
Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes—CAESAR Study
 ,
,  ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Study Information
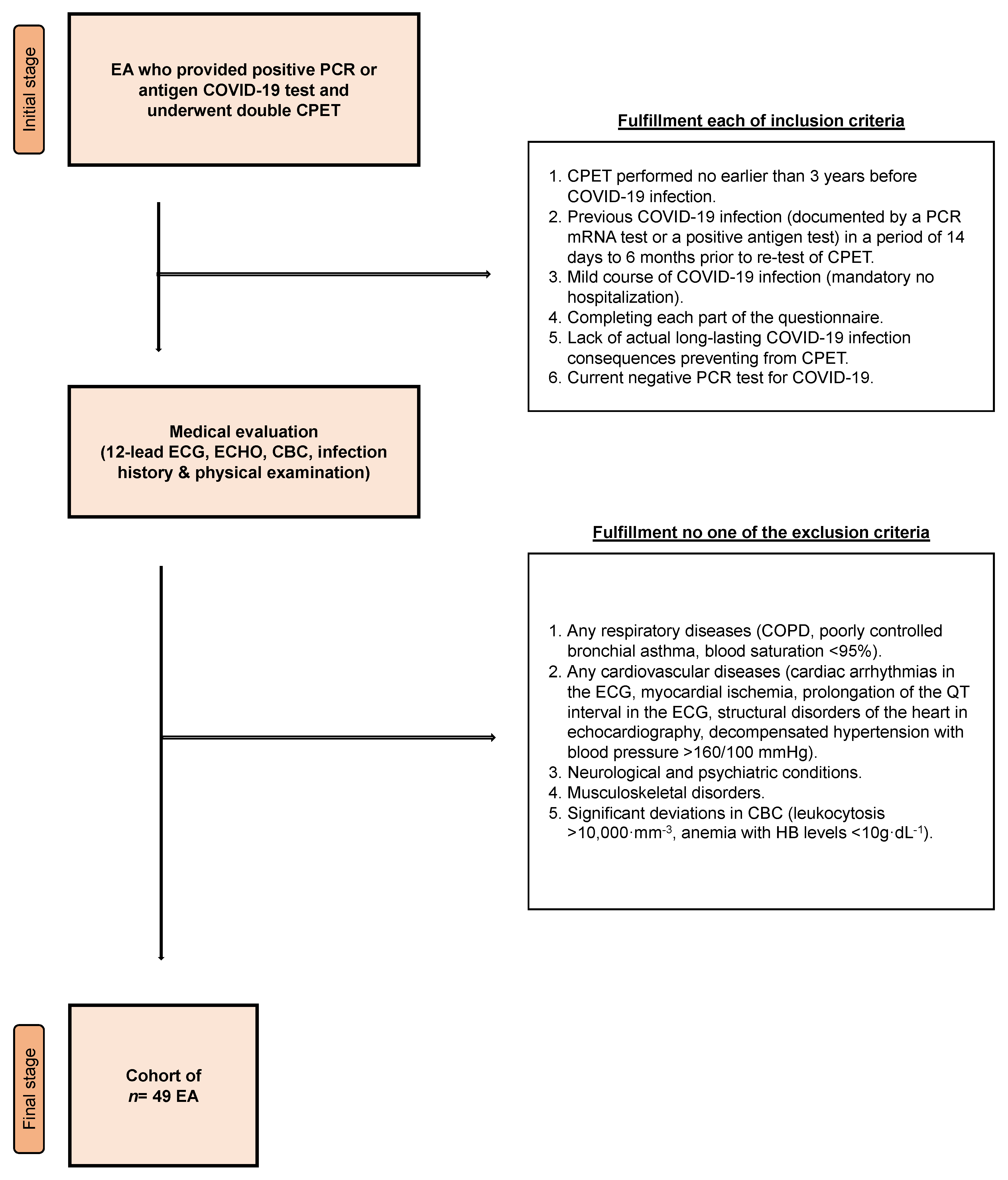
2.2. Cohort Description
2.3. Questionnaire
2.3.1. Mental Health Section
2.3.2. Sleep Section
2.4. CPET Procedure and Somatic Measurements
2.5. Data Analysis
3. Results
3.1. CPET Performance
3.2. Sleep and Mental Health
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tagliabue, F.; Galassi, L.; Mariani, P. The “Pandemic” of Disinformation in COVID-19. SN Compr. Clin. Med. 2020, 2, 1287–1289. [Google Scholar] [CrossRef] [PubMed]
- Makowska, M.; Boguszewski, R.; Podkowińska, M. Trust in Medicine as a Factor Conditioning Behaviors Recommended by Healthcare Experts during the COVID-19 Pandemic in Poland. Int. J. Envirion. Res. Public Health 2022, 19, 605. [Google Scholar] [CrossRef] [PubMed]
- Sharif, N.; Alzahrani, K.J.; Ahmed, S.N.; Dey, S.K. Efficacy, Immunogenicity and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 714170. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Roy, D.; Sinha, K.; Parveen, S.; Sharma, G.; Joshi, G. Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review with recommendations. Psychiatry Res. 2020, 293, 113429. [Google Scholar] [CrossRef]
- Rahmati, M.; Koyanagi, A.; Banitalebi, E.; Yon, D.K.; Lee, S.W.; Il Shin, J.; Smith, L. The effect of SARS-CoV-2 infection on cardiac function in post-COVID-19 survivors: A systematic review and meta-analysis. J. Med. Virol. 2023, 95, e28325. [Google Scholar] [CrossRef]
- Lemos, M.M.; Cavalini, G.R.; Pugliese Henrique, C.R.; Perli, V.A.S.; de Moraes Marchiori, G.; Marchiori, L.L.M.; Sordi, A.F.; Franzoi de Moraes, S.M.; de Paula Ramos, S.; Valdes-Badilla, P.; et al. Body composition and cardiorespiratory fitness in overweight or obese people post COVID-19: A comparative study. Front. Physiol. 2022, 13, 949351. [Google Scholar] [CrossRef]
- Ryal, J.J.; Perli, V.A.S.; Marques, D.C.S.; Sordi, A.F.; Marques, M.G.S.; Camilo, M.L.; Milani, R.G.; Mota, J.; Valdes-Badilla, P.; Magnani Branco, B.H. Effects of a Multi-Professional Intervention on Mental Health of Middle-Aged Overweight Survivors of COVID-19: A Clinical Trial. Int. J. Environ. Res. Public Health 2023, 20, 4132. [Google Scholar] [CrossRef]
- Gielen, S.; Laughlin, M.H.; O’Conner, C.; Duncker, D.J. Exercise training in patients with heart disease: Review of beneficial effects and clinical recommendations. Prog. Cardiovasc. Dis. 2015, 57, 347–355. [Google Scholar] [CrossRef]
- Belen, H. Fear of COVID-19 and Mental Health: The Role of Mindfulness in during Times of Crisis. Int. J. Ment. Health Addict. 2022, 20, 607–618. [Google Scholar] [CrossRef]
- Min, S.K.; Son, W.H.; Choi, B.H.; Lee, H.J.; Ahn, C.Y.; Yoo, J.; Park, S.; Lee, J.W.; Jee, Y.S. Psychophysical condition of adolescents in coronavirus disease 2019. J. Exerc. Rehabil. 2021, 17, 112–119. [Google Scholar] [CrossRef]
