
The Impact of Color Vision Deficiency on the Capability of Ophthalmologists to Diagnose Benign and Malignant Choroidal Tumors

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
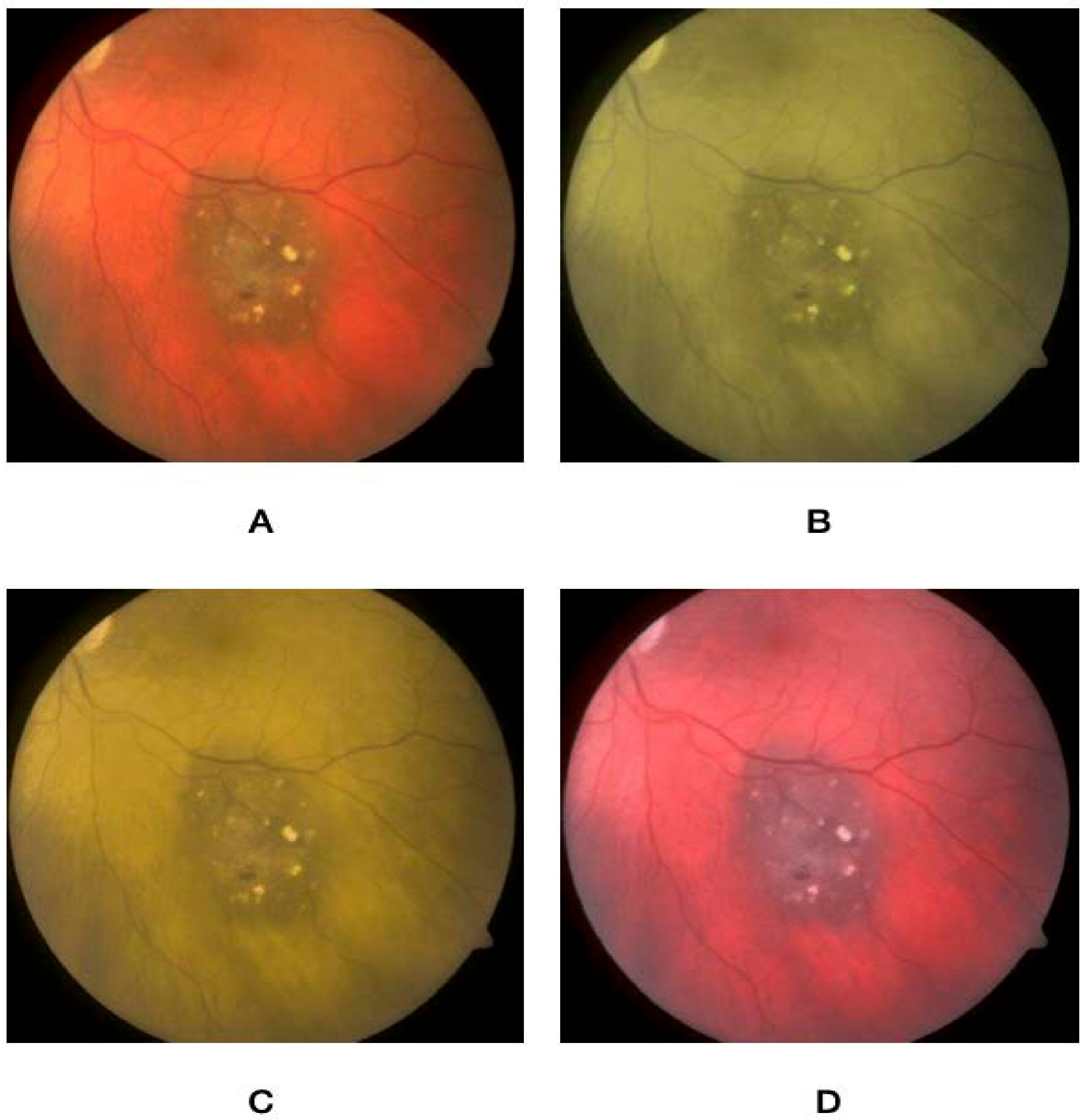
2.2. CVD Simulation and Assessment
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Campbell, J.L.; Spalding, A.J.; Mir, F.A.; Birch, J. Doctors and the Assessment of Clinical Photographs—Does Colour Blindness Matter? Br. J. Gen. Pract. J. R. Coll. Gen. Pract. 1999, 49, 459–461. [Google Scholar]
- Balasundaram, R.; Reddy, S.C. Prevalence of Colour Vision Deficiency among Medical Students and Health Personnel. Malays. Fam. Physician Off. J. Acad. Fam. Physicians Malays. 2006, 1, 52–53. [Google Scholar]
- Chan, X.B.V.; Goh, S.M.S.; Tan, N.C. Subjects with Colour Vision Deficiency in the Community: What Do Primary Care Physicians Need to Know? Asia Pac. Fam. Med. 2014, 13, 10. [Google Scholar] [CrossRef] [Green Version]
- Shields, C.L.; Manalac, J.; Das, C.; Ferguson, K.; Shields, J.A. Choroidal Melanoma: Clinical Features, Classification, and Top 10 Pseudomelanomas. Curr. Opin. Ophthalmol. 2014, 25, 177–185. [Google Scholar] [CrossRef]
- Bornfeld, N.; Biewald, E.; Bauer, S.; Temming, P.; Lohmann, D.; Zeschnigk, M. The Interdisciplinary Diagnosis and Treatment of Intraocular Tumors. Dtsch. Ärztebl. Int. 2018, 115, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Schalenbourg, A.; Zografos, L. Pitfalls in colour photography of choroidal tumours. Eye 2013, 27, 224–229. [Google Scholar] [CrossRef] [Green Version]
- Solnik, M.; Paduszyńska, N.; Czarnecka, A.M.; Synoradzki, K.J.; Yousef, Y.A.; Chorągiewicz, T.; Rejdak, R.; Toro, M.D.; Zweifel, S.; Dyndor, K.; et al. Imaging of Uveal Melanoma—Current Standard and Methods in Development. Cancers 2022, 14, 3147. [Google Scholar] [CrossRef]
- Toro, M.D.; Gozzo, L.; Tracia, L.; Cicciù, M.; Drago, F.; Bucolo, C.; Avitabile, T.; Rejdak, R.; Nowomiejska, K.; Zweifel, S.; et al. New Therapeutic Perspectives in the Treatment of Uveal Melanoma: A Systematic Review. Biomedicines 2021, 9, 1311. [Google Scholar] [CrossRef]
