1. Background
Nasopharyngeal carcinoma (NPC) can be divided into three pathological subtypes: keratinizing squamous, non-keratinizing (including differentiated and undifferentiated), and basaloid squamous. Undifferentiated non-keratinizing NPC is the most common pathological classification of NPC and is associated with Epstein–Barr virus (EBV) infection, accounting for 95% of NPC cases in southern China [
1,
2,
3].
EBV infects the host cells by expressing EBV-encoded transforming proteins and noncoding RNAs to alter multiple cellular pathways, promote cell proliferation, regulate the host microenvironment, and thereby, promote the clonal expansion of EBV-infected preinvasive nasopharyngeal epithelial cells [
4]. The detection of EBV-encoded small RNA (EBER) in the nuclei of tumor cells by in situ hybridization (ISH) was widely used in NPC, and NPC patients were classified as EBV (+) or EBV (−) based on these results.
In previous studies, EBER positivity was associated with both improved overall survival (OS) and disease-free survival (DFS) [
5]. EBV-negative NPC was correlated with worse overall survival (OS) [
6]. Since most NPC cases in the Chinese population were EBV-positive, there was a lack of research on EBV-negative patients in China, including a lack of larger-scale studies on the clinical characteristics of EBV-negative patients.
In order to further study the clinical characteristics of EBV-negative patients and investigate the correlation between EBV infection status and prognosis in this population, we combined data from four centers in China to analyze the general clinical characteristics of EBV-negative patients and compared outcomes with a matched EBV-positive NPC cohort after long-term follow-up.
2. Materials and Methods
NPC patients were classified as EBV (+) or EBV (−) based on the detection of EBV-encoded small RNA (EBER) in the nuclei of tumor cells by in situ hybridization (ISH). We collated all EBV-negative NPC patients from four hospitals (Hubei Cancer Hospital of Huazhong University of Science and Technology, Tongji Hospital of Huazhong University of Science and Technology, The Fifth Affiliated Hospital of Sun Yat-Sen University and Peking University Third Hospital) from 2013 to 2021.
Baseline/demographic and treatment-related characteristics were collected for each patient as given in their medical record. The outcomes analyzed herein were progression-free survival (PFS), which was defined as the time from cancer diagnosis to the time of tumor progression (local, regional, or distant) or death from any cause, and OS, which was defined as the time from cancer diagnosis to the time of death from any cause or was censored at the last follow-up.
To perform a comparative analysis between EBV-positive and EBV-negative patients, a propensity score matching analysis was used to reduce the effect of treatment selection bias and simulate the effects of randomization. EBV-positive NPC patients treated in the same time period as above were selected according to a 1:1.5 pairing with EBER-negative NPC patients based on several known prognostic factors, including the Eastern Cooperative Oncology Group performance status (ECOG PS), sex, age, stage, and type of therapy.
Descriptive statistics were used to compare the clinical characteristics of EBV-positive and EBV-negative NPC patients. The categorical variables (frequency and proportion) were analyzed by chi-square tests. Logistic regression analysis was applied to analyze the associations between the EBV tumor status and clinicopathologic factors. Kaplan–Meier analyses were performed to generate survival curves, and the log-rank test was applied for a statistical comparison thereof. Comparative risk factors for PFS and OS were identified by univariate and multivariate analyses using Cox regression models. All statistical analyses were conducted with SPSS version 23.0 (IBM Corp., Armonk, NY, USA). All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
3. Results
A total of 120 NPC patients with a known EBV status were included in this study, including 48 (40%) EBV-negative patients and 72 (60%) matched EBV-positive patients. The median follow-up period for the entire study population was 63.5 months (6–96 months).
The clinicopathological features of EBV-negative NPC patients are shown in
Table 1. The median age at diagnosis was 52 (range: 21–75) years, and 32 patients (66.7%) were male. Thirty-nine cases (81.3%) had the nonkeratinizing pathological subtype. The TNM stage distribution was as follows: Stage I (
n = 1), II (
n = 10), III (
n = 24), and IV nonmetastatic (
n = 13). Tumor stages were distributed as follows: T1 (
n = 9), T2 (
n = 15), T3 (
n = 16), and T4 (
n = 8). Nodal involvement was as follows: N0 (
n = 6), N1 (
n = 17), N2 (
n = 19), and N3 (
n = 6). Regarding treatment, almost all patients received concurrent chemoradiotherapy with or without induction chemotherapy or targeted therapy/immunotherapy. Seven (14.6%) of the 48 patients recurred, all of which were distant metastases (bone or lung), four (8.3%) of whom died.
