
Is Intermittent Abdominal Pressure Ventilation Still Relevant? A Multicenter Retrospective Pilot Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
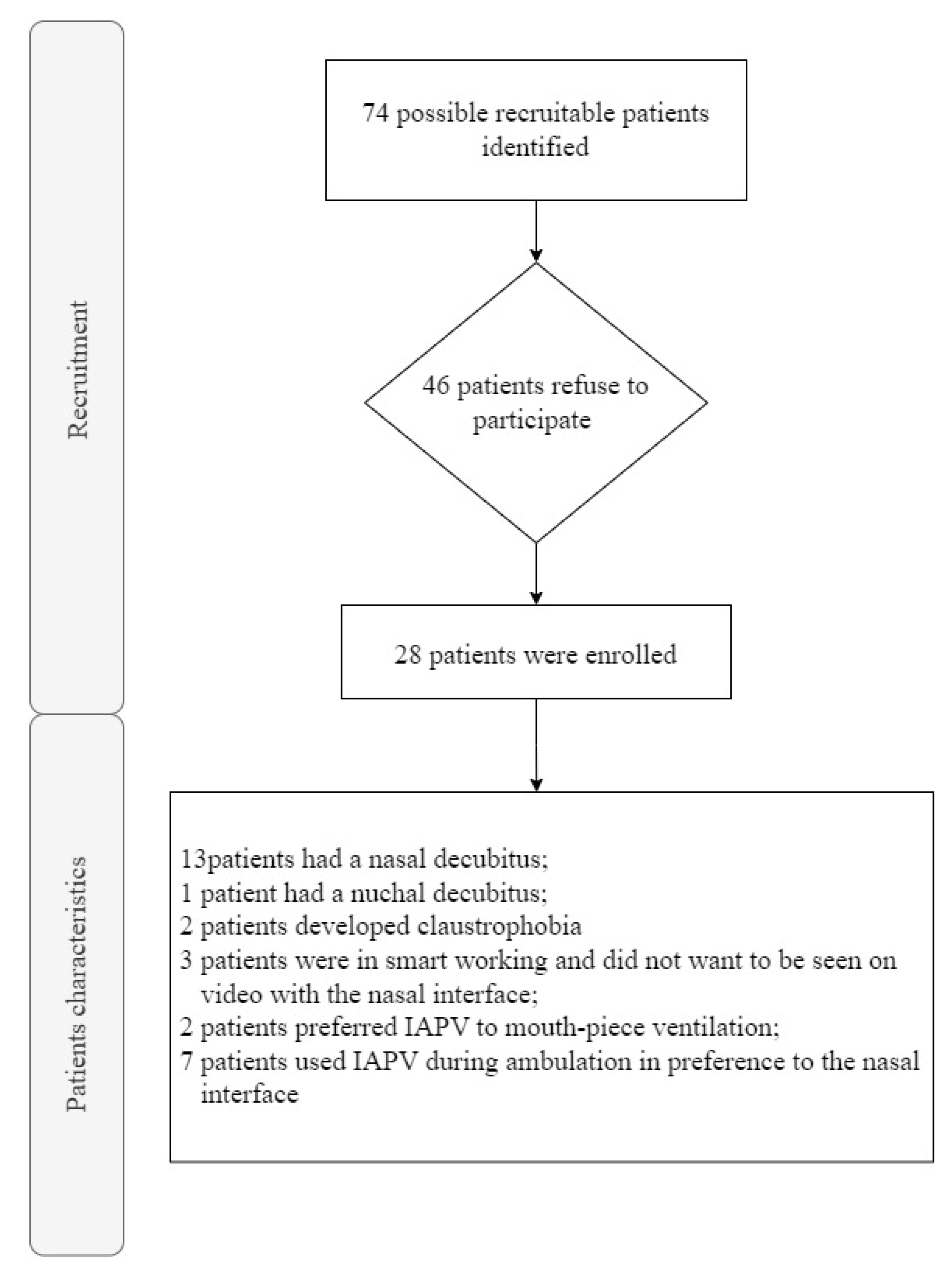
2.1. Study Design and Participants
2.2. Interventions
2.3. Outcome Measures
2.4. Measurements
- -
- Spirometry: Forced Vital Capacity (FVC), Forced Expiratory Volume in the first second (FEV1) and Tiffeneau Index (FEV1/FVC), obtained through the Master Screen Body Jaeger Vyntus™ Pneumo, Vyaire, Mettawa, IL, USA.
