
Opioids for Osteoarthritis: Cross-Sectional Survey of Patient Perspectives and Satisfaction
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
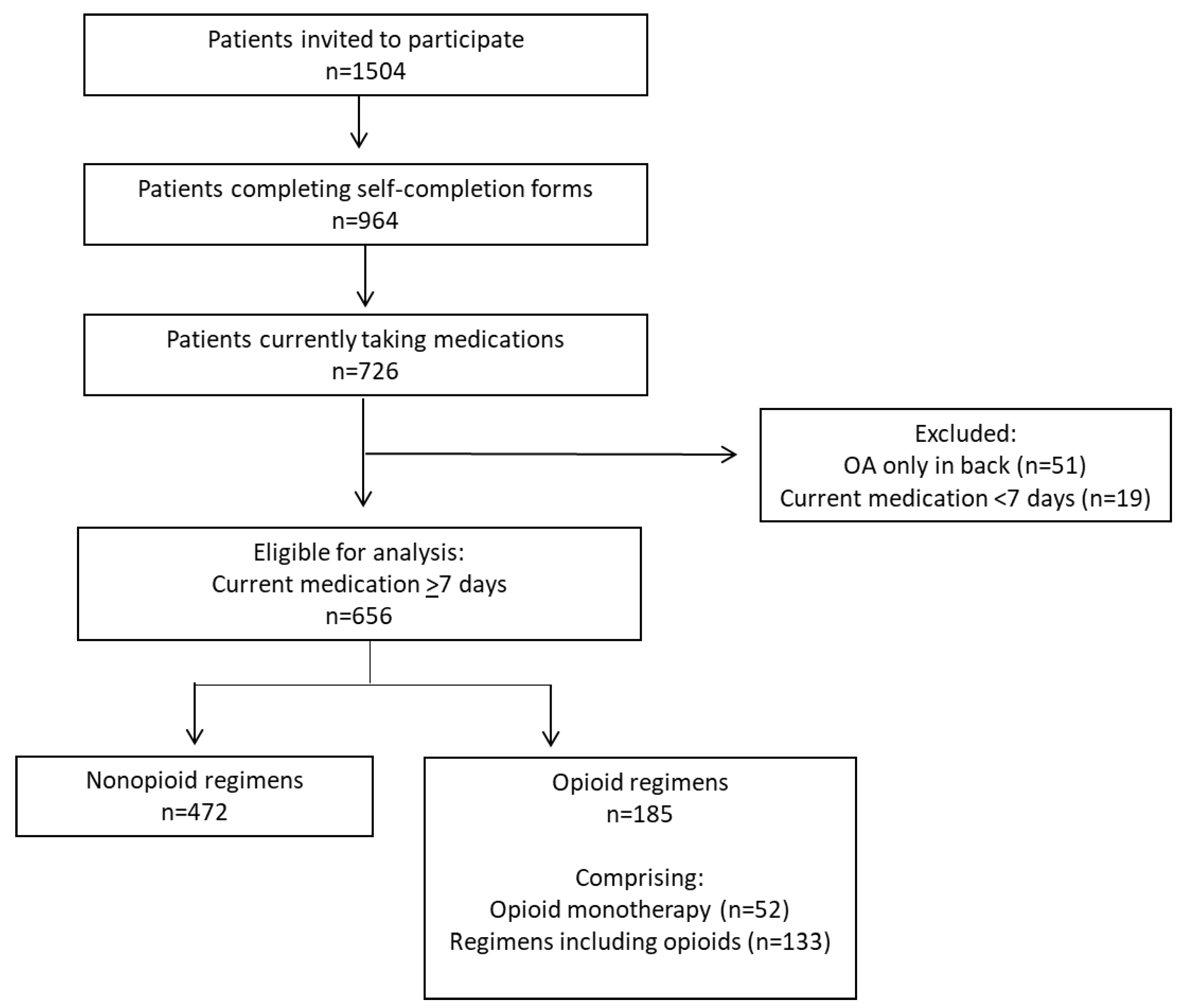
2.1. Study Population
2.2. Medication Regimens
2.3. Demographic, Clinical and Treatment Characteristics
2.4. Outcomes
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Patients across Medication Regimens
3.2. Patient-Reported Satisfaction with, Expectations of Effectiveness of, and Concerns about Medication Regimens (Patients Prescribed Current Medication for ≥7 Days)
3.3. Subgroup of Patients Prescribed Current Medication for ≥30 Days
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheatle, M.D. Prescription Opioid Misuse, Abuse, Morbidity, and Mortality: Balancing Effective Pain Management and Safety. Pain Med. 2015, 16 (Suppl. S1), S3–S8. [Google Scholar] [CrossRef] [Green Version]
- Trouvin, A.-P.; Berenbaum, F.; Perrot, S. The opioid epidemic: Helping rheumatologists prevent a crisis. RMD Open 2019, 5, e001029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tölle, T.; Fitzcharles, M.; Häuser, W. Is opioid therapy for chronic non-cancer pain associated with a greater risk of all-cause mortality compared to non-opioid analgesics? A systematic review of propensity score matched observational studies. Eur. J. Pain 2021, 25, 1195–1208. [Google Scholar] [CrossRef] [PubMed]
- Da Costa, B.R.; Nüesch, E.; Kasteler, R.; Husni, E.; Welch, V.; Rutjes, A.W.; Jüni, P. Oral or transdermal opioids for osteoarthritis of the knee or hip. Cochrane Database Syst. Rev. 2014, 17, CD003115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsch, P.; Petzke, F.; Klose, P.; Häuser, W. Opioids for chronic osteoarthritis pain: An updated systematic review and meta-analysis of efficacy, tolerability and safety in randomized placebo-controlled studies of at least 4 weeks double-blind duration. Eur. J. Pain 2019, 24, 685–703. [Google Scholar] [CrossRef] [PubMed]
- Osani, M.C.; Lohmander, L.S.; Bannuru, R.R. Is There Any Role for Opioids in the Management of Knee and Hip Osteoarthritis? A Systematic Review and Meta-Analysis. Arthritis Care Res. 2021, 73, 1413–1424. [Google Scholar] [CrossRef]
- April, K.T.; Bisaillon, J.; Welch, V.; Maxwell, L.J.; Jüni, P.; Rutjes, A.W.; Husni, M.E.; Vincent, J.; El Hindi, T.; Wells, G.A.; et al. Tramadol for osteoarthritis. Cochrane Database Syst. Rev. 2019, 2019, CD005522. [Google Scholar] [CrossRef]
