
Evaluation of Kidney Donor Risk Index/Kidney Donor Profile Index as Predictor Tools of Deceased-Donor Kidney Transplant Outcomes in a Greek Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Statistical Analysis
2.4. Ethics Statements
3. Results
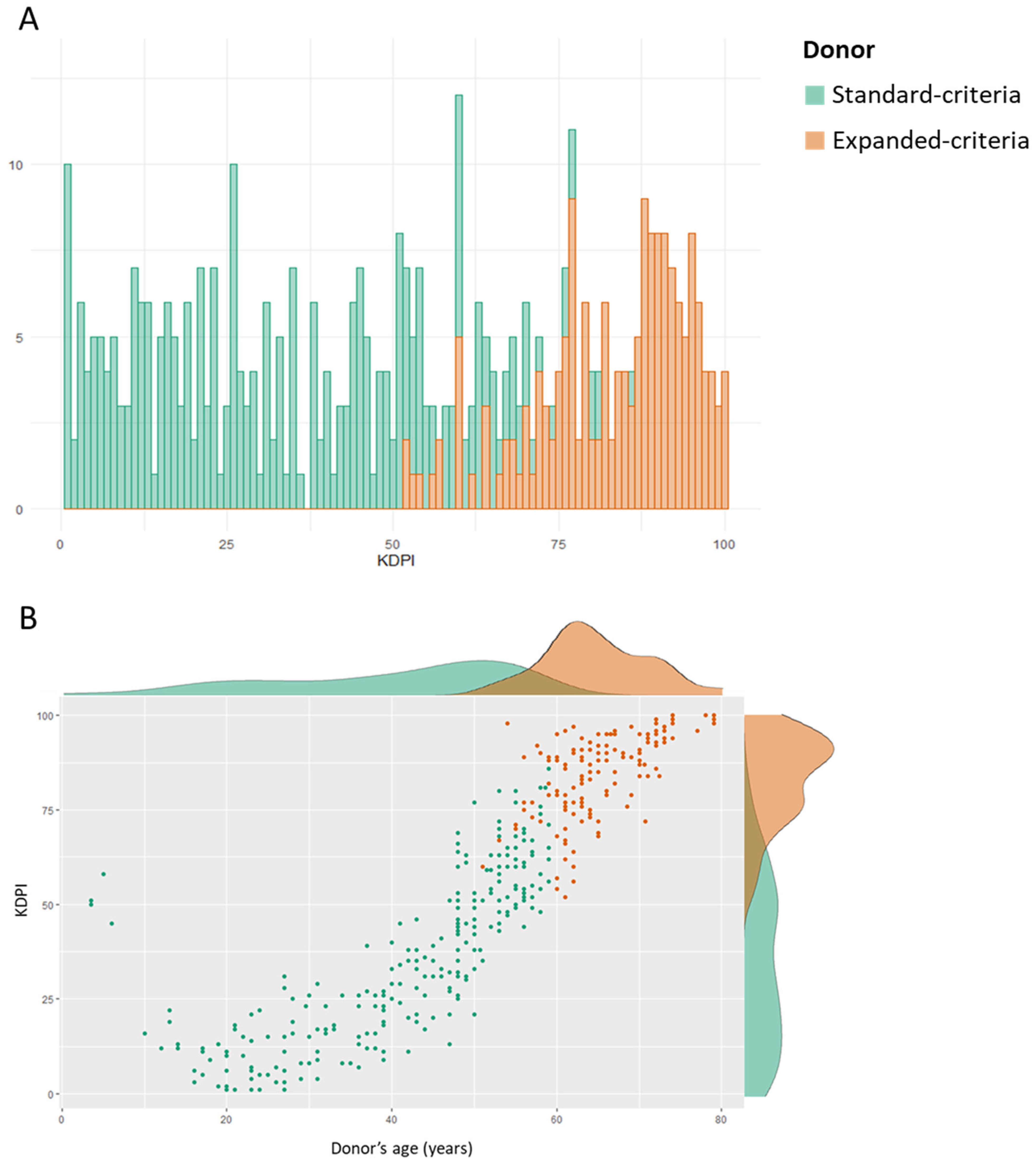
3.1. Study Population
3.2. Delayed Graft Function
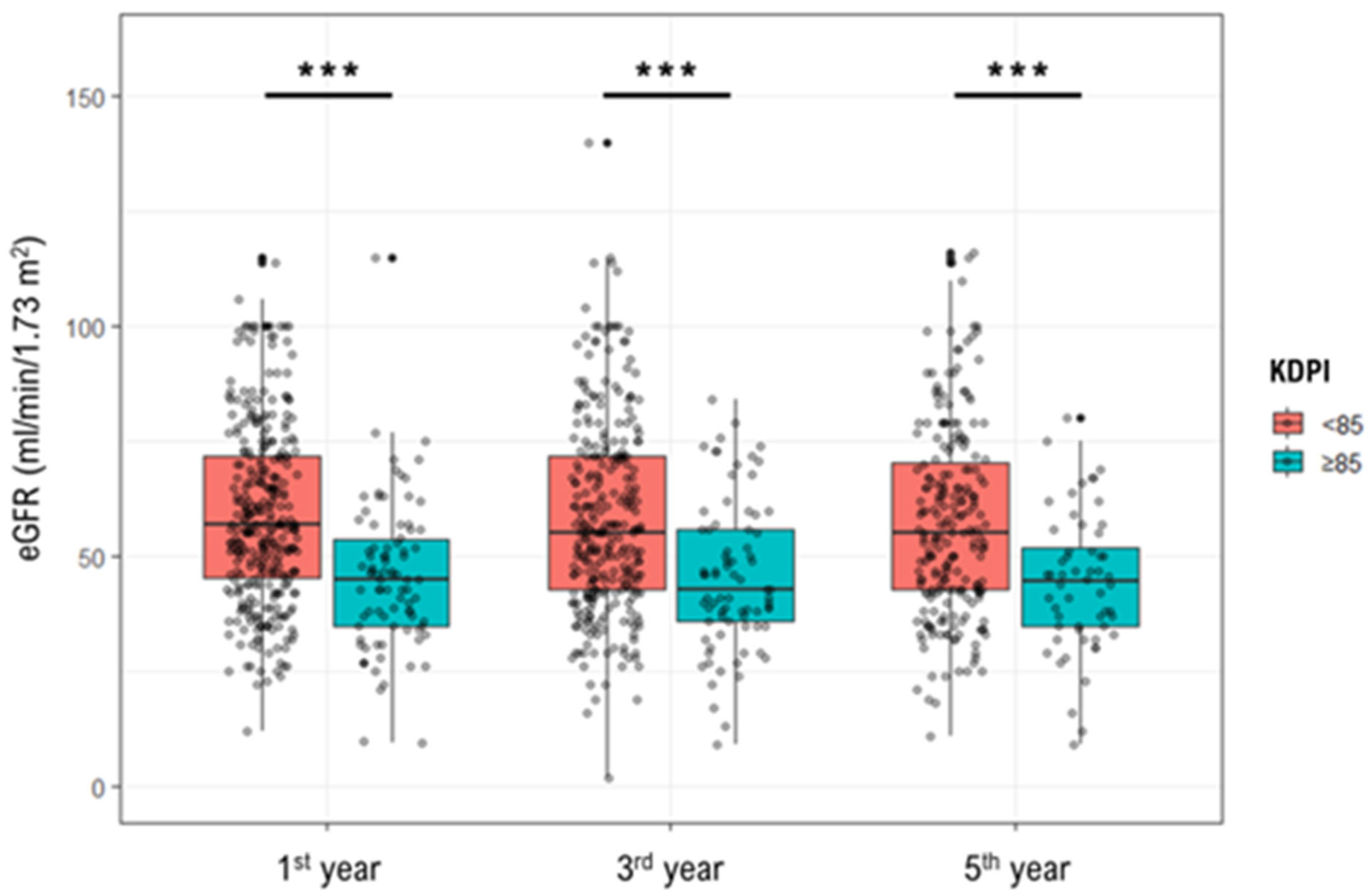
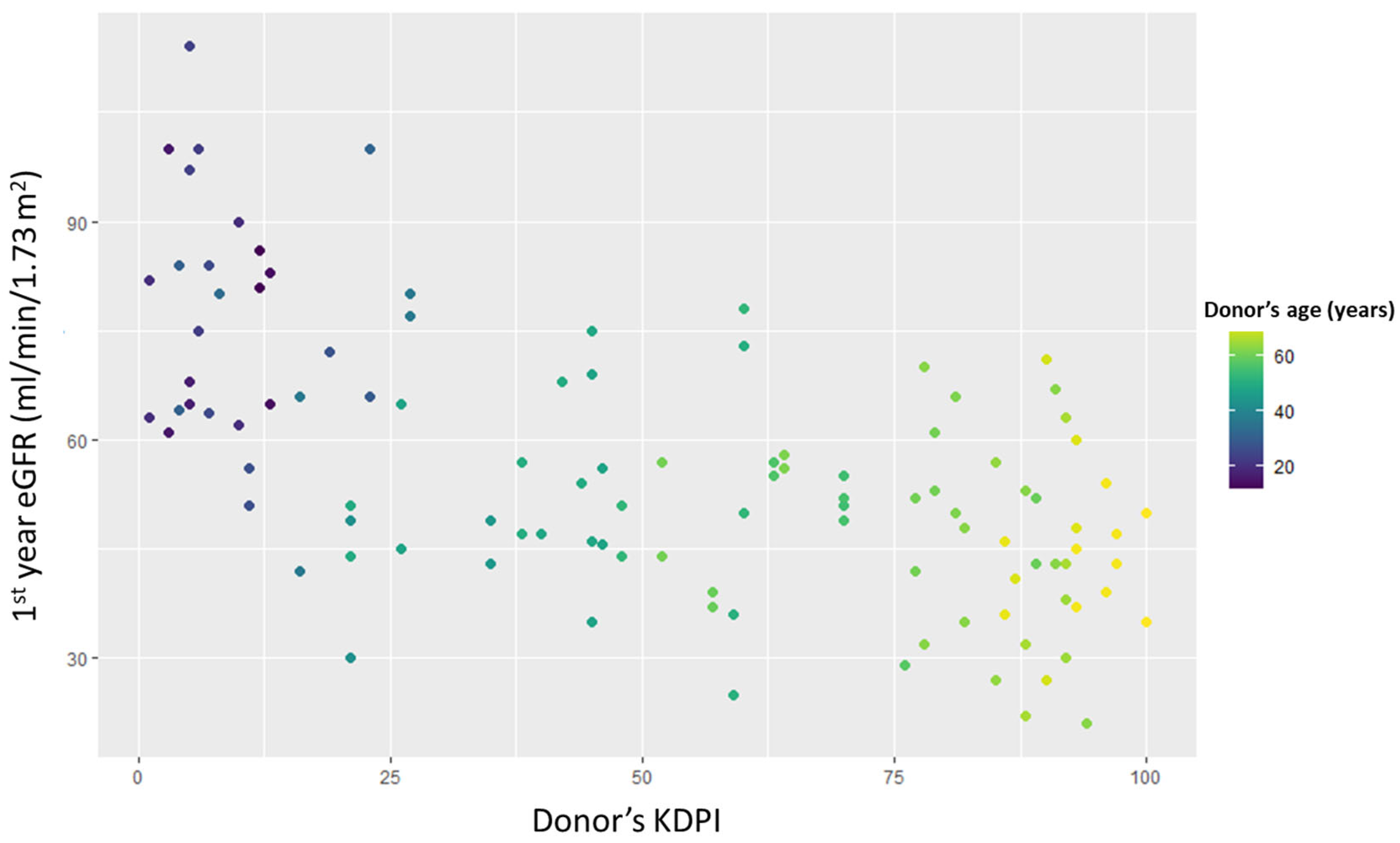
3.3. Kidney Function
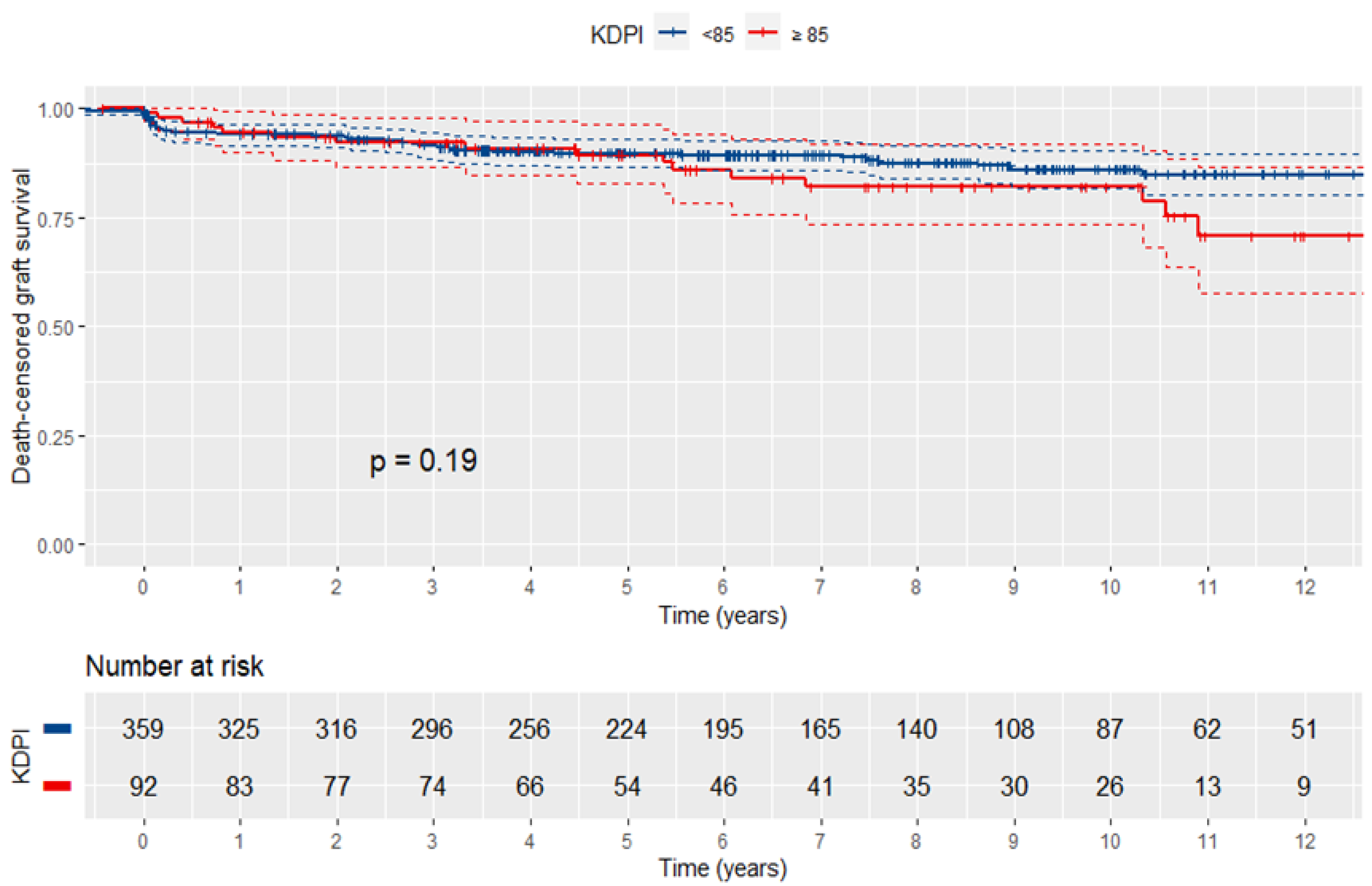
3.4. Graft Survival

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Crude Model | Model 1 | Model 2 | Model 3 | |
|---|---|---|---|---|
| eGFR—1st year | ||||
| Overall | ||||
| KDPI † | −0.33 (−0.38; −0.27) | −0.33 (−0.39; −0.28) | −0.33 (−0.39; −0.28) | −0.32 (−0.38; −0.26) |
| KDRI †† | −0.23 (−0.27; −0.19) | −0.24 (−0.28; −0.19) | −0.23 (−0.28; −0.19) | −0.22 (−0.27; −0.18) |
| Donor’s age † | −0.65 (−0.75; −0.55) | −0.63 (−0.73; −0.53) | −0.64 (−0.75; −0.54) | −0.62 (−0.72; −0.52) |
| Standard-criteria donor | ||||
| KDPI † | −0.38 (−0.48; −0.28) | −0.38 (−0.48; −0.28) | −0.38 (−0.48; −0.28) | −0.35 (−0.45; −0.24) |
| KDRI †† | −0.39 (−0.50; −0.29) | −0.39 (−0.50; −0.29) | −0.39 (−0.49; −0.28) | −0.35 (−0.46; −0.25) |
| Donor’s age † | −0.66 (−0.82; −0.50) | −0.66 (−0.81; −0.50) | −0.66 (−0.82; −0.50) | −0.62 (−0.78; −0.45) |
| Expanded-criteria donor | ||||
| KDPI † | −0.09 (−0.29; 0.11) | −0.10 (−0.31; 0.11) | −0.12 (−0.34; 0.09) | −0.11 (−0.33; 0.11) |
| KDRI †† | −0.05 (−0.12; 0.03) | −0.05 (−0.13; 0.03) | −0.06 (−0.15; 0.02) | −0.06 (−0.15; 0.03) |
