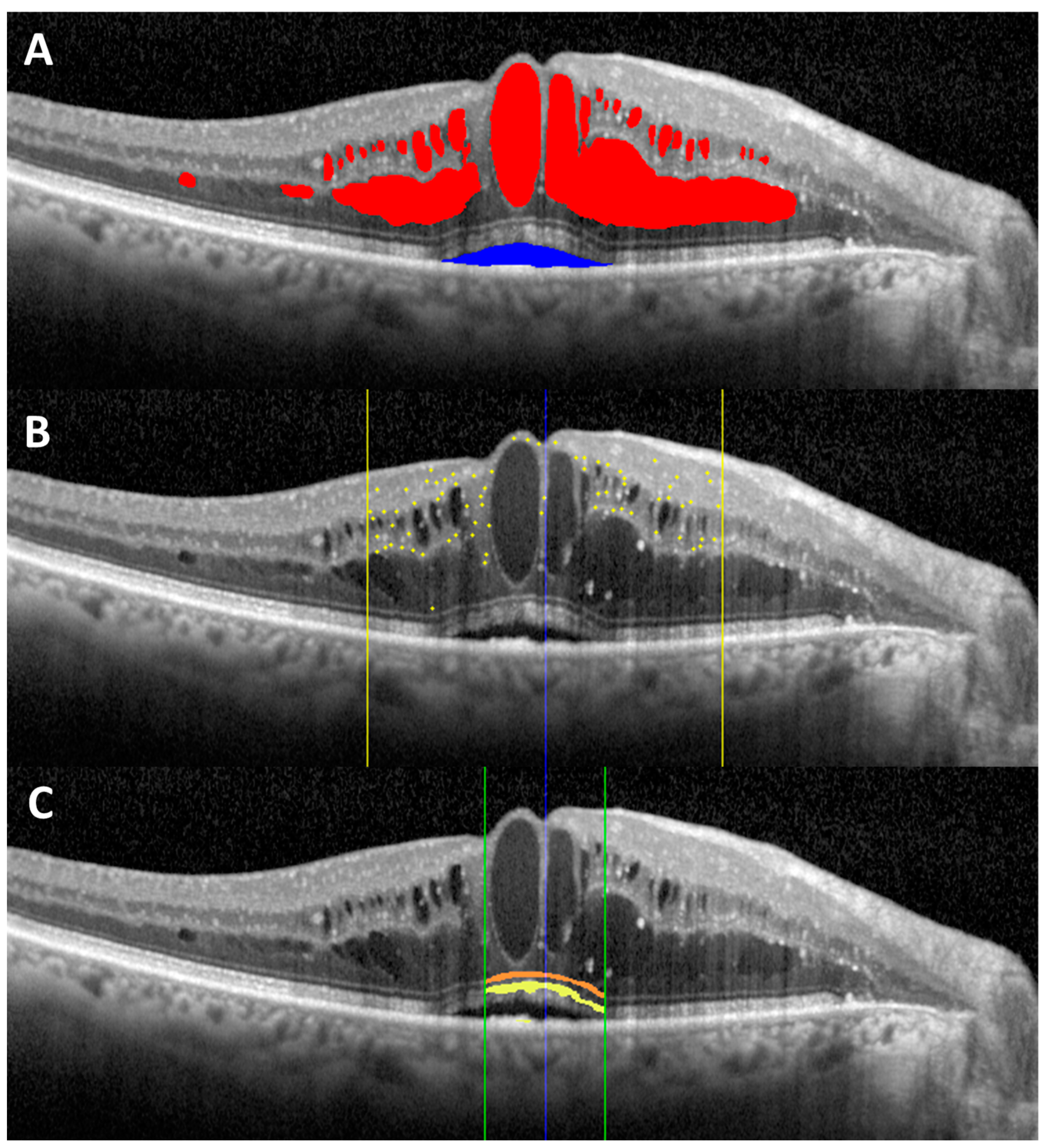
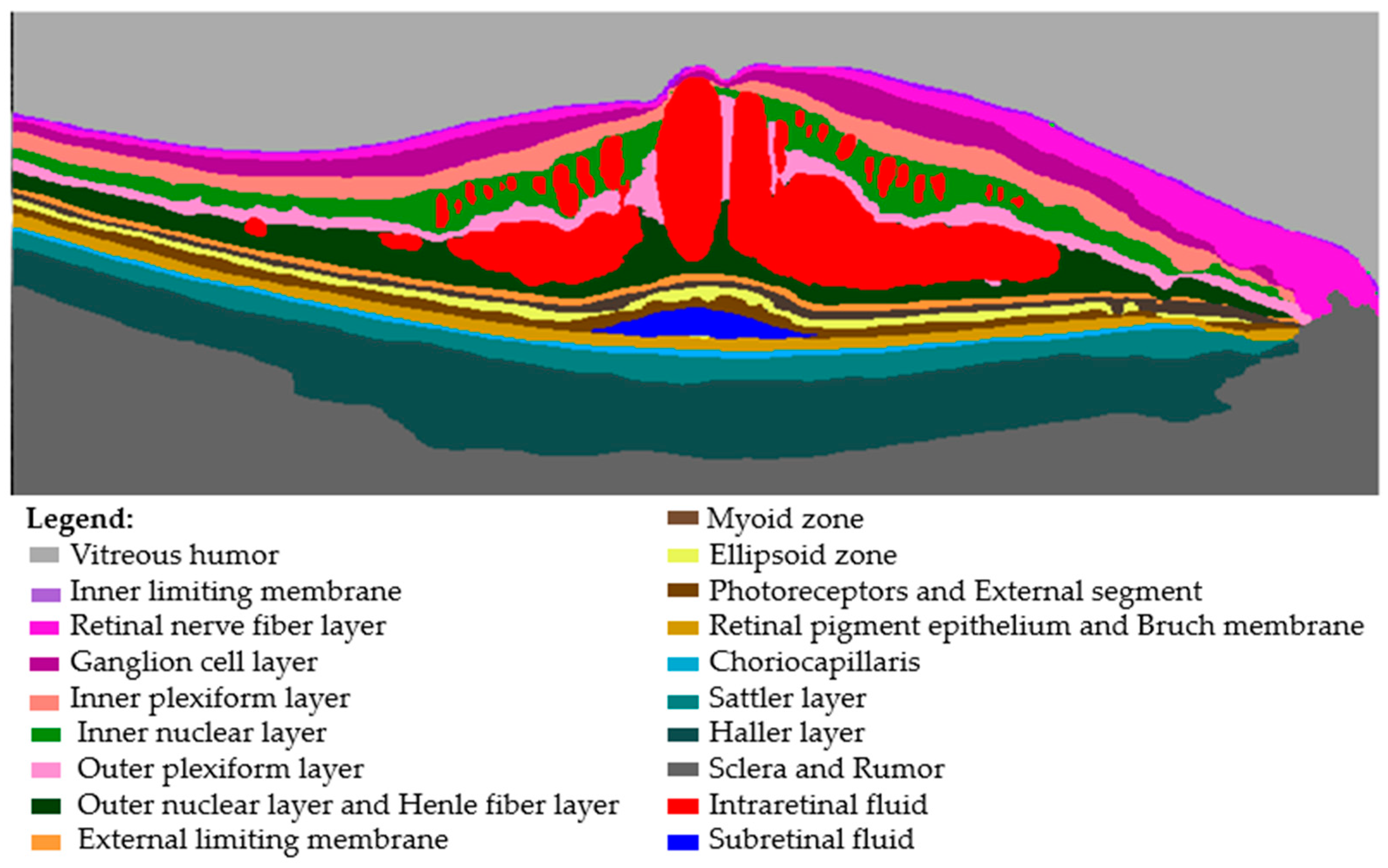
2.2. AI Algorithm Description and Analysis
2.3. Clinical Evaluation
2.4. Outcomes
2.5. Statistical Analysis
3. Results
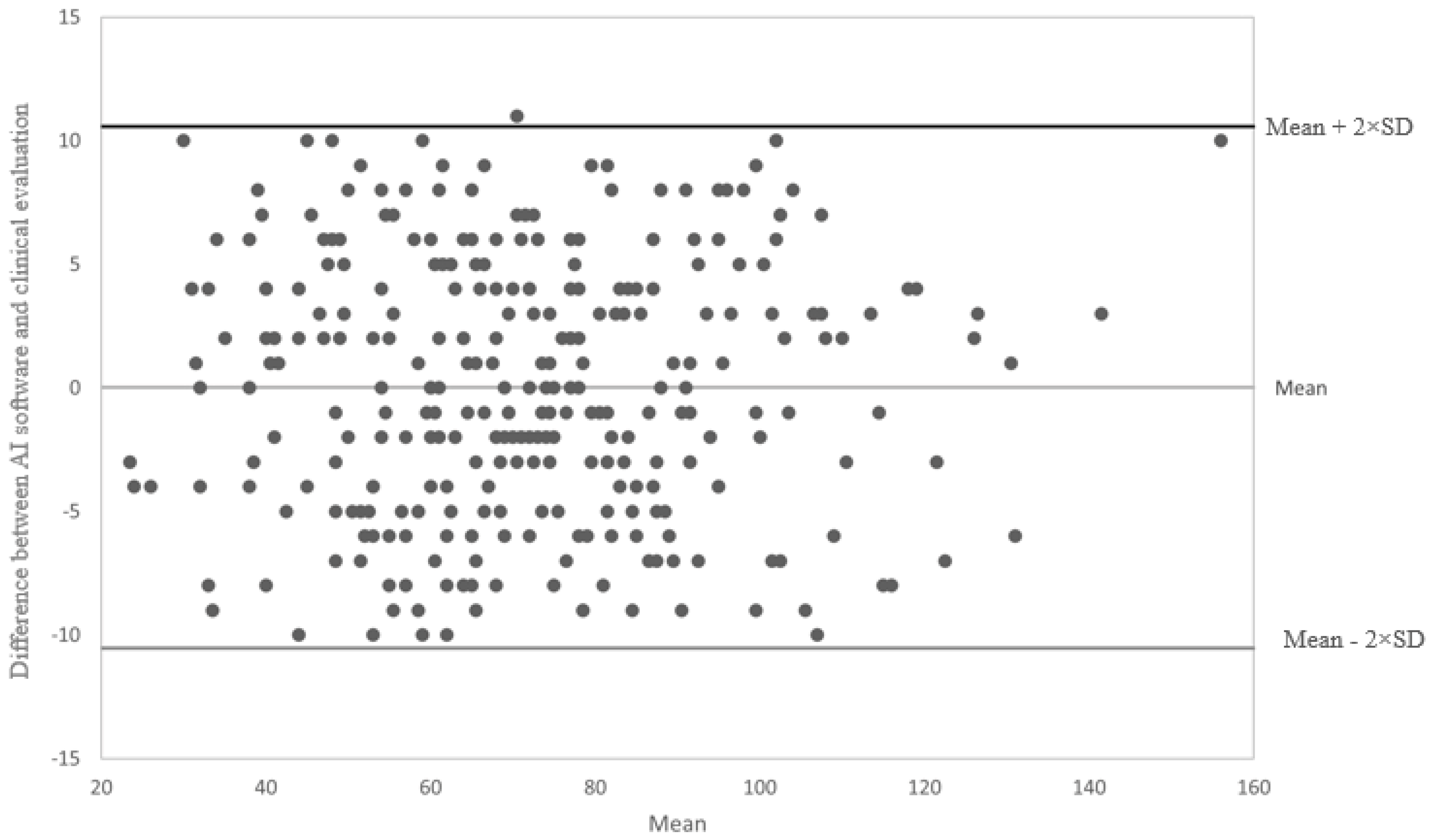
3.1. Agreement between AI Software and Clinical Evaluation
3.2. Quantification Accuracy
3.3. Quality Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Teo, Z.L.; Tham, Y.C.; Yu, M.; Chee, M.L.; Rim, T.H.; Cheung, N.; Bikbov, M.M.; Wang, Y.X.; Tang, Y.; Lu, Y.; et al. Global Prevalence of Diabetic Retinopathy and Projection of Burden through 2045: Systematic Review and Meta-analysis. Ophthalmology 2021, 128, 1580–1591. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Xu, Y.; Zha, M.; Zhang, Y.; Rudan, I. Global epidemiology of retinal vein occlusion: A systematic review and meta-analysis of prevalence, incidence, and risk factors. J. Glob. Health 2019, 9, 010427. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. About Diabetes: Diabetes Facts and Figures. Available online: https://www.idf.org/aboutdiabetes/what-is-diabetes/facts-figures.html (accessed on 27 January 2023).