- Makarowski, R.; Predoiu, R.; Piotrowski, A.; Görner, K.; Predoiu, A.; Oliveira, R.; Pelin, R.A.; Moanță, A.D.; Boe, O.; Rawat, S.; et al. Coping Strategies and Perceiving Stress among Athletes during Different Waves of the COVID-19 Pandemic-Data from Poland, Romania, and Slovakia. Healthcare 2022, 10, 1770. [Google Scholar] [CrossRef]
- Harman, B.; Dessart, G.; Puke, L.; Philippe, R.A. Coping and Resilience Among Endurance Athletes during the COVID-19 Pandemic. Front. Psychol. 2022, 13, 811499. [Google Scholar] [CrossRef]
- Mulcahey, M.K.; Gianakos, A.L.; Mercurio, A.; Rodeo, S.; Sutton, K.M. Sports Medicine Considerations during the COVID-19 Pandemic. Am. J. Sport. Med. 2021, 49, 512–521. [Google Scholar] [CrossRef]
- Fiorilli, G.; Buonsenso, A.; Davola, N.; Di Martino, G.; Baralla, F.; Boutious, S.; Centorbi, M.; Calcagno, G.; di Cagno, A. Stress Impact of COVID-19 Sports Restrictions on Disabled Athletes. Int. J. Environ. Res. Public Health 2021, 18, 2040. [Google Scholar] [CrossRef]
- Rahmati, M.; Shamsi, M.M.; Khoramipour, K.; Malakoutinia, F.; Woo, W.; Park, S.; Yon, D.K.; Lee, S.W.; Shin, J.I.; Smith, L. Baseline physical activity is associated with reduced mortality and disease outcomes in COVID-19: A systematic review and meta-analysis. Rev. Med. Virol. 2022, 32, e2349. [Google Scholar] [CrossRef]
- Rahmati, M.; Fatemi, R.; Yon, D.K.; Lee, S.W.; Koyanagi, A.; Il Shin, J.; Smith, L. The effect of adherence to high-quality dietary pattern on COVID-19 outcomes: A systematic review and meta-analysis. J. Med. Virol. 2023, 95, e28298. [Google Scholar] [CrossRef]
- Buonsenso, A.; Murri, A.; Centorbi, M.; Di Martino, G.; Calcagno, G.; di Cagno, A.; Fiorilli, G.; Iuliano, E. Psychological Wellbeing and Perceived Fatigue in Competitive Athletes after SARS-CoV-2 Infection 2 Years after Pandemic Start: Practical Indications. J. Funct. Morphol. Kinesiol. 2022, 8, 1. [Google Scholar] [CrossRef]
- Fikenzer, S.; Fikenzer, K.; Laufs, U.; Falz, R.; Pietrek, H.; Hepp, P. Impact of COVID-19 lockdown on endurance capacity of elite handball players. J. Sport. Med. Phys. Fit. 2021, 61, 977–982. [Google Scholar] [CrossRef]
- Toresdahl, B.G.; Asif, I.M. Coronavirus Disease 2019 (COVID-19): Considerations for the Competitive Athlete. Sport. Health 2020, 12, 221–224. [Google Scholar] [CrossRef]
- Wiśniowski, P.; Cieśliński, M.; Jarocka, M.; Kasiak, P.S.; Makaruk, B.; Pawliczek, W.; Wiecha, S. The Effect of Pressotherapy on Performance and Recovery in the Management of Delayed Onset Muscle Soreness: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 2077. [Google Scholar] [CrossRef]
- Colizzi, M.; Peghin, M.; De Martino, M.; Bontempo, G.; Gerussi, V.; Palese, A.; Isola, M.; Tascini, C.; Balestrieri, M. Mental health symptoms one year after acute COVID-19 infection: Prevalence and risk factors. Rev. Psiquiatr. Salud Ment. 2022, in press. [CrossRef] [PubMed]
- Pan, J.; Zhou, K.; Wang, J.; Zheng, Y.; Yu, D.; Kang, H.; Zhang, Y.; Peng, S.; Tung, T.H.; Shen, B. Quality of Life and Mental Health Status in Recovered COVID-19 Subjects at Two Years after Infection in Taizhou, China: A Longitudinal Cohort Study. Brain Sci. 2022, 12, 939. [Google Scholar] [CrossRef] [PubMed]