- Fuggle, N.; Curtis, E.; Shaw, S.; Spooner, L.; Bruyère, O.; Ntani, G.; Parsons, C.; Conaghan, P.G.; Corp, N.; Honvo, G.; et al. Safety of Opioids in Osteoarthritis: Outcomes of a Systematic Review and Meta-Analysis. Drugs Aging 2019, 36, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.J.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. EULAR Recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a Task Force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Arden, N.; Bannwarth, B.; Bijlsma, J.; Gunther, K.-P.; Hauselmann, H.J.; Herrero-Beaumont, G.; Jordan, K.; Kaklamanis, P.; et al. EULAR evidence based recommendations for the management of hip osteoarthritis: Report of a task force of the EULAR Standing Committee for International Clinical Studies Including Therapeutics (ESCISIT). Ann. Rheum. Dis. 2005, 64, 669–681. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [Green Version]
- Kolasinski, S.L.; Neogi, T.; Hochberg, M.C.; Oatis, C.; Guyatt, G.; Block, J.; Callahan, L.; Copenhaver, C.; Dodge, C.; Felson, D.; et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020, 72, 149–162. [Google Scholar] [CrossRef]
- Silverman, S.; Rice, J.B.; White, A.G.; Beck, C.G.; Robinson, R.L.M.; Fernan, C.B.; Schepman, P. Clinical and economic burden of prescribing tramadol and other opioids for patients with osteoarthritis in a commercially insured population in the United States. Pain 2021, 163, 75–82. [Google Scholar] [CrossRef]
- Desai, R.J.; Jin, Y.; Franklin, P.D.; Lee, Y.C.; Bateman, B.T.; Lii, J.; Solomon, D.H.; Katz, J.N.; Kim, S.C. Association of Geography and Access to Health Care Providers With Long-Term Prescription Opioid Use in Medicare Patients With Severe Osteoarthritis: A Cohort Study. Arthritis Rheumatol. 2019, 71, 712–721. [Google Scholar] [CrossRef]
- DeMik, D.E.; Bedard, N.A.; Dowdle, S.B.; Burnett, R.A.; McHugh, M.A.; Callaghan, J.J. Are We Still Prescribing Opioids for Osteoarthritis? J. Arthroplast. 2017, 32, 3578–3582.e1. [Google Scholar] [CrossRef]
- Jackson, J.; Iyer, R.; Mellor, J.; Wei, W. The Burden of Pain Associated with Osteoarthritis in the Hip or Knee from the Patient’s Perspective: A Multinational Cross-Sectional Study. Adv. Ther. 2020, 37, 3985–3999. [Google Scholar] [CrossRef]
- van den Driest, J.J.; Schiphof, D.; De Wilde, M.; E Bindels, P.J.; Van Der Lei, J.; A Bierma-Zeinstra, S.M. Opioid prescriptions in patients with osteoarthritis: A population-based cohort study. Rheumatology 2020, 59, 2462–2470. [Google Scholar] [CrossRef]
- Bennell, K.L.; Bayram, C.; Harrison, C.; Brand, C.; Buchbinder, R.; Haas, R.; Hinman, R.S. Trends in management of hip and knee osteoarthritis in general practice in Australia over an 11-year window: A nationwide cross-sectional survey. Lancet Reg. Health West. Pac. 2021, 12, 100187. [Google Scholar] [CrossRef]
- Ebata-Kogure, N.; Murakami, A.; Nozawa, K.; Fujii, K.; Lin, Y.; Ushida, T.; Kikuchi, S. Treatment and Healthcare Cost Among Patients with Hip or Knee Osteoarthritis: A Cross-sectional Study Using a Real-world Claims Database in Japan Between 2013 and 2019. Clin. Drug Investig. 2020, 40, 1071–1084. [Google Scholar] [CrossRef]
