
Analysis of Clinical Factors Associated with Medical Burden and Functional Status in Pyogenic Spine Infection


Abstract
:1. Introduction
2. Patients and Methods
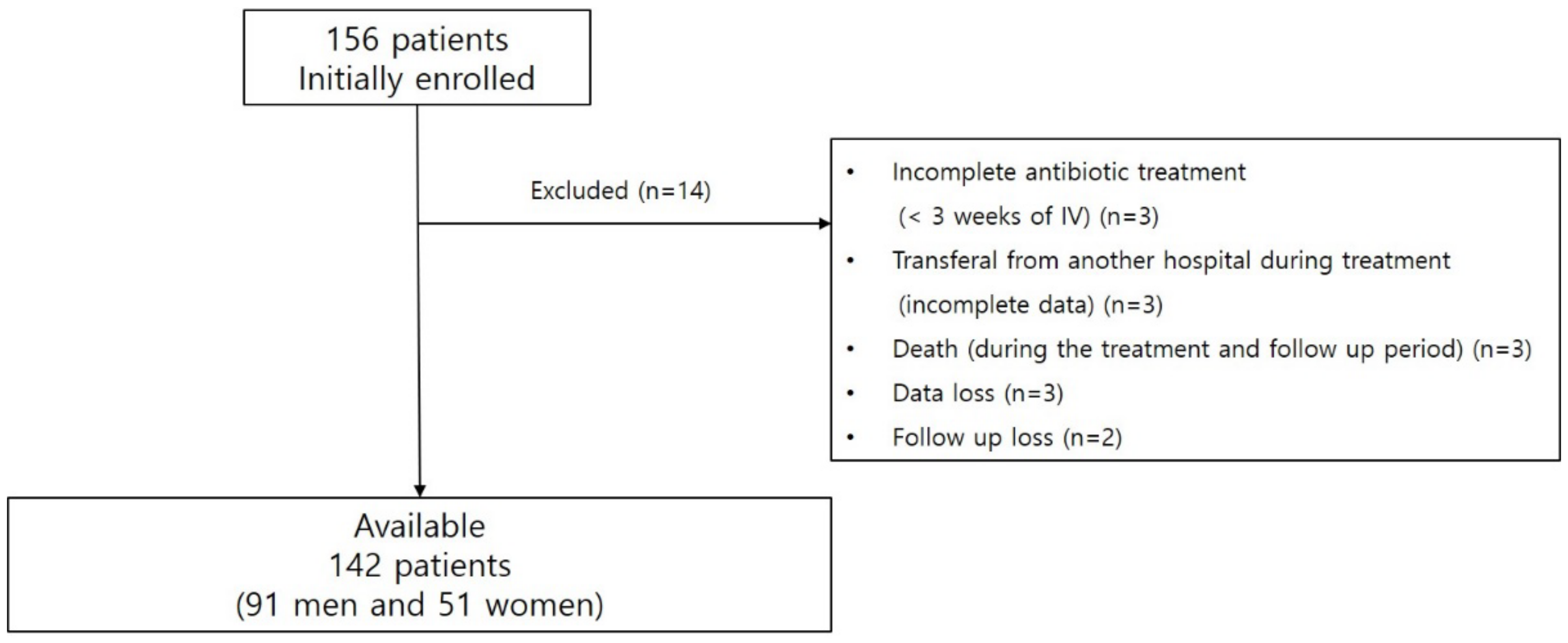
2.1. Patients and Data Collection
2.2. Diagnosis of PSI
2.3. Identification of Causative Bacteria and Treatment
2.4. Cure and Recurrence
2.5. Medical Burden of the Treatment of PSI
2.6. Functional Status Related with PSI
2.7. Statistical Analysis
3. Results
3.1. Clinical and Demographic Data
3.2. Clinical Factors Associated with Medical Burden
3.3. Clinical Factors Associated with Functional Status
3.4. Clinical Factors Associated with Above-Average Medical Burden
3.5. Clinical Factors Associated with Below-Average Functional Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Colmenero, J.D.; Jimenez-Mejias, M.E.; Sanchez-Lora, F.J.; Reguera, J.M.; Palomino-Nicas, J.; Martos, F.; Garcia de las Heras, J.; Pachon, J. Pyogenic, tuberculous, and brucellar vertebral osteomyelitis: A descriptive and comparative study of 219 cases. Ann. Rheum. Dis. 1997, 56, 709–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, Z.; Cheng, Z.; Wang, J.C.; Zhang, W.; Dai, M.; Zhang, B. Spinal Tuberculosis: Always Understand, Often Prevent, Sometime Cure. Neurospine 2021, 18, 648–650. [Google Scholar] [CrossRef]
- Issa, K.; Diebo, B.G.; Faloon, M.; Naziri, Q.; Pourtaheri, S.; Paulino, C.B.; Emami, A. The Epidemiology of Vertebral Osteomyelitis in the United States From 1998 to 2013. Clin. Spine Surg. 2018, 31, E102–E108. [Google Scholar] [CrossRef] [PubMed]
- Adam, D.; Papacocea, T.; Hornea, I.; Croitoru, R. Postoperative spondylodiscitis. A review of 24 consecutive patients. Chirurgia 2014, 109, 90–94. [Google Scholar]
- Butler, J.S.; Shelly, M.J.; Timlin, M.; Powderly, W.G.; O’Byrne, J.M. Nontuberculous pyogenic spinal infection in adults: A 12-year experience from a tertiary referral center. Spine 2006, 31, 2695–2700. [Google Scholar] [CrossRef]
- Friedman, J.A.; Maher, C.O.; Quast, L.M.; McClelland, R.L.; Ebersold, M.J. Spontaneous disc space infections in adults. Surg. Neurol. 2002, 57, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Sobottke, R.; Seifert, H.; Fatkenheuer, G.; Schmidt, M.; Gossmann, A.; Eysel, P. Current diagnosis and treatment of spondylodiscitis. Dtsch. Arztebl. Int. 2008, 105, 181–187. [Google Scholar] [CrossRef]
- Giordan, E.; Marton, E.; Scotton, G.; Canova, G. Outcomes and risk factors for spontaneous spondylodiscitis: Case series and meta-analysis of the literature. J. Clin. Neurosci. 2019, 68, 179–187. [Google Scholar] [CrossRef]
- Chong, B.S.W.; Brereton, C.J.; Gordon, A.; Davis, J.S. Epidemiology, Microbiological Diagnosis, and Clinical Outcomes in Pyogenic Vertebral Osteomyelitis: A 10-year Retrospective Cohort Study. Open Forum Infect. Dis. 2018, 5, ofy037. [Google Scholar] [CrossRef]
- Courjon, J.; Lemaignen, A.; Ghout, I.; Therby, A.; Belmatoug, N.; Dinh, A.; Gras, G.; Bernard, L.; DTS (Duration of Treatment for Spondylodiscitis) Study Group. Pyogenic vertebral osteomyelitis of the elderly: Characteristics and outcomes. PLoS ONE 2017, 12, e0188470. [Google Scholar] [CrossRef]