- -
- IAPV settings for the expiratory and inspiratory volumes and respiratory frequency, obtained via Citrex H4, DIMA Italia, Bologna [10].
- -
- Strength of respiratory muscles: Maximal Inspiratory Pressure (MIP) and Maximal Expiratory Pressure (MEP), obtained using a MicroRPM Pressure Meter, Micro Medical Ltd., Lewiston, ME, USA.
- -
- Blood gas analysis (BGA) (pH (measured acid-base balance of the blood); partial pressure of oxygen (PaO2); Partial pressure of carbon dioxide (PaCO2); and bicarbonate (HCO3−)), obtained using the GEM 3500, Instrumentation Laboratory, Milan, Italy.
- -
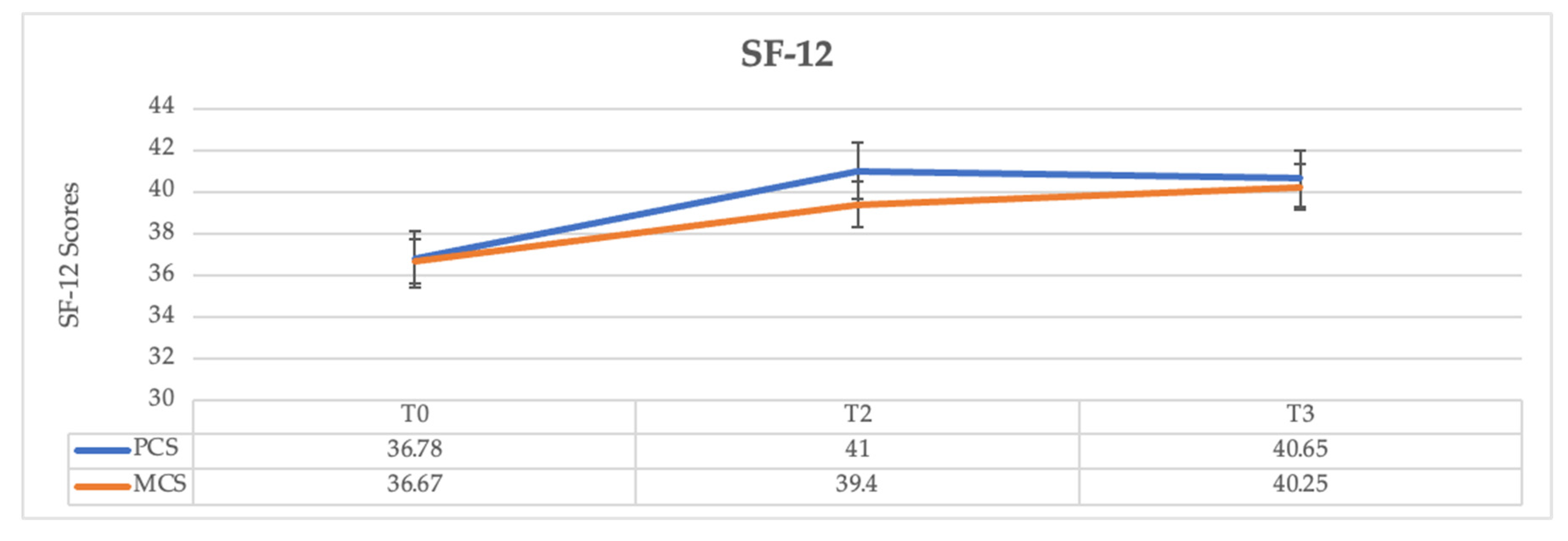
- Quality of life (QoL) was assessed by the administration of the Short Form-12 Questionnaire (SF-12) [11], a shortened version of its predecessor, the SF-36 [12], which, in turn, evolved from the Medical Outcomes Study. After two hours (T1) of ventilation with IAPV, the following variables were investigated:
- -
- Respiratory Rate (RR).
- -
- Inspiratory/expiratory volume, measured for one minute during spontaneous breathing and 10’ after starting IAPV for another minute.
