
Prevalence of Possible Dementia in Patients with Maxillofacial Defects and Difficulty of Inserting Obturator in Maxillectomy Patients: Toward Better Provision of Supportive Care


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Part I: Survey on the Prevalence of Possible Dementia
2.3. Part II: Difficulty Inserting a Maxillary Obturator Prosthesis after Maxillectomy
2.3.1. Questionnaire
2.3.2. Basic Information on Intraoral Condition and Maxillary Obturator Prostheses
2.3.3. HDS-R
2.3.4. PPT
2.3.5. Maxillary Obturator Prosthesis Insertion Time
2.3.6. Grip Strength Test
2.3.7. Understanding of the Intraoral Surgical Site
2.4. Statistical Analysis
2.4.1. Part I: Prevalence of Possible Dementia
2.4.2. Part II: Difficulty Inserting the Maxillary Obturator Prosthesis after Maxillectomy
3. Results
3.1. Part I: Prevalence of Possible Dementia
3.2. Part II: Difficulty Inserting a Maxillary Obturator Prosthesis after Maxillectomy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Phasuk, K.; Haug, S.P. Maxillofacial prosthetics. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Rosen, E.B.; Palin, C.L.; Huryn, J.M.; Wong, R.J. The role of maxillofacial prosthetics for the surgically treated patient at National Cancer Institute-designated comprehensive cancer centers. Laryngoscope 2019, 129, 409–414. [Google Scholar] [CrossRef]
- Sumita, Y.I.; Hattori, M.; Namba, T.; Ino, S. Obturators to facilitate speech and swallowing in a maxillectomy patient with dementia and cerebral infarction. Int. J. Maxillofac. Prosthet. 2019, 2, 33–35. [Google Scholar] [CrossRef]
- Yanagi, A.; Sumita, Y.; Hattori, M.; Kamiyanagi, A.; Otomaru, T.; Kanazaki, A.; Haraguchi, M.; Murase, M.; Hatano, N.; Taniguchi, H. Clinical survey over the past 35 years at the clinic for maxillofacial prosthetics Tokyo Medical and Dental University. J. Prosthodont. Res. 2018, 62, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Jaul, E.; Barron, J. Age-related diseases and clinical and public health implications for the 85 years old and over population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, K. Survival rate of patients with dementia. Jpn. J. Insur. Med. 2018, 116, 196–200, (Abstract in English). [Google Scholar]