- Murillo, O.; Grau, I.; Lora-Tamayo, J.; Gomez-Junyent, J.; Ribera, A.; Tubau, F.; Ariza, J.; Pallares, R. The changing epidemiology of bacteraemic osteoarticular infections in the early 21st century. Clin. Microbiol. Infect. 2015, 21, 254.e1–254.e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yagdiran, A.; Otto-Lambertz, C.; Lingscheid, K.M.; Sircar, K.; Samel, C.; Scheyerer, M.J.; Zarghooni, K.; Eysel, P.; Sobottke, R.; Jung, N.; et al. Quality of life and mortality after surgical treatment for vertebral osteomyelitis (VO): A prospective study. Eur. Spine J. 2021, 30, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, T.J.; Berbari, E.F.; Huddleston, P.M.; Steckelberg, J.M.; Osmon, D.R. Do follow-up imaging examinations provide useful prognostic information in patients with spine infection? Clin. Infect. Dis. 2006, 43, 172–179. [Google Scholar] [CrossRef]
- Jeon, I.; Kong, E.; Kim, S.W.; Cho, I.H.; Hong, C.P. Assessment of Therapeutic Response in Pyogenic Vertebral Osteomyelitis Using (18)F-FDG-PET/MRI. Diagnostics 2020, 10, 916. [Google Scholar] [CrossRef]
- Yu, D.; Kim, S.W.; Jeon, I. Antimicrobial therapy and assessing therapeutic response in culture-negative pyogenic vertebral osteomyelitis: A retrospective comparative study with culture-positive pyogenic vertebral osteomyelitis. BMC Infect. Dis. 2020, 20, 939. [Google Scholar] [CrossRef]
- Park, K.H.; Cho, O.H.; Jung, M.; Suk, K.S.; Lee, J.H.; Park, J.S.; Ryu, K.N.; Kim, S.H.; Lee, S.O.; Choi, S.H.; et al. Clinical characteristics and outcomes of hematogenous vertebral osteomyelitis caused by gram-negative bacteria. J. Infect. 2014, 69, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Lora-Tamayo, J.; Euba, G.; Narvaez, J.A.; Murillo, O.; Verdaguer, R.; Sobrino, B.; Narvaez, J.; Nolla, J.M.; Ariza, J. Changing trends in the epidemiology of pyogenic vertebral osteomyelitis: The impact of cases with no microbiologic diagnosis. Semin Arthritis Rheum. 2011, 41, 247–255. [Google Scholar] [CrossRef]
- Russo, A.; Graziano, E.; Carnelutti, A.; Sponza, M.; Cadeo, B.; Sartor, A.; Righi, E.; Bassetti, M. Management of vertebral osteomyelitis over an eight-year period: The UDIPROVE (UDIne PROtocol on VErtebral osteomyelitis). Int. J. Infect. Dis. 2019, 89, 116–121. [Google Scholar] [CrossRef] [Green Version]
- Davidson, M.; Keating, J.L.; Eyres, S. A low back-specific version of the SF-36 Physical Functioning scale. Spine 2004, 29, 586–594. [Google Scholar] [CrossRef]
- Guilfoyle, M.R.; Seeley, H.; Laing, R.J. The Short Form 36 health survey in spine disease—Validation against condition-specific measures. Br. J. Neurosurg. 2009, 23, 401–405. [Google Scholar] [CrossRef]
- Akiyama, T.; Chikuda, H.; Yasunaga, H.; Horiguchi, H.; Fushimi, K.; Saita, K. Incidence and risk factors for mortality of vertebral osteomyelitis: A retrospective analysis using the Japanese diagnosis procedure combination database. BMJ Open 2013, 3, e002412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, W.Y.; Luk, K.D. Pyogenic spondylitis. Int. Orthop. 2012, 36, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chae, H.J.; Kim, J.; Kim, C. Clinical Characteristics of Spinal Epidural Abscess Accompanied by Bacteremia. J. Korean Neurosurg. Soc. 2021, 64, 88–99. [Google Scholar] [CrossRef]