| Donor’s age † | −0.22 (−0.63; 0.18) | −0.30 (−0.73; 0.13) | −0.34 (−0.79; 0.10) | −0.33 (−0.80; 0.14) |
| eGFR—3rd year | ||||
| Overall | ||||
| KDPI † | −0.31 (−0.37; −0.25) | −0.31 (−0.38; −0.25) | −0.31 (−0.38; −0.25) | −0.31 (−0.38; −0.25) |
| KDRI †† | −0.21 (−0.26; −0.16) | −0.22 (−0.27; −0.17) | −0.22 (−0.27; −0.17) | −0.21 (−0.26; −0.16) |
| Donor’s age † | −0.64 (−0.75; −0.52) | −0.65 (−0.76; −0.53) | −0.64 (−0.76; −0.53) | −0.63 (−0.75; −0.51) |
| Standard-criteria donor | ||||
| KDPI † | −0.41 (−0.52; −0.29) | −0.40 (−0.52; −0.29) | −0.40 (−0.51; −0.28) | −0.40 (−0.52; −0.28) |
| KDRI †† | −0.43 (−0.55; −0.31) | −0.43 (−0.55; −0.31) | −0.42 (−0.54; −0.30) | −0.41 (−0.53; −0.29) |
| Donor’s age † | −0.74 (−0.92; −0.55) | −0.73 (−0.91; −0.54) | −0.72 (−0.91; −0.54) | −0.71 (−0.89; −0.52) |
| Expanded-criteria donor | ||||
| KDPI † | −0.10 (−0.34; 0.14) | −0.10 (−0.34; 0.15) | −0.16 (−0.40; 0.09) | −0.09 (−0.34; 0.16) |
| KDRI †† | −0.03 (−0.13; 0.06) | −0.04 (−0.13; 0.06) | −0.06 (−0.16; 0.04) | −0.03 (−0.13; 0.07) |
| Donor’s age † | −0.43 (−0.89; 0.04) | −0.49 (−0.99; 0.04) | −0.57 (−1.08; −0.07) | −0.43 (−0.95; 0.09) |
| eGFR—5th year | ||||
| Overall | ||||
| KDPI † | −0.33 (−0.40; −0.27) | −0.34 (−0.41; −0.27) | −0.34 (−0.41; −0.27) | −0.33 (−0.41; −0.26) |
| KDRI †† | −0.23 (−0.28; −0.17) | −0.23 (−0.29; −0.18) | −0.23 (−0.29; −0.18) | −0.22 (−0.28; −0.17) |
| Donor’s age † | −0.71 (−0.84; −0.59) | −0.72 (−0.85; −0.60) | −0.72 (−0.84; −0.59) | −0.70 (−0.84; −0.57) |
| Standard-criteria donor | ||||
| KDPI † | −0.49 (−0.62; −0.36) | −0.49 (−0.62; −0.36) | −0.48 (−0.61; −0.34) | −0.47 (−0.60; −0.33) |