- Perneczky, R.; Wagenpfeil, S.; Komossa, K.; Grimmer, T.; Diehl, J.; Kurz, A. Mapping scores onto stages: Mini-Mental State Examination and Clinical Dementia Rating. Am. J. Geriatr. Psychiatry 2006, 14, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Galasko, D.; Klauber, M.R.; Hofstetter, C.R.; Salmon, D.P.; Lasker, B.; Thal, L.J. The Mini-Mental State Examination in the early diagnosis of Alzheimer’s disease. Arch. Neurol. 1990, 47, 49–52. [Google Scholar] [CrossRef]
- Hodges, J.R.; Salmon, D.P.; Butters, N. Differential impairment of semantic and episodic memory in Alzheimer’s and Huntington’s disease: A controlled prospective study. J. Neurol. Neurosurg. Psychiatry 1990, 53, 1089–1095. [Google Scholar] [CrossRef] [Green Version]
- Fujiwara, Y.; Suzuki, H.; Yasunaga, M.; Sugiyama, M.; Ijuin, M.; Sakuma, N.; Inagaki, H.; Iwasa, H.; Ura, C.; Yatomi, N.; et al. Brief screening tool for mild cognitive impairment in older Japanese: Validation of the Japanese version of the Montreal Cognitive Assessment. Geriatr. Gerontol. Int. 2010, 10, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Bruno, D.; Schurmann Vignaga, S. Addenbrooke’s cognitive examination III in the diagnosis of dementia: A critical review. Neuropsychiatr. Dis. Treat. 2019, 15, 441–447. [Google Scholar] [CrossRef] [Green Version]
- Imai, Y.; Hasegawa, K. The Revised Hasegawa’s Dementia Scale (HDS-R) evaluation of its usefulness as a screening test for dementia. Hong Kong J. Psychiatry 1994, 4, 20–24. [Google Scholar]
- Jeong, J.W.; Kim, K.W.; Lee, D.Y.; Lee, S.B.; Park, J.H.; Choi, E.A.; Choe, J.Y.; Do, Y.J.; Ryang, J.S.; Roh, H.A.; et al. A normative study of the Revised Hasegawa Dementia Scale: Comparison of demographic influences between the Revised Hasegawa Dementia Scale and the Mini-Mental Status Examination. Dement. Geriatr. Cogn. Disord. 2007, 24, 288–293. [Google Scholar] [CrossRef]
- Takiura, T. Dementia screening scales in Japan. Bull. Hiroshima Shudo Univ. Stud. Humanit. 2007, 48, 347–379, (Abstract in English). [Google Scholar]
- Copeland, J.R.; McCracken, C.F.; Dewey, M.E.; Wilson, K.C.; Doran, M.; Gilmore, C.; Scott, A.; Larkin, B.A. Undifferentiated dementia, Alzheimer’s disease, and vascular dementia: Age- and gender-related incidence in Liverpool. The MRC–ALPHA Study. Br. J. Psychiatry 1999, 175, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Mazure, C.M.; Swendsen, J. Sex differences in Alzheimer’s disease and other dementias. Lancet Neurol. 2016, 15, 451–452. [Google Scholar] [CrossRef] [Green Version]
