

Laparoscopic-Assisted Colorectal Resection Can Reduce the Inhibition of Immune Function Compared with Conventional Open Surgery: A Retrospective Clinical Study


Abstract
:1. Introduction
2. Materials and Methods
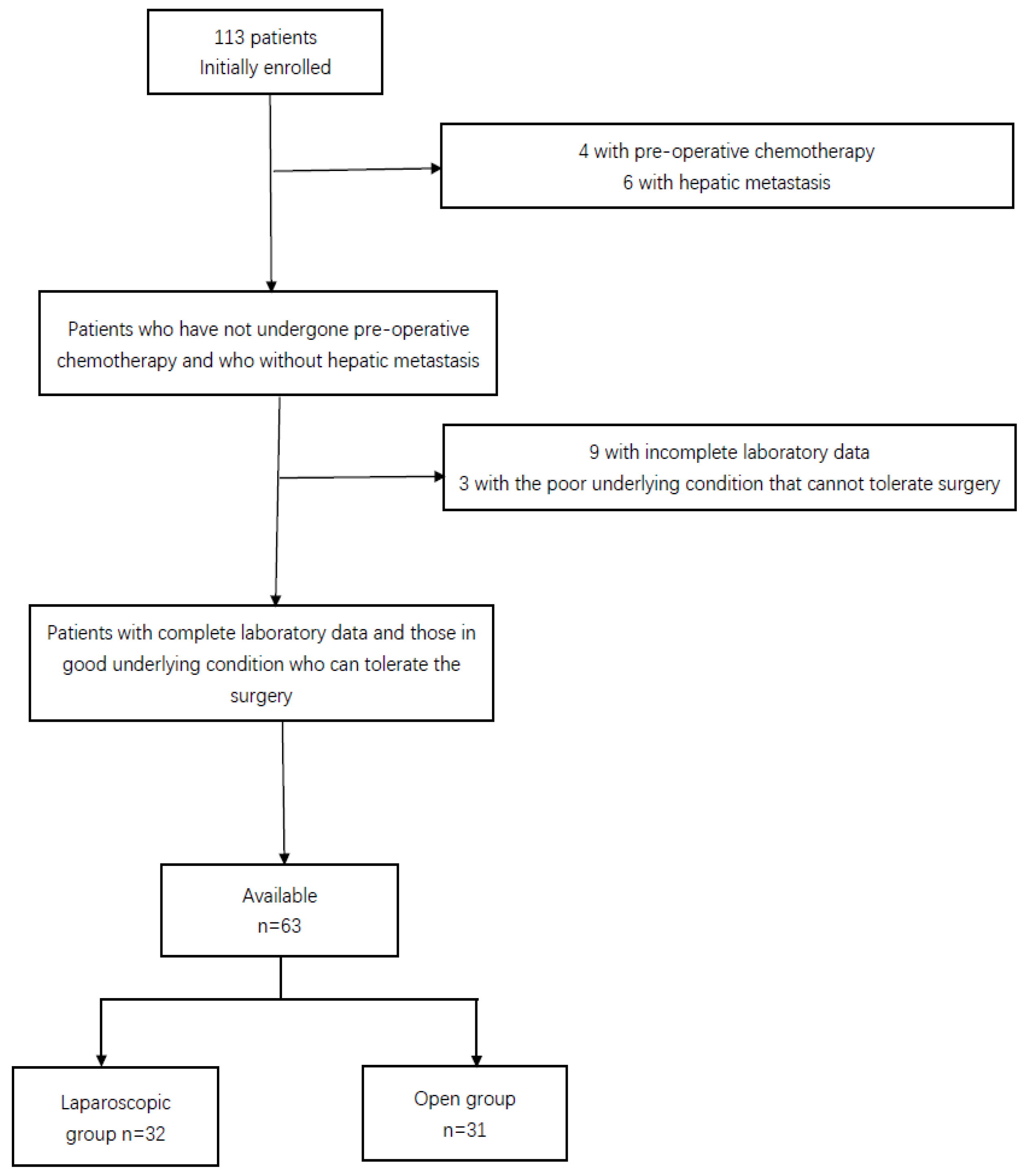
2.1. Patient Data
2.2. Immunological Index Acquisition
2.3. Statistical Analysis
3. Results
3.1. Clinical Characteristics
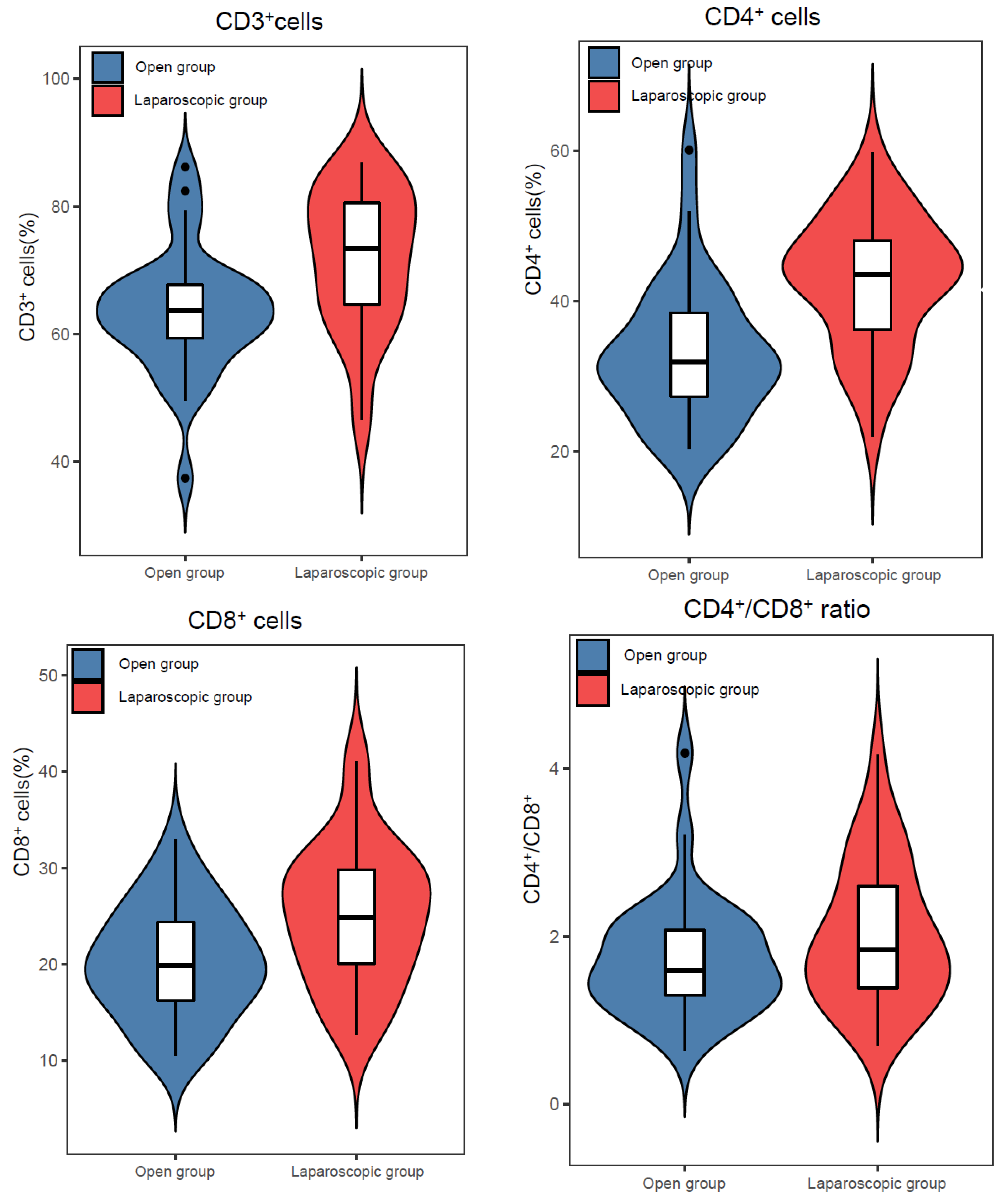
3.2. Difference of Immunological Indexes
3.3. Analysis of Influencing Factors
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Goding Sauer, A.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [Green Version]
- Buhrmann, C.; Kraehe, P.; Lueders, C.; Shayan, P.; Goel, A.; Shakibaei, M. Curcumin suppresses crosstalk between colon cancer stem cells and stromal fibroblasts in the tumor microenvironment: Potential role of EMT. PLoS ONE 2014, 9, e107514. [Google Scholar] [CrossRef] [Green Version]
- Maiorino, L.; Daßler-Plenker, J.; Sun, L.; Egeblad, M. Innate Immunity and Cancer Pathophysiology. Annu. Rev. Pathol. 2022, 17, 425–457. [Google Scholar] [CrossRef]
- Scharping, N.E.; Menk, A.V.; Moreci, R.S.; Whetstone, R.D.; Dadey, R.E.; Watkins, S.C.; Ferris, R.L.; Delgoffe, G.M. The Tumor Microenvironment Represses T Cell Mitochondrial Biogenesis to Drive Intratumoral T Cell Metabolic Insufficiency and Dysfunction. Immunity 2016, 45, 374–388. [Google Scholar] [CrossRef] [Green Version]
- Saleh, R.; Elkord, E. Acquired resistance to cancer immunotherapy: Role of tumor-mediated immunosuppression. Semin. Cancer Biol. 2020, 65, 13–27. [Google Scholar] [CrossRef]
- Mkrtichyan, M.; Najjar, Y.G.; Raulfs, E.C.; Liu, L.; Langerman, S.; Guittard, G.; Ozbun, L.; Khleif, S.N. B7-DC-Ig enhances vaccine effect by a novel mechanism dependent on PD-1 expression level on T cell subsets. J. Immunol. 2012, 189, 2338–2347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varanasi, S.K.; Kumar, S.V.; Rouse, B.T. Determinants of Tissue-Specific Metabolic Adaptation of T Cells. Cell Metab. 2020, 32, 908–919. [Google Scholar] [CrossRef]
- Liu, G.; Shi, L.; Wu, Z. Is Natural Orifice Specimen Extraction Surgery Really Safe in Radical Surgery for Colorectal Cancer? Front. Endocrinol. 2022, 13, 837902. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Jiang, Z.; Zhao, K.; Li, G.; Liu, F.; Pan, H.; Li, J. Immunologic response after laparoscopic colon cancer operation within an enhanced recovery program. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2012, 16, 1379–1388. [Google Scholar] [CrossRef] [PubMed]