- Price, S.; Wiecha, S.; Cieśliński, I.; Śliż, D.; Kasiak, P.S.; Lach, J.; Gruba, G.; Kowalski, T.; Mamcarz, A. Differences between Treadmill and Cycle Ergometer Cardiopulmonary Exercise Testing Results in Triathletes and Their Association with Body Composition and Body Mass Index. Int. J. Environ. Res. Public Health 2022, 19, 3557. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Lin, J.; Ying, W.; Zheng, C.; Tao, L.; Ying, B.; Cheng, B.; Jin, S.; Hu, B. Correlation Study of Short-Term Mental Health in Patients Discharged After Coronavirus Disease 2019 (COVID-19) Infection without Comorbidities: A Prospective Study. Neuropsychiatr. Dis. Treat. 2020, 16, 2661–2667. [Google Scholar] [CrossRef] [PubMed]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and mental health complications post-COVID-19: Scoping review. J. Psychosom. Res. 2021, 147, 110525. [Google Scholar] [CrossRef]
- Bourmistrova, N.W.; Solomon, T.; Braude, P.; Strawbridge, R.; Carter, B. Long-term effects of COVID-19 on mental health: A systematic review. J. Affect. Disord. 2022, 299, 118–125. [Google Scholar] [CrossRef]
- Scheer, V.; Valero, D.; Villiger, E.; Rosemann, T.; Knechtle, B. The Impact of the COVID-19 Pandemic on Endurance and Ultra-Endurance Running. Medicina 2021, 57, 52. [Google Scholar] [CrossRef]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Fullagar, H.H.; Skorski, S.; Duffield, R.; Hammes, D.; Coutts, A.J.; Meyer, T. Sleep and athletic performance: The effects of sleep loss on exercise performance, and physiological and cognitive responses to exercise. Sport. Med. 2015, 45, 161–186. [Google Scholar] [CrossRef]
- Ulaszewska, K.; Jodczyk, A.M.; Dlugolecki, P.; Emerla, S.; Stanska, W.; Kasiak, P.S.; Gasior, J.S.; Parol, D.; Mamcarz, A.; Sliz, D. Factors Associated with Willingness to Receive a COVID-19 Vaccine in Adult Polish Population-A Cross-Sectional Survey. Vaccines 2022, 10, 1715. [Google Scholar] [CrossRef]
- Kaminsky, L.A.; Arena, R.; Myers, J. Reference Standards for Cardiorespiratory Fitness Measured With Cardiopulmonary Exercise Testing: Data From the Fitness Registry and the Importance of Exercise National Database. Mayo Clin. Proc. 2015, 90, 1515–1523. [Google Scholar] [CrossRef]
- Boraita, A.; Diaz-Gonzalez, L.; Valenzuela, P.L.; Heras, M.E.; Morales-Acuna, F.; Castillo-Garcia, A.; Lucia, M.J.; Suja, P.; Santos-Lozano, A.; Lucia, A. Normative Values for Sport-Specific Left Ventricular Dimensions and Exercise-Induced Cardiac Remodeling in Elite Spanish Male and Female Athletes. Sport. Med. Open. 2022, 8, 116. [Google Scholar] [CrossRef]
- Pluhar, E.; McCracken, C.; Griffith, K.L.; Christino, M.A.; Sugimoto, D.; Meehan, W.P., III. Team Sport Athletes May Be Less Likely To Suffer Anxiety or Depression than Individual Sport Athletes. J. Sport. Sci. Med. 2019, 18, 490–496. [Google Scholar]
