
Nail Apparatus Melanoma: Current Management and Future Perspectives


Abstract
:1. Introduction
2. Materials and Methods
3. Epidemiology
4. Diagnosis
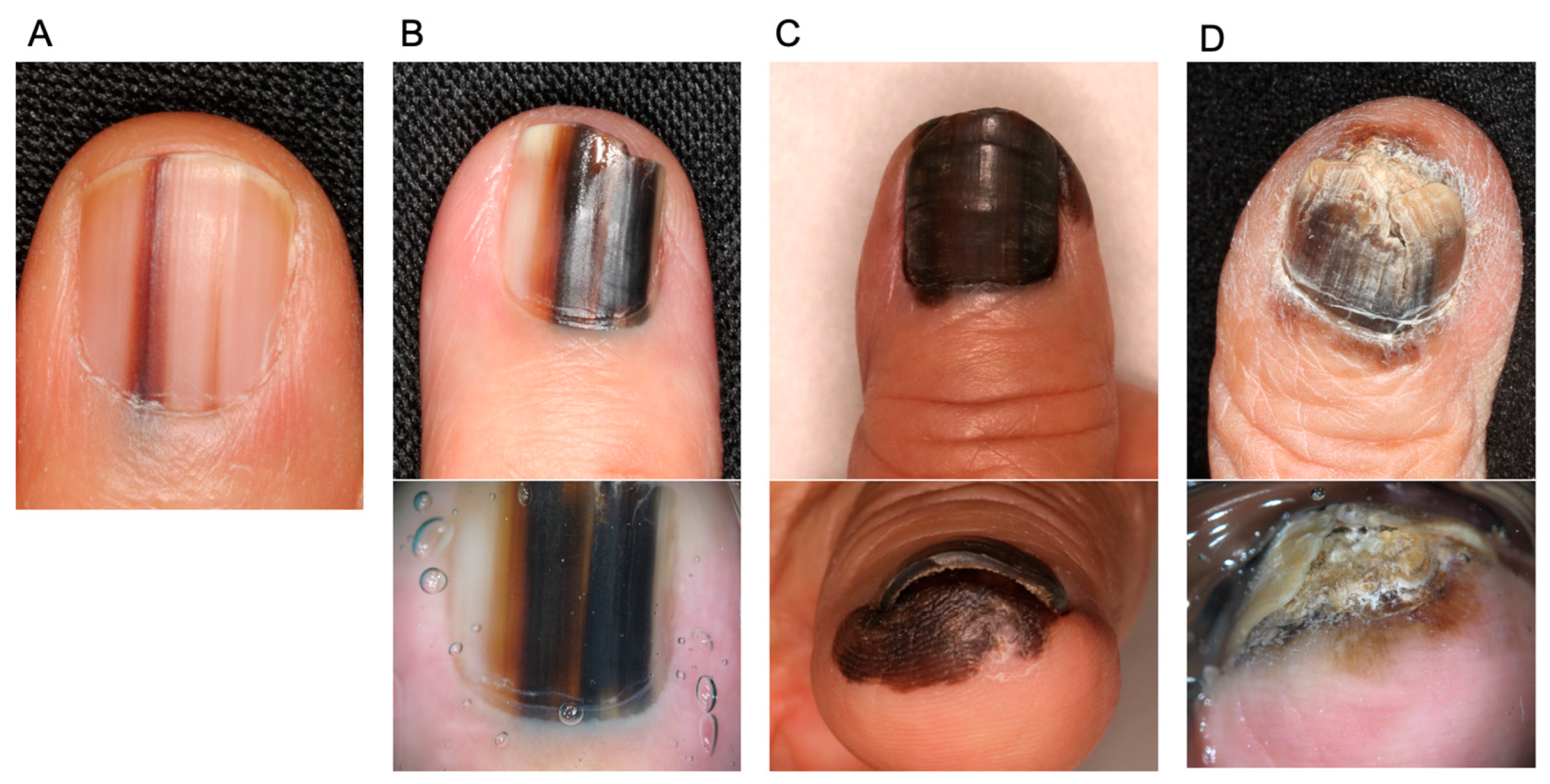
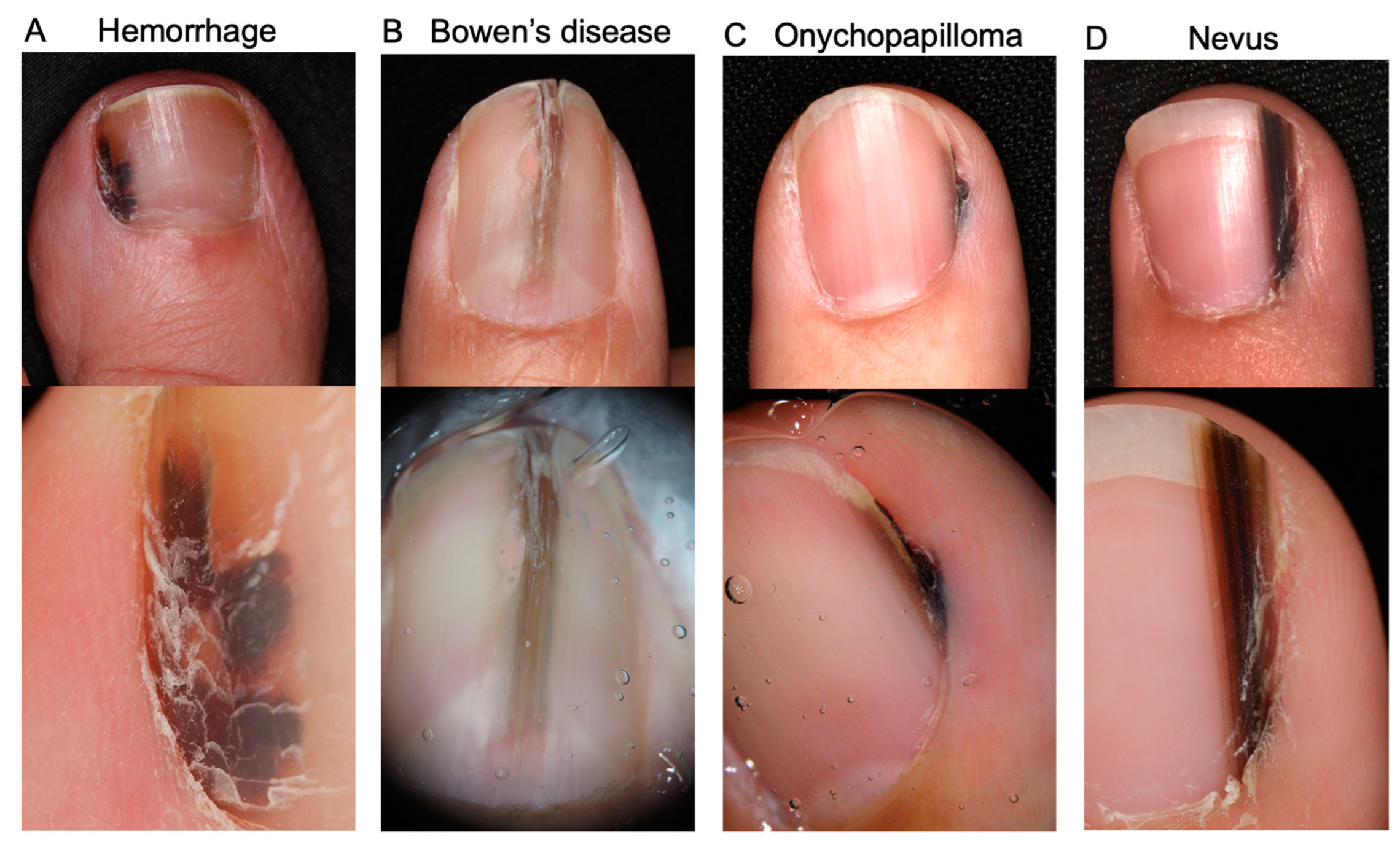
4.1. Clinical Findings
4.2. Treatment of Obtained Samples
4.3. Histopathological Findings
4.4. Genetic Findings
5. Treatment
5.1. Surgical Management
5.1.1. Surgery for Primary Tumor
5.1.2. Sentinel Lymph Node Biopsy
5.1.3. Completion Lymph Node Dissection
5.2. Systemic Adjuvant Therapy for Resected NAM
5.3. Systemic Therapy for Metastatic NAM
5.3.1. Immune Checkpoint Inhibitors
5.3.2. Targeted Therapy
5.3.3. New Classes of Therapeutic Antibodies
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Falotico, J.M.; Lipner, S.R. The pharmacotherapeutic management of nail unit and acral melanomas. Expert Opin. Pharmacother. 2022, 23, 1273–1289. [Google Scholar] [CrossRef] [PubMed]
- Kibbi, N.; Kluger, H.; Choi, J.N. Melanoma: Clinical presentations. Melanoma 2015, 167, 107–129. [Google Scholar] [CrossRef]
- Bradford, P.T.; Goldstein, A.M.; McMaster, M.L.; Tucker, M.A. Acral lentiginous melanoma: Incidence and survival patterns in the United States, 1986–2005. Arch. Dermatol. 2009, 145, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, M.A.; Adamson, A.S.; Halpern, A.C. Melanoma and racial health disparities in black individuals-facts, fallacies, and fixes. JAMA Dermatol. 2021, 157, 1031–1032. [Google Scholar] [CrossRef]
- De Giorgi, V.; Saggini, A.; Grazzini, M.; Gori, A.; Rossari, S.; Scarfì, F.; Verdelli, A.; Chimenti, S.; Lotti, T.; Massi, D. Specific challenges in the management of subungual melanoma. Expert Rev. Anticancer. Ther. 2011, 11, 749–761. [Google Scholar] [CrossRef]
- Nevares-Pomales, O.W.; Sarriera-Lazaro, C.J.; Barrera-Llaurador, J.; Santiago-Vazquez, M.; Lugo-Fagundo, N.; Sanchez, J.E.; Sanchez, J.L. Pigmented lesions of the nail unit. Am. J. Dermatopathol. 2018, 40, 793–804. [Google Scholar] [CrossRef]
- Tosti, A.; Piraccini, B.M.; Cagalli, A.; Haneke, E. In situ melanoma of the nail unit in children: Report of two cases in fair-skinned caucasian children. Pediatr. Dermatol. 2011, 29, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Iorizzo, M.; Tosti, A.; Di Chiacchio, N.; Hirata, S.H.; Misciali, C.; Michalany, N.; Domiguez, J.; Toussaint, S. Nail melanoma in children: Differential diagnosis and management. Dermatol. Surg. 2008, 34, 974–978. [Google Scholar] [CrossRef]
- Levit, E.K.; Kagen, M.H.; Scher, R.K.; Grossman, M.; Altman, E. The ABC rule for clinical detection of subungual melanoma. J. Am. Acad. Dermatol. 2000, 42, 269–274. [Google Scholar] [CrossRef]
- Jellinek, N.J.; Lipner, S.R. Longitudinal erythronychia: Retrospective single-center study evaluating differential diagnosis and the likelihood of malignancy. Dermatol. Surg. 2016, 42, 310–319. [Google Scholar] [CrossRef]
- Phan, A.; Touzet, S.; Dalle, S.; Ronger-Savlé, S.; Balme, B.; Thomas, L. Acral lentiginous melanoma: A clinicoprognostic study of 126 cases. Br. J. Dermatol. 2006, 155, 561–569. [Google Scholar] [CrossRef]
- Kuchelmeister, C.; Schaumburg-Lever, G.; Garbe, C. Acral cutaneous melanoma in caucasians: Clinical features, histopathology and prognosis in 112 patients. Br. J. Dermatol. 2000, 143, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Nagore, E.; Pereda, C.; Botella-Estrada, R.; Requena, C.; Guillén, C. Acral lentiginous melanoma presents distinct clinical profile with high cancer susceptibility. Cancer Causes Control 2008, 20, 115–119. [Google Scholar] [CrossRef]
- Jung, H.J.; Kweon, S.S.; Lee, J.B.; Lee, S.C.; Yun, S.J. A clinicopathologic analysis of 177 acral melanomas in Koreans: Relevance of spreading pattern and physical stress. JAMA Dermatol. 2013, 149, 1281–1288. [Google Scholar]
- Minagawa, A.; Omodaka, T.; Okuyama, R. Melanomas and mechanical stress points on the plantar surface of the foot. N. Engl. J. Med. 2016, 374, 2404–2406. [Google Scholar] [CrossRef] [Green Version]
- Sheen, Y.-S.; Liao, Y.-H.; Lin, M.-H.; Chen, J.-S.; Liau, J.-Y.; Tseng, Y.-J.; Lee, C.-H.; Chang, Y.-L.; Chu, C.-Y. A clinicopathological analysis of 153 acral melanomas and the relevance of mechanical stress. Sci. Rep. 2017, 7, 1–6. [Google Scholar] [CrossRef]