- Jain, P.; Finger, P.T.; Damato, B.; Coupland, S.E.; Heimann, H.; Kenawy, N.; Brouwer, N.J.; Marinkovic, M.; Van Duinen, S.G.; Caujolle, J.P.; et al. Multicenter, International Assessment of the Eighth Edition of the American Joint Committee on Cancer Cancer Staging Manual for Conjunctival Melanoma. JAMA Ophthalmol. 2019, 137, 905–911. [Google Scholar] [CrossRef] [Green Version]
- Jaradat, I.; Zewar, A.; AlNawaiseh, I.; AlRawashdeh, K.; Khurma, S.; Mehyar, M.; Abdeen, G.; Yousef, Y.A. Characteristics, management, and outcome of patients with uveal melanoma treated by Iodine-125 radioactive plaque therapy in a single tertiary cancer center in Jordan. Saudi J. Ophthalmol. 2018, 32, 130–133. [Google Scholar] [CrossRef]
- Zewar, A.; Nawaiseh, I.; Jaradat, I.; Khzouz, J.; Alrawashdeh, K.; Abdeen, G.; Mehyar, M.; Khurma, S.; Yousef, Y.A. Management and Outcome of Uveal Melanoma in a Single Tertiary Cancer Center in Jordan. Turk Patoloji Derg. 2016, 32, 186–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nawaiseh, I.; Sultan, I.; Mehyar, M.; Haddad, H.; Yousef, Y.A. Amelanotic choroidal melanoma in 16-month-old child. Can. J. Ophthalmol. 2013, 48, e87–e90. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Kalyani, P.; Topham, A. Estimating the risk of malignant transformation of a choroidal nevus. Ophthalmology 2005, 112, 1784–1789. [Google Scholar] [CrossRef]
- Maheshwari, A.; Finger, P.T. Cancers of the eye. Cancer Metastasis Rev. 2018, 37, 677–690. [Google Scholar] [CrossRef] [PubMed]
- Yousef, Y.A.; Finger, P.T. Lack of radiation maculopathy after palladium-103 plaque radiotherapy for iris melanoma. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 1107–1112. [Google Scholar] [CrossRef]
- Schindelin, J.; Arganda-Carreras, I.; Frise, E.; Kaynig, V.; Longair, M.; Pietzsch, T.; Preibisch, S.; Rueden, C.; Saalfeld, S.; Schmid, B.; et al. Fiji—An Open Source Platform for Biological Image Analysis. Nat. Methods 2012, 9, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Lillo, J.; Alvaro, L.; Moreira, H. An Experimental Method for the Assessment of Color Simulation Tools. J. Vis. 2014, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlRyalat, S.A.; Muhtaseb, R.; Alshammari, T. Simulating a Colour-Blind Ophthalmologist for Diagnosing and Staging Diabetic Retinopathy. Eye 2020, 35, 2229–2232. [Google Scholar] [CrossRef]
