
One-Lung Ventilation during Rigid Bronchoscopy Using a Single-Lumen Endotracheal Tube: A Descriptive, Retrospective Single-Center Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
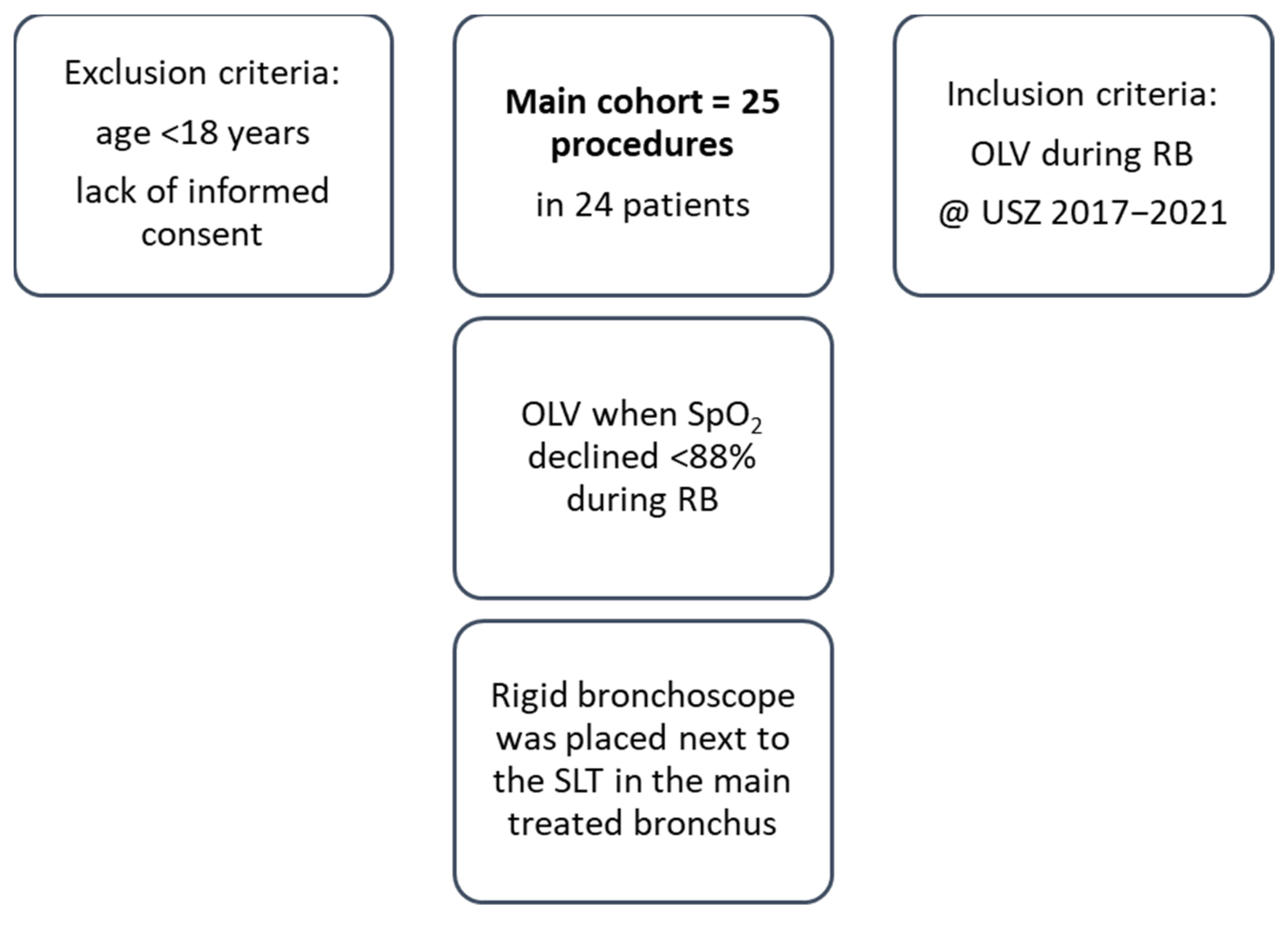
2.1. Patient Selection and Study Design
2.2. Bronchoscopy
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
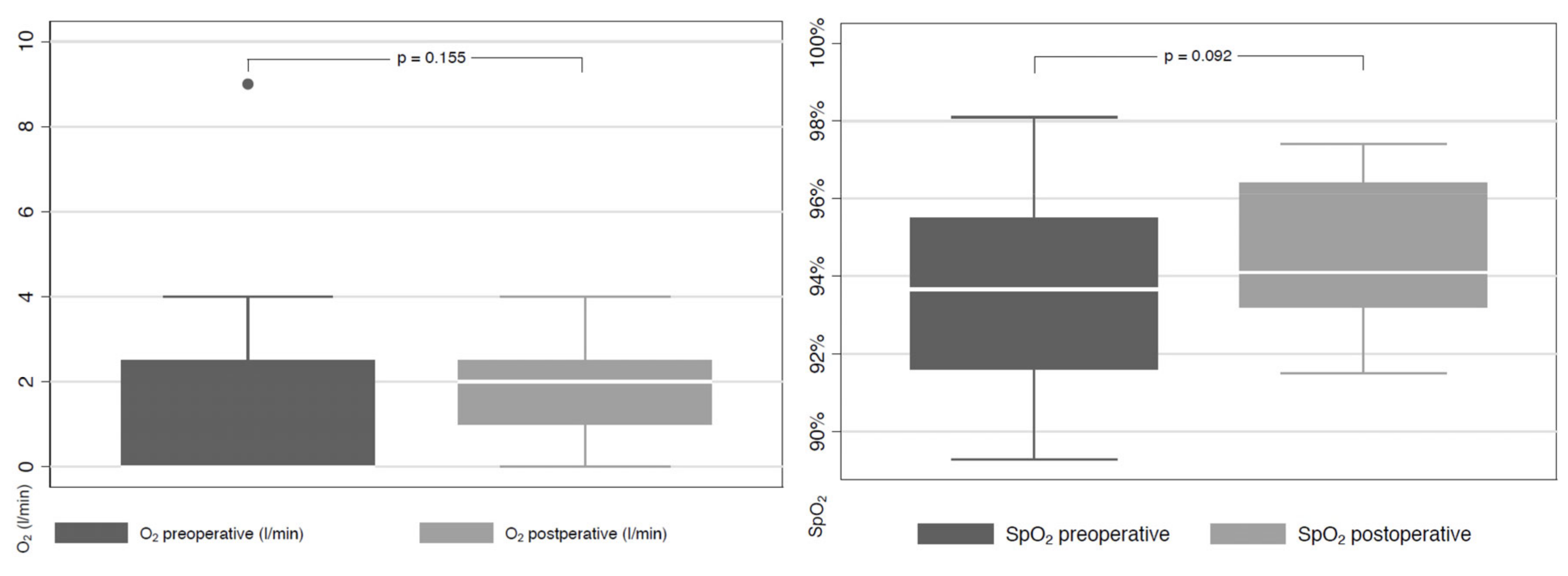
3.2. Perioperative Data and Adverse Events
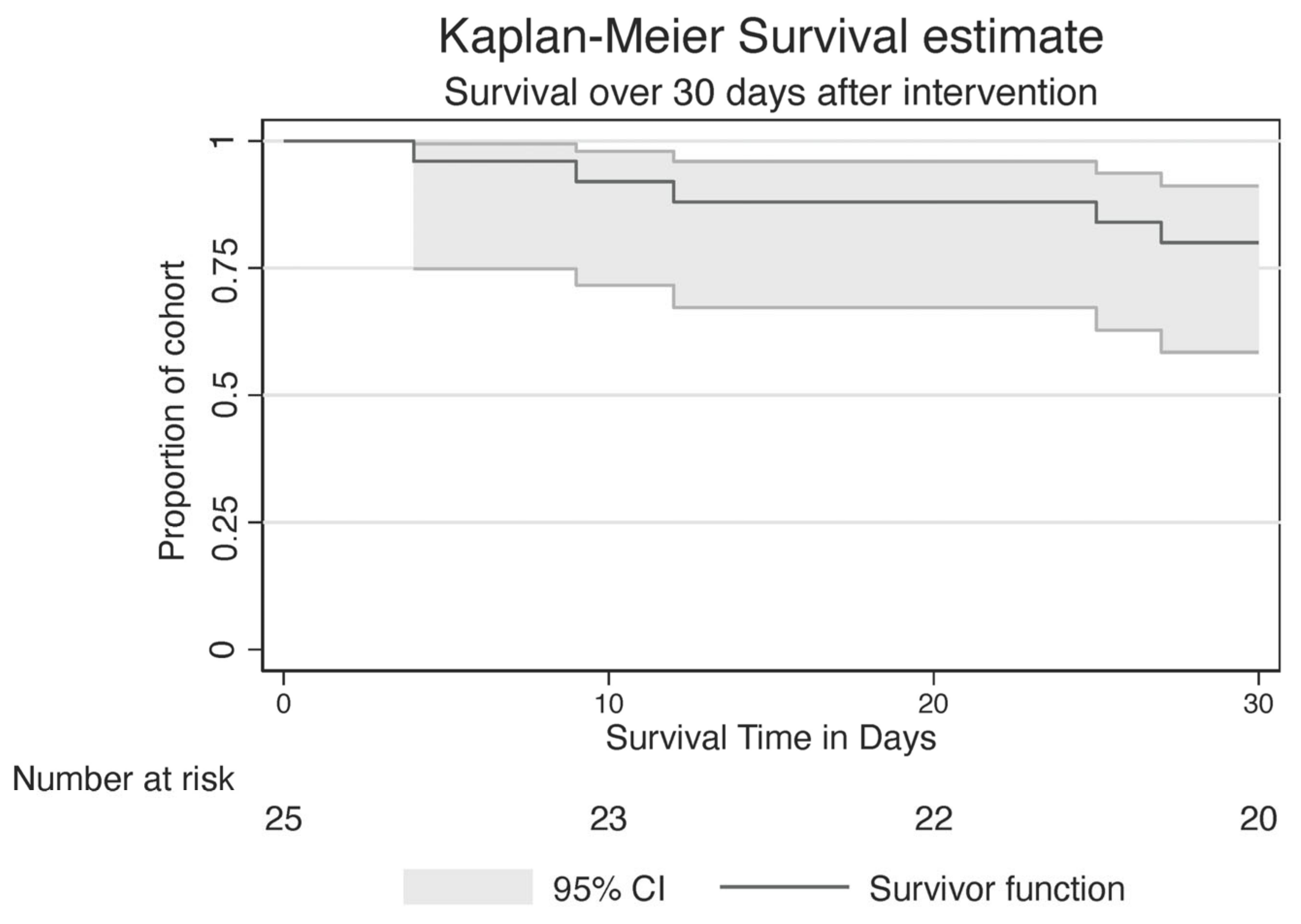
3.3. Postoperative Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ernst, A.; Feller-Kopman, D.; Becker, H.D.; Mehta, A.C. Central airway obstruction. Am. J. Respir. Crit. Care Med. 2004, 169, 1278–1297. [Google Scholar] [CrossRef] [PubMed]
- Seaman, J.C.; Musani, A.I. Endobronchial ablative therapies. Clin. Chest Med. 2013, 34, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Folch, E.; Mehta, A.C. Airway interventions in the tracheobronchial tree. Semin. Respir. Crit. Care Med. 2008, 29, 441–452. [Google Scholar] [CrossRef]
- Sachdeva, A.; Pickering, E.M.; Lee, H.J. From electrocautery, balloon dilatation, neodymium-doped:yttrium-aluminum-garnet (Nd:YAG) laser to argon plasma coagulation and cryotherapy. J. Thorac. Dis. 2015, 7 (Suppl. S4), S363–S379. [Google Scholar] [PubMed]
- Mahmood, K.; Wahidi, M.M. Ablative therapies for central airway obstruction. Semin. Respir. Crit. Care Med. 2014, 35, 681–692. [Google Scholar]
- Apfelbaum, J.L.; Caplan, R.A.; Barker, S.J.; Connis, R.T.; Cowles, C.; Ehrenwerth, J.; Nickinovich, D.G.; Pritchard, D.; Roberson, D.W.; Caplan, R.A.; et al. Practice advisory for the prevention and management of operating room fires: An updated report by the American Society of Anesthesiologists Task Force on Operating Room Fires. Anesthesiology 2013, 118, 271–290. [Google Scholar]