- Park, K.H.; Cho, O.H.; Lee, J.H.; Park, J.S.; Ryu, K.N.; Park, S.Y.; Lee, Y.M.; Chong, Y.P.; Kim, S.H.; Lee, S.O.; et al. Optimal Duration of Antibiotic Therapy in Patients With Hematogenous Vertebral Osteomyelitis at Low Risk and High Risk of Recurrence. Clin. Infect. Dis. 2016, 62, 1262–1269. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.; Jang, S.J.; Lee, H.J.; Ryoo, N.; Kim, M.; Hong, S.G.; Chong, Y.; Korean Nationwide Surveillance of Antimicrobial Resistance Group. Increasing prevalence of vancomycin-resistant Enterococcus faecium, expanded-spectrum cephalosporin-resistant Klebsiella pneumoniae, and imipenem-resistant Pseudomonas aeruginosa in Korea: KONSAR study in 2001. J. Korean Med. Sci. 2004, 19, 8–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.M.; Park, E.S.; Jeong, J.S.; Kim, K.M.; Kim, J.M.; Oh, H.S.; Yoon, S.W.; Chang, H.S.; Chang, K.H.; Lee, S.I.; et al. Multicenter surveillance study for nosocomial infections in major hospitals in Korea. Nosocomial Infection Surveillance Committee of the Korean Society for Nosocomial Infection Control. Am. J. Infect. Control 2000, 28, 454–458. [Google Scholar] [CrossRef]
- Lee, K.; Lim, C.H.; Cho, J.H.; Lee, W.G.; Uh, Y.; Kim, H.J.; Yong, D.; Chong, Y.; Group, K. High prevalence of ceftazidime-resistant Klebsiella pneumoniae and increase of imipenem-resistant Pseudomonas aeruginosa and Acinetobacter spp. in Korea: A KONSAR program in 2004. Yonsei Med. J. 2006, 47, 634–645. [Google Scholar] [CrossRef] [Green Version]
- Pola, E.; Taccari, F.; Autore, G.; Giovannenze, F.; Pambianco, V.; Cauda, R.; Maccauro, G.; Fantoni, M. Multidisciplinary management of pyogenic spondylodiscitis: Epidemiological and clinical features, prognostic factors and long-term outcomes in 207 patients. Eur. Spine J. 2018, 27, 229–236. [Google Scholar] [CrossRef]
- Li, H.K.; Rombach, I.; Zambellas, R.; Walker, A.S.; McNally, M.A.; Atkins, B.L.; Lipsky, B.A.; Hughes, H.C.; Bose, D.; Kumin, M.; et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. N. Engl. J. Med. 2019, 380, 425–436. [Google Scholar] [CrossRef]
- Babouee Flury, B.; Elzi, L.; Kolbe, M.; Frei, R.; Weisser, M.; Scharen, S.; Widmer, A.F.; Battegay, M. Is switching to an oral antibiotic regimen safe after 2 weeks of intravenous treatment for primary bacterial vertebral osteomyelitis? BMC Infect. Dis. 2014, 14, 226. [Google Scholar] [CrossRef] [Green Version]
- McHenry, M.C.; Easley, K.A.; Locker, G.A. Vertebral osteomyelitis: Long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin. Infect. Dis. 2002, 34, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Geisler Crone, C.; Mose Tetens, M.; Bengaard Andersen, A.; Obel, N.; Lebech, A.M. Clinical characteristics of pyogenic vertebral osteomyelitis, and factors associated with inadequate treatment response. Int. J. Infect. Dis. 2021, 108, 487–493. [Google Scholar] [CrossRef]