Table 2 shows a comparison between EBV-negative NPC and the matched EBV-positive cohort. The former was more associated with the keratinizing subtype (18.8% vs. 1.4%,
p < 0.05). Compared to EBV-negative NPC patients, EBV-positive NPC patients were more likely to develop a local recurrence (9.7% vs. 0%,
p = 0.026). There was no statistical difference in mortality (8.3% vs. 4.2%,
p = 0.34) during follow-up. There were no significant differences between EBV-negative NPC and EBV-positive NPC in any other characteristics.
A logistic regression model was then constructed to evaluate the relationship between patient characteristics and EBV status. As shown in
Table 3, the NPC subtype (OR = 15.142, 95% CI: 1.741–131.695,
p = 0.014) was associated with higher odds of having an EBV-negative status. There was no significant association between EBV status and age, sex, life history (smoking, alcohol), or TNM stage.
As shown in
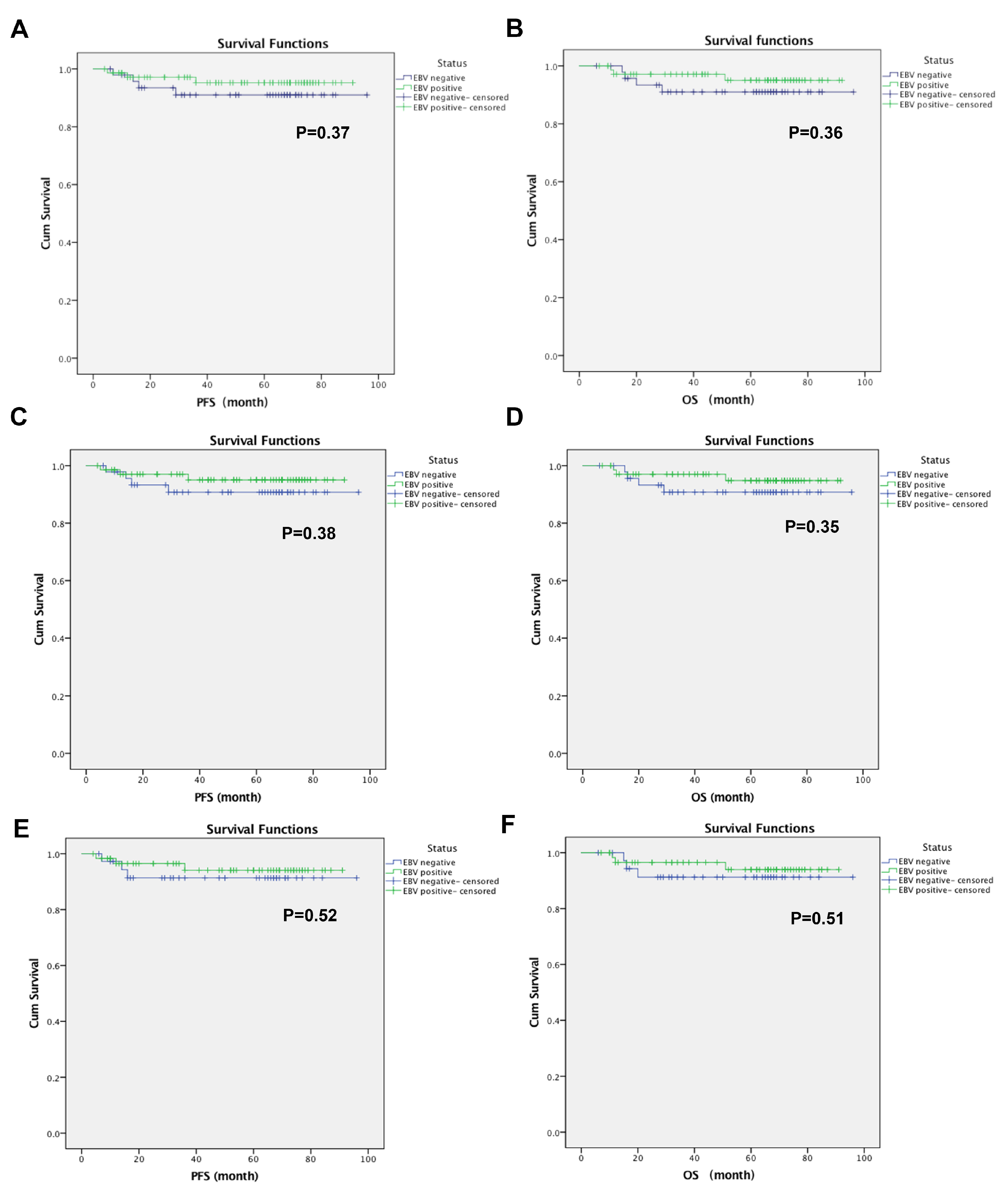
Table 1, the PFS and OS of the EBV-negative NPC patients had no significant correlation with age, sex, NPC subtype, social history (smoking, alcohol), and TNM stage by Cox regression models. Kaplan–Meier estimates suggested that EBV-positive NPC patients may have better survival than EBV-negative NPC patients, although the median PFS and median OS were not reached (
Figure 1). The 3-year PFS rate was 68.8% vs. 70.8% (EBV-negative vs. EBV-positive,
p = 0.06), and the 3-year OS rate was 70.8% vs. 76.4% (EBV-negative vs. EBV-positive,
p = 0.464), the 5-year PFS rate was 56.3% vs. 50% (EBV-negative vs. EBV-positive,
p = 0.451), and the 5-year OS rate was 56.3% vs. 58.3% (EBV-negative vs. EBV-positive,
p = 0.051), respectively. As shown in
Figure 1, there was no significant difference in the cumulative PFS between EBV-positive NPC and EBV-negative NPC (
p = 0.37). There was also no significant difference in the cumulative OS between EBV-positive NPC and EBV-negative NPC (
p = 0.36). In the subgroup analysis, there were no significant differences in PFS or OS between EBV-positive NPC and EBV-negative NPC in stage II-IV or III-IV NPC patients.
4. Discussion
Owing to its rarity in the Chinese population, little is known about the clinical characteristics of EBV-negative patients and the differences in prognosis between EBV-positive and EBV-negative NPCs. In this multicenter study, we found that the keratinizing NPC subtype was more common in EBV-negative NPC than in EBV-positive NPC and that EBV-positive NPC patients were more likely to develop a local recurrence (9.7% vs. 0%, p = 0.026).