- Pathak, V.; Welsby, I.; Mahmood, K.; Wahidi, M.; MacIntyre, N.; Shofer, S. Ventilation and anesthetic approaches for rigid bronchoscopy. Ann. Am. Thorac. Soc. 2014, 11, 628–634. [Google Scholar] [CrossRef] [Green Version]
- Ayers, M.L.; Beamis, J.F., Jr. Rigid bronchoscopy in the twenty-first century. Clin. Chest Med. 2001, 22, 355–364. [Google Scholar] [CrossRef]
- Dincq, A.S.; Gourdin, M.; Collard, E.; Ocak, S.; D’Odémont, J.P.; Dahlqvist, C.; Lacrosse, D.; Putz, L. Anesthesia for adult rigid bronchoscopy. Acta Anaesthesiol. Belg. 2014, 65, 95–103. [Google Scholar]
- Batra, H.; Yarmus, L. Indications and complications of rigid bronchoscopy. Expert Rev. Respir. Med. 2018, 12, 509–520. [Google Scholar] [CrossRef]
- Galmen, K.; Harbut, P.; Freedman, J.; Jakobsson, J.G. The use of high-frequency ventilation during general anaesthesia: An update. F1000 Res. 2017, 6, 756. [Google Scholar] [CrossRef] [Green Version]
- Bohn, D. The history of high-frequency ventilation. Respir. Care Clin. N. Am. 2001, 7, 535–548. [Google Scholar] [CrossRef]
- McGrath, B.; Tennuci, C.; Lee, G. The History of One-Lung Anesthesia and the Double-Lumen Tube. J. Anesth. Hist. 2017, 3, 76–86. [Google Scholar] [CrossRef]
- Mirzabeigi, E.; Johnson, C.; Ternian, A. One-lung anesthesia update. Semin. Cardiothorac. Vasc. Anesth. 2005, 9, 213–226. [Google Scholar] [CrossRef]
- Bernasconi, F.; Piccioni, F. One-lung ventilation for thoracic surgery: Current perspectives. Tumori 2017, 103, 495–503. [Google Scholar] [CrossRef] [PubMed]
- Campos, J.H.; Feider, A. Hypoxia During One-Lung Ventilation-A Review and Update. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2330–2338. [Google Scholar] [CrossRef]