- Michelucci, A.; Cordes, T.; Ghelfi, J.; Pailot, A.; Reiling, N.; Goldmann, O.; Binz, T.; Wegner, A.; Tallam, A.; Rausell, A.; et al. Immune-responsive gene 1 protein links metabolism to immunity by catalyzing itaconic acid production. Proc. Natl. Acad. Sci. USA 2013, 110, 7820–7825. [Google Scholar] [CrossRef] [Green Version]
- Kobashi, Y.; Shimizu, H.; Ohue, Y.; Mouri, K.; Obase, Y.; Miyashita, N.; Oka, M. Comparison of T-cell interferon-gamma release assays for Mycobacterium tuberculosis-specific antigens in patients with active and latent tuberculosis. Lung 2010, 188, 283–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, R.; Yuan, D.; Guo, Y.; Yan, R.; Li, K. Immune Effects of γδ T Cells in Colorectal Cancer: A Review. Front. Immunol. 2020, 11, 1600. [Google Scholar] [CrossRef] [PubMed]
- Degrandi, D.; Hoffmann, R.; Beuter-Gunia, C.; Pfeffer, K. The proinflammatory cytokine-induced IRG1 protein associates with mitochondria. J. Interferon Cytokine Res. Off. J. Int. Soc. Interferon Cytokine Res. 2009, 29, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Tsimogiannis, K.E.; Tellis, C.C.; Tselepis, A.D.; Pappas-Gogos, G.K.; Tsimoyiannis, E.C.; Basdanis, G. Toll-like receptors in the inflammatory response during open and laparoscopic colectomy for colorectal cancer. Surg. Endosc. 2012, 26, 330–336. [Google Scholar] [CrossRef]
- Podda, M.; Pisanu, A.; Morello, A.; Segalini, E.; Jayant, K.; Gallo, G.; Sartelli, M.; Coccolini, F.; Catena, F.; Di Saverio, S. Laparoscopic versus open colectomy for locally advanced T4 colonic cancer: Meta-analysis of clinical and oncological outcomes. Br. J. Surg. 2022, 109, 319–331. [Google Scholar] [CrossRef] [PubMed]
- Milasiene, V.; Stratilatovas, E.; Norkiene, V. The importance of T-lymphocyte subsets on overall survival of colorectal and gastric cancer patients. Medicina 2007, 43, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Oh, D.Y.; Fong, L. Cytotoxic CD4+ T cells in cancer: Expanding the immune effector toolbox. Immunity 2021, 54, 2701–2711. [Google Scholar] [CrossRef]