Other reports of EBV-negative NPC in Chinese populations remain scarce. In one investigation, the mean OS of EBV-positive NPC patients was 57 months, and the mean DFS was 49 months; in the EBV-negative cohort, the mean OS was 43 months, and the mean DFS was 36 months [
5]. Another publication suggested no significant difference in survival between EBV-negative and EBV-positive NPC patients [
7]. Our study also did not discern significant differences in survival between EBV-negative and EBV-positive NPC patients but found that EBV-positive NPC patients had higher local recurrence rates. This seems to imply the need to strengthen local treatment in EBV-positive NPC patients and potentially systemic treatment in EBV-negative NPC patients.
Under these conditions, the treatment mode and efficacy of EBV-negative NPC were worth exploring. Induction chemotherapy followed by chemoradiotherapy has become the main treatment method and contributed to improvements in treatment outcomes [
8]. The five-year OS rate was 74–88% [
9,
10,
11]. However, the effect of radiotherapy alone was not inferior to concurrent chemoradiotherapy in patients with low-risk nasopharyngeal carcinoma [
12]. In an international multicenter retrospective study [
13], patients with NPC diagnosed between 2004 and 2017 in 36 hospitals in 11 countries were analyzed. The treatments that these patients received were divided into non-intensive treatment (NIT), including simple two-dimensional radiotherapy (RT), three-dimensional conformal radiotherapy (3D-CRT) or intensity-modulated radiation therapy (IMRT), and intensive treatment (IT), including concurrent chemoradiotherapy (CCRT) combined with induction or adjuvant chemotherapy. The five-year OS and DFS results of EBER (+) and EBER (−) after different intensities of treatment suggested that the OS of EBER (+) and EBER (−) NPC patients did not differ by treatment type. DFS was higher in EBER (+) NPC patients treated with IT than in EBER (−) NPC patients, whereas treatment type had no significant effect on DFS in EBER (−) NPC patients [
13]. This study also showed that advanced stages and age (>65 years) were important factors affecting the prognosis of patients with EBER (+) NPC, while age (>65 years) was an important factor affecting the prognosis of patients with EBER (−) NPC. However, due to insufficient sample sizes, we did not observe the same results.