- Choi, M.E.; Cho, H.; Won, C.H.; Chang, S.E.; Lee, M.W.; Lee, W.J. Clinicopathologic characteristics of trauma-related nail apparatus melanoma: A comparative study according to the presence of trauma prior to melanoma development. Dermatology 2022, 239, 165–173. [Google Scholar] [CrossRef]
- Holman, B.N.; Van Gulick, R.J.; Amato, C.M.; Macbeth, M.L.; Davies, K.D.; Aisner, D.L.; Robinson, W.A.; Couts, K.L. Clinical and molecular features of subungual melanomas are site-specific and distinct from acral melanomas. Melanoma Res. 2020, 30, 562–573. [Google Scholar] [CrossRef] [PubMed]
- Teramoto, Y.; Keim, U.; Gesierich, A.; Schuler, G.; Fiedler, E.; Tüting, T.; Ulrich, C.; Wollina, U.; Hassel, J.; Gutzmer, R.; et al. Acral lentiginous melanoma: A skin cancer with unfavourable prognostic features. A study of the German central malignant melanoma registry (CMMR) in 2050 patients. Br. J. Dermatol. 2017, 178, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.; Kim, H.; Kwon, S.T.; Jo, S.J.; Mun, J.-H.; Lee, C.; Kwak, Y.; Kim, B.J. Tumor invasion in the hyponychium is associated with distant metastasis and poor prognosis in subungual melanoma: A histologic landscape of 44 cases. J. Am. Acad. Dermatol. 2021, 86, 1027–1034. [Google Scholar] [CrossRef]
- Wei, X.; Wu, D.; Li, H.; Zhang, R.; Chen, Y.; Yao, H.; Chi, Z.; Sheng, X.; Cui, C.; Bai, X.; et al. The clinicopathological and survival profiles comparison across primary sites in acral melanoma. Ann. Surg. Oncol. 2020, 27, 3478–3485. [Google Scholar] [CrossRef]
- Weber, P.; Tschandl, P.; Sinz, C.; Kittler, H. Dermatoscopy of neoplastic skin lesions: Recent advances, updates, and revisions. Curr. Treat. Options Oncol. 2018, 19, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Darmawan, C.C.; Ohn, J.; Mun, J.; Kim, S.; Lim, Y.; Jo, S.J.; Kim, Y.; Kim, B.; Seong, M.; Lee, C.; et al. Diagnosis and treatment of nail melanoma: A review of the clinicopathologic, dermoscopic, and genetic characteristics. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 651–660. [Google Scholar] [CrossRef]
- Mannava, K.A.; Mannava, S.; Koman, L.A.; Robinson-Bostom, L.; Jellinek, N. Longitudinal melanonychia: Detection and management of nail melanoma. Hand Surg. 2013, 18, 133–139. [Google Scholar] [CrossRef]
- Barros, A.M.; Duarte, A.F.; Haneke, E.; Correia, O.; Ventura, F. Nail melanoma in situ: Clinical, dermoscopic, pathologic clues, and steps for minimally invasive treatment. Dermatol. Surg. 2015, 41, 59–68. [Google Scholar] [CrossRef]
- Goettmann, S.; Moulonguet, I.; Zaraa, I. In situ nail unit melanoma: Epidemiological and clinic-pathologic features with conservative treatment and long-term follow-up. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 2300–2306. [Google Scholar] [CrossRef]
- Thomas, L.; Dalle, S. Dermoscopy provides useful information for the management of melanonychia striata. Dermatol. Ther. 2007, 20, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Benati, E.; Ribero, S.; Longo, C.; Piana, S.; Puig, S.; Carrera, C.; Cicero, F.; Kittler, H.; Deinlein, T.; Zalaudek, I.; et al. Clinical and dermoscopic clues to differentiate pigmented nail bands: An international dermoscopy society study. J. Eur. Acad. Dermatol. Venereol. 2016, 31, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Ohn, J.; Choe, Y.S.; Mun, J.-H. Dermoscopic features of nail matrix nevus (NMN) in adults and children: A comparative analysis. J. Am. Acad. Dermatol. 2016, 75, 535–540. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Uchi, H.; Yamada, Y.; Oda, Y.; Furue, M. Onychopapilloma manifesting longitudinal melanonychia: A mimic of subungual malignancy. J. Dermatol. 2015, 42, 1199–1201. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Ito, T.; Yamada, Y.; Oda, Y.; Furue, M. Onychopapilloma presenting as longitudinal melanonychia: A case report and literature review. Australas. J. Dermatol. 2021, 62, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Peruilh-Bagolini, L.; Dossi, M.T.; Wortsman, X.; Montero, T. Pigmented onychomatricoma: A clinical simulator that could not mislead ultrasound. Acta Bio-Med. Atenei Parm. 2021, 92, e2021158–e20211582021. [Google Scholar] [CrossRef]