- Gruba, G.; Kasiak, P.S.; Gebarowska, J.; Adamczyk, N.; Sikora, Z.; Jodczyk, A.M.; Mamcarz, A.; Sliz, D. PaLS Study of Sleep Deprivation and Mental Health Consequences of the COVID-19 Pandemic among University Students: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 9581. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Beaver, W.L.; Wasserman, K.; Whipp, B.J. A New Method for Detecting Anaerobic Threshold by Gas-Exchange. J. Appl. Physiol. 1986, 60, 2020–2027. [Google Scholar] [CrossRef]
- Sliz, D.; Wiecha, S.; Gasior, J.S.; Kasiak, P.S.; Ulaszewska, K.; Postula, M.; Malek, L.A.; Mamcarz, A. The Influence of Nutrition and Physical Activity on Exercise Performance after Mild COVID-19 Infection in Endurance Athletes-CESAR Study. Nutrients 2022, 14, 5381. [Google Scholar] [CrossRef]
- Sliz, D.; Wiecha, S.; Ulaszewska, K.; Gasior, J.S.; Lewandowski, M.; Kasiak, P.S.; Mamcarz, A. COVID-19 and athletes: Endurance sport and activity resilience study-CAESAR study. Front. Physiol. 2022, 13, 1078763. [Google Scholar] [CrossRef]
- Vitale, K.C.; Owens, R.; Hopkins, S.R.; Malhotra, A. Sleep Hygiene for Optimizing Recovery in Athletes: Review and Recommendations. Int. J. Sport. Med. 2019, 40, 535–543. [Google Scholar] [CrossRef]
- Mejri, M.A.; Yousfi, N.; Mhenni, T.; Tayech, A.; Hammouda, O.; Driss, T.; Chaouachi, A.; Souissi, N. Does one night of partial sleep deprivation affect the evening performance during intermittent exercise in Taekwondo players? J. Exerc. Rehabil. 2016, 12, 47–53. [Google Scholar] [CrossRef]
- Kamdar, B.B.; Kaplan, K.A.; Kezirian, E.J.; Dement, W.C. The impact of extended sleep on daytime alertness, vigilance, and mood. Sleep. Med. 2004, 5, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Doherty, R.; Madigan, S.; Warrington, G.; Ellis, J. Sleep and Nutrition Interactions: Implications for Athletes. Nutrients 2019, 11, 822. [Google Scholar] [CrossRef] [PubMed]
- Rebello, L.J.; Roberts, A.W.; Fenuta, A.M.; Cote, A.T.; Bodner, M.E. Sleep Quality and Sleep Behaviors in Varsity Athletes: A Pilot Study. Front. Sport. Act. Living 2022, 4, 906663. [Google Scholar] [CrossRef] [PubMed]
- Knufinke, M.; Nieuwenhuys, A.; Geurts, S.A.E.; Coenen, A.M.L.; Kompier, M.A.J. Self-reported sleep quantity, quality and sleep hygiene in elite athletes. J. Sleep Res. 2018, 27, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Roche, M.; Sainani, K.; Noordsy, D.; Fredericson, M. The Impacts of COVID-19 on Mental Health and Training in US Professional Endurance Athletes. Clin. J. Sport. Med. 2022, 32, 290–296. [Google Scholar] [CrossRef]
- Tamm, A.L.; Parm, Ü.; Aluoja, A.; Tomingas, T. Changes in the Mental Health Indicators and Training Opportunities for Estonian Elite Athletes Compared to the COVID-19 Isolation Period. Sport 2022, 10, 76. [Google Scholar] [CrossRef]
- Watson, A.; Haraldsdottir, K.; Biese, K.; Schwarz, A.; Hetzel, S.; Reardon, C.; Brooks, M.A.; Bell, D.R.; McGuine, T. Impact of COVID-19 on the physical activity, quality of life and mental health of adolescent athletes: A 2-year evaluation of over 17 000 athletes. Br. J. Sport. Med. 2022, 57, 359–363. [Google Scholar] [CrossRef]