- Detterbeck, F.C. The eighth edition TNM stage classification for lung cancer: What does it mean on main street? J. Thorac. Cardiovasc. Surg. 2018, 155, 356–359. [Google Scholar] [CrossRef] [Green Version]
- Pawlowski, J. Anesthetic considerations for interventional pulmonary procedures. Curr. Opin. Anaesthesiol. 2013, 26, 6–12. [Google Scholar] [CrossRef]
- Kern, M.; Niemeyer, D.; Kerner, T.; Tank, S. Anesthesia in interventional pulmonology—Bronchoscopy and jet ventilation. Anasthesiol. Intensiv. Notf. Schmerzther 2015, 50, 8–18. [Google Scholar]
- Horvath, B.; Kloesel, B.; Todd, M.M.; Cole, D.J.; Prielipp, R.C. The Evolution, Current Value, and Future of the American Society of Anesthesiologists Physical Status Classification System. Anesthesiology 2021, 135, 904–919. [Google Scholar] [CrossRef]
- Richards, J.B. Calculated decisions: mMRC (Modified Medical Research Council) Dyspnea Scale. Emerg. Med. Pract. 2017, 19 (Suppl. S10), 1–2. [Google Scholar] [PubMed]
- Chaddha, U.; Murgu, S. Complications of rigid bronchoscopy. Respirology 2021, 26, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Eapen, G.A.; Shah, A.M.; Lei, X.; Jimenez, C.A.; Morice, R.C.; Yarmus, L.; Yarmus, L.; Filner, J.; Ray, C.; Michaud, G.; et al. Complications, consequences, and practice patterns of endobronchial ultrasound-guided transbronchial needle aspiration: Results of the AQuIRE registry. Chest 2013, 143, 1044–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murgu, S.; Laxmanan, B.; Stoy, S.; Egressy, K.; Chaddha, U.; Farooqui, F.; Brunner, R.; Hogarth, K.; Chaney, M. Evaluation of Safety and Short-term Outcomes of Therapeutic Rigid Bronchoscopy Using Total Intravenous Anesthesia and Spontaneous Assisted Ventilation. Respiration 2020, 99, 239–247. [Google Scholar] [CrossRef]