- Furuna, T.; Nagasaki, H.; Nishizawa, S.; Sugiura, M.; Okuzumi, H.; Ito, H.; Kinugasa, T.; Hashizume, K.; Maruyama, H. Longitudinal change in the physical performance of older adults in the community. J. Jpn. Phys. Ther. Assoc. 1998, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Kounnavong, S.; Ratsavong, K.; Soundavong, K.; Xayavong, S.; Kariya, T.; Saw, Y.M.; Yamamoto, E.; Horibe, K.; Toba, K.; Hamajima, N. Cognitive function measured with the Revised Hasegawa’s Dementia Scale among elderly individuals in Lao PDR. Nagoya J. Med. Sci. 2019, 81, 281–290. [Google Scholar] [PubMed]
- Irie, K.; Iseki, H.; Okamoto, K.; Nishimura, S.; Kagechika, K. Introduction of the Purdue Pegboard Test for fine assessment of severity of cervical myelopathy before and after surgery. J. Phys. Ther. Sci. 2020, 32, 210–214. [Google Scholar] [CrossRef] [Green Version]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Alqutaibi, A.Y. Enhancing retention of maxillary obturators using dental implants. Int. J. Contemp. Dent. Med. Rev. 2015, 2, 010915. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Item No. | Questions | Score | |
|---|---|---|---|
| 1 | Age (1 point if correct within ±2 years) | 0, 1 | |
| 2 | Year, month, date, day (1 point each) | Year Month Date Day | 0, 1 0, 1 0, 1 0, 1 |
| 3 | Current location (2 points for a correct answer given within 5 s; 1 point for correct choice between hospital and office) | 0, 1, 2 | |
| 4 | Repeating 3 words (1 point each; use only one version per test) 1 (a) cherry blossom, (b) cat, (c) train; 2 (a) plum blossom, (b) dog, (c) car | 0, 1 0, 1 0, 1 | |
| 5 | 100 − 7 = ? (1 point for the correct answer; if not correct, skip to item 6) −7 again = ? (1 point for a correct answer) | (93) (86) | 0, 1 0, 1 |
| 6 | Repeating 6-8-2 backward (Skip to item 7 if not correct answer) Repeating 3-5-2-9 backward | 2-8-6 9-2-5-3 | 0, 1 0, 1 |
| 7 | Recalling 3 words from item 4. (2 points for spontaneous recall; 1 point for a correct recall after category cue) (a) plant, (b) animal, (c) transportation | a: 0, 1, 2 b: 0, 1, 2 c: 0, 1, 2 | |