- Li, J.Q.; Welchowski, T.; Schmid, M.; Letow, J.; Wolpers, C.; Pascual-Camps, I.; Holz, F.G.; Finger, R.P. Prevalence, incidence and future projection of diabetic eye disease in Europe: A systematic review and meta-analysis. Eur. J. Epidemiol. 2020, 35, 11–23. [Google Scholar] [CrossRef]
- Das, A.; McGuire, P.G.; Rangasamy, S. Diabetic Macular Edema: Pathophysiology and Novel Therapeutic Targets. Ophthalmology 2015, 122, 1375–1394. [Google Scholar] [CrossRef]
- Daruich, A.; Matet, A.; Moulin, A.; Kowalczuk, L.; Nicolas, M.; Sellam, A.; Rothschild, P.R.; Omri, S.; Gélizé, E.; Jonet, L.; et al. Mechanisms of macular edema: Beyond the surface. Prog. Retin. Eye Res. 2018, 63, 20–68. [Google Scholar] [CrossRef] [PubMed]
- Hui, V.W.M.; Szeto, S.K.F.; Tang, F.; Yang, D.M.; Chen, H.; Lai, T.Y.M.; Rong, A.; Zhang, S.M.; Zhao, P.M.; Ruamviboonsuk, P.; et al. Optical Coherence Tomography Classification Systems for Diabetic Macular Edema and Their Associations With Visual Outcome and Treatment Responses—An Updated Review. Asia-Pac. J. Ophthalmol. 2022, 11, 247–257. [Google Scholar] [CrossRef]
- Midena, E.; Pilotto, E. Emerging Insights into Pathogenesis. Dev. Ophthalmol. 2017, 60, 16–27. [Google Scholar] [CrossRef]
- Midena, E.; Bini, S. Multimodal retinal imaging of diabetic macular edema: Toward new paradigms of pathophysiology. Graefe's Arch. Clin. Exp. Ophthalmol. 2016, 254, 1661–1668. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.M.; Wolfson, Y.; Bressler, S.B.; Do, D.V.; Ying, H.S.; Bressler, N.M. Comparison of time- and spectral-domain optical coherence tomography in management of diabetic macular edema. Investig. Opthalmology Vis. Sci. 2014, 55, 1370–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuenca, N.; Ortuno-Lizaran, I.; Sanchez-Saez, X.; Kutsyr, O.; Albertos-Arranz, H.; Fernandez-Sanchez, L.; Martinez-Gil, N.; Noailles, A.; López-Garrido, J.A.; Lopez-Galvez, M.; et al. Interpretation of OCT and OCTA images from a histological approach: Clinical and experimental implications. Prog. Retin. Eye Res. 2020, 77, 100828. [Google Scholar] [CrossRef]
- Vujosevic, S.; Bini, S.; Torresin, T.; Berton, M.; Midena, G.; Parrozzani, R.; Martini, F.; Pucci, P.; Daniele, A.R.; Cavarzeran, F.; et al. Hyperreflective Retinal Spots in Normal and Diabetic Eyes: B-Scan and En Face Spectral Domain Optical Coherence Tomography Evaluation. Retina 2017, 37, 1092–1103. [Google Scholar] [CrossRef] [PubMed]
- Vujosevic, S.; Torresin, T.; Bini, S.; Convento, E.; Pilotto, E.; Parrozzani, R.; Midena, E. Imaging retinal inflammatory biomarkers after intravitreal steroid and anti-VEGF treatment in diabetic macular oedema. Acta Ophthalmol. 2017, 95, 464–471. [Google Scholar] [CrossRef] [PubMed]
- Zur, D.; Iglicki, M.; Busch, C.; Invernizzi, A.; Mariussi, M.; Loewenstein, A.; International Retina Group. OCT Biomarkers as Functional Outcome Predictors in Diabetic Macular Edema Treated with Dexamethasone Implant. Ophthalmology 2018, 125, 267–275. [Google Scholar] [CrossRef]