- Steward, J.M.; Cole, B.L. What Do Color Vision Defectives Say about Everyday Tasks? Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 1989, 66, 288–295. [Google Scholar] [CrossRef]
- Goh, S.; Chan, V.; Tan, N. Colour Vision Deficiency: Is It a Handicap? A Narrative Review of Its Impact on Medical & Dental Education and Practice. Proc. Singap. Healthc. 2014, 23, 149–157. [Google Scholar]
- Spalding, J.A. Colour Vision Deficiency in the Medical Profession. Br. J. Gen. Pract. 1999, 49, 469–475. [Google Scholar] [PubMed]
- Spalding, J.A.B.; Cole, B.L.; Mir, F.A. Advice for Medical Students and Practitioners with Colour Vision Deficiency: A Website Resource. Clin. Exp. Optom. 2010, 93, 39–41. [Google Scholar] [CrossRef] [PubMed]
- Pandit, R.; Dhakal, R. Assessment of Color Vision among Health Science Students. Nepal Med. Coll. J. 2020, 22, 49–53. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Simulated Images Diagnosis Score | Simulated Protanopia Images Diagnosis Score | Simulated Deuteranopia Images Diagnosis Score | Simulated Tritanopia Images Diagnosis Score | |||||
|---|---|---|---|---|---|---|---|---|
| Choroidal Lesion | Correct (%) | Correct (%) | p Value | Correct (%) | p Value | Correct (%) | p Value | |
| Normal | Diagnosis | 41 (100%) | 32 (78%) | 0.002 | 33 (81%) | 0.005 | 40 (98%) | 1.00 |
| Need for referral | 41 (100%) | 40 (98%) | 1.00 | 40 (98%) | 1.00 | 41 (100%) | 1.00 | |
| Hemangioma | Diagnosis | 16 (39%) | 5 (12%) | 0.01 | 6 (15%) | 0.02 | 13 (32%) | 0.64 |
| Need for referral | 38 (93%) | 31 (76%) | 0.70 | 34 (83%) | 0.31 | 35 (85%) | 0.47 | |
| Nevus | Diagnosis | 36 (88%) | 26 (63%) | 0.019 | 24 (59%) | 0.005 | 34 (83%) | 0.75 |
| Need for referral | 39 (95%) | 32 (78%) | 0.007 | 30 (73%) | 0.003 | 38 (93%) | 1.00 | |
| Melanoma | Diagnosis | 38 (93%) | 30 (73%) | 0.03 | 30 (73%) | 0.03 | 36 (88%) | 0.70 |
| Need for referral | 41 (100%) | 39 (95%) | 0.49 | 40 (98%) | 1.00 | 41 (100%) | 1.00 | |
| Metastasis | Diagnosis | 30 (73%) | 19 (46%) | 0.024 | 18 (44%) | 0.013 | 26 (63%) | 0.47 |
| Need for referral | 38 (93%) | 34 (83%) | 0.31 | 35 (85%) | 0.48 | 39 (95%) | 1.00 | |
| 41 Participants (41) | Specialty | ||||
|---|---|---|---|---|---|
| Overall (41) | General Ophthalmologists (28) | Retina Specialist & Ocular Oncologist (13) | p Value | ||
| N (%) | N (%) | N (%) | |||