- -
- BGA.
- -
- Spirometry (FVC, FEV1, FEV1/FVC).
- -
- Inspiratory/expiratory volume, measured for one minute during spontaneous breathing and 10’ after starting IAPV for another minute.
- -
- Quality of life.
- -
- Spirometry.
- -
- Quality of life.
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hess, D.R. Noninvasive ventilation in neuromuscular disease: Equipment and application. Respir. Care 2006, 51, 896–911; discussion 911–912. [Google Scholar]
- Fiorentino, G.; Annunziata, A.; Gaeta, A.M.; Lanza, M.; Esquinas, A. Continuous noninvasive ventilation for respiratory failure in patients with amyotrophic lateral sclerosis: Current perspectives. Degener. Neurol. Neuromuscul. Dis. 2018, 8, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach, J.R.; Alba, A.S. Intermittent Abdominal Pressure Ventilator in a Regimen of Noninvasive Ventilatory Support. Chest 1991, 99, 630–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardus, D.; Vallbona, C.; Spencer, W.A. Effects of Three Kinds of Artificial Respirators on the Pulmonary Ventilation and Arterial Blood of Patients with Chronic Respiratory Insufficiency. Dis. Chest 1966, 50, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Pierucci, P.; Di Lecce, V.; Carpagnano, G.E.; Banfi, P.; Bach, J.R. The Intermittent Abdominal Pressure Ventilator as an Alternative Modality of Noninvasive Ventilatory Support: A Narrative Review. Am. J. Phys. Med. Rehabil. 2022, 101, 179–183. [Google Scholar] [CrossRef]
- Puricelli, C.; Volpato, E.; Sciurello, S.; Nicolini, A.; Banfi, P. Intermittent abdominal pressure ventilation: Feasibility and efficacy in neuromuscular disease. A case report. Monaldi Arch. Chest Dis. 2021, 91. [Google Scholar] [CrossRef]
- Fiorentino, G.; Annunziata, A.; Coppola, A.; Marotta, A.; Simioli, F.; Imitazione, P.; Lanza, M.; Cauteruccio, R.; Esquinas, A.M. Intermittent Abdominal Pressure Ventilation: An Alternative for Respiratory Support. Can. Respir. J. 2021, 2021, 5554765. [Google Scholar] [CrossRef] [PubMed]
- De Mattia, E.; Iatomasi, M.; Garabelli, B.; Lunetta, C.; Sansone, V.; Rao, F. Use of the Intermittent Abdominal Pressure Ventilation to guarantee speech in a tracheostomised Amyotrophic Lateral Sclerosis patient. Rev. Port. Pneumol. 2017, 23, 236–239. [Google Scholar] [CrossRef]
- Pierucci, P.; Bach, J.; Valentina, V.D.L.; Banfi, P.; Carpagnano, G.; Resta, O. Daytime non-invasive ventilatory support via intermittent abdominal pressure for a patient with Pompe disease. Pulmonology 2021, 27, 182–184. [Google Scholar] [CrossRef]
- Baboi, L.; Subtil, F.; Guérin, C. A bench evaluation of fraction of oxygen in air delivery and tidal volume accuracy in home care ventilators available for hospital use. J. Thorac. Dis. 2016, 8, 3639–3647. [Google Scholar] [CrossRef] [Green Version]
- Monica 1776 Main Street Santa, California 90401-3208. 12-Item Short form Survey from the RAND Medical Outcomes Study. Available online: https://www.rand.org/health-care/surveys_tools/mos/12-item-short-form.html (accessed on 23 January 2023).