- Cho, S.-K.; Jung, S.-Y.; Choi, S.; Im, S.G.; Kim, H.; Choi, W.S.; Jang, E.J.; Sung, Y.-K. Factors related to the use of opioids as early treatment in patients with knee osteoarthritis. Thromb. Haemost. 2019, 21, 222. [Google Scholar] [CrossRef] [Green Version]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. JAMA 2016, 315, 1624–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schnitzer, T.J.; Robinson, R.L.; Viktrup, L.; Cappelleri, J.C.; Bushmakin, A.G.; Tive, L.; Berry, M.; Walker, C.; Jackson, J. Opioid prescribing for osteoarthritis pain: Cross-sectional survey among primary care physicians, rheumatologists, and orthopedic surgeons. Int. J. Clin. Pract. 2022. submitted. [Google Scholar]
- Garrison, L.P.; Schepman, P.; Bushmakin, A.G.; Robinson, R.L.; Tive, L.; Hall, J.; Dzingina, M.; Jackson, J.; Berry, M.; Cappelleri, J.C.; et al. Concern about addiction is associated with lower quality of life in patients with osteoarthritis: An exploratory, real-world data analysis. Qual. Life Res. 2021, 31, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Ueda, K.; Sasaki, N.; Goren, A.; Calhoun, S.R.; Shinjo, K.; Enomoto, H.; Muneta, T. Treatment satisfaction with pharmaceutical interventions in Japanese adults with osteoarthritis and chronic knee pain: An analysis of a web-based survey. Clin. Interv. Aging 2018, 13, 2179–2191. [Google Scholar] [CrossRef] [Green Version]
- Gimenez, S.; Armada, B.; Iriso, J.I.; Mendoza, L.G.; Fernández-Morales, B. Clinical management of patients with hip and knee osteoarthritis: Patient satisfaction with treatment switch. Rheumatol. Int. 2014, 34, 823–832. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Jensen, M.P.; Gould, E.; Jones, B.A.; Xiang, Q.; Galer, B.S.; Gammaitoni, A.R. Treatment Satisfaction in Osteoarthritis and Chronic Low Back Pain: The Role of Pain, Physical and Emotional Functioning, Sleep, and Adverse Events. J. Pain 2011, 12, 416–424. [Google Scholar] [CrossRef]
- Schepman, P.; Thakkar, S.; Robinson, R.; Malhotra, D.; Emir, B.; Beck, C. Moderate to Severe Osteoarthritis Pain and Its Impact on Patients in the United States: A National Survey. J. Pain Res. 2021, 14, 2313–2326. [Google Scholar] [CrossRef]
- Robinson, R.L.; Schnitzer, T.J.; Barlow, S.; Berry, M.; Bushmakin, A.G.; Cappelleri, J.C.; Tive, L.; Jackson, J.; Jackson, J.; Viktrup, L. Satisfaction with Medications Prescribed for Osteoarthritis: A Cross-Sectional Survey of Patients and Their Physicians in the United States. Pain Ther. 2022, 11, 191–208. [Google Scholar] [CrossRef]