- Orchard, G.E.; Torres, J.; Sounthararajah, R. Use of softening agents to improve the production of formalin-fixed, paraffin-embedded sections of nail tissue: An assessment. Br. J. Biomed. Sci. 2008, 65, 68–70. [Google Scholar] [CrossRef] [PubMed]
- Orchard, G.E.; Torres, J.; Poirier, A.; Sounthararajah, R.; Webster, J.; Notini, L.; Hacker, L.; Ismail, F.; Nwokie, T.; Humphrey, P.; et al. Investigation into a new softening agent for use on formalin-fixed, paraffin wax-embedded tissue. Br. J. Biomed. Sci. 2009, 66, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Tan, K.B.; Moncrieff, M.; Thompson, J.F.; McCarthy, S.W.; Shaw, H.M.; Quinn, M.J.; Li, L.X.; Crotty, K.A.; Stretch, J.R.; Scolyer, R.A. Subungual melanoma: A study of 124 cases highlighting features of early lesions, potential pitfalls in diagnosis, and guidelines for histologic reporting. Am. J. Surg. Pathol. 2007, 31, 1902–1912. [Google Scholar]
- Yun, S.J.; Bastian, B.C.; Duncan, L.M.; Haneke, E.; Uhara, H. Acral melanoma. In WHO Classification of Skin Tumours, 4th ed.; Elder, D.E., Massi, D., Scolyer, R.A., Willemze, R., Eds.; IARC Press: Lyon, France, 2018; pp. 116–118. [Google Scholar]
- Chu, A.; André, J.; Rich, P.; Leachman, S.; Thompson, C.T. Immunohistochemical characterization of benign activation of junctional melanocytes and melanoma in situ of the nail unit. J. Cutan. Pathol. 2019, 46, 479–483. [Google Scholar] [CrossRef] [Green Version]
- Rothrock, A.T.; Torres-Cabala, C.A.; Milton, D.R.; Cho, W.C.; Nagarajan, P.; Vanderbeck, K.; Curry, J.L.; Ivan, D.; Prieto, V.G.; Aung, P.P. Diagnostic utility of PRAME expression by immunohistochemistry in subungual and non-subungual acral melanocytic lesions. J. Cutan. Pathol. 2022, 49, 859–867. [Google Scholar] [CrossRef]
- Santandrea, G.; Valli, R.; Zanetti, E.; Ragazzi, M.; Pampena, R.; Longo, C.; Lai, M.; Piana, S.; Cesinaro, A.M. Comparative analysis of PRAME expression in 127 acral and nail melanocytic lesions. Am. J. Surg. Pathol. 2022, 46, 579–590. [Google Scholar] [CrossRef]
- Kim, Y.J.; Jung, C.J.; Na, H.; Lee, W.J.; Chang, S.E.; Lee, M.W.; Park, C.-S.; Lim, Y.; Won, C.H. Cyclin D1 and PRAME expression in distinguishing melanoma in situ from benign melanocytic proliferation of the nail unit. Diagn. Pathol. 2022, 17, 1–10. [Google Scholar] [CrossRef]
- Ren, M.; Ren, J.; Cai, X.; Shen, X.X.; Kong, J.C.; Dai, B.; Kong, Y.Y. Clinicopathological, Immunohistochemical and fluorescence in-situ hybridisation features of early subungual melanoma: An analysis of 65 cases. Histopathology 2021, 78, 717–726. [Google Scholar]
- Romano, R.C.; Shon, W.; Sukov, W.R. Malignant melanoma of the nail apparatus: A fluorescence in situ hybridization analysis of 7 cases. Int. J. Surg. Pathol. 2016, 24, 512–518. [Google Scholar]
- Shojiguchi, N.; Takai, S.; Arai, E. Hyperplastic melanocytes with chromosomal aberrations in surrounding skin of subungual melanoma: Fluorescence in situ hybridisation analysis using whole-slide digital imaging. Histopathology 2022, 81, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Curtin, J.A.; Fridlyand, J.; Kageshita, T.; Patel, H.N.; Busam, K.J.; Kutzner, H.; Cho, K.-H.; Aiba, S.; Bröcker, E.-B.; LeBoit, P.E.; et al. Distinct sets of genetic alterations in melanoma. N. Engl. J. Med. 2005, 353, 2135–2147. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, M.S.; Stojanov, P.; Polak, P.; Kryukov, G.V.; Cibulskis, K.; Sivachenko, A.; Carter, S.L.; Stewart, C.; Mermel, C.H.; Roberts, S.A.; et al. Mutational heterogeneity in cancer and the search for new cancer-associated genes. Nature 2013, 499, 214–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayward, N.K.; Wilmott, J.S.; Waddell, N.; Johansson, P.A.; Field, M.A.; Nones, K.; Patch, A.-M.; Kakavand, H.; Alexandrov, L.B.; Burke, H.; et al. Whole-genome landscapes of major melanoma subtypes. Nature 2017, 545, 175–180. [Google Scholar] [CrossRef]