- Wagemans, J.; Catteeuw, P.; Vandenhouten, J.; Jansen, J.; de Corte, X.; Ceusters, C.; Vissers, D. The Impact of COVID-19 on Physical Performance and Mental Health-A Retrospective Case Series of Belgian Male Professional Football Players. Front. Sport. Act. Living 2021, 3, 803130. [Google Scholar] [CrossRef]
- Daugherty, S.E.; Guo, Y.; Heath, K.; Dasmariñas, M.C.; Jubilo, K.G.; Samranvedhya, J.; Lipsitch, M.; Cohen, K. Risk of clinical sequelae after the acute phase of SARS-CoV-2 infection: Retrospective cohort study. BMJ 2021, 373, n1098. [Google Scholar] [CrossRef]
- Petek, B.J.; Moulson, N.; Baggish, A.L.; Kliethermes, S.A.; Patel, M.R.; Churchill, T.W.; Harmon, K.G.; Drezner, J.A.; Investigators, O. Prevalence and clinical implications of persistent or exertional cardiopulmonary symptoms following SARS-CoV-2 infection in 3597 collegiate athletes: A study from the Outcomes Registry for Cardiac Conditions in Athletes (ORCCA). Br. J. Sport. Med. 2022, 56, 913–918. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Cristanziano, V.D.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Liu, K.; Chen, Y.; Wu, D.; Lin, R.; Wang, Z.; Pan, L. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complement. Clin. Pract. 2020, 39, 101132. [Google Scholar] [CrossRef]
- Lindsay, R.K.; Wilson, J.J.; Trott, M.; Olanrewaju, O.; Tully, M.A.; López-Sánchez, G.F.; Shin, J.I.; Pizzol, D.; Allen, P.; Butler, L.T.; et al. What are the recommendations for returning athletes who have experienced long term COVID-19 symptoms? Ann. Med. 2021, 53, 1935–1944. [Google Scholar] [CrossRef]
- Kasiak, P.S.; Adamczyk, N.; Jodczyk, A.M.; Kapron, A.; Lisowska, A.; Mamcarz, A.; Sliz, D. COVID-19 Pandemic Consequences among Individuals with Eating Disorders on a Clinical Sample in Poland-A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 8484. [Google Scholar] [CrossRef]
- Selimbegović, L.; Dupuy, O.; Terache, J.; Blandin, Y.; Bosquet, L.; Chatard, A. Evaluative Threat Increases Effort Expenditure in a Cycling Exercise: An Exploratory Study. J. Sport. Exerc. Psychol. 2020, 42, 336–343. [Google Scholar] [CrossRef]
- Solberg, E.E.; Ingjer, F.; Holen, A.; Sundgot-Borgen, J.; Nilsson, S.; Holme, I. Stress reactivity to and recovery from a standardised exercise bout: A study of 31 runners practising relaxation techniques. Br. J. Sport. Med. 2000, 34, 268–272. [Google Scholar] [CrossRef]
- Nien, J.T.; Wu, C.H.; Yang, K.T.; Cho, Y.M.; Chu, C.H.; Chang, Y.K.; Zhou, C. Mindfulness Training Enhances Endurance Performance and Executive Functions in Athletes: An Event-Related Potential Study. Neural Plast. 2020, 2020, 8213710. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Pre-COVID-19 | Post-COVID-19 | p-Value |
|---|---|---|---|
| Weight (kg) | 76.6 (10.0) | 76.7 (10.9) | 0.951 |
| BMI (kg·m−2) | 24.0 (2.5) | 24.0 (2.7) | 0.931 |
| Lean mass (kg) | 63.4 (7.6) | 63.5 (8.0) | 0.774 |
| BF (%) | 17.1 (4.7) | 16.9 (5.1) | 0.604 |
| Fat mass (kg) | 13.3 (4.7) | 13.2 (5.2) | 0.848 |
| VO2AT (ml·kg·min−1) | 35.0 (6.5) | 32.4 (6.0) | <0.001 * |
| VO2ATa (ml·min−1) | 2650.0 (470.9) | 2446.1 (400.3) | <0.001 * |