| KDRI †† | −0.49 (−0.63; −0.36) | −0.49 (−0.63; −0.36) | −0.48 (−0.62; −0.34) | −0.47 (−0.61; −0.33) |
| Donor’s age † | −0.92 (−1.13; −0.72) | −0.92 (−1.13; −0.72) | −0.91 (−1.12; −0.71) | −0.88 (−1.09; −0.67) |
| Expanded-criteria donor | ||||
| KDPI † | −0.19 (−0.46; 0.07) | −0.19 (−0.46; 0.09) | −0.24 (−0.51; 0.03) | −0.20 (−0.48; 0.08) |
| KDRI †† | −0.07 (−0.16; 0.03) | −0.06 (−0.17; 0.03) | −0.09 (−0.19; 0.01) | −0.07 (−0.17; 0.04) |
| Donor’s age † | −0.44 (−0.93; 0.04) | −0.47 (−0.97; 0.04) | −0.46 (−0.96; 0.05) | −0.35 (−0.89; 0.18) |
3.5. Overall Survival
3.6. Recipient Pairs Transplanted from the Same Donor
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Donor Characteristics | Category | Component |
|---|---|---|
| Age (years) | 18–50 | 0.0128 × (Age − 40) |
| <18 | −0.0194 × (Age − 18) | |
| >50 | 0.0107 × (Age − 50) | |
| Height (cm) | All | −0.0464 × (Height − 170)/10 |
| Weight (kg) | <80 | −0.0199 × (Weight − 80)/5 |
| Ethnicity | African American | 0.1790 |
| Hypertension | Yes | 0.1260 |
| Diabetes mellitus | Yes | 0.1300 |
| Death cause | Cerebrovascular accident | 0.0881 |
| Serum creatinine (mg/dL) | <1.5 | 0.2200 × (Creatinine − 1) |
| >1.5 | −0.2090 × (Creatinine − 1.5) | |
| Hepatitis C status | Positive | 0.2400 |
| Donation after Circulatory Death | Yes | 0.1330 |
| Overall Survival | ||||
|---|---|---|---|---|
| Crude Model | Model 1 | Model 2 | Model 3 | |
| Overall | ||||
| KDPI † | 1.00 (0.99–1.01) | 1.00 (0.99–1.01) | 1.00 (0.99–1.01) | 1.00 (0.99–1.01) |
| KDPI (Q4 vs. Q1) | 1.42 (0.77–2.64) | 1.33 (0.70–2.52) | 1.60 (0.83–3.06) | 1.25 (0.63–2.46) |