- Lee, M.; Yoon, J.; Chung, Y.-J.; Lee, S.Y.; Choi, J.Y.; Shin, O.R.; Park, H.Y.; Bahk, W.-J.; Yu, D.S.; Lee, Y.B. Whole-exome sequencing reveals differences between nail apparatus melanoma and acral melanoma. J. Am. Acad. Dermatol. 2018, 79, 559–561.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haugh, A.M.; Zhang, B.; Quan, V.L.; Garfield, E.M.; Bubley, J.A.; Kudalkar, E.; Verzi, A.E.; Walton, K.; VandenBoom, T.; Merkel, E.A.; et al. Distinct patterns of acral melanoma based on site and relative sun exposure. J. Investig. Dermatol. 2018, 138, 384–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newell, F.; Wilmott, J.S.; Johansson, P.A.; Nones, K.; Addala, V.; Mukhopadhyay, P.; Broit, N.; Amato, C.M.; Van Gulick, R.; Kazakoff, S.H.; et al. Whole-genome sequencing of acral melanoma reveals genomic complexity and diversity. Nat. Commun. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Dai, B.; Cai, X.; Kong, Y.-Y.; Yang, F.; Shen, X.-X.; Wang, L.-W.; Kong, J.-C. Analysis of KIT expression and gene mutation in human acral melanoma: With a comparison between primary tumors and corresponding metastases/recurrences. Hum. Pathol. 2013, 44, 1472–1478. [Google Scholar] [CrossRef]
- Dika, E.; Altimari, A.; Patrizi, A.; Gruppioni, E.; Fiorentino, M.; Piraccini, B.M.; Misciali, C.; Barisani, A.; Fanti, P.A. KIT, NRAS, and BRAF mutations in nail apparatus melanoma. Pigment. Cell Melanoma Res. 2013, 26, 758–760. [Google Scholar] [CrossRef]
- Sakaizawa, K.; Ashida, A.; Uchiyama, A.; Ito, T.; Fujisawa, Y.; Ogata, D.; Matsushita, S.; Fujii, K.; Fukushima, S.; Shibayama, Y.; et al. Clinical characteristics associated with BRAF, NRAS and KIT mutations in Japanese melanoma patients. J. Dermatol. Sci. 2015, 80, 33–37. [Google Scholar] [CrossRef]
- Moon, K.R.; Choi, Y.D.; Kim, J.M.; Jin, S.; Shin, M.-H.; Shim, H.-J.; Lee, J.-B.; Yun, S.J. Genetic alterations in primary acral melanoma and acral melanocytic nevus in Korea: Common mutated genes show distinct cytomorphological features. J. Investig. Dermatol. 2018, 138, 933–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheen, Y.-S.; Tan, K.-T.; Tse, K.-P.; Liao, Y.-H.; Lin, M.-H.; Chen, J.-S.; Liau, J.-Y.; Tseng, Y.-J.; Lee, C.-H.; Hong, C.-B.; et al. Genetic alterations in primary melanoma in Taiwan. Br. J. Dermatol. 2020, 182, 1205–1213. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Yoon, D.; Lee, D.-Y. Novel mutations identified by whole-exome sequencing in acral melanoma. J. Am. Acad. Dermatol. 2020, 83, 1792–1794. [Google Scholar] [CrossRef] [PubMed]
- Borkowska, A.; Szumera-Ciećkiewicz, A.; Spałek, M.; Teterycz, P.; Czarnecka, A.; Kowalik, A.; Rutkowski, P. Mutation profile of primary subungual melanomas in Caucasians. Oncotarget 2020, 11, 2404–2413. [Google Scholar] [CrossRef]
- Reilly, D.; Aksakal, G.; Gilmour, R.; Gyorki, D.; Chauhan, A.; Webb, A.; Henderson, M. Subungual melanoma: Management in the modern era. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 1746–1752. [Google Scholar] [CrossRef]
- Cochran, A.M.; Buchanan, P.J.; Bueno, R.A., Jr.; Neumeister, M.W. Subungual melanoma: A review of current treatment. Plast. Reconstr. Surg. 2014, 134, 259–273. [Google Scholar]
- Sureda, N.; Phan, A.; Poulalhon, N.; Balme, B.; Dalle, S.; Thomas, L. Conservative surgical management of subungual (matrix derived) melanoma: Report of seven cases and literature review. Br. J. Dermatol. 2011, 165, 852–858. [Google Scholar] [CrossRef]
- Chow, W.; Bhat, W.; Magdub, S.; Orlando, A. In situ subungual melanoma: Digit salvaging clearance. J. Plast. Reconstr. Aesthetic Surg. 2013, 66, 274–276. [Google Scholar] [CrossRef]
- Cohen, T.; Busam, K.J.; Patel, A.; Brady, M.S. Subungual melanoma: Management considerations. Am. J. Surg. 2008, 195, 244–248. [Google Scholar] [CrossRef]
- Zhang, J.; Yun, S.J.; McMurray, S.L.; Miller, C.J. Management of nail unit melanoma. Dermatol. Clin. 2021, 39, 269–280. [Google Scholar] [CrossRef] [PubMed]
- Ogata, D.; Uhara, H.; Tsutsumida, A.; Yamazaki, N.; Mochida, K.; Amano, M.; Yoshikawa, S.; Kiyohara, Y.; Tsuchida, T. Nail apparatus melanoma in a Japanese population: A comparative study of surgical procedures and prognoses in a large series of 151 cases. Eur. J. Dermatol. 2017, 27, 620–626. [Google Scholar] [CrossRef]
- NCCN Guidelines Version 3.2020 Cutaneous Melanoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cutaneous_melanoma.pdf (accessed on 16 June 2020).