- Folch, E.E.; Mahajan, A.K.; Oberg, C.L.; Maldonado, F.; Toloza, E.; Krimsky, W.S.; Oh, S.; Bowling, M.R.; Benzaquen, S.; Kinsey, C.M.; et al. Standardized Definitions of Bleeding After Transbronchial Lung Biopsy: A Delphi Consensus Statement From the Nashville Working Group. Chest 2020, 158, 393–400. [Google Scholar] [CrossRef]
- Huo, J.M.; Bai, K.; Fu, Y.Q.; Liu, C.J.; Xu, F. Clinical efficacy of one-lung ventilation in treatment of children postoperatively intractable atelectasis. Zhonghua Er Ke Za Zhi 2017, 55, 840–843. [Google Scholar]
- See, K.C.; Ong, V.; Tan, Y.L.; Sahagun, J.; Taculod, J. Chest radiography versus lung ultrasound for identification of acute respiratory distress syndrome: A retrospective observational study. Crit. Care 2018, 22, 203. [Google Scholar] [CrossRef] [Green Version]
- Fortin, M.; Yarmus, L.; Rendina, E.A.; Rafeq, S.; Andrade, R.; Michaud, G.; Kazakov, J.; Arias, S.; Ciccone, A.M.; Ortiz, R.; et al. Multi-institutional retrospective analysis of adverse events following rigid tracheobronchoscopy. Respirology 2021, 26, 87–91. [Google Scholar] [CrossRef]
- Kamra, S.K.; Jaiswal, A.A.; Garg, A.K.; Mohanty, M.K. Rigid Bronchoscopic Placement of Fogarty Catheter as a Bronchial Blocker for One Lung Isolation and Ventilation in Infants and Children Undergoing Thoracic Surgery: A Single Institution Experience of 27 Cases. Indian J. Otolaryngol. Head Neck Surg. 2017, 69, 159–171. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Data | Total (n = 25) |
|---|---|
| Male sex | 16 (64%) |
| Age, years | 69.16 (± 9.89) |
| Lung cancer | 21 (84%) |
| Squamous cell carcinoma | 9 (36%) |
| Adenocarcinoma | 7 (28%) |
| Small cell carcinoma | 5 (20%) |