| HRAT (beats·min−1) | 145.1 (10.9) | 141.1 (10.1) | 0.001 * |
| VEAT (l·min−1) | 70.8 (18.7) | 68.1 (14.7) | 0.090 |
| SAT (km·h−1) | 11.4 (1.4) | 11.1 (1.3) | 0.044 * |
| PAT (Watts) | 162.8 (25.9) | 154.8 (25.9) | 0.066 |
| fRAT (breaths·min−1) | 32.1 (9.0) | 32.1 (8.1) | 0.706 |
| LacAT (mmol·L−1) | 2.0 (0.9) | 2.1 (0.9) | 0.630 |
| VO2RCP (ml·kg·min−1) | 43.9 (7.4) | 40.5 (6.7) | <0.001 * |
| VO2RCPa (ml·min−1) | 3324.3 (512.9) | 3063.7 (440.1) | <0.001 * |
| HRRCP (beats·min−1) | 168.8 (9.2) | 165.1 (9.8) | <0.001 * |
| VERCP (l·min−1) | 106.8 (21.7) | 98.9 (18.3) | <0.001 * |
| SRCP (km·h−1) | 14.3 (1.9) | 13.8 (1.5) | <0.001 * |
| PRCP (Watts) | 245.2 (42.0) | 232.2 (39.7) | 0.061 |
| fRRCP (breaths·min−1) | 41.3 (8.7) | 40.1 (8.9) | 0.876 |
| LacRCP (mmol·L−1) | 4.9 (1.4) | 4.3 (1.1) | 0.013 * |
| VO2max (ml·kg·min−1) | 47.8 (8.0) | 45.0 (7.1) | <0.001 * |
| VO2maxa (ml·min−1) | 3623.5 (552.1) | 3406.0 (474.5) | <0.001 * |
| HRmax (beats·min−1) | 180.8 (10.1) | 179.8 (10.0) | 0.273 |
| VEmax (l·min−1) | 143.0 (26.9) | 138.50 (23.9) | 0.068 |
| Smax (km·h−1) | 16.6 (1.6) | 16.4 (1.7) | 0.264 |
| Pmax (Watts) | 310.0 (37.2) | 312.2 (49.1) | 0.811 |
| fRmax (breaths·min−1) | 58.9 (14.4) | 57.3 (11.0) | 0.959 |
| Lacmax (mmol·L−1) | 9.7 (2.3) | 9.6 (2.4) | 0.880 |
| Question | Answer Type | Lack of Answer | |||
|---|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| Sleep induction | No problem | Slightly delayed | Markedly delayed | Very delayed or did not sleep at all | 2 (4.1) |
| 22 (44,9) | 16 (32.7) | 7 (14.3) | 2 (4.1) | ||
| Awakenings during the night | No problem | Minor problem | Considerable problem | Serious problem or did not sleep at all | 2 (4.1) |
| 8 (16.3) 71.4 for HRRCP | 27 (55.1) 55.1 for HRRCP | 12 (24.5) 99.9 for HRRCP | 0 (0.0) | ||
| Final awakening | Not earlier | A little earlier | Markedly earlier | Much earlier or did not sleep at all | 3 (6.1) |
| 28 (57.1) | 15 (30.6) | 3 (6.1) | 0 (0.0) | ||
| Total sleep duration | Sufficient | Slightly insufficient | Markedly insufficient | Very insufficient or did not sleep at all | 2 (4.1) |
| 19 (38.8) 30.4 for VERCP 29.2 for fRRCP 24.9 for LacRCP | 25 (51.0) 18.5 for VERCP 20.4 for fRRCP 13.9 for LacRCP | 3 (6.1) 29.7 for VERCP 21.3 for fRRCP 18.0 for LacRCP | 0 (0.0) | ||
| Sleep quality | Satisfactory | Slightly unsatisfactory | Markedly unsatisfactory | Very unsatisfactory or did not sleep at all | 2 (4.1) |
| 22 (44.9) 27.2 for SRCP/PRCP 29.4 for VO2RCPa 29.2 for VO2RCP 29.1 for VERCP 27.6 for VO2max 27.5 for VO2maxa 27.3 for HRmax 25.9 for VEmax | 22 (44.9) 19.3 for SRCP/PRCP 17.6 for VO2RCPa 18.0 for VO2RCP 18.3 for VERCP 18.8 for VO2max 18.6 for VO2maxa 19.4 for HRmax 19.8 for VEmax | 3 (6.1) 35.3 for SRCP/PRCP 31.3 for VO2RCPa 28.7 for VO2RCP 28.7 for VERCP 35.3 for VO2maxa 38.0 for VO2maxa 33.8 for HRmax 40.7 for VEmax | 0 (0.0) | ||
| Well-being during the day | Normal | Slightly decreased | Markedly decreased | Very decreased | 2 (4.1) |