- Midena, E.; Pilotto, E.; Bini, S. Hyperreflective Intraretinal Foci as an OCT Biomarker of Retinal Inflammation in Diabetic Macular Edema. Investig. Opthalmology Vis. Sci. 2018, 59, 5366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Midena, E.; Torresin, T.; Velotta, E.; Pilotto, E.; Parrozzani, R.; Frizziero, L. OCT Hyperreflective Retinal Foci in Diabetic Retinopathy: A Semi-Automatic Detection Comparative Study. Front. Immunol. 2021, 12, 613051. [Google Scholar] [CrossRef]
- Szeto, S.K.; Hui, V.W.K.; Tang, F.Y.; Yang, D.; Sun, Z.H.; Mohamed, S.; Chan, C.K.M.; Lai, T.Y.Y.; Cheung, C. OCT-based biomarkers for predicting treatment response in eyes with centre-involved diabetic macular oedema treated with anti-VEGF injections: A real-life retina clinic-based study. Br. J. Ophthalmol. 2021, in press. [Google Scholar] [CrossRef]
- Huang, Y.-T.; Chang, Y.-C.; Meng, P.-P.; Lin, C.-J.; Lai, C.-T.; Hsia, N.-Y.; Chen, H.-S.; Tien, P.-T.; Bair, H.; Lin, J.-M.; et al. Optical Coherence Tomography Biomarkers in Predicting Treatment Outcomes of Diabetic Macular Edema After Dexamethasone Implants. Front. Med. 2022, 9, 852022. [Google Scholar] [CrossRef]
- Zhou, J.; Song, S.; Zhang, Y.; Jin, K.; Ye, J. OCT-Based Biomarkers are Associated with Systemic Inflammation in Patients with Treatment-Naïve Diabetic Macular Edema. Ophthalmol. Ther. 2022, 11, 2153–2167. [Google Scholar] [CrossRef]
- Schmidt-Erfurth, U.; Sadeghipour, A.; Gerendas, B.S.; Waldstein, S.M.; Bogunović, H. Artificial intelligence in retina. Prog. Retin. Eye Res. 2018, 67, 1–29. [Google Scholar] [CrossRef]
- Chakroborty, S.; Gupta, M.; Devishamani, C.S.; Patel, K.; Ankit, C.; Babu, T.G.; Raman, R. Narrative review of artificial intelligence in diabetic macular edema: Diagnosis and predicting treatment response using optical coherence tomography. Indian J. Ophthalmol. 2021, 69, 2999–3008. [Google Scholar] [CrossRef]
- Shahriari, M.H.; Sabbaghi, H.; Asadi, F.; Hosseini, A.; Khorrami, Z. Artificial intelligence in screening, diagnosis, and classification of diabetic macular edema: A systematic review. Surv. Ophthalmol. 2023, 68, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Schlegl, T.; Waldstein, S.M.; Bogunovic, H.; Endstraßer, F.; Sadeghipour, A.; Philip, A.M.; Podkowinski, D.; Gerendas, B.S.; Langs, G.; Schmidt-Erfurth, U. Fully Automated Detection and Quantification of Macular Fluid in OCT Using Deep Learning. Ophthalmology 2018, 125, 549–558. [Google Scholar] [CrossRef] [Green Version]
- Habra, O.; Gallardo, M.; Meyer, Z.; Westram, T.; De Zanet, S.; Jaggi, D.; Zinkernagel, M.; Wolf, S.; Sznitman, R. Evaluation of an Artificial Intelligence-based Detector of Sub- and Intra-Retinal Fluid on a large set of OCT volumes in AMD and DME. Ophthalmologica 2022, 245, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Roberts, P.K.; Vogl, W.-D.; Gerendas, B.S.; Glassman, A.R.; Bogunovic, H.; Jampol, L.M.; Schmidt-Erfurth, U.M. Quantification of Fluid Resolution and Visual Acuity Gain in Patients With Diabetic Macular Edema Using Deep Learning: A Post Hoc Analysis of a Randomized Clinical Trial. JAMA Ophthalmol. 2020, 138, 945–953. [Google Scholar] [CrossRef]