- Nakamura, Y.; Asai, J.; Igaki, H.; Inozume, T.; Namikawa, K.; Hayashi, A.; Fukushima, S.; Fujimura, T.; Ito, T.; Imafuku, K.; et al. Japanese dermatological association guidelines: Outlines of guidelines for cutaneous melanoma 2019. J. Dermatol. 2019, 47, 89–103. [Google Scholar] [CrossRef]
- Ito, T.; Kaku-Ito, Y.; Wada-Ohno, M.; Furue, M. Narrow-margin excision for invasive acral melanoma: Is it acceptable? J. Clin. Med. 2020, 9, 2266. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Wada, M.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Acral lentiginous melanoma: Who benefits from sentinel lymph node biopsy? J. Am. Acad. Dermatol. 2015, 72, 71–77. [Google Scholar] [CrossRef] [PubMed]
- LaRocca, C.J.; Lai, L.; Nelson, R.A.; Modi, B.; Crawford, B. Subungual melanoma: A single institution experience. Med. Sci. 2021, 9, 57. [Google Scholar] [CrossRef]
- Ito, T.; Moroi, Y.; Oba, J.; Nakahara, T.; Takeuchi, S.; Uchi, H.; Takahara, M.; Masuda, T.; Furue, M. The prognostic value of a reverse transcriptase-PCR assay of sentinel lymph node biopsy for patients with cutaneous melanoma: A single-center analysis in Japan. Melanoma Res. 2012, 22, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Wada, M.; Ito, T.; Tsuji, G.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Acral lentiginous melanoma versus other melanoma: A single-center analysis in Japan. J. Dermatol. 2017, 44, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Yeh, J.; Shen, S.; Lo, Y.; Kuo, T.; Chang, J.W.C. Regressed subungual melanoma simulating cellular blue nevus: Managed with sentinel lymph node biopsy. Dermatol. Surg. 2006, 32, 577–581. [Google Scholar] [CrossRef]
- Chakera, A.H.; Quinn, M.J.; Lo, S.; Drummond, M.; Haydu, L.E.; Bond, J.S.; Stretch, J.R.; Saw, R.P.M.; Lee, K.J.; McCarthy, W.H.; et al. Subungual melanoma of the hand. Ann. Surg. Oncol. 2018, 26, 1035–1043. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Wada, M.; Nagae, K.; Nakano-Nakamura, M.; Nakahara, T.; Hagihara, A.; Furue, M.; Uchi, H. Triple-marker PCR assay of sentinel lymph node as a prognostic factor in melanoma. J. Eur. Acad. Dermatol. Venereol. 2014, 29, 912–918. [Google Scholar] [CrossRef]
- Faries, M.B.; Thompson, J.F.; Cochran, A.J.; Andtbacka, R.H.; Mozzillo, N.; Zager, J.S.; Jahkola, T.; Bowles, T.L.; Testori, A.; Beitsch, P.D.; et al. Completion dissection or observation for sentinel-node metastasis in melanoma. N. Engl. J. Med. 2017, 376, 2211–2222. [Google Scholar] [CrossRef]
- Leiter, U.; Stadler, R.; Mauch, C.; Hohenberger, W.; Brockmeyer, N.H.; Berking, C.; Sunderkötter, C.; Kaatz, M.; Schatton, K.; Lehmann, P.; et al. German dermatologic cooperative oncology group (2019). Final analysis of DeCOG-SLT trial: No survival benefit for complete lymph node dissection in patients with melanoma with positive sentinel node. J. Clin. Oncol. 2019, 37, 3000–3008. [Google Scholar] [CrossRef] [PubMed]
- Wada-Ohno, M.; Ito, T.; Furue, M. Adjuvant therapy for melanoma. Curr. Treat. Options Oncol. 2019, 20, 63. [Google Scholar] [CrossRef]
- Weber, J.; Mandalà, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant nivolumab versus ipilimumab in resected stage III or IV melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Long, G.V.; Hauschild, A.; Santinami, M.; Atkinson, V.; Mandalà, M.; Chiarion-Sileni, V.; Larkin, J.; Nyakas, M.; Dutriaux, C.; Haydon, A.; et al. Adjuvant dabrafenib plus trametinib in stage III BRAF-mutated melanoma. N. Engl. J. Med. 2017, 377, 1813–1823. [Google Scholar] [CrossRef] [Green Version]
- Luke, P.R.J.J.; Queirolo, P.; Del Vecchio, M.; Mackiewicz, J.; Chiarion Sileni, V.; de la Cruz Merino, L.; Khattak, M.A.; Shadendorf, D.; Long, G.V.; Ascierto, P.A.; et al. LBA3 PR-pembrolizumab versus placebo after complete resection of high-risk stage II melanoma: Efficacy and safety results from the KEYNOTE-716 double-blind phase III trial. Ann. Oncol. 2021, 32, S1283e346. [Google Scholar] [CrossRef]
- Eggermont, A.M.; Blank, C.U.; Mandalà, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.M.; Meshcheryakov, A.; Khattak, M.; Carlino, M.S.; et al. Pembrolizumab versus placebo after complete resection of high-risk stage III melanoma: New recurrence-free survival results from the EORTC 1325-MG/Keynote 054 double-blinded phase III trial at three-year median follow-up. J. Clin. Oncol. 2020, 38, 10000. [Google Scholar] [CrossRef]
- Ascierto, P.A.; Del Vecchio, M.; Mandalá, M.; Gogas, H.; Arance, A.M.; Dalle, S.; Cowey, C.L.; Schenker, M.; Grob, J.J.; Chiarion-Sileni, V.; et al. Adjuvant nivolumab versus ipilimumab in resected stage IIIB-C and stage IV melanoma (CheckMate 238): 4-year results from a multicentre, double-blind, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 1465–1477. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Xu, Y.; Sun, W.; Yan, W.; Wang, C.; Hu, T.; Zhang, X.; Luo, Z.; Liu, X.; Chen, Y. Adjuvant Anti-PD-1 Immunotherapy versus conventional therapy for stage III melanoma: A real-world retrospective cohort study. Pharmaceuticals 2022, 16, 41. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Li, J.; Liu, X.; Wen, X.; Li, D.; Ding, Y.; Jiang, H.; Huang, F.; Zhang, X. Adjuvant PD-1 inhibitor versus high-dose interferon α-2b for Chinese patients with cutaneous and acral melanoma: A retrospective cohort analysis. J. Clin. Oncol. 2021, 39, e21516–e215162021. [Google Scholar] [CrossRef]