| KDPI ≥ 85 | 0.97 (0.56–1.68) | 0.84 (0.48–1.47) | 0.89 (0.50–1.57) | 0.83 (0.46–1.49) |
| KDRI † | 1.30 (0.77–2.21) | 1.08 (0.63–1.84) | 1.26 (0.72–2.18) | 1.13 (0.63–2.02) |
| KDRI (Q4 vs. Q1) | 1.35 (0.74–2.45) | 1.13 (0.61–2.11) | 1.25 (0.66–2.37) | 1.10 (0.57–2.13) |
| Donor’s age † | 1.01 (0.998–1.03) | 1.00 (0.99–1.02) | 1.01 (0.995–1.02) | 1.01 (0.99–1.02) |
| Standard-criteria donor | ||||
| KDPI † | 1.00 (0.99–1.02) | 1.00 (0.99–1.01) | 1.00 (0.99–1.02) | 1.00 (0.99–1.02) |
| KDPI (Q4 vs. Q1) | 1.26 (0.60–2.65) | 1.10 (0.50–2.45) | 1.13 (0.50–2.53) | 1.06 (0.45–2.48) |
| KDPI ≥85 | - | - | - | - |
| KDRI † | 1.22 (0.35–4.23) | 1.03 (0.27–3.85) | 1.14 (0.29–4.43) | 0.99 (0.22–4.42) |
| KDRI (Q4 vs. Q1) | 1.16 (0.54–2.49) | 1.02 (0.44–2.37) | 1.12 (0.48–2.66) | 1.01 (0.40–2.54) |
| Donor’s age † | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) |
| Expanded-criteria donor | ||||
| KDPI † | 0.99 (0.97–1.02) | 0.98 (0.96–1.01) | 0.99 (0.96–1.02) | 0.99 (0.96–1.02) |
| KDPI (Q4 vs. Q1) | 0.97 (0.37–2.56) | 0.73 (0.26–1.98) | 0.84 (0.30–2.34) | 0.96 (0.32–2.87) |
| KDPI ≥85 | 0.61 (0.31–1.21) | 0.52 (0.26–1.05) | 0.55 (0.27–1.12) | 0.55 (0.26–1.17) |
| KDRI † | 0.83 (0.28–2.43) | 0.48 (0.17–1.37) | 0.60 (0.20–1.77) | 0.74 (0.24–2.32) |
| KDRI (Q4 vs. Q1) | 1.33 (0.50–3.58) | 1.44 (0.53–3.87) | 1.26 (0.45–3.57) | 1.13 (0.40–3.18) |
| Donor’s age † | 1.01 (0.96–1.07) | 0.97 (0.92–1.03) | 0.97 (0.92–1.02) | 0.98 (0.92–1.05) |

References