- Wu, Z.; Zheng, Y.; Sheng, J.; Han, Y.; Yang, Y.; Pan, H.; Yao, J. CD3(+)CD4(-)CD8(-) (Double-Negative) T Cells in Inflammation, Immune Disorders and Cancer. Front. Immunol. 2022, 13, 816005. [Google Scholar] [CrossRef]
- St Paul, M.; Ohashi, P.S. The Roles of CD8+ T Cell Subsets in Antitumor Immunity. Trends Cell Biol. 2020, 30, 695–704. [Google Scholar] [CrossRef]
- Xia, X.J.; Liu, B.C.; Su, J.S.; Pei, H.; Chen, H.; Li, L.; Liu, Y.F. Preoperative CD4 count or CD4/CD8 ratio as a useful indicator for postoperative sepsis in HIV-infected patients undergoing abdominal operations. J. Surg. Res. 2012, 174, e25–e30. [Google Scholar] [CrossRef]
- Wichmann, M.W.; Hüttl, T.P.; Winter, H.; Spelsberg, F.; Angele, M.K.; Heiss, M.M.; Jauch, K.W. Immunological effects of laparoscopic vs open colorectal surgery: A prospective clinical study. Arch. Surg. 2005, 140, 692–697. [Google Scholar] [CrossRef] [Green Version]
- Mölkänen, T.; Rostila, A.; Ruotsalainen, E.; Alanne, M.; Perola, M.; Järvinen, A. Genetic polymorphism of the C-reactive protein (CRP) gene and a deep infection focus determine maximal serum CRP level in Staphylococcus aureus bacteremia. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2010, 29, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Vittimberga, F.J., Jr.; Foley, D.P.; Meyers, W.C.; Callery, M.P. Laparoscopic surgery and the systemic immune response. Ann. Surg. 1998, 227, 326–334. [Google Scholar] [CrossRef]
- Strowitzki, M.J.; Nelson, R.; Garcia, M.P.; Tuffs, C.; Bleul, M.B.; Fitzsimons, S.; Navas, J.; Uzieliene, I.; Ritter, A.S.; Phelan, D.; et al. Carbon Dioxide Sensing by Immune Cells Occurs through Carbonic Anhydrase 2-Dependent Changes in Intracellular pH. J. Immunol. 2022, 208, 2363–2375. [Google Scholar] [CrossRef] [PubMed]
- Albers, K.I.; Polat, F.; Helder, L.; Panhuizen, I.F.; Snoeck, M.M.J.; Polle, S.B.W.; de Vries, H.; Dias, E.M.; Slooter, G.D.; de Boer, H.D.; et al. Quality of Recovery and Innate Immune Homeostasis in Patients Undergoing Low-pressure Versus Standard-pressure Pneumoperitoneum During Laparoscopic Colorectal Surgery (RECOVER): A Randomized Controlled Trial. Ann. Surg. 2022, 276, e664–e673. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.L.; Eu, K.W.; Tai, B.C.; Soh, J.G.; MacHin, D.; Seow-Choen, F. Randomized clinical trial of the effect of open versus laparoscopically assisted colectomy on systemic immunity in patients with colorectal cancer. Br. J. Surg. 2001, 88, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.B.; Wang, B.; Wang, X.Y.; Zhang, L. Influence of video-assisted thoracoscopic lobectomy on immunological functions in non-small cell lung cancer patients. Med. Oncol. 2015, 32, 201. [Google Scholar] [CrossRef]