- Roblot, F.; Besnier, J.M.; Juhel, L.; Vidal, C.; Ragot, S.; Bastides, F.; Le Moal, G.; Godet, C.; Mulleman, D.; Azais, I.; et al. Optimal duration of antibiotic therapy in vertebral osteomyelitis. Semin. Arthritis Rheum. 2007, 36, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Chung, S.K.; Kim, K.J.; Kim, H.J.; Jin, Y.J.; Kim, H.B. Pyogenic vertebral osteomyelitis: Identification of microorganism and laboratory markers used to predict clinical outcome. Eur. Spine J. 2010, 19, 575–582. [Google Scholar] [CrossRef] [Green Version]
- Jean, M.; Irisson, J.O.; Gras, G.; Bouchand, F.; Simo, D.; Duran, C.; Perronne, C.; Mulleman, D.; Bernard, L.; Dinh, A. Diagnostic delay of pyogenic vertebral osteomyelitis and its associated factors. Scand. J. Rheumatol. 2017, 46, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Jeon, I.; Kong, E.; Kim, S.W. Simultaneous 18F-FDG PET/MRI in tuberculous spondylitis: An independent method for assessing therapeutic response—Case series. BMC Infect. Dis. 2019, 19, 845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.S.; Kim, T.H. Recurrence Rates and Its Associated Factors after Early Spinal Instrumentation for Pyogenic Spondylodiscitis: A Nationwide Cohort Study of 2148 Patients. J. Clin. Med. 2022, 11, 3356. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kim, J.G.; Yi, J.; Choi, J.M.; Chung, C.K.; Choi, U.Y.; Han, I.B.; Sohn, S. Changes in the medical burden of pyogenic and tuberculous spondylitis between 2007 and 2016: A nationwide cohort study. J. Clin. Neurosci. 2020, 73, 89–93. [Google Scholar] [CrossRef]
- McGrath, J.M.; Schaefer, M.P.; Malkamaki, D.M. Incidence and characteristics of complications from epidural steroid injections. Pain Med. 2011, 12, 726–731. [Google Scholar] [CrossRef] [Green Version]
- Pountos, I.; Panteli, M.; Walters, G.; Bush, D.; Giannoudis, P.V. Safety of Epidural Corticosteroid Injections. Drugs R D 2016, 16, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Hooten, W.M.; Mizerak, A.; Carns, P.E.; Huntoon, M.A. Discitis after lumbar epidural corticosteroid injection: A case report and analysis of the case report literature. Pain Med. 2006, 7, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Factors | Values (%) |
|---|---|
| Age, years | 66.51 ± 11.76 (41–90) |
| Sex, male:female | 91:51 |
| Underlying diseases | |
| Diabetes mellitus | 40 (28.2) |
| Rheumatic disease | 7 (4.9) |
| Liver disease | 3 (2.1) |
| Chronic kidney disease | 3 (2.1) |
| Procedure-related (non-surgical) | 87 (61.3) |
| Epidural injection | 66 (75.9) |
| Acupuncture | 13 (14.9) |
| Epidural injection & acupuncture | 8 (9.2) |
| Clinical symptoms | |
| Fever, ≥37.3 °C | 26 (18.3) |
| Back pain | 140 (98.6) |
| Leg radiculopathy | 71 (50.0) |
| Leg weakness | 50 (35.2) |
| Bowel and bladder symptoms | 4 (2.8) |
| CCI | 3.07 ± 1.77 (0–9) |
| Features of MR imaging | |
| Extent of lesion, levels | 3.38 ± 1.69 (1–11) |
| Epidural abscess | 94 (66.2) |
| Paraspinal abscess | 110 (77.5) |
| Psoas abscess | 49 (34.5) |
| Discitis | 107 (75.4) |
| Back muscle abscess | 48 (33.8) |
| Initial blood inflammatory markers | |
| WBC, count | 10,625 ± 4921 (3750–28,790) |
| ESR, mm/h | 71.23 ± 31.37 (2–120) |
| CRP, mg/dL | 9.57 ± 9.71 (0.03–38.00) |
| Last blood inflammatory markers (at completion of antibiotic therapy) | |