- Ware, J.E., Jr. SF-36 Health Survey Update. Spine 2000, 25, 3130–3139. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E.R.; Bye, P.T.; Bruderer, J.W.; Sullivan, C.E. Treatment of respiratory failure during sleep in patients with neuromuscular disease. Positive-pressure ventilation through a nose mask. Am. Rev. Respir. Dis. 1987, 135, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Kerby, G.R.; Mayer, L.S.; Pingleton, S.K. Nocturnal positive pressure ventilation via nasal mask. Am. Rev. Respir. Dis. 1987, 135, 738–740. [Google Scholar] [CrossRef] [PubMed]
- Cross, A.M. Review of the role of non-invasive ventilation in the emergency department. Emerg. Med. J. 2000, 17, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Liesching, T.; Kwok, H.; Hill, N.S. Acute Applications of Noninvasive Positive Pressure Ventilation. Chest 2003, 124, 699–713. [Google Scholar] [CrossRef]
- American Thoracic Society; Infectious Diseases Society of America. Guidelines for the Management of Adults with Hospital-acquired, Ventilator-associated, and Healthcare-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2005, 171, 388–416. [Google Scholar] [CrossRef] [Green Version]
- Chastre, J.; Fagon, J.-Y. Ventilator-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2002, 165, 867–903. [Google Scholar] [CrossRef]
- Melsen, W.G.; Rovers, M.; Koeman, M.; Bonten, M.J.M. Estimating the attributable mortality of ventilator-associated pneumonia from randomised prevention studies. Crit. Care Med. 2011, 39, 2736–2742. [Google Scholar] [CrossRef]
- Melsen, W.G.; Rovers, M.M.; Groenwold, R.H.; Bergmans, D.C.; Camus, C.; Bauer, T.T.; Hanisch, E.W.; Klarin, B.; Koeman, M.; Krueger, W.A.; et al. Attributable mortality of ventilator-associated pneumonia: A meta-analysis of individual patient data from randomised prevention studies. Lancet Infect. Dis. 2013, 13, 665–671. [Google Scholar] [CrossRef]
- Pulmonary Rehabilitation—The Obstructive and Paralytic Conditions by Bach, John R. (MD): Very Good Hardcover (1996) First Edition.|UHR Books. Available online: https://www.abebooks.com/first-edition/Pulmonary-Rehabilitation-Obstructive-Paralytic-Conditions-Bach/1007548809/bd (accessed on 23 January 2023).
- Finlay, G.; Concannon, D.; McDonnell, T.J. Treatment of respiratory failure due to kyphoscoliosis with nasal intermittent positive pressure ventilation (NIPPV). Ir. J. Med. Sci. 1995, 164, 28–30. [Google Scholar] [CrossRef]