- Anderson, P.; Benford, M.; Harris, N.; Karavali, M.; Piercy, J. Real-world physician and patient behaviour across countries: Disease-Specific Programmes—A means to understand. Curr. Med. Res. Opin. 2008, 24, 3063–3072. [Google Scholar] [CrossRef]
- Theiler, R.; Spielberger, J.; Bischoff, H.; Bellamy, N.; Huber, J.; Kroesen, S. Clinical evaluation of the WOMAC 3.0 OA Index in numeric rating scale format using a computerized touch screen version. Osteoarthr. Cartil. 2002, 10, 479–481. [Google Scholar] [CrossRef] [Green Version]
- Herdman, M.; Gudex, C.; Lloyd, A.; Janssen, M.; Kind, P.; Parkin, D.; Bonsel, G.; Badia, X. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual. Life Res. 2011, 20, 1727–1736. [Google Scholar] [CrossRef] [Green Version]
- Rosner, B. Fundamentals of Biostatistics, 8th ed.; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Mehta, C.R.; Patel, N.R. A network algorithm for performing Fisher’s exact test in r × c contingency tables. J. Am. Stat. Assoc. 1983, 78, 427–434. [Google Scholar] [CrossRef]
- Nalamachu, S.R.; Robinson, R.L.; Viktrup, L.; Cappelleri, J.C.; Bushmakin, A.G.; Tive, L.; Mellor, J.; Hatchell, N.; Jackson, J. Multimodal Treatment Patterns for Osteoarthritis and Their Relationship to Patient-Reported Pain Severity: A Cross-Sectional Survey in the United States. J. Pain Res. 2020, 13, 3415–3425. [Google Scholar] [CrossRef]
- King, L.; Marshall, D.; Jones, C.; Woodhouse, L.; Ravi, B.; Faris, P.; Hawker, G.; Bohm, E.; Dunbar, M.; Noseworthy, T. Are medical comorbidities contributing to the use of opioid analgesics in patients with knee osteoarthritis? Osteoarthr. Cartil. 2020, 28, 1030–1037. [Google Scholar] [CrossRef]
- Power, J.D.; Perruccio, A.V.; Gandhi, R.; Veillette, C.; Davey, J.R.; Lewis, S.J.; Syed, K.; Mahomed, N.N.; Rampersaud, Y.R. Factors Associated with Opioid Use in Presurgical Knee, Hip, and Spine Osteoarthritis Patients. Arthritis Care Res. 2019, 71, 1178–1185. [Google Scholar] [CrossRef]
- Hoogeboom, T.J.; den Broeder, A.A.; Swierstra, B.A.; De Bie, R.A.; van den Ende, C.H. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: A cross-sectional study. Arthritis Care Res. 2012, 64, 54–58. [Google Scholar] [CrossRef]
- Muckelt, P.E.; Roos, E.M.; Stokes, M.; McDonough, S.; Grønne, D.T.; Ewings, S.T.; Skou, S. Comorbidities and their link with individual health status: A cross-sectional analysis of 23,892 people with knee and hip osteoarthritis from primary care. J. Comorb. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Radu, A.-F.; Bungau, S.G.; Tit, D.M.; Behl, T.; Uivaraseanu, B.; Marcu, M.F. Highlighting the Benefits of Rehabilitation Treatments in Hip Osteoarthritis. Medicina 2022, 58, 494. [Google Scholar] [CrossRef]