- Zhou, L.W.; Ding, H.L.; Li, M.Q.; Jin, S.; Wang, X.S.; Ji, L.J. Effect of tramadol on perioperative immune function in patients undergoing gastric cancer surgeries. Anesth. Essays Res. 2013, 7, 54–57. [Google Scholar]
- Préfontaine, L.; Hélie, P.; Vachon, P. Postoperative pain in Sprague Dawley rats after liver biopsy by laparotomy versus laparoscopy. Lab Anim. 2015, 44, 174–178. [Google Scholar] [CrossRef] [PubMed]
- Toor, S.M.; Murshed, K.; Al-Dhaheri, M.; Khawar, M.; Abu Nada, M.; Elkord, E. Immune Checkpoints in Circulating and Tumor-Infiltrating CD4(+) T Cell Subsets in Colorectal Cancer Patients. Front. Immunol. 2019, 10, 2936. [Google Scholar] [CrossRef]
- West, M.A.; Baker, J.; Bellingham, J. Kinetics of decreased LPS-stimulated cytokine release by macrophages exposed to CO2. J. Surg. Res. 1996, 63, 269–274. [Google Scholar] [CrossRef]
- Zawadzki, M.; Krzystek-Korpacka, M.; Gamian, A.; Witkiewicz, W. Comparison of inflammatory responses following robotic and open colorectal surgery: A prospective study. Int. J. Colorectal Dis. 2017, 32, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, Z.; Min, W. Mitochondria, Oxidative Stress and Innate Immunity. Front. Physiol. 2018, 9, 1487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I. Eustress and Malondialdehyde (MDA): Role of Panax Ginseng: Randomized Placebo Controlled Study. Iran. J. Psychiatry 2017, 12, 194–200. [Google Scholar] [PubMed]
- Galon, J.; Fridman, W.H.; Pagès, F. The adaptive immunologic microenvironment in colorectal cancer: A novel perspective. Cancer Res. 2007, 67, 1883–1886. [Google Scholar] [CrossRef] [Green Version]
- Braga, M.; Pecorelli, N.; Frasson, M.; Vignali, A.; Zuliani, W.; Carlo, V.D. Long-term outcomes after laparoscopic colectomy. World J. Gastrointest. Oncol. 2011, 3, 43–48. [Google Scholar] [CrossRef] [PubMed]
- Karanika, S.; Karantanos, T.; Theodoropoulos, G.E. Immune response after laparoscopic colectomy for cancer: A review. Gastroenterol. Rep. 2013, 1, 85–94. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Items | Open Group (n = 31) | Laparoscopic Group (n = 32) | p |