| Lung metastasis | 4 (16%) |
| Cancer location | |
| Right superior lobe | 2 (8%) |
| Right inferior lobe | 2 (8%) |
| Left superior lobe | 2 (8%) |
| Left inferior lobe | 2 (8%) |
| Perihilar right | 12 (48%) |
| Perihilar left | 4 (16%) |
| Perihilar left and right | 1 (4%) |
| AJCC stages | |
| IIA | 1 (4%) |
| IIB | 1 (4%) |
| IIIA | 2 (8%) |
| IIIB | 1 (4%) |
| IIIC | 1 (4%) |
| IVA | 7 (28%) |
| IVB | 9 (36%) |
| Comorbidities | |
| Metabolic comorbidities | |
| Diabetes mellitus | 4 (16%) |
| Dyslipidemia | 4 (16%) |
| Obesity | 3 (12%) |
| Malnutrition | 2 (8%) |
| Metabolic syndrome | 1 (4%) |
| Heart comorbidities | 11 (44%) |
| Arterial hypertension | 10 (40%) |
| Stroke | 3 (12%) |
| Lung comorbidities | |
| COPD | 10 (40%) |
| Previous lung embolism | 2 (8%) |
| Asthma | 1 (4%) |
| Previous pneumothorax | 1 (4%) |
| Bronchiectasis | 1 (4%) |
| Smoking | |
| Active | 5 (20%) |
| Former | 16 (64%) |
| Non-smoker | 4 (16%) |
| Pack years | 30 [15–50] |
| ASA classification | |
| 1 | 0 |
| 2 | 0 |
| 3 | 18 (72%) |
| 4 | 7 (28%) |
| Preoperative mMRC score | |
| 0 | 1 (4%) |
| 1 | 3 (12%) |
| 2 | 6 (24%) |
| 3 | 7 (28%) |
| 4 | 8 (32%) |
| Perioperative Procedures | |
|---|---|
| Endobronchial treatment | |
| Stent | 17 (68%) |
| Laser | 16 (64%) |
| APC | 14 (56%) |
| Forceps | 10 (40%) |
| Electric loop | 5 (20%) |
| Cryoprobe | 1 (4%) |
| RB size before OLV | |
| 8.5 | 8 (32%) |
| 12.0 | 9 (36%) |
| 12.5 | 1 (4%) |
| 14.0 | 2 (8%) |
| 16.0 | 1 (4%) |
| A priori OLV | 3 (9%) |
| Missing data | 1 (4%) |
| RB size during OLV | |
| 6.0 | 2 (8%) |
| 6.5 | 7 (28%) |
| 7.0 | 1 (4%) |
| 7.5 | 9 (36%) |
| 8.5 | 4 (16%) |
| Missing data | 2 (8%) |
| Perioperative Adverse Events | Total (n = 25) |
|---|---|