- Thurlow, J.S.; Joshi, M.; Yan, G.; Norris, K.C.; Agodoa, L.Y.; Yuan, C.M.; Nee, R. Global Epidemiology of End-Stage Kidney Disease and Disparities in Kidney Replacement Therapy. Am. J. Nephrol. 2021, 52, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.C.; Held, P.J.; Port, F.K. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia Garcia, G.; Harden, P.; Chapman, J. The Global Role of Kidney Transplantation. Iran. J. Kidney Dis. 2012, 6, 81–87. [Google Scholar] [PubMed]
- Port, F.K.; Bragg-Gresham, J.L.; Metzger, R.A.; Dykstra, D.M.; Gillespie, B.W.; Young, E.W.; Delmonico, F.L.; Wynn, J.J.; Merion, R.M.; Wolfe, R.A.; et al. Donor Characteristics Associated with Reduced Graft Survival: An Approach to Expanding the Pool of Kidney Donors. Transplantation 2002, 74, 1281–1286. [Google Scholar] [CrossRef] [PubMed]
- Querard, A.H.; Foucher, Y.; Combescure, C.; Dantan, E.; Larmet, D.; Lorent, M.; Pouteau, L.M.; Giral, M.; Gillaizeau, F. Comparison of Survival Outcomes between Expanded Criteria Donor and Standard Criteria Donor Kidney Transplant Recipients: A Systematic Review and Meta-Analysis. Transpl. Int. 2016, 29, 403–415. [Google Scholar] [CrossRef] [Green Version]
- Rao, P.S.; Schaubel, D.E.; Guidinger, M.K.; Andreoni, K.A.; Wolfe, R.A.; Merion, R.M.; Port, F.K.; Sung, R.S. A Comprehensive Risk Quantification Score for Deceased Donor Kidneys: The Kidney Donor Risk Index. Transplantation 2009, 88, 231–236. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Organ Procurement and Transplantation Network: KDPI Calculator. Available online: https://optn.transplant.hrsa.gov/data/allocation-calculators/kdpi-calculator/ (accessed on 10 August 2022).