|---|---|---|---|
| Gender | 0.677+ | ||
| Male | 20 | 19 | |
| Female | 11 | 13 | |
| Age (years) | 68.58 ± 9.135 | 64.97 ± 8.102 | 0.102 |
| BMI (kg/m2) | 22.17 ± 2.43 | 22.49 ± 5.14 | 0.746 |
| Operation times (min) | 156.32 ± 48.10 | 188.78 ± 65.10 | 0.028 |
| Postoperative hospital stay (days) | 12.46 ± 2.41 | 12.50 ± 3.99 | 0.753 |
| Tumor differentiation | 0.892+ | ||
| Well or Moderate | 14 | 15 | |
| Poorly | 17 | 17 | |
| Maximal tumor diameter (cm) | 0.246+ | ||
| ≤5 cm | 19 | 24 | |
| >5 cm | 12 | 8 | |
| N stage | 0.267+ | ||
| 0 | 18 | 14 | |
| 1 | 6 | 12 | |
| 2 | 7 | 6 | |
| Tumor stage | 0.378+ | ||
| II | 18 | 15 | |
| III | 13 | 17 | |
| Blood Type | 0.742+ | ||
| A | 10 | 10 | |
| B | 9 | 12 | |
| O | 7 | 6 | |
| AB | 5 | 4 | |
| Tumor Location | 0.367+ | ||
| Right colon cancer | 7 | 11 | |
| Left colon cancer | 10 | 9 | |
| Rectal cancer | 14 | 12 |
| Group | CD3+T (%) | CD4+T (%) | CD8+T (%) | CD4+T/CD8+T |
|---|---|---|---|---|
| Open group | ||||
| The day before operation | 66.59 ± 11.05 | 42.35 ± 9.21 | 23.08 ± 8.40 | 2.04 ± 0.78 |
| The third day after operation | 63.56 ± 9.72 * | 32.86 ± 9.02 *# | 20.21 ± 5.80 *# | 1.73 ± 0.71 *# |
| Laparoscopic group | ||||
| The day before operation | 69.10 ± 10.70 | 43.76 ± 9.64 | 24.52 ± 8.13 | 2.06 ± 1.17 |
| The third day after operation | 71.87 ± 10.89 # | 42.75 ± 8.70 | 25.08 ± 7.20 | 2.01 ± 0.85 |
| Items | Postoperative CD3+T | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95%CI) | p | OR (95%CI) | p | |
| Gender (male/female) | 1.379 (0.497~3.825) | 0.537 | ||
| Age (years, ≤65/>65) | 0.930 (0.873~0.991) | 0.025 | 0.933 (0.870~1.001) | 0.052 |
| BMI (kg/m2, ≤18.5/>18.5) | 1.027 (0.906~1.165) | 0.676 | ||
| Operation times (min, ≤150/>150) | 1.003 (0.994~1.011) | 0.544 | ||
| Tumor differentiation (Well or Moderate/Poor) | 1.071 (0.398~2.887) | 0.891 | ||
| Maximal tumor diameter (≤5 cm/>5 cm) | 1.406 (0.484~4.079) | 0.531 | ||
| Tumor stage (II/III) | 0.941 (0.350~2.531) | 0.904 | ||
| Blood type | ||||
| AB | 1 | |||
| A | 2.321 (0.467~11.545) | 0.303 | ||
| B | 0.769 (0.158~3.744) | 0.745 | ||
| O | 1.458 (0.264~8.048) | 0.665 | ||
| Tumor location | ||||
| Rectal cancer | 1 | |||
| Right colon cancer | 4.911 (1.325~18.205) | 0.017 | 5.349 (1.250~22.898) | 0.024 |
| Left colon cancer | 2.099 (0.626~7.037) | 0.230 | ||