- Muto, Y.; Kambayashi, Y.; Kato, H.; Fukushima, S.; Ito, T.; Maekawa, T.; Fujisawa, Y.; Yoshino, K.; Uchi, H.; Matsushita, S.; et al. Adjuvant anti-PD-1 antibody therapy for advanced melanoma: A multicentre study of 78 japanese cases. Acta Derm.-Venereol. 2022, 102, adv00756. [Google Scholar] [CrossRef] [PubMed]
- Maeda, T.; Yanagi, T.; Miyamoto, K.; Tokuchi, K.; Kitamura, S.; Ujiie, H. Adjuvant nivolumab therapy may not improve disease-free survival in resected acral lentiginous melanoma patients: A retrospective case series. Dermatol. Ther. 2022, 35, e15817. [Google Scholar] [CrossRef] [PubMed]
- Furue, M.; Ito, T.; Wada, N.; Wada, M.; Kadono, T.; Uchi, H. Melanoma and immune checkpoint inhibitors. Curr. Oncol. Rep. 2018, 20, 29. [Google Scholar] [CrossRef]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Long-term outcomes with nivolumab plus ipilimumab or nivolumab alone versus ipilimumab in patients with advanced melanoma. J. Clin. Oncol. 2022, 40, 127–137. [Google Scholar] [CrossRef]
- Robert, C.; Grob, J.J.; Stroyakovskiy, D.; Karaszewska, B.; Hauschild, A.; Levchenko, E.; Chiarion Sileni, V.; Schachter, J.; Garbe, C.; Bondarenko, I.; et al. Five-year outcomes with dabrafenib plus trametinib in metastatic melanoma. N. Engl. J. Med. 2019, 381, 626–636. [Google Scholar] [CrossRef]
- Dummer, R.; Flaherty, K.T.; Robert, C.; Arance, A.; de Groot, J.W.B.; Garbe, C.; Gogas, H.J.; Gutzmer, R.; Krajsová, I.; Liszkay, G.; et al. COLUMBUS 5-year update: A randomized, open-label, phase III trial of encorafenib plus binimetinib versus vemurafenib or encorafenib in patients with BRAF V600-mutant melanoma. J. Clin. Oncol. 2022, 40, 4178–4188. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Fujisawa, Y. Diagnosis and management of acral lentiginous melanoma. Curr. Treat. Options Oncol. 2018, 19, 42. [Google Scholar] [CrossRef] [PubMed]
- Yeh, I.; Jorgenson, E.; Shen, L.; Xu, M.; North, J.P.; Shain, A.H.; Reuss, D.; Wu, H.; Robinson, W.A.; Olshen, A.; et al. Targeted genomic profiling of acral melanoma. Gynecol. Oncol. 2019, 111, 1068–1077. [Google Scholar] [CrossRef]
- Broit, N.; Johansson, P.A.; Rodgers, C.B.; Walpole, S.T.; Hayward, N.K.; Pritchard, A.L. Systematic review and meta-analysis of genomic alterations in acral melanoma. Pigment. Cell Melanoma Res. 2022, 35, 369–386. [Google Scholar] [CrossRef]
- Zebary, A.; Omholt, K.; Vassilaki, I.; Höiom, V.; Lindén, D.; Viberg, L.; Kanter-Lewensohn, L.; Johansson, C.H.; Hansson, J. KIT, NRAS, BRAF and PTEN mutations in a sample of Swedish patients with acral lentiginous melanoma. J. Dermatol. Sci. 2013, 72, 284–289. [Google Scholar] [CrossRef] [Green Version]
- Yarchoan, M.; Hopkins, A.; Jaffee, E.M. Tumor mutational burden and response rate to PD-1 inhibition. N. Engl. J. Med. 2017, 377, 2500–2501. [Google Scholar] [CrossRef]
- Cho, K.K.; Cust, A.E.; Foo, Y.M.; Long, G.V.; Menzies, A.M.; Eslick, G.D. Metastatic acral melanoma treatment outcomes: A systematic review and meta-analysis. Melanoma Res. 2021, 31, 482–486. [Google Scholar] [CrossRef]
- Fujimura, T.; Muto, Y.; Asano, Y. Immunotherapy for melanoma: The Significance of immune checkpoint inhibitors for the treatment of advanced melanoma. Int. J. Mol. Sci. 2022, 23, 15720. [Google Scholar] [CrossRef]
- Mao, L.; Qi, Z.; Zhang, L.; Guo, J.; Si, L. Immunotherapy in acral and mucosal melanoma: Current status and future directions. Front. Immunol. 2021, 12, 680407. [Google Scholar] [CrossRef]
- Warner, A.B.; Palmer, J.S.; Shoushtari, A.N.; Goldman, D.A.; Panageas, K.S.; Hayes, S.A.; Bajwa, R.; Momtaz, P.; Callahan, M.K.; Wolchok, J.D.; et al. Long-term outcomes and responses to retreatment in patients with melanoma treated with PD-1 blockade. J. Clin. Oncol. 2020, 38, 1655–1663. [Google Scholar] [CrossRef] [PubMed]
- Ogata, D.; Haydu, L.E.; Glitza, I.C.; Patel, S.P.; Tawbi, H.A.; McQuade, J.L.; Diab, A.; Ekmekcioglu, S.; Wong, M.K.; Davies, M.A.; et al. The efficacy of anti-programmed cell death protein 1 therapy among patients with metastatic acral and metastatic mucosal melanoma. Cancer Med. 2021, 10, 2293–2299. [Google Scholar] [CrossRef] [PubMed]
- Shoushtari, A.N.; Munhoz, R.R.; Kuk, D.; Ott, P.A.; Johnson, D.B.; Tsai, K.K.; Rapisuwon, S.; Eroglu, Z.; Sullivan, R.J.; Luke, J.J.; et al. The efficacy of anti-PD-1 agents in acral and mucosal melanoma. Cancer 2016, 122, 3354–3362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, T.; Yoshino, K.; Nagai, K.; Oaku, S.; Kato, M.; Hiura, A.; Hata, H. Efficacy of nivolumab monotherapy against acral lentiginous melanoma and mucosal melanoma in Asian patients. Br. J. Dermatol. 2018, 180, 1230–1231. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Namikawa, K.; Ogata, D.; Jinnai, S.; Nakano, E.; Yamazaki, N. Updated analysis of nivolumab and ipilimumab combination therapy in Japanese patients with advanced melanoma. J. Dermatol. 2022. [Google Scholar] [CrossRef]