- Pierucci, P.; Portacci, A.; Carpagnano, G.E.; Banfi, P.; Crimi, C.; Misseri, G.; Gregoretti, C. The right interface for the right patient in noninvasive ventilation: A systematic review. Expert Rev. Respir. Med. 2022, 16, 931–944. [Google Scholar] [CrossRef]
- Bach, J.R. Body Ventilator Use for the Ventilatory Support of Individuals with Neuromuscular Disease. J. Neurol. Rehabil. 1992, 6, 81–86. [Google Scholar] [CrossRef]
- McSweeney, C.J. Bragg-Paul Pulsator for Respiratory Paralysis. BMJ 1938, 1, 1206–1207. [Google Scholar] [CrossRef] [Green Version]
- Adamson, J.P.; Lewis, L.; Stein, J.D. Application of Abdominal Pressure for Artificial Respiration. J. Am. Med. Assoc. 1959, 169, 1613–1617. [Google Scholar] [CrossRef]
- Bach, J.R. Noninvasive Ventilation Is More Than Mask Ventilation. Chest 2003, 123, 2156–2157. [Google Scholar] [CrossRef]
- Miller, H.J.; Thomas, E.; Wilmot, C.B. Pneumobelt use among high quadriplegic population. Arch. Phys. Med. Rehabil. 1988, 69, 369–372. [Google Scholar]
- Yang, G.F.; Alba, A.; Lee, M.; Khan, A. Pneumobelt for sleep in the ventilator user: Clinical experience. Arch. Phys. Med. Rehabil. 1989, 70, 707–711. [Google Scholar] [PubMed]
- Bach, J.R. Noninvasive Respiratory Management of Patients With Neuromuscular Disease. Ann. Rehabil. Med. 2017, 41, 519–538. [Google Scholar] [CrossRef] [Green Version]
- Nardi, J.; Leroux, K.; Orlikowski, D.; Prigent, H.; Lofaso, F. Home monitoring of daytime mouthpiece ventilation effectiveness in patients with neuromuscular disease. Chronic Respir. Dis. 2016, 13, 67–74. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Sample (N = 28) |
|---|---|
| Age | 54.5 (±16.3) |
| Female, % | 35.7 (±0.50) |
| Age at onset of NVS, yr | 40.35 (±16.63) |
| NVS use, mo | 139.5 (±255.8) |
| NVS use time (h/day) | 18.3 (±2.54) |
| pH | 7.41 (±0.03) |
| PaCO2 (mmHg) | 50.1 (±5.33) |
| PaO2 (mmHg) | 62.6 (±7.46) |
| HCO3− (mmHg) | 32.3 (±4.76) |
| FVC % | 31 (±15) |
| FEV1% | 33.8 (±15.1) |
| FEV1/FVC | 89.7 (±9.06) |
| MIP | 28.7 (±10.3) |
| MEP | 32.1 (±10.8) |
| Spontaneous Breathing (T0) | IAPV after 2 h (T1) | |||
|---|---|---|---|---|
| Min | Max | Min | Max | |
| Frequency | 27 (±4.36) | 32 (±4.22) | 15.0 (±1.12) | 15.0 (±1.12) |
| Inspiratory Volume | 197 (±38.5) | 254 (±49.4) | 731 (±72.6) | 802 (±75.1) |