- Gerendas, B.S.; Sadeghipour, A.; Michl, M.; Goldbach, F.; Mylonas, G.; Gruber, A.M.; Alten, T.M.; Leingang, O.; Sacu, S.; Bogunovic, H.; et al. Validation of an Automated Fluid Algorithm on Real-World Data of Neovascular Age-Related Macular Degeneration over Five Years. Retina 2022, 42, 1673–1682. [Google Scholar] [CrossRef] [PubMed]
- Jiang, T.; Gradus, J.L.; Rosellini, A.J. Supervised Machine Learning: A Brief Primer. Behav. Ther. 2020, 51, 675–687. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Tavares, J.; Santinha, G.; Rocha, N.P. Age-Friendly Health Care: A Systematic Review. Healthcare 2021, 9, 83. [Google Scholar] [CrossRef]
- Castro-Navarro, V.; Monferrer-Adsuara, C.; Navarro-Palop, C.; Montero-Hernández, J.; Cervera-Taulet, E. Effect of Dexamethasone Intravitreal Implant on Visual Acuity and Foveal Photoreceptor Integrity in Macular Edema Secondary to Retinal Vascular Disease. Ophthalmologica 2021, 244, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Michl, M.; Fabianska, M.; Seeböck, P.; Sadeghipour, A.; Najeeb, B.H.; Bogunovic, H.; Schmidt-Erfurth, U.M.; Gerendas, B.S. Automated quantification of macular fluid in retinal diseases and their response to anti-VEGF therapy. Br. J. Ophthalmol. 2022, 106, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Damian, I.; Nicoară, S.D. SD-OCT Biomarkers and the Current Status of Artificial Intelligence in Predicting Progression from Intermediate to Advanced AMD. Life 2022, 12, 454. [Google Scholar] [CrossRef]
- Bellemo, V.; Lim, G.; Rim, T.H.; Tan, G.S.W.; Cheung, C.Y.; Sadda, S.; He, M.-G.; Tufail, A.; Lee, M.L.; Hsu, W.; et al. Artificial Intelligence Screening for Diabetic Retinopathy: The Real-World Emerging Application. Curr. Diabetes Rep. 2019, 19, 72. [Google Scholar] [CrossRef] [PubMed]
- Shah, P.; Mishra, D.K.; Shanmugam, M.P.; Doshi, B.; Jayaraj, H.; Ramanjulu, R. Validation of Deep Convolutional Neural Network-based algorithm for detection of diabetic retinopathy—Artificial intelligence versus clinician for screening. Indian J. Ophthalmol. 2020, 68, 398–405. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Hardware/Technical Features | Requirements |
|---|---|
| Physical memory space available in the computer | At least 4 GB |
| Operating system | Windows 10 or higher 64-bit |
| RAM memory in the computer | 8 GB or more |
| Input images | Horizontal B scans and/or volumetric scans composed of parallel horizontal B scans |
| Linear scans (High Resolution mode) | ART > 90, Quality Index > 30 |
| Volumetric scans | ART > 12, Quality Index > 28 |
| AI algorithm | Clinicians | p Value a | |
|---|---|---|---|
| IRF, mm3 Mean ± SD Range | 8.98 ± 13.67 0.00–110.7 | N.A. | N.A. |
| SRF *, n (%) Absent Present | 260 (85.8) 43 (14.2) | 264 (87.1) 39 (12.9) | 0.9811 |
| ELM interruption, n (%) Absent Present | 233 (76.9) 70 (23.1) | 236 (77.9) 67 (22.1) | 0.1660 |
| EZ interruption, n (%) Absent Present | 192 (66.4) 111 (36.6) | 195 (64.4) 108 (35.6) | 0.1646 |
| HRF, n Mean ± SD Range | 71.9 ± 22.8 22.0–161.0 | 71.9 ± 22.7 25.0–151.0 | 1.0000 b |
| Parameter | + + | + − | − + | − − | p0 | BI | PI | Kappa | PABAK | AC1 |
|---|---|---|---|---|---|---|---|---|---|---|
| SRF | 35 | 8 | 4 | 256 | 0.96 | 0.01 | 0.73 | 0.83 (0.74–0.92) | 0.92 (0.88–0.97) | 0.95 (0.92–0.98) |