| 8 | Recalling 5 unrelated common objects after they are shown and then covered (Scissors, mirror, battery, pen, coin, etc.) | 0, 1, 2 3, 4, 5 | |
| 9 | Naming all vegetables that come to mind (Stop after a 10 s interval with no response) 0–5 = 0 points, 6 = 1 point, 7 = 2 points, 8 = 3 points, 9 = 4 points, 10 = 5 points | 0, 1, 2 3, 4, 5 | |
| Total score | |||
| Age Group (Years) | HDS-R Score | Adjusted p-Value | |
|---|---|---|---|
| 0–20 # | 21–30 | ||
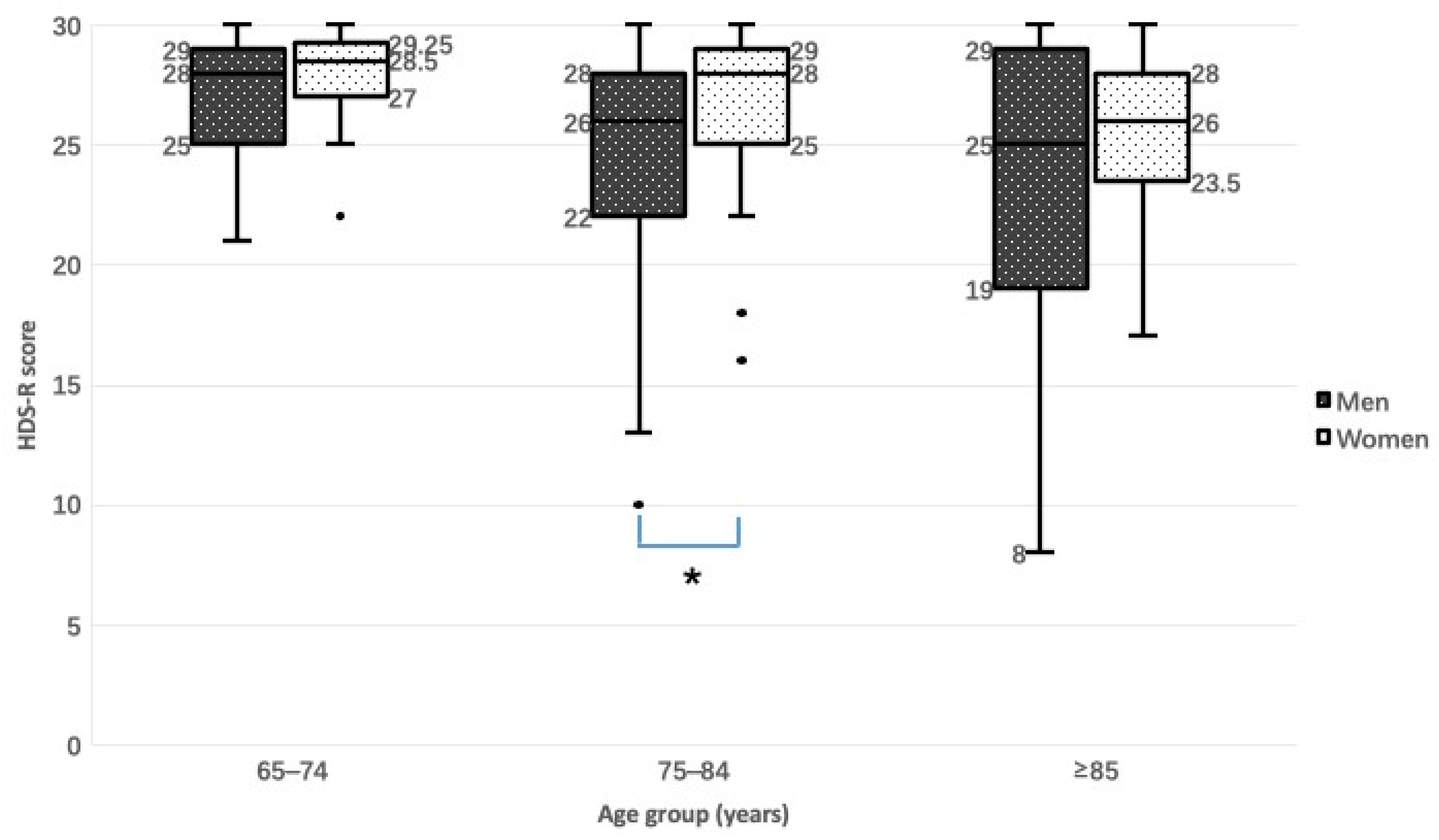
| 65–74 | 0 | 71 | 65–74 vs. 75–84: 0.010 * |
| 75–84 | 9 | 71 | 65–74 vs. ≥85: 0.001 * |
| ≥85 | 7 | 25 | 75–84 vs. ≥85: 0.690 |
| Total | 16 | 167 | |
| Question | Score | Male, n (%) | Female, n (%) | Total, n (%) | p-Value |
|---|---|---|---|---|---|
| 1 (Age) | 0 | 2 (2) | 0 (0) | 2 (1.1) | 0.502 |
| 1 | 98 (98) | 83 (100) | 181 (98.9) | ||
| 2 (Date) | 0–3 | 13 (13) | 11 (13.3) | 24 (13.1) | 1 |
| 4 | 87 (87) | 72 (86.7) | 159 (86.9) | ||
| 3 (Place) | 0–1 | 2 (2) | 0 (0) | 2 (1.1) | 0.502 |
| 2 | 98 (98) | 83 (100) | 181 (98.9) | ||
| 4 (Repetition) | 0–2 | 1 (1) | 0 (0) | 1 (0.5) | 1 |
| 3 | 99 (99) | 83 (100) | 182 (99.5) | ||
| 5 (Subtraction) | 0–1 | 15 (15) | 17 (20.5) | 32 (17.5) | 0.337 |
| 2 | 85 (85) | 66 (79.5) | 151 (82.5) | ||
| 6 (Backward repetition) | 0–1 | 23 (23) | 32 (38.6) | 55 (30.1) | 0.024 * |
| 2 | 77 (77) | 51 (61.4) | 128 (69.9) | ||
| 7 (Recall) | 0–5 | 66 (66) | 41 (49.4) | 107 (58.5) | 0.025 * |
| 6 | 34 (34) | 42 (50.6) | 76 (41.5) | ||
| 8 (Naming objects) | 0–4 | 44 (44) | 28 (33.7) | 72 (39.3) | 0.174 |
| 5 | 56 (56) | 55 (66.3) | 111 (60.7) | ||
| 9 (Naming vegetables) | 0 | 14 (14) | 0 (0) | 14 (7.7) | <0.001 ** |
| 1–2 | 17 (17) | 5 (6) | 22 (12) | ||
| 3–4 | 9 (9) | 13 (15.7) | 22 (12) | ||
| 5 | 60 (60) | 65 (78.3) | 125 (68.3) | ||
| Total score | 0–10 | 3 (3) | 0 (0) | 3 (1.6) | 0.178 |
| 11–20 | 9 (9) | 4 (4.8) | 13 (7.1) | ||
| 21–30 | 88 (88) | 79 (95.2) | 167 (91.3) |
| Subjective Comments | (N = 47) |
|---|---|
| Visual analogue scale score | n (%) |
| <50 | 1 (2) |
| ≥50, <70 | 4 (9) |
| ≥70, <90 | 11 (23) |
| ≥90, <100 | 31 (66) |
| Problems with inserting a maxillary obturator prosthesis | n (%) |
| No | 21 (45) |
| Yes | 26 (55) |
| Reasons for problems | |
| Defect | 12 (26) |
| Hand coordination | 4 (9) |
| Mouth opening | 5 (10) |
| Other | 5 (10) |