| WBC, count | 5989 ± 1.98 (2340–15,020) |
| ESR, mm/h | 41.17 ± 26.63 (2–120) |
| CRP, mg/dL | 0.81 ± 1.46 (0.02–13.36) |
| Duration of parenteral antibiotics, days | 44.73 ± 18.00 (21–140) |
| Additional surgical treatment | 60 (42.3) |
| Length of hospitalization, days | 55.56 ± 27.09 (7–172) |
| Cost of hospitalization, $ | 14,070.17 ± 9289.39 (1611.87–48,722.35) |
| Initial SF-36 (at diagnosis) | 34.20 ± 12.89 (3–57) |
| 6-month SF-36 (after completion of antibiotic therapy) | 49.12 ± 8.76 (26–60) |
| Follow up period (after completion of antibiotic therapy), months | 18.13 ± 14.99 |
| Recurrence | 11 (7.7) |
| Causative Pathogens | Values (%) |
|---|---|
| Culture-positive | 62 (43.7) |
| Gram-positive bacteria | |
| Staphylococcus aureus | 31 (21.8) |
| Methicillin-sensitive | 19 |
| Methicillin-resistant | 12 |
| Coagulase-negative staphylococci | 4 (2.8) |
| Streptococcus species | 9 (6.3) |
| Enterococcus species | 4 (2.8) |
| Gram-negative bacteria | |
| Acinetobacter | 3 (2.1) |
| Achrombacter | 1 (0.7) |
| Enterobacter | 1 (0.7) |
| Klebsiella | 4 (2.8) |
| Escherichia coli | 4 (2.8) |
| Pseudomonas | 1 (0.7) |
| Culture-negative | 80 (56.3) |
| Factors | Length of Hospitalization (Days) | Cost of Hospitalization ($) | ||
|---|---|---|---|---|
| Values | p | Values | p | |
| Age, years | r = 0.014 | 0.869 | r = 0.021 | 0.805 |
| Sex | ||||
| Male | 53.67 ± 27.54 | 0.267 | 12,926.69 ± 8324.47 | 0.068 |
| Female | 58.94 ± 26.18 | 16,110.50 ± 10,582.32 | ||
| Procedure−related | ||||
| (−) | 53.71 ± 25.48 | 0.519 | 14,543.60 ± 9631.17 | 0.631 |
| (+) | 56.74 ± 28.14 | 13,770.87 ± 9110.53 | ||
| Clinical symptoms | ||||
| Fever, >37.3 °C | ||||
| (−) | 54.77 ± 27.70 | 0.461 | 13,302.40 ± 9021.03 | 0.037 |
| (+) | 59.12 ± 24.34 | 17,495.58 ± 9869.66 | ||
| Back pain | ||||
| (−) | 30.00 ± 5.66 | 0.180 | 5306.99 ± 370.78 | 0.180 |
| (+) | 55.93 ± 27.10 | 14,195.36 ± 9295.84 | ||
| Leg radiculopathy | ||||
| (−) | 53.49 ± 26.15 | 0.365 | 12,737.38 ± 8208.99 | 0.087 |
| (+) | 57.63 ± 28.02 | 10,140.39 ± 1203.44 | ||
| Leg weakness | ||||
| (−) | 50.30 ± 24.63 | 0.001 * | 11,886.06 ± 7774.35 | 0.000 * |
| (+) | 65.24 ± 28.94 | 18,088.94 ± 10,518.01 | ||
| Bowel and bladder symptoms | ||||
| (−) | 55.38 ± 27.17 | 0.631 | 14,012.61 ± 9288.03 | 0.666 |
| (+) | 62.00 ± 26.57 | 16,055.98 ± 10,526.08 | ||
| Initial blood inflammatory markers | ||||
| WBC, count | r = 0.223 | 0.008 * | r = 0.358 | 0.000 * |
| ESR, mm/h | r = 0.172 | 0.040 * | r = 0.224 | 0.007 * |
| CRP, mg/dL | r = 0.300 | 0.000 * | r = 0.440 | 0.000 * |
| CCI | r = 0.080 | 0.344 | r = −0.002 | 0.982 |
| Identification of causative bacteria | ||||
| (−) | 51.01 ± 22.86 | 0.028 * | 11,563.03 ± 6371.57 | 0.001 * |
| (+) | 61.44 ± 30.93 | 17,305.18 ± 11,314.02 | ||
| Bacteremia | ||||
| (−) | 52.02 ± 25.78 | 0.003 * | 12,410.88 ± 7909.22 | 0.001 * |
| (+) | 67.75 ± 28.31 | 19,773.99 ± 11,366.02 | ||
| Additional surgical treatment | ||||
| (−) | 46.40 ± 18.58 | 0.000 * | 10,5333.59 ± 6647.80 | 0.000 * |
| (+) | 68.08 ± 31.68 | 18,903.50 ± 10,218.26 | ||
| Recurrence | ||||