| Types of surgery (open/laparoscopic) | 4.620 (1.599~13.349) | 0.005 | 3.908 (1.225~12.468) | 0.021 |
| Items | Postoperative CD4+T | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95%CI) | p | OR (95%CI) | p | |
| Gender (male/female) | 0.612 (0.219~1.710) | 0.349 | ||
| Age (years, ≤65/>65) | 0.959 (0.903~1.017) | 0.161 | ||
| BMI (kg/m2, ≤18.5/>18.5) | 0.897 (0.771~1.042) | 0.155 | ||
| Operation times (min, ≤150/>150) | 1.012 (1.002~1.023) | 0.021 | 1.012 (0.999~1.024) | 0.064 |
| Tumor differentiation (Well or Moderate/Poor) | 0.830 (0.308~2.237) | 0.712 | ||
| Maximal tumor diameter (≤5 cm/>5 cm) | 1.895 (0.645~5.569) | 0.245 | ||
| Tumor stage (II/III) | 0.376 (0.136~1.043) | 0.060 | ||
| Blood type | ||||
| AB | 1 | |||
| A | 0.533 (0.109~2.616) | 0.438 | ||
| B | 1.067 (0.221~5.145) | 0.936 | ||
| O | 0.933 (0.169~5.151) | 0.937 | ||
| Tumor location | ||||
| Rectal cancer | 1 | |||
| Right colon cancer | 7.875 (1.964~31.574) | 0.004 | 10.384 (2.076~51.936) | 0.004 |
| Left colon cancer | 2.5 (0.733~8.524) | 0.143 | ||
| Types of surgery (open/laparoscopic) | 6.247 (2.093~18.641) | 0.001 | 5.656 (1.602~19.982) | 0.007 |
| Items | Postoperative CD8+T | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95%CI) | p | OR (95%CI) | p | |
| Gender (male/female) | 1.379 (0.497~3.825) | 0.537 | ||
| Age (years, ≤65/>65) | 0.998 (0.942~1.056) | 0.934 | ||
| BMI (kg/m2, ≤18.5/>18.5) | 1.012 (0.894~1.146) | 0.848 | ||
| Operation times (min, ≤150/>150) | 0.997 (0.988~1.005) | 0.423 | ||
| Tumor differentiation (Well or Moderate/Poor) | 2.338 (0.848~6.447) | 0.101 | ||
| Maximal tumor diameter (≤5 cm/>5 cm) | 0.711 (0.245~2.065) | 0.531 | ||
| Tumor stage (II/III) | 1.775 (0.654~4.819) | 0.260 | ||
| Blood type | ||||
| AB | 1 | |||
| A | 1.250 (0.257~6.070) | 0.782 | ||
| B | 2.031 (0.417~9.886) | 0.380 | ||
| O | 0.781 (0.139~4.387) | 0.779 | ||
| Tumor location | ||||
| Rectal cancer | 1 | |||
| Right colon cancer | 0.500 (0.144~1.737) | 0.275 | 0.353 (0.090~1.389) | 0.136 |
| Left colon cancer | 2.167 (0.630~7.454) | 0.220 | ||
| Types of surgery (open/laparoscopic) | 3.471 (1.232~9.782) | 0.019 | 4.780 (1.495~15.280) | 0.008 |
| Items | Postoperative CD4+T/CD8+T | |||
|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | |||
| OR (95%CI) | p | OR (95%CI) | p | |