| 28 (57.1) 27.8 for SRCP/PRCP 28.3 for Smax/Pmax | 19 (38.8) 18.5 for SRCP/PRCP 17.6 for Smax/Pmax | 0 (0.0) | 0 (0.0) | ||
| Functioning capacity during the day | Normal | Slightly decreased | Markedly decreased | Very decreased | 3 (6.1) |
| 26 (53.1) | 19 (38.8) | 1 (2.0) | 0 (0.0) | ||
| Sleepiness during the day | None | Mild | Considerable | Intense | 2 (4.1) |
| 5 (10.2) | 28 (57.1) | 13 (26.5) | 1 (2.0) | ||
| What hour did you usually get out of bed in the morning | 7.1 (2.5) | 4 (8.2) | |||
| Hours of actual sleep per night | 6.8 (1.0) | ||||
| Hours spend in front of the screen of devices emitting blue light per day | 7.0 (2.9) | 3 (6.1) | |||
| Self-assessed impact of COVID-19 pandemic and imposed restrictions sleep (in -5/0/+5 scale) | 0.4 (1.3) | 2 (4.1) | |||
| Question | Answer Type | Lack of Answer | |||
|---|---|---|---|---|---|
| I Did Not Try This Method | I Used It in My Everyday Life, but Only to a Small Extent | I Used This Method Often, or It Was One of the Basic Methods to Cope with COVID-19 Induced Stress | I Used This Method Regularly | ||
| n (%) | n (%) | n (%) | n (%) | n (%) | |
| I wanted to return to work and duties as soon as possible to stop thinking about my illness | 24 (49.0) | 8 (16.3) | 4 (8.2) | 11 (22.4) | 2 (4.1) |
| I was concentrating very hard on the situation I found myself in | 27 (55.1) | 11 (22.4) | 0 (0.0) | 8 (16.3) | 3 (6.1) |
| I told myself „It can’t be true that I am infected with COVID-19” | 43 (87.8) | 4 (8.2) | 0 (0.0) | 1 (2.0) | 1 (2.0) |
| I used alcohol or other stimulants to improve my mood | 37 (75.5) | 7 (14.3) | 1 (2.0) | 1 (2.0) | 3 (6.1) |
| I gave up after trying to cope with the whole situation | 42 (85.7) | 1 (2.0) | 3 (6.1) | 0 (0.0) | 3 (6.1) |
| I was looking for support from family, friends and other people | 33 (67.3) | 8 (16.3) | 1 (2.0) | 4 (8.2) | 3 (6.1) |
| I undertook activities to improve my situation by expanding my knowledge about COVID-19 | 17 (34.7) 24.9 for lean mass | 13 (26.5) 15.4 for lean mass | 3 (6.1) 35.0 for lean mass | 13 (26.5) 27.2 for lean mass | 3 (6.1) |
| I was looking for positives in the situation I found myself in | 12 (24.5) | 7 (14.3) | 8 (16.3) | 19 (38.8) | 3 (6.1) |
| I criticized myself for not taking precautions enough, which resulted in COVID-19 infection | 40 (81.6) | 6 (12.2) | 0 (0.0) | 0 (0.0) | 3 (6.1) |
| I tried to joke about the COVID-19 infection | 18 (36.7) 27.7 for HRAT 25.6 for VO2RCP 27.3 for VERCP 24.9 for VO2max 26.3 for VO2maxa | 11 (22.4) 23.5 for HRAT 28.5 for VO2RCP 22.5for VERCP 28.6 for VO2max 28.0 for VO2maxa | 4 (8.2) 41.5 for HRAT 30.3 for VO2RCP 34.3 for VERCP 30.3 for VO2max 31.3 for VO2maxa | 13 (26.5) 15.2 for HRAT 14.3 for VO2RCP 15.8 for VERCP 15.1 for VO2max 13.5 for VO2maxa | 3 (6.1) |
| I quickly accepted the state I was in | 3 (6.1) | 7 (14.3) | 20 (40.8) | 16 (32.7) | 3 (6.1) |
| I expressed my negative emotions expressively by screaming loudly or arguing with others | 37 (75.5) 20.4 for VEAT | 7 (14.3) 34.4 for VEAT | 1 (2.0) 44.0 for VEAT | 1 (2.0) 42.0 for VEAT | 3 (6.1) |