- Namikawa, K.; Kiyohara, Y.; Takenouchi, T.; Uhara, H.; Uchi, H.; Yoshikawa, S.; Takatsuka, S.; Koga, H.; Wada, N.; Minami, H.; et al. Final analysis of a phase II study of nivolumab in combination with ipilimumab for unresectable chemotherapy—Naive advanced melanoma. J. Dermatol. 2020, 47, 1257–1266. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Namikawa, K.; Ogata, D.; Nakano, E.; Jinnai, S.; Nakama, K.; Tsutsui, K.; Muto, Y.; Mizuta, H.; Yamazaki, N. Real-world efficacy and safety data of nivolumab and ipilimumab combination therapy in Japanese patients with advanced melanoma. J. Dermatol. 2020, 47, 1267–1275. [Google Scholar] [CrossRef]
- Si, L.; Zhang, X.; Shu, Y.; Pan, H.; Wu, D.; Liu, J.; Lou, F.; Mao, L.; Wang, X.; Wen, X.; et al. A phase Ib study of pembrolizumab as second-line therapy for Chinese patients with advanced or metastatic melanoma (KEYNOTE-151). Transl. Oncol. 2019, 12, 828–835. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Ding, Y.; Li, J.; Zhao, J.; Peng, R.; Li, D.; Zhu, B.; Wang, Y.; Zhang, X.; Zhang, X. The experience of immune checkpoint inhibitors in Chinese patients with metastatic melanoma: A retrospective case series. Cancer Immunol. Immunother. 2017, 66, 1153–1162. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Namikawa, K.; Yoshino, K.; Yoshikawa, S.; Uchi, H.; Goto, K.; Nakamura, Y.; Fukushima, S.; Kiniwa, Y.; Takenouchi, T.; et al. Anti-PD1 checkpoint inhibitor therapy in acral melanoma: A multicenter study of 193 Japanese patients. Ann. Oncol. 2020, 31, 1198–1206. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, N.; Kiyohara, Y.; Uhara, H.; Tsuchida, T.; Maruyama, K.; Shakunaga, N.; Itakura, E.; Komoto, A. Real-world safety and efficacy data of ipilimumab in Japanese radically unresectable malignant melanoma patients: A postmarketing surveillance. J. Dermatol. 2020, 47, 834–848. [Google Scholar] [CrossRef]
- Nathan, P.; Ascierto, P.A.; Haanen, J.; Espinosa, E.; Demidov, L.; Garbe, C.; Guida, M.; Lorigan, P.; Chiarion-Sileni, V.; Gogas, H.; et al. Safety and efficacy of nivolumab in patients with rare melanoma subtypes who progressed on or after ipilimumab treatment: A single-arm, open-label, phase II study (CheckMate 172). Eur. J. Cancer 2019, 119, 168–178. [Google Scholar] [CrossRef]
- Zheng, Q.; Li, J.; Zhang, H.; Wang, Y.; Zhang, S. Immune checkpoint inhibitors in advanced acral melanoma: A systematic review. Front. Oncol. 2020, 10, 602705. [Google Scholar] [CrossRef]
- Li, J.; Smalley, I.; Chen, Z.; Wu, J.-Y.; Phadke, M.S.; Teer, J.K.; Nguyen, T.; Karreth, F.A.; Koomen, J.M.; Sarnaik, A.A.; et al. Single-cell characterization of the cellular landscape of acral melanoma identifies novel targets for immunotherapy. Clin. Cancer Res. 2022, 28, 2131–2146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lan, S.; Wu, D. Advanced acral melanoma therapies: Current status and future directions. Curr. Treat. Options Oncol. 2022, 23, 1405–1427. [Google Scholar] [CrossRef] [PubMed]
- Zaremba, A.; Murali, R.; Jansen, P.; Möller, I.; Sucker, A.; Paschen, A.; Zimmer, L.; Livingstone, E.; Brinker, T.J.; Hadaschik, E.; et al. Clinical and genetic analysis of melanomas arising in acral sites. Eur. J. Cancer 2019, 119, 66–76. [Google Scholar] [CrossRef]
- Fujisawa, Y.; Ito, T.; Kato, H.; Irie, H.; Kaji, T.; Maekawa, T.; Asai, J.; Yamamoto, Y.; Fujimura, T.; Nakai, Y.; et al. Outcome of combination therapy using BRAF and MEK inhibitors among Asian patients with advanced melanoma: An analysis of 112 cases. Eur. J. Cancer 2021, 145, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.K.; Lee, S.; Kim, K.; Heo, M.H.; Lee, H.; Cho, J.; Kim, N.K.; Park, W.; Lee, S.J.; Kim, J.H.; et al. Efficacy of BRAF inhibitors in Asian metastatic melanoma patients: Potential implications of genomic sequencing in BRAF-mutated melanoma. Transl. Oncol. 2016, 9, 557–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mao, L.; Ding, Y.; Bai, X.; Sheng, X.; Dai, J.; Chi, Z.; Cui, C.; Kong, Y.; Fan, Y.; Xu, Y.; et al. Overall survival of patients with unresectable or metastatic BRAF V600-mutant acral/cutaneous melanoma administered dabrafenib plus trametinib: Long-term follow-up of a multicenter, single-arm phase IIa trial. Front. Oncol. 2021, 11, 720044. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, A.; Namikawa, K.; Nakano, E.; Yamazaki, N. Real-world efficacy and safety data for dabrafenib and trametinib combination therapy in Japanese patients with BRAF V600 mutation-positive advanced melanoma. J. Dermatol. 2019, 47, 257–264. [Google Scholar] [CrossRef]
- Si, L.; Zhang, X.; Shin, S.J.; Fan, Y.; Lin, C.-C.; Kim, T.M.; Dechaphunkul, A.; Maneechavakajorn, J.; Wong, C.S.; Ilankumaran, P.; et al. Open-label, phase IIa study of dabrafenib plus trametinib in East Asian patients with advanced BRAF V600-mutant cutaneous melanoma. Eur. J. Cancer 2020, 135, 31–38. [Google Scholar] [CrossRef]
- Häfliger, E.M.; Ramelyte, E.; Mangana, J.; Kunz, M.; Kazakov, D.; Dummer, R.; Cheng, P. Metastatic acral lentiginous melanoma in a tertiary referral center in Switzerland: A systematic analysis. Melanoma Res. 2018, 28, 442–450. [Google Scholar] [CrossRef]