| Gender (male/female) | 1.379 (0.497~3.825) | 0.537 | ||
| Age (years, ≤65/>65) | 0.968 (0.913~1.026) | 0.275 | ||
| BMI (kg/m2, ≤18.5/>18.5) | 1.006 (0.889~1.139) | 0.921 | ||
| Operation times (time, ≤150/>150) | 1.017 (1.005~1.028) | 0.005 | 1.016 (1.004~1.028) | 0.009 |
| Tumor differentiation (Well or Moderate/Poorly) | 1.071 (0.398~2.887) | 0.891 | ||
| Maximal tumor diameter (≤5 cm/>5 cm) | 0.711 (0.245~2.065) | 0.531 | ||
| Tumor stage (II/III) | 1.214 (0.451~3.269) | 0.701 | ||
| Blood type | ||||
| AB | 1 | |||
| A | 0.269 (0.051~1.420) | 0.122 | ||
| B | 0.813 (0.157~4.197) | 0.804 | ||
| O | 0.429 (0.073~2.500) | 0.346 | ||
| Tumor location | ||||
| Rectal cancer | 1 | |||
| Right colon cancer | 3.545 (0.974~12.905) | 0.055 | ||
| Left colon cancer | 0.992 (0.299~3.285) | 0.989 | ||
| Types of surgery (open/laparoscopic) | 2.024 (0.742~5.519) | 0.168 | 1.360 (0.451~4.102) | 0.586 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shi, B.; Tai, Q.; Chen, J.; Shi, X.; Chen, G.; Yao, H.; Mi, X.; Sun, J.; Zhou, G.; Gu, W.; et al. Laparoscopic-Assisted Colorectal Resection Can Reduce the Inhibition of Immune Function Compared with Conventional Open Surgery: A Retrospective Clinical Study. J. Clin. Med. 2023, 12, 2320. https://doi.org/10.3390/jcm12062320
Shi B, Tai Q, Chen J, Shi X, Chen G, Yao H, Mi X, Sun J, Zhou G, Gu W, et al. Laparoscopic-Assisted Colorectal Resection Can Reduce the Inhibition of Immune Function Compared with Conventional Open Surgery: A Retrospective Clinical Study. Journal of Clinical Medicine. 2023; 12(6):2320. https://doi.org/10.3390/jcm12062320
Chicago/Turabian StyleShi, Bo, Qingliang Tai, Junjie Chen, Xinyu Shi, Guoliang Chen, Huihui Yao, Xiuwei Mi, Jinbing Sun, Guoqiang Zhou, Wen Gu, and et al. 2023. "Laparoscopic-Assisted Colorectal Resection Can Reduce the Inhibition of Immune Function Compared with Conventional Open Surgery: A Retrospective Clinical Study" Journal of Clinical Medicine 12, no. 6: 2320. https://doi.org/10.3390/jcm12062320
APA StyleShi, B., Tai, Q., Chen, J., Shi, X., Chen, G., Yao, H., Mi, X., Sun, J., Zhou, G., Gu, W., & He, S. (2023). Laparoscopic-Assisted Colorectal Resection Can Reduce the Inhibition of Immune Function Compared with Conventional Open Surgery: A Retrospective Clinical Study. Journal of Clinical Medicine, 12(6), 2320. https://doi.org/10.3390/jcm12062320