| I tried to improve my mood through religious practices or meditation relaxation techniques | 35 (71.4) 22.3 for Smax/Pmax 23.0 for VO2max 13.7 for Lacmax | 6 (12.2) 35.8 for Smax/Pmax 34.2 for VO2max 21.7 for Lacmax | 0 (0.0) | 5 (10.2) 17.2 for Smax/Pmax 14.4 for VO2max 7.8 for Lacmax | 3 (6.1) |
| Self-assessed impact of COVID-19 pandemic and imposed restrictions mental health (in -5/0/+5 scale) | 0.6 (1.8) | 2 (4.1) | |||
| CPET Variable | Survey Question | p-Value |
|---|---|---|
| Part A. Sleep | ||
| HRRCP | Awakenings during the night | 0.028 * |
| VERCP | Total sleep duration | 0.013 * |
| fRRCP | Total sleep duration | 0.010 * |
| LacRCP | Total sleep duration | 0.013 * |
| SRCP/PRCP | Sleep quality | 0.046 * |
| VO2RCPa | Sleep quality | 0.011 * |
| VO2RCP | Sleep quality | 0.018 * |
| VERCP | Sleep quality | 0.027 * |
| VO2max | Sleep quality | 0.034 * |
| VO2maxa | Sleep quality | 0.019 * |
| HRmax | Sleep quality | 0.070 |
| VEmax | Sleep quality | 0.032 * |
| SRCP/PRCP | Well-being during the day | 0.023 * |
| Smax/Pmax | Well-being during the day | 0.007 * |
| Part B. Mental health | ||
| Lean mass | Undertaking activities to improve one’s situation | 0.042 * |
| HRAT | Joking about the COVID-19 infection | 0.042 * |
| VO2RCP | Joking about the COVID-19 infection | 0.029 * |
| VERCP | Joking about the COVID-19 infection | 0.041 * |
| VO2max | Joking about the COVID-19 infection | 0.047 * |
| VO2maxa | Joking about the COVID-19 infection | 0.014 * |
| VEAT | Expressing negative emotions expressively | 0.012 * |
| Smax/Pmax | Improving mood through religious practices or meditation relaxation techniques | 0.033 * |
| VO2max | Improving mood through religious practices or meditation relaxation techniques | 0.046 * |
| Lacmax | Improving mood through religious practices or meditation relaxation techniques | 0.045 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Śliż, D.; Wiecha, S.; Gąsior, J.S.; Kasiak, P.S.; Ulaszewska, K.; Lewandowski, M.; Barylski, M.; Mamcarz, A. Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes—CAESAR Study. J. Clin. Med. 2023, 12, 3002. https://doi.org/10.3390/jcm12083002
Śliż D, Wiecha S, Gąsior JS, Kasiak PS, Ulaszewska K, Lewandowski M, Barylski M, Mamcarz A. Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes—CAESAR Study. Journal of Clinical Medicine. 2023; 12(8):3002. https://doi.org/10.3390/jcm12083002
Chicago/Turabian StyleŚliż, Daniel, Szczepan Wiecha, Jakub S. Gąsior, Przemysław Seweryn Kasiak, Katarzyna Ulaszewska, Marcin Lewandowski, Marcin Barylski, and Artur Mamcarz. 2023. "Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes—CAESAR Study" Journal of Clinical Medicine 12, no. 8: 3002. https://doi.org/10.3390/jcm12083002
APA StyleŚliż, D., Wiecha, S., Gąsior, J. S., Kasiak, P. S., Ulaszewska, K., Lewandowski, M., Barylski, M., & Mamcarz, A. (2023). Impact of COVID-19 Infection on Cardiorespiratory Fitness, Sleep, and Psychology of Endurance Athletes—CAESAR Study. Journal of Clinical Medicine, 12(8), 3002. https://doi.org/10.3390/jcm12083002