| Non-simulated images diagnosis score | Overall Score | 36 (88%) | 23 (82%) | 13 (100%) | 0.159 |
| Benign vs. Malignant | 40 (98%) | 27 (96%) | 13 (100%) | 1.00 | |
| p value | 0.201 | 0.19 | 1.00 | ||
| Simulated protanopia images diagnosis score | Overall Score | 30 (%) | 20 (%) | 10 (%) | 1.00 |
| Benign vs. Malignant | 38 (%) | 26 (%) | 12 (%) | 1.00 | |
| p value | 0.037 | 0.07 | 0.59 | ||
| Simulated deuteranopia images diagnosis score | Overall Score | 28 (%) | 18 (%) | 10 (%) | 0.49 |
| Benign vs. Malignant | 37 (%) | 25 (%) | 12 (%) | 0.45 | |
| p value | 0.027 | 0.055 | 0.59 | ||
| Simulated tritanopia images diagnosis Score | Overall Score | 35 (%) | 23 (%) | 12 (%) | 0.644 |
| Benign vs. Malignant | 39 (%) | 26 (%) | 13 (%) | 1.00 | |
| p value | 0.26 | 0.42 | 1.00 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elfalah, M.; AlRyalat, S.A.; Abu-Yaghi, N.E.; Mohammad, M.; AlNawiaseh, I.; Rayyan, D.; Albliwi, M.; Elfalah, M.; AlSarairah, F.; Yousef, Y.A. The Impact of Color Vision Deficiency on the Capability of Ophthalmologists to Diagnose Benign and Malignant Choroidal Tumors. J. Clin. Med. 2023, 12, 2744. https://doi.org/10.3390/jcm12072744
Elfalah M, AlRyalat SA, Abu-Yaghi NE, Mohammad M, AlNawiaseh I, Rayyan D, Albliwi M, Elfalah M, AlSarairah F, Yousef YA. The Impact of Color Vision Deficiency on the Capability of Ophthalmologists to Diagnose Benign and Malignant Choroidal Tumors. Journal of Clinical Medicine. 2023; 12(7):2744. https://doi.org/10.3390/jcm12072744
Chicago/Turabian StyleElfalah, Mutasem, Saif Aldeen AlRyalat, Nakhleh E. Abu-Yaghi, Mona Mohammad, Ibrahim AlNawiaseh, Deema Rayyan, Moath Albliwi, Mohammad Elfalah, Fawaz AlSarairah, and Yacoub A. Yousef. 2023. "The Impact of Color Vision Deficiency on the Capability of Ophthalmologists to Diagnose Benign and Malignant Choroidal Tumors" Journal of Clinical Medicine 12, no. 7: 2744. https://doi.org/10.3390/jcm12072744
APA StyleElfalah, M., AlRyalat, S. A., Abu-Yaghi, N. E., Mohammad, M., AlNawiaseh, I., Rayyan, D., Albliwi, M., Elfalah, M., AlSarairah, F., & Yousef, Y. A. (2023). The Impact of Color Vision Deficiency on the Capability of Ophthalmologists to Diagnose Benign and Malignant Choroidal Tumors. Journal of Clinical Medicine, 12(7), 2744. https://doi.org/10.3390/jcm12072744