| Advice for inserting a maxillary obturator prosthesis | n (%) |
| Follow doctor’s instructions and become accustomed to it | 14 (30) |
| Use tongue to help | 1 (2) |
| No advice provided | 32 (68) |
| Characteristics | (N = 47) |
|---|---|
| Age (years), (mean ± SD) | 74 ± 8 |
| Sex, n | |
| Men | 23 |
| Women | 24 |
| Duration of wearing dentures before maxillectomy (year), median (range, IQR) | 0 (0–40, 7) |
| Communication between the oral cavity and nasal cavity, n | |
| Yes | 31 |
| No | 16 |
| Number of remaining teeth, median (range, IQR) | 3 (0–10, 6) |
| Mouth opening (mm), median (range, IQR) | 42 (11–70, 14) |
| Prosthesis material, n | |
| Resin base denture | 43 |
| Metal flame denture | 4 |
| Prosthesis weight (g) (mean ± SD) | 25.8 ± 10.4 |
| Obturator height (mm) (mean ± SD) | 24.4 ± 11.2 |
| Number of clasps, median (range, IQR) | 2 (0–6, 3) |
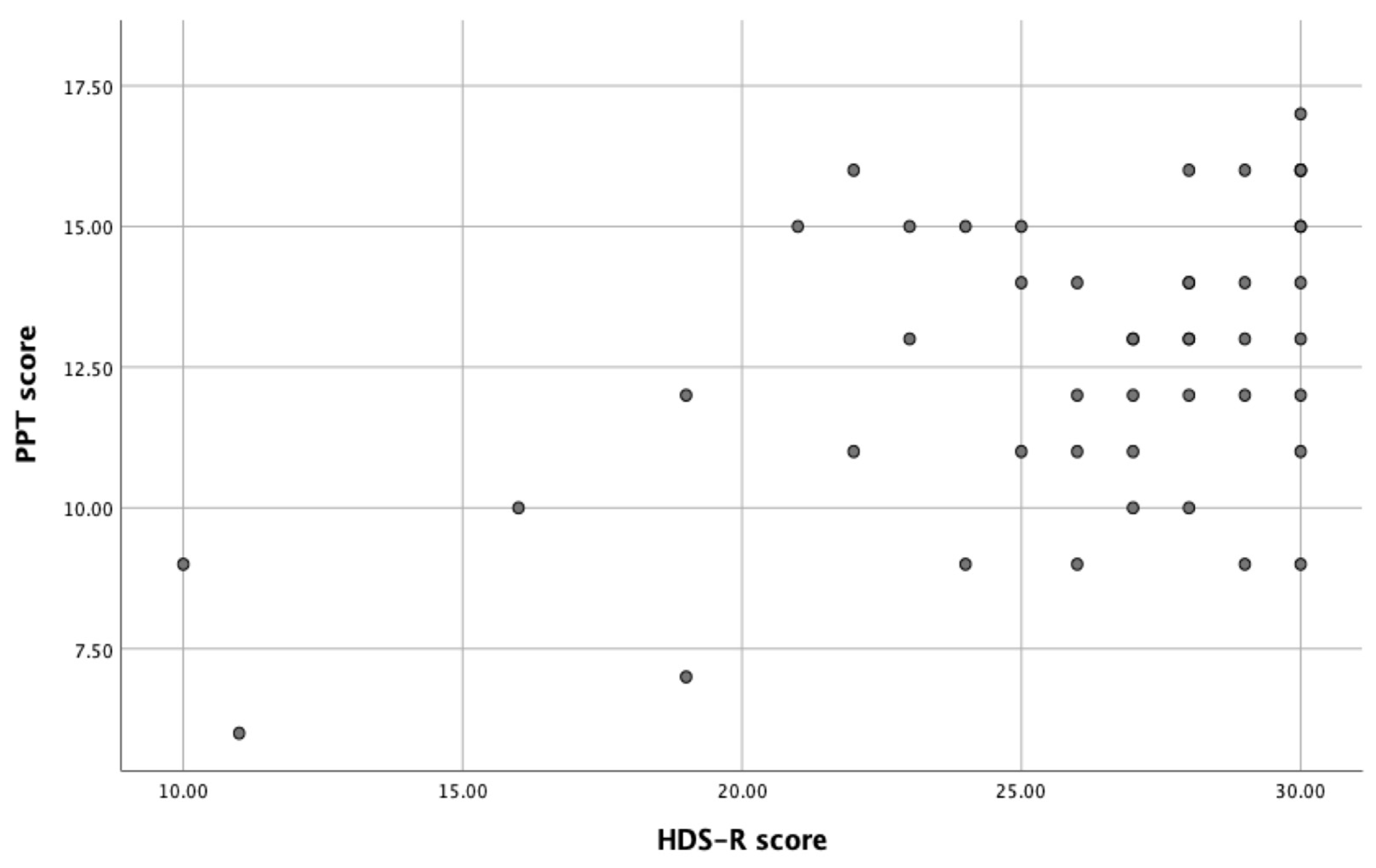
| HDS-R total score, median (range, IQR) | 27 (10–30, 5) |
| PPT score (mean ± SD) | 13 ± 3 |
| Insertion time, median (range, IQR) | 5 (2–31, 3.39) |
| Grip strength (kg), median (range, IQR) | 24.5 (13.9–48.2, 13) |
| Understanding of the surgical site, n | |
| Yes | 39 |
| No | 8 |
| Potential Affecting Factors | Regression Coefficient | Standardized Coefficients | p Value | VIF | |
|---|---|---|---|---|---|
| B | Std. Error | ||||
| Age | 0.080 | 0.167 | 0.130 | 0.634 | 3.875 |
| sex | −2.359 | 2.394 | −0.244 | 0.332 | 3.255 |
| Duration of wearing dentures before maxillectomy (years) | 0.114 | 0.102 | 0.203 | 0.272 | 1.758 |
| Communication between the oral and nasal cavities | 0.923 | 1.555 | 0.090 | 0.557 | 1.234 |
| Number of remaining teeth | 0.048 | 0.387 | 0.034 | 0.901 | 3.992 |
| Degree of mouth opening | −0.032 | 0.068 | −0.077 | 0.643 | 1.458 |
| Prosthesis materials | −1.356 | 2.916 | −0.078 | 0.645 | 1.504 |
| Prosthesis weight | −0.027 | 0.085 | −0.057 | 0.755 | 1.745 |
| Obturator height | −0.013 | 0.079 | −0.030 | 0.870 | 1.718 |
| Number of clasps | −0.328 | 0.820 | −0.110 | 0.692 | 3.997 |
| HDS-R total score | −0.394 | 0.251 | −0.379 | 0.127 | 3.113 |
| PPT score | −0.102 | 0.462 | −0.054 | 0.827 | 3.213 |
| Grip strength | −0.216 | 0.155 | −0.383 | 0.174 | 4.036 |
| Understanding the surgical site | −1.937 | 3.572 | −0.150 | 0.591 | 4.095 |
| (a) Model 1 | |||||