- Rose, C.; Sun, Y.; Ferre, E.; Gill, J.; Landsberg, D.; Gill, J. An Examination of the Application of the Kidney Donor Risk Index in British Columbia. Can. J. Kidney Health Dis. 2018, 5, 2054358118761052. [Google Scholar] [CrossRef] [Green Version]
- Metzger, R.A.; Delmonico, F.L.; Feng, S.; Port, F.K.; Wynn, J.J.; Merion, R.M. Expanded Criteria Donors for Kidney Transplantation. Am. J. Transplant. 2003, 3 (Suppl. 4), 114–125. [Google Scholar] [CrossRef] [Green Version]
- Organ Procurement and Transplantation Network. KDRI to KDPI Mapping Table 2020. Available online: https://optn.transplant.hrsa.gov/media/2150/kdpi_mapping_table.pdf (accessed on 10 August 2022).
- Organ Procurement and Transplantation Network Estimated Post Transplant Survival Calculator. Available online: https://optn.transplant.hrsa.gov/resources/allocation-calculators/epts-calculator (accessed on 10 August 2022).
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Therneau, T. A Package for Survival Analysis in R; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Kassambara, A.; Kosinski, M.; Biecek, P. Package “Survminer” Type Package Title Drawing Survival Curves Using “Ggplot2”; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Massey, F.J. The Kolmogorov-Smirnov Test for Goodness of Fit. J. Am. Stat. Assoc. 1951, 46, 68–78. [Google Scholar] [CrossRef]
- Fay, M.P.; Proschan, M.A. Wilcoxon-Mann-Whitney or T-Test? On Assumptions for Hypothesis Tests and Multiple Interpretations of Decision Rules. Stat. Surv. 2010, 4, 1–39. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical Notes for Clinical Researchers: Chi-Squared Test and Fisher’s Exact Test. Restor. Dent. Endod. 2017, 42, 152. [Google Scholar] [CrossRef]
- Harrell, F.E.; Lee, K.L.; Califf, R.M.; Pryor, D.B.; Rosati, R.A. Regression Modelling Strategies for Improved Prognostic Prediction. Stat. Med. 1984, 3, 143–152. [Google Scholar] [CrossRef]
- Lehner, L.J.; Kleinsteuber, A.; Halleck, F.; Khadzhynov, D.; Schrezenmeier, E.; Duerr, M.; Eckardt, K.U.; Budde, K.; Staeck, O. Assessment of the Kidney Donor Profile Index in a European Cohort. Nephrol. Dial. Transplant. 2018, 33, 1465–1472. [Google Scholar] [CrossRef]
- Dahmen, M.; Becker, F.; Pavenstädt, H.; Suwelack, B.; Schütte-Nütgen, K.; Reuter, S. Validation of the Kidney Donor Profile Index (KDPI) to Assess a Deceased Donor’s Kidneys’ Outcome in a European Cohort. Sci. Rep. 2019, 9, 11234. [Google Scholar] [CrossRef] [Green Version]
- Arias-Cabrales, C.; Pérez-Sáez, M.J.; Redondo-Pachón, D.; Buxeda, A.; Burballa, C.; Bermejo, S.; Sierra, A.; Mir, M.; Burón, A.; Zapatero, A.; et al. Usefulness of the KDPI in Spain: A Comparison with Donor Age and Definition of Standard/Expanded Criteria Donor. Nefrol. (Engl. Ed.) 2018, 38, 503–513. [Google Scholar] [CrossRef]
- Sexton, D.J.; O’Kelly, P.; Kennedy, C.; Denton, M.; De Freitas, D.G.; Magee, C.; O’Seaghdha, C.M.; Conlon, P.J. Assessing the Discrimination of the Kidney Donor Risk Index/Kidney Donor Profile Index Scores for Allograft Failure and Estimated Glomerular Filtration Rate in Ireland’s National Kidney Transplant Programme. Clin. Kidney J. 2019, 12, 569–573. [Google Scholar] [CrossRef]