| Hypoxemia (SpO2 < 90%) | 22 (88%) |
| Mean duration (min) | 12.5 ± 7.64 |
| Mean lowest SpO2 (%) | 81.7 ± 6.2 |
| Relevant blood pressure changes | 16 (64%) |
| Increase > 20 mmHg | 11 (44%) |
| Decrease > 20 mmHg | 5 (20%) |
| Bleeding grade 1 | 2 (8%) |
| Bleeding grade 2 | 5 (20%) |
| Bleeding grade 3 | 5 (20%) |
| Bleeding grade 4 | 0 |
| Procedure-related bronchial fistula | 0 |
| Bronchospasm | 1 (4%) |
| New onset abnormal heart rhythm before onset of OLV | 1 (4%) |
| Barotrauma | 0 |
| ICU admission | 3 (12%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinack, C.; Balmer, H.; Ulrich, S.; Gaisl, T.; Franzen, D.P. One-Lung Ventilation during Rigid Bronchoscopy Using a Single-Lumen Endotracheal Tube: A Descriptive, Retrospective Single-Center Study. J. Clin. Med. 2023, 12, 2426. https://doi.org/10.3390/jcm12062426
Steinack C, Balmer H, Ulrich S, Gaisl T, Franzen DP. One-Lung Ventilation during Rigid Bronchoscopy Using a Single-Lumen Endotracheal Tube: A Descriptive, Retrospective Single-Center Study. Journal of Clinical Medicine. 2023; 12(6):2426. https://doi.org/10.3390/jcm12062426
Chicago/Turabian StyleSteinack, Carolin, Helene Balmer, Silvia Ulrich, Thomas Gaisl, and Daniel P. Franzen. 2023. "One-Lung Ventilation during Rigid Bronchoscopy Using a Single-Lumen Endotracheal Tube: A Descriptive, Retrospective Single-Center Study" Journal of Clinical Medicine 12, no. 6: 2426. https://doi.org/10.3390/jcm12062426
APA StyleSteinack, C., Balmer, H., Ulrich, S., Gaisl, T., & Franzen, D. P. (2023). One-Lung Ventilation during Rigid Bronchoscopy Using a Single-Lumen Endotracheal Tube: A Descriptive, Retrospective Single-Center Study. Journal of Clinical Medicine, 12(6), 2426. https://doi.org/10.3390/jcm12062426