| Expiratory Volume | 196 (±38.9) | 258 (±50.4) | 730 (±79.4) | 835 (±75.9) |
| T0 | T1 | T2 | T3 | |
|---|---|---|---|---|
| pH | 7.41 (±0.03) | 7.47 (±0.03) | 7.40 (±0.02) | 7.40 (±0.02) |
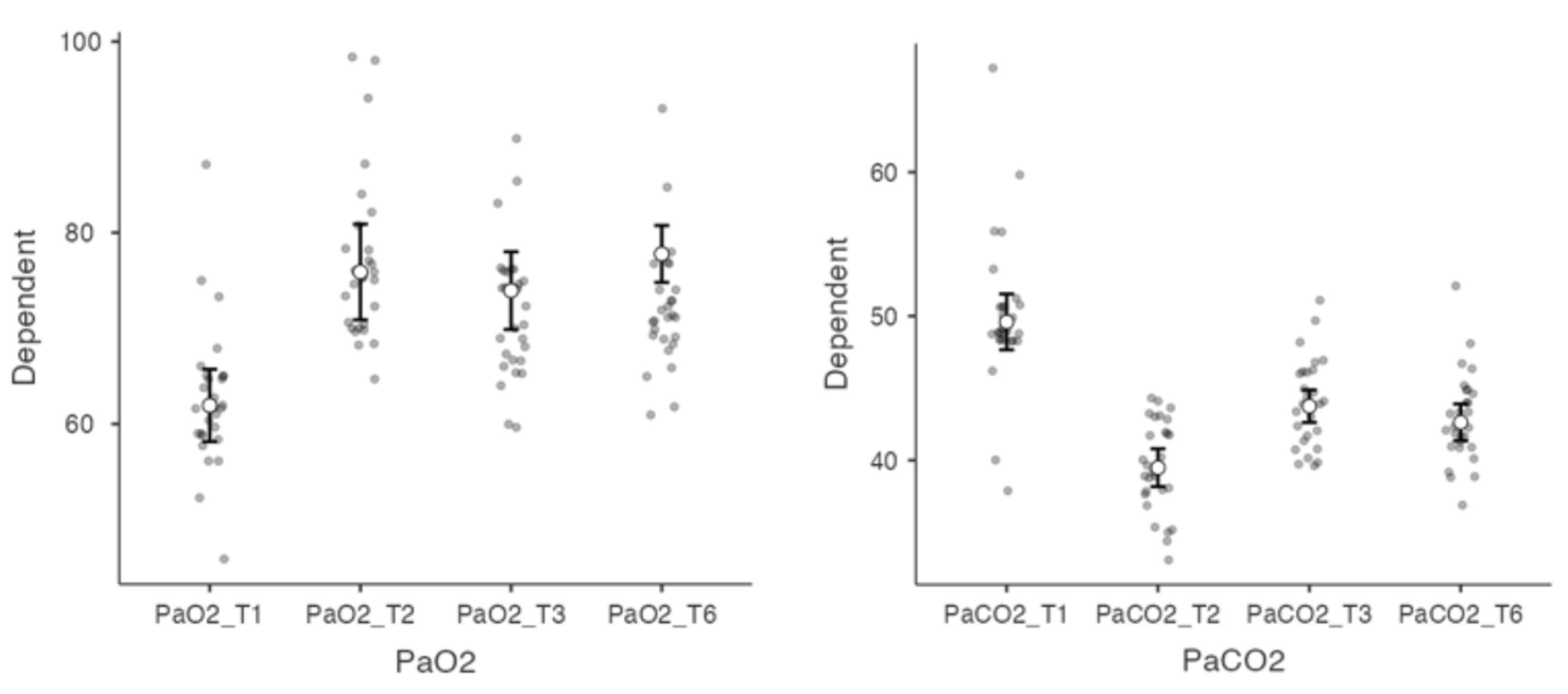
| PaCO2 (mmHg) | 50.1 (±5.33) | 39.6 (±3.25) | 44.0 (±2.99) | 42.85 (±3.12) |
| PaO2 (mmHg) | 62.6 (±7.46) | 76.9 (±8.63) | 71.8 (±7.01) | 72.32 (±7.01) |
| HCO3− (mmHg) | 32.3 (±4.76) | 30.3 (±4.29) | 28 (±2.90) | 28.53 (±2.33) |
| MIP | 28.7 (±10.3) | n.a. | 32.2(±30) | n.a. |
| MEP | 32.1 (±10.8) | n.a. | 36.5 (35.5) | n.a. |
| Variation | p | |
|---|---|---|
| PaO2_T0–PaO2_T1 | 12.23 | <0.001 |
| PaO2_T0–PaO2_T2 | 7.79 | <0.001 |
| PaO2_T0–PaO2_T3 | 9.51 | <0.001 |
| PaCO2_T0–PaCO2_T1 | 13.77 | <0.001 |
| PaCO2_T0–PaCO2_T2 | 6.97 | <0.001 |
| PaCO2_T0–PaCO2_T3 | 8.42 | <0.001 |
| PaO2_T1–PaO2_T2 | 4.44 | <0.001 |
| PaO2_T1–PaO2_T3 | 2.72 | 0.007 |
| PaCO2_T1–PaCO2_T2 | 6.79 | <0.001 |
| PaCO2_T1–PaCO2_T3 | 5.34 | <0.001 |
| PaO2_T2–PaO2_T3 | 1.72 | 0.087 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Volpi, V.; Volpato, E.; Compalati, E.; Pierucci, P.; Nicolini, A.; Lax, A.; Fagetti, L.; Annunziata, A.; Cauteruccio, R.; Fiorentino, G.; et al. Is Intermittent Abdominal Pressure Ventilation Still Relevant? A Multicenter Retrospective Pilot Study. J. Clin. Med. 2023, 12, 2453. https://doi.org/10.3390/jcm12072453
Volpi V, Volpato E, Compalati E, Pierucci P, Nicolini A, Lax A, Fagetti L, Annunziata A, Cauteruccio R, Fiorentino G, et al. Is Intermittent Abdominal Pressure Ventilation Still Relevant? A Multicenter Retrospective Pilot Study. Journal of Clinical Medicine. 2023; 12(7):2453. https://doi.org/10.3390/jcm12072453
Chicago/Turabian StyleVolpi, Valeria, Eleonora Volpato, Elena Compalati, Paola Pierucci, Antonello Nicolini, Agata Lax, Laura Fagetti, Anna Annunziata, Rosa Cauteruccio, Giuseppe Fiorentino, and et al. 2023. "Is Intermittent Abdominal Pressure Ventilation Still Relevant? A Multicenter Retrospective Pilot Study" Journal of Clinical Medicine 12, no. 7: 2453. https://doi.org/10.3390/jcm12072453
APA StyleVolpi, V., Volpato, E., Compalati, E., Pierucci, P., Nicolini, A., Lax, A., Fagetti, L., Annunziata, A., Cauteruccio, R., Fiorentino, G., & Banfi, P. (2023). Is Intermittent Abdominal Pressure Ventilation Still Relevant? A Multicenter Retrospective Pilot Study. Journal of Clinical Medicine, 12(7), 2453. https://doi.org/10.3390/jcm12072453