In addition, we explored the association between patient characteristics and EBV status. The results showed that the NPC subtype was closely related to EBV status. The keratinizing NPC subtype was more common in EBV-negative NPC than in EBV-positive NPC. Compared with EBV-negative patients, most NPC patients had nonkeratinizing tissue, which was more common in EBER (+) tumors (91% vs. 70%) [
13]. Our study also confirmed this finding (98.6% vs. 81.3%). This may be related to EBV in the process of tumorigenesis; EBV infection was present in almost all undifferentiated NPCs and almost every NPC cell [
14].
To our knowledge, this is the first multicenter retrospective study to describe the clinical features of EBV-negative NPC patients in the Chinese population. However, there are several limitations to this work. First, the retrospective nature and small sample sizes limit statistical robustness. Second, the manner of EBV testing (assay or technique) may limit reproducibility. Third, propensity matching is not meant to substitute for randomized data. Lastly, these data are not meant to identify the optimal treatment regimen or sequencing of therapies for EBV-negative NPC.
5. Conclusions
In conclusion, owing to the rarity in the Chinese population, little is known about the clinical characteristics of EBV-negative patients and the differences in prognosis between EBV-positive and EBV-negative NPCs. In this multicenter study, we found that the keratinizing NPC subtype was more common in EBV-negative NPC than in EBV-positive NPC and that EBV-positive NPC patients were more likely to develop a local recurrence (9.7% vs. 0%, p = 0.026). This may imply the need to strengthen local treatment in EBV-positive NPC patients and potentially the same for systemic treatment in EBV-negative NPC patients. Whether EGFR-targeted therapy (cetuximab or nimotuzumab) or immunotherapy (PD-1/L1) has differential effects dependent on EBV status requires further investigation.
Author Contributions
Concept and design: G.H. and S.T.; Acquisition, analysis, or interpretation of data: Y.X., M.Y., Z.L., J.H., J.B., G.P., Y.L. (Ying Li), Y.L. (Yanping Li), H.H., V.V., S.T. and G.H.; Drafting of the manuscript: Y.X. and M.Y.; Critical revision of the manuscript for important intellectual content: Y.X., M.Y., Z.L., J.H., J.B., G.P., Y.L. (Ying Li), Y.L. (Yanping Li), H.H., V.V., S.T. and G.H.; Statistical analysis: G.H., Y.X., and J.B.; Administrative, technical, or material support: Z.L., J.H., S.T. and G.H.; Supervision: S.T. and G.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by Anti-Angiogenesis Targeted Tumor Research Funding of China Anti-Cancer Association (CACA), (No. 2021001049) and Wuhan 2022 Knowledge Innovation Project (No. 2022020801010512).
Institutional Review Board Statement
This retrospective study followed the principles of the Helsinki Declaration and was approved by the Ethics Committee of Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Hubei, China (Permit Number: LLHBCH2022YN-037). Approval was not required from other hospitals.