- Jun, H.; Yoon, H.E.; Lee, K.W.; Lee, D.R.; Yang, J.; Ahn, C.; Han, S.Y. Kidney Donor Risk Index Score Is More Reliable Than Kidney Donor Profile Index in Kidney Transplantation from Elderly Deceased Donors. Transplant. Proc. 2020, 52, 1744–1748. [Google Scholar] [CrossRef]
- Formica, R.N. A Critical Assessment on Kidney Allocation Systems. Transplant. Rev. 2017, 31, 61–67. [Google Scholar] [CrossRef]
- Philipse, E.; Lee, A.P.K.; Bracke, B.; Hartman, V.; Chapelle, T.; Roeyen, G.; De Greef, K.; Ysebaert, D.K.; Van Beeumen, G.; Couttenye, M.M.; et al. Does Kidney Donor Risk Index Implementation Lead to the Transplantation of More and Higher-Quality Donor Kidneys? Nephrol. Dial. Transplant. 2017, 32, 1934–1938. [Google Scholar] [CrossRef] [Green Version]
- Pippias, M.; Stel, V.S.; Arnol, M.; Bemelman, F.; Berger, S.P.; Buturovic Ponikvar, J.B.; Kramar, R.; Magaz, Á.; Nordio, M.; Peters-Sengers, H.; et al. Temporal Trends in the Quality of Deceased Donor Kidneys and Kidney Transplant Outcomes in Europe: An Analysis by the ERA-EDTA Registry. Nephrol. Dial. Transplant. 2022, 37, 175. [Google Scholar] [CrossRef] [PubMed]



| Variable | Overall | Expanded-Criteria Donor | p-Value | |
|---|---|---|---|---|
| Yes | No | |||
| Donors | ||||
| Patients no. | 394 | 143 | 251 | |
| Age (years) | 53 [39.3–61] | 64 [61–69] | 45 [30.5–52.5] | <0.001 |
| Male sex | 225 (57.1%) | 69 (48.3%) | 156 (62.2%) | 0.010 |
| BMI (kg/m2) | 26.2 [24.2–28.6] | 26.6 [24.8–29.5] | 26.2 [23.7–27.8] | 0.006 |
| Diabetes mellitus | 26 (6.6%) | 20 (14.0%) | 6 (2.4%) | <0.001 |
| Hypertension | 117 (29.7%) | 79 (55.2%) | 38 (15.1%) | <0.001 |
| Serum creatinine (mg/dL) | 0.80 [0.60–1.00] | 0.83 [0.63–1.10] | 0.80 [0.60–1.07] | 0.270 |
| KDPI | 54 [26–79] | 86 [76–92] | 33 [16–52] | <0.001 |
| KDRI | 1.02 [0.78–1.34] | 1.48 [1.29–1.64] | 0.84 [0.70–1.01] | <0.001 |
| Recipients | ||||
| Patients no. | 456 | 169 | 287 | |
| Age (years) | 52 [43–59] | 54 [45–61.8] | 51 [42–59] | <0.001 |
| Male sex | 264 (57.9%) | 95 (56.2%) | 169 (58.9%) | 0.646 |
| BMI (kg/m2) | 25.0 [23.0–27.7] | 25.0 [22.8–27.2] | 24.8 [23.0–27.7] | 0.738 |
| Diabetes mellitus | 25 (5.5%) | 9 (5.3%) | 16 (5.6%) | 1 |
| Dialysis vintage (years) | 7 [5–9] | 7 [5–8] | 7 [5–9] | 0.768 |
| EPTS score | 37 [21–57] | 41 [22–64] | 34.5 [18.8–57] | 0.072 |
| Induction therapy | ||||
| Basiliximab | 346 (75.9%) | 107 (63.3%) | 239 (83.3%) | <0.001 |
| Basiliximab + Rituximab | 23 (5.0%) | 13 (7.7%) | 10 (3.5%) | |
| Daclizumab | 37 (8.1%) | 19 (11.2%) | 18 (6.3%) | |
| Antithymocyte globulin | 50 (11.0%) | 30 (17.8%) | 20 (7.0%) | |
| Maintenance immunosuppression | ||||
| MMF/CNI/Corticosteroids | 398 (87.3%) | 136 (80.5%) | 262 (91.3%) | <0.001 |
| MMF/mTORi/Corticosteroids | 1 (0.2%) | 0 (0.0%) | 1 (0.3%) | |
| mTORi/CNI/Corticosteroids | 23 (5.0%) | 9 (5.3%) | 14 (4.9%) | |
| MMF/Corticosteroids | 32 (7.0%) | 24 (14.2%) | 8 (2.8%) | |
| Delayed graft function | 169 (37.1%) | 78 (46.2%) | 91 (31.7%) | 0.558 |
| eGFR—1st year (mL/min/1.73 m2) | 54 [42.3–68] | 46.7 [37–56.8] | 59.5 [47–75] | <0.001 |
| eGFR—3rd year (mL/min/1.73 m2) | 52 [41–70] | 46 [37–56] | 57 [43–72] | <0.001 |
| eGFR—5th year (mL/min/1.73 m2) | 52 [41–67] | 46 [35–56] | 59 [43–76] | <0.001 |
| Graft loss | 58 (12.7%) | 28 (16.6%) | 30 (11.9%) | 0.086 |
| Death | 89 (19.5%) | 34 (20.1%) | 55 (19.2%) | 0.942 |
| Follow-up period (years) | 6.3 [3.6–10] | 7.5 [4.5–10.6] | 7.3 [4.03–10.2] | 0.965 |