| ELM | 65 | 5 | 2 | 231 | 0.98 | 0.01 | 0.55 | 0.93 (0.89–0.98) | 0.95 (0.92–0.99) | 0.96 (0.94–0.99) |
| EZ | 105 | 6 | 3 | 189 | 0.97 | 0.01 | 0.28 | 0.94 (0.89–0.98) | 0.94 (0.90–0.98) | 0.95 (0.91–0.98) |
| SD-OCT Measurements | ||||||
|---|---|---|---|---|---|---|
| Biomarker, n (%) | Among Centers | p a | Overall | |||
| Center 1 | Center 2 | Center 3 | Center 4 | |||
| IRF Accurate Not-accurate | 71 (94.7) 4 (5.3) | 77 (98.7) 1 (1.3) | 71 (94.7) 4 (5.3) | 70 (93.3) 5 (6.7) | 0.3543 | 289 (95.4) 14 (4.6) |
| SRF Accurate Not-accurate | 71 (94.7) 4 (5.3) | 74 (94.9) 4 (5.1) | 68 (90.7) 7 (9.3) | 74 (98.7) 1 (1.3) | 0.1808 | 287 (94.7) 16 (5.3) |
| ELM Accurate Not-accurate | 72 (96.0) 3 (4.0) | 74 (94.9) 4 (5.19 | 71 (94.7) 4 (5.3) | 73 (97.3) 2 (2.7) | 0.9241 | 290 (95.7) 13 (84.3) |
| EZ Accurate Not-accurate | 72 (96.0) 3 (4.0) | 74 (94.9) 4 (5.1) | 71 (94.7) 4 (5.3) | 71 (94.7) 4 (5.3) | 1.0000 | 288 (95.1) 15 (4.9) |
| SD-OCT Quality Parameters | ||||||
| Among Centers | p a | Overall | ||||
| Center 1 | Center 2 | Center 3 | Center 4 | |||
| FCM Accurate Not-accurate | 75 (100.0) 0 (0.0) | 78 (100.0) 0 (0.0) | 74 (98.7) 1 (1.39) | 75 (100.0) 0 (0.0) | 0.7426 | 302 (99.7) 1 (0.3) |
| FCL Accurate Not-accurate | 75 (100.0) 0 (0.0) | 78 (100.0) 0 (0.0) | 75 (100.0) 0 (0.0) | 75 (100.0) 0 (0.0) | 1.0000 | 303 (100.0) 0 (0.0) |
| LSM Accurate Not-accurate | 72 (96.0) 3 (4.0) | 78 (100.0) 0 (0.0) | 75 (100.0) 0 (0.0) | 75. (100.0) 0 (0.0) | 0.0441 | 300 (99.0) 3 (1.0) |
| LSL Accurate Not-accurate | 74 (98.7) 1 (1.39) | 78 (100.0) 0 (0.0) | 75 (100.0) 0 (0.0) | 75 (100.0) 0 (0.0) | 0.7426 | 302 (99.7) 1 (0.3) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Midena, E.; Toto, L.; Frizziero, L.; Covello, G.; Torresin, T.; Midena, G.; Danieli, L.; Pilotto, E.; Figus, M.; Mariotti, C.; et al. Validation of an Automated Artificial Intelligence Algorithm for the Quantification of Major OCT Parameters in Diabetic Macular Edema. J. Clin. Med. 2023, 12, 2134. https://doi.org/10.3390/jcm12062134
Midena E, Toto L, Frizziero L, Covello G, Torresin T, Midena G, Danieli L, Pilotto E, Figus M, Mariotti C, et al. Validation of an Automated Artificial Intelligence Algorithm for the Quantification of Major OCT Parameters in Diabetic Macular Edema. Journal of Clinical Medicine. 2023; 12(6):2134. https://doi.org/10.3390/jcm12062134
Chicago/Turabian StyleMidena, Edoardo, Lisa Toto, Luisa Frizziero, Giuseppe Covello, Tommaso Torresin, Giulia Midena, Luca Danieli, Elisabetta Pilotto, Michele Figus, Cesare Mariotti, and et al. 2023. "Validation of an Automated Artificial Intelligence Algorithm for the Quantification of Major OCT Parameters in Diabetic Macular Edema" Journal of Clinical Medicine 12, no. 6: 2134. https://doi.org/10.3390/jcm12062134
APA StyleMidena, E., Toto, L., Frizziero, L., Covello, G., Torresin, T., Midena, G., Danieli, L., Pilotto, E., Figus, M., Mariotti, C., & Lupidi, M. (2023). Validation of an Automated Artificial Intelligence Algorithm for the Quantification of Major OCT Parameters in Diabetic Macular Edema. Journal of Clinical Medicine, 12(6), 2134. https://doi.org/10.3390/jcm12062134