Informed Consent Statement
The need for informed consent in this retrospective study was waived by the ethics committee of Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Data Availability Statement
Data are available on request due to privacy/ethical restrictions. Data can be obtained by contacting the corresponding author’s email (
[email protected]) and the first author’s email (
[email protected]).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| NPC | nasopharyngeal carcinoma |
| EBV | Epstein–Barr virus |
| EBER | EBV-encoded small RNA |
| ISH | in situ hybridization |
| OS | overall survival |
| DFS | disease-free survival |
| PFS | progression-free survival |
| ECOG PS | Eastern Cooperative Oncology Group performance status |
| OR | odds ratio |
References
- Young, L.S.; Dawson, C.W. Epstein-Barr virus and nasopharyngeal carcinoma. Chin. J. Cancer 2014, 33, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Coghill, A.E.; Hildesheim, A. Epstein-Barr virus antibodies and the risk of associated malignancies: Review of the literature. Am. J. Epidemiol 2014, 180, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.L.; Chen, W.Q.; Xue, W.Q.; He, Y.Q.; Zheng, R.S.; Zeng, Y.X.; Jia, W.H. Global trends in incidence and mortality of nasopharyngeal carcinoma. Cancer Lett. 2016, 374, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef] [PubMed]
- Ooft, M.L.; van Ipenburg, J.A.; Braunius, W.W.; Zuur, C.I.; Koljenovic, S.; Willems, S.M. Prognostic role of tumor infiltrating lymphocytes in EBV positive and EBV negative nasopharyngeal carcinoma. Oral. Oncol. 2017, 71, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Ooft, M.L.; van Ipenburg, J.A.; Sanders, M.E.; Kranendonk, M.; Hofland, I.; de Bree, R.; Koljenovic, S.; Willems, S.M. Prognostic role of tumour-associated macrophages and regulatory T cells in EBV-positive and EBV-negative nasopharyngeal carcinoma. J. Clin. Pathol. 2018, 71, 267–274. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; Schroeder, L.; Ingarfield, K.; Diehl, S.; Werner, J.; Brenner, N.; Liu, Z.; Pawlita, M.; Pring, M.; Butt, J.; et al. Epstein-Barr virus and human papillomavirus serum antibodies define the viral status of nasopharyngeal carcinoma in a low endemic country. Int. J. Cancer 2020, 147, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.C.W.; Hui, E.P.; Lo, K.W.; Lam, W.K.J.; Johnson, D.; Li, L.; Tao, Q.; Chan, K.C.A.; To, K.F.; King, A.D.; et al. Nasopharyngeal carcinoma: An evolving paradigm. Nat. Rev. Clin. Oncol. 2021, 18, 679–695. [Google Scholar] [CrossRef] [PubMed]
- Du, T.; Xiao, J.; Qiu, Z.; Wu, K. The effectiveness of intensity-modulated radiation therapy versus 2D-RT for the treatment of nasopharyngeal carcinoma: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219611. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, L.; Hu, G.Q.; Zhang, N.; Zhu, X.D.; Yang, K.Y.; Jin, F.; Shi, M.; Chen, Y.P.; Hu, W.H.; et al. Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. N. Engl. J. Med. 2019, 381, 1124–1135. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, L.; Hu, G.Q.; Zhang, N.; Zhu, X.D.; Yang, K.Y.; Jin, F.; Shi, M.; Chen, Y.P.; Hu, W.H.; et al. Final Overall Survival Analysis of Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma: A Multicenter, Randomized Phase III Trial. J. Clin. Oncol. 2022, 40, 2420–2425. [Google Scholar] [CrossRef]
- Tang, L.L.; Guo, R.; Zhang, N.; Deng, B.; Chen, L.; Cheng, Z.B.; Huang, J.; Hu, W.H.; Huang, S.H.; Luo, W.J.; et al. Effect of Radiotherapy Alone vs Radiotherapy with Concurrent Chemoradiotherapy on Survival Without Disease Relapse in Patients with Low-risk Nasopharyngeal Carcinoma: A Randomized Clinical Trial. JAMA 2022, 328, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Bossi, P.; Trama, A.; Bernasconi, A.; Grisanti, S.; Mohamad, I.; Galiana, I.L.; Ozyar, E.; Franco, P.; Vecchio, S.; Bonomo, P.; et al. Nasopharyngeal cancer in non-endemic areas: Impact of treatment intensity within a large retrospective multicentre cohort. Eur. J. Cancer 2021, 159, 194–204. [Google Scholar] [CrossRef] [PubMed]
- Young, L.S.; Rickinson, A.B. Epstein-Barr virus: 40 years on. Nat. Rev. Cancer 2004, 4, 757–768. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).






 ,
, 


{kind=link}