- Skou, S.T.; Roos, E.M. Physical therapy for patients with knee and hip osteoarthritis: Supervised, active treatment is current best practice. Clin. Exp. Rheumatol. 2019, 37, 112–117, Erratum in Clin. Exp. Rheumatol. 2020, 38, 1036. [Google Scholar]


{kind=link}
| Nonopioid Regimens (n = 471) | Opioid Regimens (n = 185) | p Value | |
|---|---|---|---|
| Currently prescribed medication, n (%) | |||
| NSAID | 400 (84.9) | 103 (55.7) | <0.0001 |
| Tramadol | 0 (0.0) | 104 (56.2) | NA |
| Non-tramadol opioid | 0 (0.0) | 93 (50.3) | NA |
| Corticosteroid | 39 (8.3) | 39 (21.1) | <0.0001 |
| Viscosupplementation | 27 (5.7) | 9 (4.9) | 0.6606 |
| Other a | 122 (25.9) | 68 (36.8) | 0.0058 |
| Current medication regimen duration, mean (SD), week b | 37.59 (32.13) | 37.81 (33.28) | 0.9364 |
| Current medication regimen duration ≥30 days, n (%) b | 407 (86.4) | 173 (93.5) | 0.0105 |
| Lines of OA medication, mean (SD) | 1.74 (0.93) | 2.47 (0.94) | <0.0001 |
| Over-the-counter medication recommended, n (%) | 147 (31.2) | 70 (37.8) | 0.1045 |
| Nonpharmacologic therapy, n (%) | |||
| Physical or occupational therapy | 195 (41.4) | 116 (62.7) | <0.0001 |
| Acupuncture | 25 (5.3) | 19 (10.3) | 0.0222 |
| TENS | 15 (3.2) | 28 (15.1) | <0.0001 |
| CBT / psychotherapy | 7 (1.5) | 11 (5.9) | 0.0017 |
| Opioid dose-sparing approach for this patient, n (%) c | <0.0001 | ||
| Currently trying | 79 (16.8) | 51 (27.6) | |
| Tried in the past but not currently | 19 (4.0) | 32 (17.3) | |
| No but will consider in the future | 206 (43.7) | 67 (36.2) | |
| Never will consider | 167 (35.5) | 35 (18.9) |
| Nonopioid Regimens (n = 471) | Opioid Regimens (n = 185) | p Value | |
|---|---|---|---|
| Age, y | |||
| Mean (SD) | 64.70 (11.18) | 66.86 (11.32) | 0.0268 |
| <55, n (%) | 81 (17.2) | 27 (14.6) | 0.0452 |
| 55–64, n (%) | 143 (30.4) | 48 (25.9) | |
| 65–74, n (%) | 162 (34.4) | 63 (34.1) | |
| ≥75, n (%) | 85 (18.0) | 47 (25.4) | |
| Female, n (%) | 286 (60.7) | 109 (58.9) | 0.6712 |
| Ethnicity, n (%) | 0.0377 | ||
| White/Caucasian | 375 (79.6) | 135 (73.0) | |
| African American | 54 (11.5) | 24 (13.0) | |
| Native American | 2 (0.4) | 1 (0.5) | |
| Asian-Indian subcontinent | 5 (1.1) | 1 (0.5) | |
| Asian—other | 5 (1.1) | 1 (0.5) | |
| Chinese | 1 (0.2) | 0 (0.0) | |
| Hispanic/Latino | 28 (5.9) | 17 (9.2) | |
| Middle Eastern | 0 (0.0) | 3 (1.6) | |
| Mixed race | 1 (0.2) | 3 (1.6) | |
| Body mass index, kg/m2 | |||
| Mean (SD) | 29.09 (5.66) | 29.98 (6.44) | 0.0822 |
| <30, n (%) | 294 (62.4) | 105 (56.8) | 0.1815 |
| ≥30, n (%) | 177 (37.6) | 80 (43.2) | |
| Number of comorbidities, mean (SD) e | 2.13 (1.76) | 3.79 (2.50) | <0.0001 |
| Number of medications currently received to treat concomitant conditions, mean (SD) | 2.08 (1.76) | 3.76 (2.55) | <0.0001 |
| Number of affected joints, mean (SD) | 3.19 (2.44) | 4.42 (2.68) | <0.0001 |