| (−) | 52.02 ± 22.42 | 0.004 * | 13,093.90 ± 8370.68 | 0.006 * |
| (+) | 97.82 ± 41.02 | 25,696.66 ± 12,027.55 | ||
| Features of MR imaging at diagnosis | ||||
| Extent of lesion, levels | r = 0.275 | 0.001 * | r = 0.406 | 0.000 * |
| Epidural abscess | ||||
| (−) | 44.48 ± 22.00 | 0.000 * | 9175.41 ± 5855.07 | 0.000 * |
| (+) | 61.22 ± 27.79 | 16,569.62 ± 9737.84 | ||
| Paraspinal abscess | ||||
| (−) | 51.34 ± 26.09 | 0.318 | 11,576.66 ± 6252.27 | 0.030 * |
| (+) | 56.79 ± 27.36 | 14,795.56 ± 9907.19 | ||
| Psoas abscess | ||||
| (−) | 53.97 ± 27.13 | 0.335 | 13,010.61 ± 8335.86 | 0.061 |
| (+) | 58.59 ± 27.03 | 16,081.18 ± 10,677.02 | ||
| Discitis | ||||
| (−) | 52.63 ± 22.17 | 0.462 | 13,523.31 ± 10,236.22 | 0.690 |
| (+) | 56.52 ± 28.54 | 14,249.05 ± 9002.55 | ||
| Back muscle abscess | ||||
| (−) | 50.95 ± 23.55 | 0.009 * | 12,554.67 ± 8229.47 | 0.012 * |
| (+) | 64.60 ± 31.27 | 17,038.03 ± 10,549.01 | ||
| Length of hospitalization, days | - | - | r = 0.790 | 0.000 * |
| Cost of hospitalization, $ | r = 0.790 | 0.000 * | - | - |
| Factors | Initial SF-36 | 6-Month SF-36 | ||
|---|---|---|---|---|
| Values | p | Values | p | |
| Age, years | r = −0.184 | 0.028 * | r = −0.219 | 0.009 * |
| Sex | ||||
| Male | 36.02 ± 12.17 | 0.024 * | 50.18 ± 8.18 | 0.055 |
| Female | 30.94 ± 13.60 | 47.24 ± 9.50 | ||
| Procedure−related | ||||
| (−) | 31.65 ± 14.68 | 0.078 | 47.33 ± 9.29 | 0.052 |
| (+) | 35.80 ± 11.41 | 50.25 ± 8.27 | ||
| Clinical symptoms | ||||
| Fever, >37.3 °C | ||||
| (−) | 34.63 ± 12.74 | 0.401 | 49.44 ± 8.18 | 0.453 |
| (+) | 32.27 ± 13.64 | 47.69 ± 11.06 | ||
| Back pain | ||||
| (−) | 38.50 ± 7.78 | 0.636 | 54.50 ± 6.36 | 0.384 |
| (+) | 34.14 ± 12.95 | 49.04 ± 8.78 | ||
| Leg radiculopathy | ||||
| (−) | 37.17 ± 11.26 | 0.006 * | 51.25 ± 6.84 | 0.003 * |
| (+) | 31.23 ± 13.78 | 46.99 ± 9.93 | ||
| Leg weakness | ||||
| (−) | 40.70 ± 7.93 | 0.000 * | 52.71 ± 5.54 | 0.000 * |
| (+) | 22.24 ± 11.66 | 42.52 ± 9.76 | ||
| Bowel and bladder symptoms | ||||
| (−) | 34.67 ± 12.64 | 0.010 * | 49.32 ± 8.57 | 0.112 |
| (+) | 18.00 ± 12.25 | 42.25 ± 13.77 | ||
| Initial blood inflammatory markers | ||||
| WBC, count | r = −0.273 | 0.001 * | r = −0.253 | 0.002 * |
| ESR, mm/h | r = −0.076 | 0.369 | r = −0.132 | 0.118 |
| CRP, mg/dL | r = −0.313 | 0.000 * | r = −0.240 | 0.004 * |
| CCI | r = −0.207 | 0.013 * | r = −0.204 | 0.004 * |
| Identification of causative bacteria | ||||
| (−) | 37.83 ± 10.68 | 0.000 * | 51.38 ± 6.10 | 0.001 * |
| (+) | 29.52 ± 14.03 | 46.21 ± 10.67 | ||
| Bacteremia | ||||
| (−) | 36.67 ± 11.32 | 0.000 * | 50.21 ± 7.26 | 0.037 * |
| (+) | 25.69 ± 14.49 | 45.38 ± 12.04 | ||
| Additional surgical treatment | ||||
| (−) | 35.70 ± 12.62 | 0.106 | 49.70 ± 8.18 | 0.362 |
| (+) | 32.15 ± 13.08 | 48.33 ± 9.51 | ||
| Recurrence | ||||
| (−) | 34.37 ± 12.95 | 0.574 | 49.31 ± 8.74 | 0.385 |
| (+) | 32.09 ± 12.48 | 46.91 ± 9.15 | ||
| Features of MR imaging at diagnosis | ||||
| Extent of lesion, levels | r = −0.191 | 0.023 * | r = −0.168 | 0.046 * |
| Epidural abscess | ||||
| (−) | 38.71 ± 8.56 | 0.000 * | 52.10 ± 4.66 | 0.000 * |
| (+) | 31.89 ± 14.11 | 47.60 ± 9.92 | ||
| Paraspinal abscess | ||||