- Fujimura, T.; Yoshino, K.; Kato, H.; Fujisawa, Y.; Nakamura, Y.; Yamamoto, Y.; Kunimoto, K.; Ito, T.; Matsushita, S.; Maekawa, T.; et al. Case series of BRAF-mutated advanced melanoma treated with encorafenib plus binimetinib combination therapy. J. Dermatol. 2020, 48, 397–400. [Google Scholar] [CrossRef]
- Bai, X.; Mao, L.L.; Chi, Z.H.; Sheng, X.N.; Cui, C.L.; Kong, Y.; Dai, J.; Wang, X.; Li, S.M.; Tang, B.X.; et al. BRAF inhibitors: Efficacious and tolerable in BRAF-mutant acral and mucosal melanoma. Neoplasma 2017, 64, 626–632. [Google Scholar] [CrossRef] [Green Version]
- Nathan, P.; Hassel, J.C.; Rutkowski, P.; Baurain, J.-F.; Butler, M.O.; Schlaak, M.; Sullivan, R.J.; Ochsenreither, S.; Dummer, R.; Kirkwood, J.M.; et al. Overall survival benefit with tebentafusp in metastatic uveal melanoma. N. Engl. J. Med. 2021, 385, 1196–1206. [Google Scholar] [CrossRef]
- Barros, L.R.C.; Couto, S.C.F.; Santurio, D.D.S.; Paixão, E.A.; Cardoso, F.; da Silva, V.J.; Klinger, P.; Ribeiro, P.D.A.C.; Rós, F.A.; Oliveira, T.G.M.; et al. Systematic review of available CAR-T cell trials around the world. Cancers 2022, 14, 2667. [Google Scholar] [CrossRef] [PubMed]
- Soltantoyeh, T.; Akbari, B.; Karimi, A.; Chalbatani, G.M.; Ghahri-Saremi, N.; Hadjati, J.; Hamblin, M.; Mirzaei, H. Chimeric antigen receptor (CAR) T cell therapy for metastatic melanoma: Challenges and road ahead. Cells 2021, 10, 1450. [Google Scholar] [CrossRef] [PubMed]
- Esnault, C.; Schrama, D.; Houben, R.; Guyétant, S.; Desgranges, A.; Martin, C.; Berthon, P.; Viaud-Massuard, M.-C.; Touzé, A.; Kervarrec, T.; et al. Antibody–drug conjugates as an emerging therapy in oncodermatology. Cancers 2022, 14, 778. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Johnson, D.B. Antibody-drug conjugates for melanoma and other skin malignancies. Curr. Treat. Options Oncol. 2022, 23, 1428–1442. [Google Scholar] [CrossRef] [PubMed]
- Murata, M.; Ito, T.; Tanaka, Y.; Kaku-Ito, Y.; Furue, M. NECTIN4 expression in extramammary paget’s disease: Implication of a new therapeutic target. Int. J. Mol. Sci. 2020, 21, 5891. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Murata, M.; Oda, Y.; Furue, M.; Ito, T. Nectin cell adhesion molecule 4 (NECTIN4) expression in cutaneous squamous cell carcinoma: A new therapeutic target? Biomedicines 2021, 9, 355. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Hashimoto, H.; Tanaka, Y.; Tanegashima, K.; Murata, M.; Oda, Y.; Kaku-Ito, Y. NECTIN4 expression in sebaceous and sweat gland carcinoma. Eur. J. Dermatol. 2022, 32, 181–186. [Google Scholar] [CrossRef]
- Tanaka, Y.; Murata, M.; Shen, C.-H.; Furue, M.; Ito, T. NECTIN4: A novel therapeutic target for melanoma. Int. J. Mol. Sci. 2021, 22, 976. [Google Scholar] [CrossRef]
- Tanaka, Y.; Murata, M.; Tanegashima, K.; Oda, Y.; Ito, T. Nectin cell adhesion molecule 4 regulates angiogenesis through Src signaling and serves as a novel therapeutic target in angiosarcoma. Sci. Rep. 2022, 12, 1–16. [Google Scholar] [CrossRef]
- Hashimoto, H.; Tanaka, Y.; Murata, M.; Ito, T. Nectin-4: A novel therapeutic target for skin cancers. Curr. Treat. Options Oncol. 2022, 23, 578–593. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Tanegashima, K.; Tanaka, Y.; Hashimoto, H.; Murata, M.; Oda, Y.; Kaku-Ito, Y. Trop2 expression in extramammary paget’s disease and normal skin. Int. J. Mol. Sci. 2021, 22, 7706. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Hashimoto, H.; Tanaka, Y.; Tanegashima, K.; Murata, M.; Ichiki, T.; Iwasaki, T.; Oda, Y.; Kaku-Ito, Y. TROP2 expression in sebaceous and sweat gland carcinoma. J. Clin. Med. 2022, 11, 607. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Ito, T.; Kaku-Ito, Y.; Tanegashima, K.; Tsuji, G.; Kido-Nakahara, M.; Oda, Y.; Nakahara, T. Human epidermal growth factor receptor 3 serves as a novel therapeutic target for acral melanoma. Cell Death Discov. 2023, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Nail Unit Melanoma | Acral Melanoma | Cutaneous Melanoma |
|---|---|---|
| NF1, | KIT, | BRAF, |
| KIT, | NRAS, | NRAS, |
| NRAS, | BRAF, | KIT, |
| BRAF, | TERT, | NF1, |
| PIK3CA, | CDK4, | CDKN2A, |
| STK11, | NF1, | TP53, |
| EGFR, | TP53, | PTEN, |
| FGFR3, | CDKN2A, etc. | TERT, etc. |
| PEPN11, etc. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ito, T.; Hashimoto, H.; Kaku-Ito, Y.; Tanaka, Y.; Nakahara, T. Nail Apparatus Melanoma: Current Management and Future Perspectives. J. Clin. Med. 2023, 12, 2203. https://doi.org/10.3390/jcm12062203
Ito T, Hashimoto H, Kaku-Ito Y, Tanaka Y, Nakahara T. Nail Apparatus Melanoma: Current Management and Future Perspectives. Journal of Clinical Medicine. 2023; 12(6):2203. https://doi.org/10.3390/jcm12062203
Chicago/Turabian StyleIto, Takamichi, Hiroki Hashimoto, Yumiko Kaku-Ito, Yuka Tanaka, and Takeshi Nakahara. 2023. "Nail Apparatus Melanoma: Current Management and Future Perspectives" Journal of Clinical Medicine 12, no. 6: 2203. https://doi.org/10.3390/jcm12062203
APA StyleIto, T., Hashimoto, H., Kaku-Ito, Y., Tanaka, Y., & Nakahara, T. (2023). Nail Apparatus Melanoma: Current Management and Future Perspectives. Journal of Clinical Medicine, 12(6), 2203. https://doi.org/10.3390/jcm12062203