| Years since OA diagnosis, mean (SD) a | 2.26 (2.91) | 4.15 (4.17) | <0.0001 |
| Location of affected joints, n (%) | |||
| Knee | 302 (64.1) | 123 (66.5) | 0.5678 |
| Hip | 162 (34.4) | 78 (42.2) | 0.0631 |
| Back | 146 (31.0) | 99 (53.5) | <0.0001 |
| Other | 221 (46.9) | 115 (62.2) | 0.0004 |
| Pain intensity, on average in the last week b | |||
| Mean score (SD) | 4.11 (2.30) | 5.47 (2.18) | <0.0001 |
| Mild (0–3), n (%) | 216 (46.7) | 43 (23.9) | <0.0001 |
| Moderate (4–6), n (%) | 171 (36.9) | 78 (43.3) | |
| Severe (7–10), n (%) | 76 (16.4) | 59 (32.8) | |
| WOMAC Physical Function c | |||
| Mean score (SD) | 3.13 (2.11) | 4.98 (2.48) | <0.0001 |
| Mild (0–3), n (%) | 294 (67.4) | 50 (30.9) | <0.0001 |
| Moderate (4–6), n (%) | 101 (23.2) | 61 (37.7) | |
| Severe (7–10), n (%) | 41 (9.4) | 51 (31.5) | |
| EQ-5D-5L index value, mean (SD) d | 0.71 (0.22) | 0.45 (0.37) | <0.0001 |
| Nonopioid Regimens (n = 471) | Opioid Regimens (n = 185) | |
|---|---|---|
| Reasons for choice of current medication a | ||
| Efficacy | 261 (55.4) | 123 (66.5) |
| Safety | 267 (56.7) | 99 (53.5) |
| Quality of life | 88 (18.7) | 58 (31.4) |
| Cost considerations | 58 (12.3) | 26 (14.1) |
| Convenience/acceptability | 59 (12.5) | 49 (26.5) |
| Issues with current medication regimen b | ||
| No current issues | 371 (78.8) | 102 (55.1) |
| Lack of efficacy | 66 (14.0) | 52 (28.1) |
| Patient decision | 13 (2.8) | 12 (6.5) |
| Drug interactions/comorbidities | 2 (0.4) | 5 (2.7) |
| Adverse events or tolerability issues | 26 (5.5) | 54 (29.2) |
| Worries about addiction | 4 (0.8) | 16 (8.6) |
| Cost or access issues | 3 (0.6) | 3 (1.6) |
| Nonopioid Regimens | Opioid Regimens | Medication Regimen Comparison | |||||
|---|---|---|---|---|---|---|---|
| Models | Scores (1 to5) Higher Score = | n | LS Mean (95% CI) | n | LS Mean (95% CI) | LS Mean Difference (95% CI) | p Value |
| Satisfaction | Greater satisfaction | ||||||
| overall, with regimen | 392 | 3.67 (3.50, 3.84) | 161 | 3.40 (3.16, 3.64) | −0.27 (−0.52, −0.02) | 0.0322 | |
| with pain relief | 417 | 3.52 (3.38, 3.67) | 169 | 3.29 (3.10, 3.48) | −0.23 (−0.42, −0.05) | 0.0132 | |
| with functional change | 415 | 3.61 (3.47, 3.74) | 168 | 3.22 (3.06, 3.38) | −0.39 (−0.54, −0.23) | <0.0001 | |
| with tolerability | 407 | 3.63 (3.48, 3.78) | 168 | 3.42 (3.27, 3.58) | −0.21 (−0.39, −0.03) | 0.0208 | |
| with convenience | 414 | 3.92 (3.80, 4.04) | 168 | 3.64 (3.52, 3.76) | −0.28 (−0.42, −0.14) | <0.0001 | |
| Expectations of effectiveness of medications | Met expectation better | 414 | 3.13 (2.98, 3.28) | 167 | 2.72 (2.55, 2.90) | −0.41 (−0.59, −0.24) | <0.0001 |
| Concerns | Stronger agreement | ||||||