| (−) | 36.53 ± 9.92 | 0.172 | 51.13 ± 6.27 | 0.072 |
| (+) | 33.52 ± 13.60 | 48.54 ± 9.30 | ||
| Psoas abscess | ||||
| (−) | 36.78 ± 10.96 | 0.003 * | 51.59 ± 6.47 | 0.000 * |
| (+) | 29.29 ± 14.84 | 44.43 ± 10.53 | ||
| Discitis | ||||
| (−) | 35.43 ± 12.30 | 0.517 | 51.17 ± 8.09 | 0.111 |
| (+) | 33.79 ± 13.11 | 48.45 ± 8.90 | ||
| Back muscle abscess | ||||
| (−) | 36.04 ± 12.91 | 0.016 * | 50.50 ± 8.05 | 0.013 * |
| (+) | 30.58 ± 12.18 | 46.42 ± 9.53 | ||
| Length of hospitalization, days | r = −0.241 | 0.004 * | r = −0.241 | 0.004 * |
| Cost of hospitalization, $ | r = −0.343 | 0.000 * | r = −0.321 | 0.000 * |
| Length of Hospitalization (Days) | Cost of Hospitalization ($) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | Univariable Analysis | Multivariable Analysis | Univariable Analysis | Multivariable Analysis | ||||||||
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Age, years | 0.993 | 0.965–1.022 | 0.633 | 1.013 | 0.984–1.044 | 0.384 | ||||||
| Sex (female) | 1.807 | 0.895–3.648 | 0.099 | 2.279 | 1.121–4.635 | 0.023 * | 4.438 | 1.524–2.920 | 0.006 * | |||
| Procedure-related | 1.451 | 0.716–2.941 | 0.302 | 2.702 | 1.072–6.810 | 0.035 * | 0.896 | 0.446–1.803 | 0.759 | |||
| Fever, >37.3 °C | 1.829 | 0.776–4.314 | 0.168 | 2.395 | 1.010–5.676 | 0.047 * | ||||||
| Leg radiculopathy | 1.828 | 0.920–3.632 | 0.085 | 1.630 | 0.818–3.246 | 0.165 | ||||||
| Leg weakness | 2.826 | 1.383–5.775 | 0.004 * | 2.750 | 1.343–.5.631 | 0.006 * | ||||||
| WBC | 1.101 | 1.024–1.184 | 0.009 * | 1.110 | 1.032–1.194 | 0.005 * | ||||||
| ESR, mm/h | 1.011 | 1.000–1.022 | 0.061 | 1.008 | 0.997–1.020 | 0.141 | ||||||
| CRP, mg/dL | 1.072 | 1.031–1.113 | <0.001 * | 1.062 | 1.010–1.118 | 0.019 * | 1.075 | 1.035–1.118 | <0.001 * | 1.071 | 1.010–1.135 | 0.022 * |
| CCI | 1.012 | 0.835–1.226 | 0.906 | 1.064 | 0.877–1.291 | 0.531 | ||||||
| Identification of causative bacteria | 2.187 | 1.097–4.363 | 0.026 * | 3.200 | 1.573–6.509 | 0.001 * | ||||||
| Bacteremia | 4.455 | 1.931–10.274 | <0.001 * | 4.966 | 1.706–14.453 | 0.003 * | 4.865 | 2.101–11.263 | <0.001 * | 4.647 | 1.411–15.299 | 0.012 * |
| Additional surgical treatment | 5.333 | 2.557–11.122 | <0.001 * | 6.524 | 2.570–16.562 | <0.001 * | 5.353 | 2.552–11.226 | <0.001 * | 6.737 | 2.276–19.942 | <0.001 * |
| Recurrence | 8.600 | 1.782–41.504 | 0.007 * | 12.453 | 2.139–72.509 | 0.005 * | 9.209 | 1.906–44.487 | 0.006 * | 22.543 | 3.682–138.013 | <0.001 * |
| Extent of lesion, levels | 1.590 | 1.242–2.035 | <0.001 * | 1.665 | 1.291–2.147 | <0.001 * | 1.431 | 1.010–2.028 | 0.044 * | |||
| Epidural abscess | 4.792 | 2.027–11.325 | <0.001 * | 4.400 | 1.861–10.402 | <0.001 * | ||||||
| Paraspinal abscess | 1.769 | 0.749–4.178 | 0.193 | 5.965 | 1.701–20.923 | 0.005 * | 2.000 | 0.824–4.853 | 0.125 | |||
| Psoas abscess | 1.553 | 0.766–3.150 | 0.222 | 2.229 | 1.091–4.552 | 0.028 * | ||||||
| Discitis | 1.051 | 0.478–2.313 | 0.901 | 1.144 | 0.514–2.547 | 0.741 | ||||||
| Back muscle abscess | 2.436 | 1.191–4.984 | 0.015 * | 1.805 | 0.884–3.688 | 0.105 | ||||||