| Death-Censored Graft Loss | ||||
|---|---|---|---|---|
| Crude Model | Model 1 | Model 2 | Model 3 | |
| Overall | ||||
| KDPI † | 1.01 (0.998–1.02) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) | 1.01 (1.00–1.02) |
| KDPI (Q4 vs. Q1) | 1.87 (0.87–4.03) | 2.68 (1.09–6.59) | 2.91 (1.14–7.42) | 3.07 (1.20–7.89) |
| KDPI ≥ 85 | 1.47 (0.82–2.61) | 1.79 (0.99–3.21) | 1.58 (0.84–2.96) | 1.53 (0.81–2.88) |
| KDRI † | 1.65 (0.90–3.02) | 2.37 (1.25–4.47) | 2.23 (1.16–4.31) | 2.21 (1.16–4.22) |
| KDRI (Q4 vs. Q1) | 1.80 (0.86–3.79) | 2.84 (1.24–6.51) | 3.08 (1.21–7.87) | 3.32 (1.29–8.53) |
| Donor’s age † | 1.01 (0.99–1.02) | 1.02 (0.999–1.04) | 1.02 (1.00–1.04) | 1.03 (1.00–1.05) |
| Standard-criteria donor | ||||
| KDPI † | 1.00 (0.99–1.02) | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) |
| KDPI (Q4 vs. Q1) | 1.51 (0.54–4.24) | 1.88 (0.66–6.10) | 1.99 (0.59–6.76) | 2.08 (0.60–7.19) |
| KDPI ≥ 85 | - | - | - | - |
| KDRI † | 0.98 (0.18–5.29) | 1.97 (0.33–11.82) | 2.82 (0.43–18.61) | 2.90 (0.41–20.46) |
| KDRI (Q4 vs. Q1) | 1.31 (0.45–3.77) | 2.20 (0.65–7.40) | 2.21 (0.65–7.50) | 2.34 (0.68–8.04) |
| Donor’s age † | 1.00 (0.97–1.02) | 1.00 (0.97–1.03) | 1.01 (0.98–1.05) | 1.01 (0.98–1.05) |
| Expanded-criteria donor | ||||
| KDPI † | 1.00 (0.97–1.03) | 1.00 (0.97–1.03) | 1.00 (0.96–1.03) | 0.99 (0.96–1.02) |
| KDPI (Q4 vs. Q1) | 1.07 (0.41–2.76) | 1.12 (0.43–2.91) | 0.98 (0.36–2.65) | 0.85 (0.31–2.30) |
| KDPI ≥ 85 | 1.11 (0.52–2.36) | 1.14 (0.53–2.43) | 1.01 (0.46–2.22) | 0.81 (0.37–1.78) |
| KDRI † | 1.40 (0.43–4.53) | 1.62 (0.47–5.55) | 1.42 (0.39–5.20) | 1.03 (0.29–3.71) |
| KDRI (Q4 vs. Q1) | 1.33 (0.50–3.58) | 1.44 (0.53–3.87) | 1.26 (0.45–3.57) | 1.13 (0.40–3.18) |
| Donor’s age † | 1.00 (0.94–1.06) | 1.02 (0.95–1.09) | 1.01 (0.95–1.08) | 1.01 (0.94–1.08) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darema, M.; Athanasopoulou, D.; Bellos, I.; Tsoumbou, I.; Vittoraki, A.G.; Bokos, J.; Marinaki, S.; Boletis, I.N. Evaluation of Kidney Donor Risk Index/Kidney Donor Profile Index as Predictor Tools of Deceased-Donor Kidney Transplant Outcomes in a Greek Cohort. J. Clin. Med. 2023, 12, 2439. https://doi.org/10.3390/jcm12062439
Darema M, Athanasopoulou D, Bellos I, Tsoumbou I, Vittoraki AG, Bokos J, Marinaki S, Boletis IN. Evaluation of Kidney Donor Risk Index/Kidney Donor Profile Index as Predictor Tools of Deceased-Donor Kidney Transplant Outcomes in a Greek Cohort. Journal of Clinical Medicine. 2023; 12(6):2439. https://doi.org/10.3390/jcm12062439
Chicago/Turabian StyleDarema, Maria, Diamanto Athanasopoulou, Ioannis Bellos, Ioanna Tsoumbou, Angeliki G. Vittoraki, John Bokos, Smaragdi Marinaki, and Ioannis N. Boletis. 2023. "Evaluation of Kidney Donor Risk Index/Kidney Donor Profile Index as Predictor Tools of Deceased-Donor Kidney Transplant Outcomes in a Greek Cohort" Journal of Clinical Medicine 12, no. 6: 2439. https://doi.org/10.3390/jcm12062439
APA StyleDarema, M., Athanasopoulou, D., Bellos, I., Tsoumbou, I., Vittoraki, A. G., Bokos, J., Marinaki, S., & Boletis, I. N. (2023). Evaluation of Kidney Donor Risk Index/Kidney Donor Profile Index as Predictor Tools of Deceased-Donor Kidney Transplant Outcomes in a Greek Cohort. Journal of Clinical Medicine, 12(6), 2439. https://doi.org/10.3390/jcm12062439