| about treatments not being very good | 463 | 3.22 (3.01, 3.42) | 180 | 3.66 (3.41, 3.92) | 0.45 (0.16, 0.73) | 0.0026 | |
| about becoming addicted | 414 | 2.65 (2.41, 2.89) | 165 | 3.30 (3.00, 3.59) | 0.65 (0.37, 0.93) | <0.0001 | |
| Nonopioid Regimens | Opioid Regimens | Medication Regimen Comparison | |||||
|---|---|---|---|---|---|---|---|
| Models | Scores (1 to5) Higher Score = | n | LS Mean (95% CI) | n | LS Mean (95% CI) | LS mean Difference (95% CI) | p Value |
| Satisfaction | Greater satisfaction | ||||||
| overall, with regimen | 346 | 3.68 (3.48, 3.87) | 151 | 3.38 (3.12, 3.64) | −0.30 (−0.56, −0.03) | 0.0267 | |
| with pain relief | 364 | 3.54 (3.38, 3.70) | 158 | 3.26 (3.07, 3.46) | −0.27 (−0.47, −0.08) | 0.0056 | |
| with functional change | 363 | 3.60 (3.45, 3.75) | 157 | 3.18 (3.01, 3.34) | −0.42 (−0.59, −0.25) | <0.0001 | |
| with tolerability | 355 | 3.61 (3.45, 3.76) | 157 | 3.42 (3.26, 3.58) | −0.19 (−0.37, −0.00) | 0.0469 | |
| with convenience | 362 | 3.88 (3.76, 4.01) | 157 | 3.63 (3.50, 3.75) | −0.26 (−0.40, −0.12) | 0.0004 | |
| Expectations of effectiveness of medications | Met expectation better | 362 | 3.10 (2.95, 3.25) | 157 | 2.68 (2.50, 2.86) | −0.42 (−0.60, −0.24) | <0.0001 |
| Concerns | Stronger agreement | ||||||
| about treatments not being very good | 402 | 3.27 (3.03, 3.50) | 168 | 3.69 (3.43, 3.95) | 0.42 (0.12, 0.73) | 0.0074 | |
| about becoming addicted | 355 | 2.61 (2.37, 2.86) | 154 | 3.26 (2.96, 3.56) | 0.65 (0.37, 0.92) | <0.0001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnitzer, T.J.; Robinson, R.L.; Viktrup, L.; Cappelleri, J.C.; Bushmakin, A.G.; Tive, L.; Berry, M.; Walker, C.; Jackson, J. Opioids for Osteoarthritis: Cross-Sectional Survey of Patient Perspectives and Satisfaction. J. Clin. Med. 2023, 12, 2733. https://doi.org/10.3390/jcm12072733
Schnitzer TJ, Robinson RL, Viktrup L, Cappelleri JC, Bushmakin AG, Tive L, Berry M, Walker C, Jackson J. Opioids for Osteoarthritis: Cross-Sectional Survey of Patient Perspectives and Satisfaction. Journal of Clinical Medicine. 2023; 12(7):2733. https://doi.org/10.3390/jcm12072733
Chicago/Turabian StyleSchnitzer, Thomas J., Rebecca L. Robinson, Lars Viktrup, Joseph C. Cappelleri, Andrew G. Bushmakin, Leslie Tive, Mia Berry, Chloe Walker, and James Jackson. 2023. "Opioids for Osteoarthritis: Cross-Sectional Survey of Patient Perspectives and Satisfaction" Journal of Clinical Medicine 12, no. 7: 2733. https://doi.org/10.3390/jcm12072733
APA StyleSchnitzer, T. J., Robinson, R. L., Viktrup, L., Cappelleri, J. C., Bushmakin, A. G., Tive, L., Berry, M., Walker, C., & Jackson, J. (2023). Opioids for Osteoarthritis: Cross-Sectional Survey of Patient Perspectives and Satisfaction. Journal of Clinical Medicine, 12(7), 2733. https://doi.org/10.3390/jcm12072733