| Initial SF-36 | 6-month SF-36 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Factors | Univariable Analysis | Multivariable Analysis | Univariable Analysis | Multivariable Analysis | ||||||||
| OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p | |
| Age, years | 1.025 | 0.995–1.055 | 0.099 | 1.023 | 0.993–1.053 | 0.135 | ||||||
| Sex (female) | 1.977 | 0.985–3.967 | 0.055 | 2.287 | 1.133–4.618 | 0.021 * | ||||||
| Procedure-related | 0.561 | 0.283–1.113 | 0.098 | 0.546 | 0.274–1.087 | 0.085 | ||||||
| Fever, >37.3 °C | 1.214 | 0.516–2.855 | 0.656 | 1.352 | 0.574–3.185 | 0.490 | ||||||
| Leg radiculopathy | 2.902 | 1.453–5.795 | 0.003 * | 3.152 | 1.561–6.362 | 0.001 * | ||||||
| Leg weakness | 17.503 | 7.256–42.220 | <0.001 * | 15.966 | 5.967–42.724 | <0.001 * | 6.375 | 2.985–13.615 | <0.001 * | 7.975 | 3.307–19.232 | <0.001 * |
| WBC | 1.159 | 1.068–1.257 | <0.001 * | 1.116 | 1.007–1.237 | 0.036 * | 1.093 | 1.017–1.174 | 0.015 * | 1.094 | 1.006–1.190 | 0.035 * |
| ESR, mm/h | 1.002 | 0.992–1.013 | 0.668 | 1.007 | 0.996–1.018 | 0.202 | ||||||
| CRP, mg/dL | 1.060 | 1.021–1.100 | 0.002 * | 1.040 | 1.004–1.077 | 0.029 * | ||||||
| CCI | 1.283 | 1.049–1.569 | 0.015 * | 1.485 | 1.130–1.952 | 0.005 * | 1.142 | 0.942–1.385 | 0.177 | |||
| Identification of causative bacteria | 4.764 | 2.327–9.754 | <0.001 * | 2.913 | 1.087–7.803 | 0.033 * | 2.077 | 1.049–4.113 | 0.036 * | |||
| Bacteremia | 5.042 | 2.120–11.989 | <0.001 * | 1.429 | 0.646–3.159 | 0.378 | ||||||
| Additional surgical treatment# | - | – | – | 1.418 | 0.719–2.796 | 0.313 | ||||||
| Recurrence # | - | – | – | 2.835 | 0.790–10.177 | 0.110 | ||||||
| Extent of lesion, levels | 1.356 | 1.087–1.692 | 0.007 * | 1.111 | 0.911–1.355 | 0.299 | ||||||
| Epidural abscess | 2.692 | 1.267–5.723 | 0.010 * | 2.755 | 1.278–5.941 | 0.010 * | ||||||
| Paraspinal abscess | 1.290 | 0.575–2.897 | 0.537 | 1.154 | 0.513–2.595 | 0.729 | ||||||
| Psoas abscess | 1.962 | 0.972–3.958 | 0.060 | 2.577 | 1.265–5.249 | 0.009 * | ||||||
| Discitis | 1.131 | 0.520–2.460 | 0.756 | 1.391 | 0.627–3.085 | 0.417 | ||||||
| Back muscle abscess | 2.377 | 1.168–4.836 | 0.017 * | 2.106 | 1.036–4.279 | 0.040 * | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, S.; Yu, D.; Bae, S.W.; Kim, S.W.; Jeon, I. Analysis of Clinical Factors Associated with Medical Burden and Functional Status in Pyogenic Spine Infection. J. Clin. Med. 2023, 12, 2551. https://doi.org/10.3390/jcm12072551
Jeon S, Yu D, Bae SW, Kim SW, Jeon I. Analysis of Clinical Factors Associated with Medical Burden and Functional Status in Pyogenic Spine Infection. Journal of Clinical Medicine. 2023; 12(7):2551. https://doi.org/10.3390/jcm12072551
Chicago/Turabian StyleJeon, Seongmin, Dongwoo Yu, Sang Woon Bae, Sang Woo Kim, and Ikchan Jeon. 2023. "Analysis of Clinical Factors Associated with Medical Burden and Functional Status in Pyogenic Spine Infection" Journal of Clinical Medicine 12, no. 7: 2551. https://doi.org/10.3390/jcm12072551
APA StyleJeon, S., Yu, D., Bae, S. W., Kim, S. W., & Jeon, I. (2023). Analysis of Clinical Factors Associated with Medical Burden and Functional Status in Pyogenic Spine Infection. Journal of Clinical Medicine, 12(7), 2551. https://doi.org/10.3390/jcm12072551