| Affecting Factors | Regression Coefficient | Standardized Coefficients | p Value | VIF | |
| B | Std. Error | ||||
| Age | 0.112 | 0.105 | 0.182 | 0.289 | 1.79 |
| Duration of wearing dentures before maxillectomy (years) | 0.135 | 0.079 | 0.24 | 0.102 | 1.292 |
| Prosthesis weight | −0.013 | 0.061 | −0.029 | 0.828 | 1.06 |
| HDS-R score | −0.357 | 0.157 | −0.344 | 0.028 | 1.43 |
| Grip strength | −0.110 | 0.092 | −0.194 | 0.24 | 1.662 |
| Adjusted R2: 0.264 | |||||
| (b) Model 2 | |||||
| Affecting Factors | Regression Coefficient | Standardized Coefficients | p Value | VIF | |
| B | Std. Error | ||||
| Duration of wearing dentures before maxillectomy (years) | 0.154 | 0.079 | 0.274 | 0.058 | 1.232 |
| Prosthesis weight | −0.025 | 0.06 | −0.053 | 0.68 | 1.026 |
| HDS-R score | −0.437 | 0.139 | −0.420 | 0.003 | 1.112 |
| Grip strength | −0.154 | 0.082 | −0.273 | 0.069 | 1.328 |
| Adjusted R2: 0.261 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Fujita, H.; Akiyama, M.; Sumita, Y.I.; Wakabayashi, N. Prevalence of Possible Dementia in Patients with Maxillofacial Defects and Difficulty of Inserting Obturator in Maxillectomy Patients: Toward Better Provision of Supportive Care. J. Clin. Med. 2023, 12, 2722. https://doi.org/10.3390/jcm12072722
Yu H, Fujita H, Akiyama M, Sumita YI, Wakabayashi N. Prevalence of Possible Dementia in Patients with Maxillofacial Defects and Difficulty of Inserting Obturator in Maxillectomy Patients: Toward Better Provision of Supportive Care. Journal of Clinical Medicine. 2023; 12(7):2722. https://doi.org/10.3390/jcm12072722
Chicago/Turabian StyleYu, Hongli, Haruka Fujita, Masako Akiyama, Yuka I. Sumita, and Noriyuki Wakabayashi. 2023. "Prevalence of Possible Dementia in Patients with Maxillofacial Defects and Difficulty of Inserting Obturator in Maxillectomy Patients: Toward Better Provision of Supportive Care" Journal of Clinical Medicine 12, no. 7: 2722. https://doi.org/10.3390/jcm12072722
APA StyleYu, H., Fujita, H., Akiyama, M., Sumita, Y. I., & Wakabayashi, N. (2023). Prevalence of Possible Dementia in Patients with Maxillofacial Defects and Difficulty of Inserting Obturator in Maxillectomy Patients: Toward Better Provision of Supportive Care. Journal of Clinical Medicine, 12(7), 2722. https://doi.org/10.3390/jcm12072722