

Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature

 ,
,  ,
,  , and
, and
Abstract
:1. Introduction
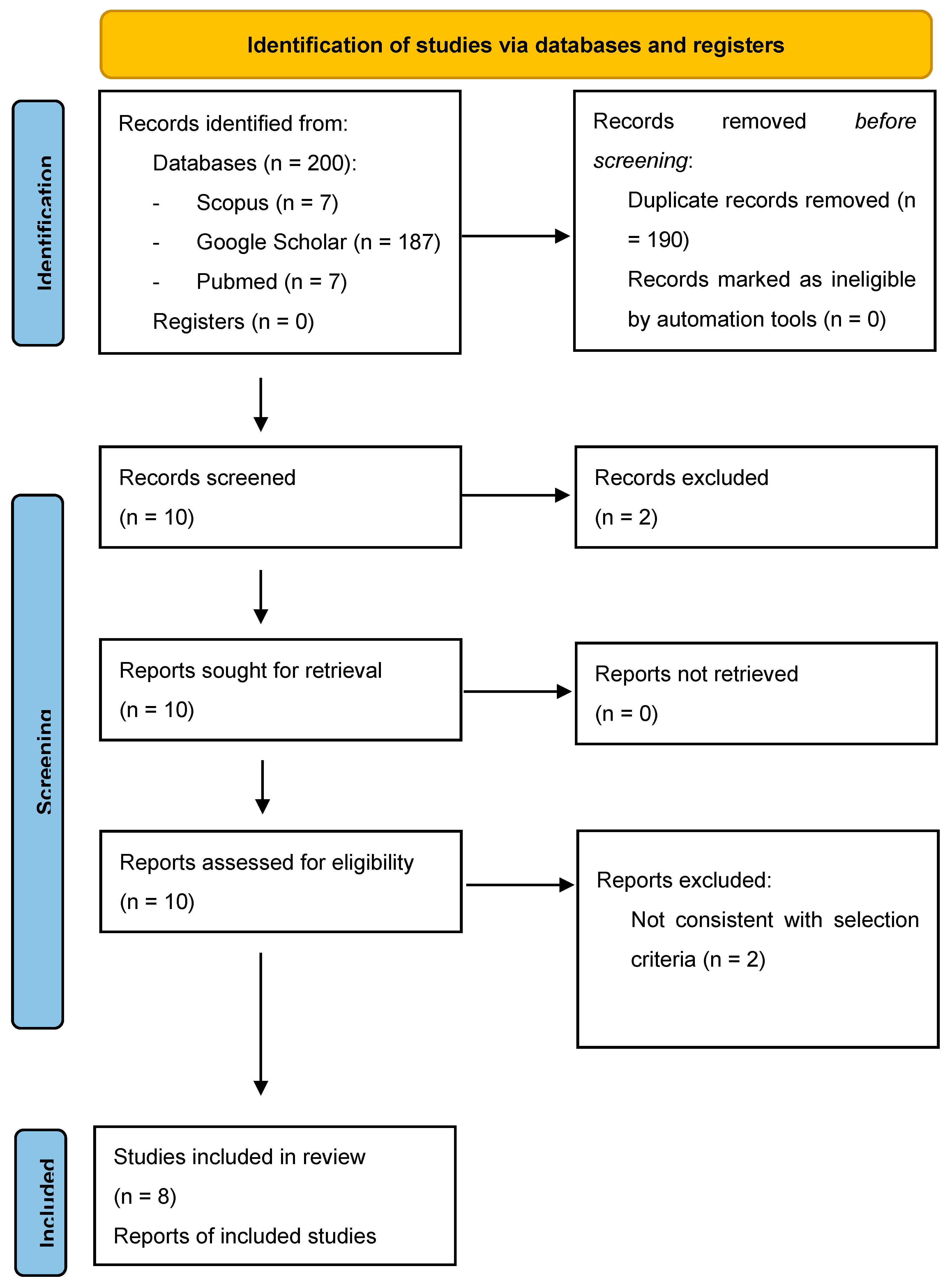
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Redline, R.W. Classification of placental lesions. Am. J. Obstet. Gynecol. 2015, 213 (Suppl. S4), S21–S28. [Google Scholar] [CrossRef]
- Carlucci, S.; Stabile, G.; Sorrentino, F.; Nappi, L.; Botta, G.; Menato, G.; Masturzo, B. The singular case of multiple chorangioma syndrome in an IVF pregnancy. Analysis of the case and review of literature. Placenta 2021, 103, 120–123. [Google Scholar] [CrossRef]
- Soper, J.T. Gestational Trophoblastic Disease: Current Evaluation and Management. Obstet. Gynecol. 2021, 137, 355–370, Erratum in: Obstet Gynecol. 2022, 139, 149. [Google Scholar] [CrossRef]
- Carlucci, S.; Stabile, G.; Catagini, S.; Borghi, C.; Scutiero, G.; Morano, D.; Greco, P. Fetal disseminated intravascular coagulopathy, hydrops and massive umbilical vein thrombosis consequence of a rare placental condition: Multifocal chorangiomatosis. J. Matern.-Fetal Neonatal Med. 2022, 35, 4009–4013. [Google Scholar] [CrossRef] [PubMed]
- Khong, T.Y. Chorangioma with trophoblastic proliferation. Virchows Arch. 2000, 436, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Gallot, D.; Sapin, V.; Beaufrère, A.-M.; Boda, C.; Laurichesse-Delmas, H.; Déchelotte, P.; Lémery, D. Récurrence de chorio-angiomes multiples: à propos d’un cas. [Recurrence of multiple chorio-angiomas: A case-report]. Gynecol. Obstet. Fertil. 2003, 31, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Faes, T.; Pecceu, A.; Van Calenbergh, S.; Moerman, P. Chorangiocarcinoma of the placenta: A case report and clinical review. Placenta 2012, 33, 658–661. [Google Scholar] [CrossRef] [PubMed]
- Guschmann, M.; Schulz-Bischof, K.; Vogel, M. Inzidentelles Chorangiokarzinom. Fallbericht, Immunhistochemie und Theorien zur möglichen Histogenese. [Incidental chorangiocarcinoma. Case report, immunohistochemistry and theories of possible histogenesis]. Pathologe 2003, 24, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Trask, C.; Lage, J.M.; Roberts, D.J. A second case of "chorangiocarcinoma" presenting in a term asymptomatic twin pregnancy: Choriocarcinoma in situ with associated villous vascular proliferation. Int. J. Gynecol. Pathol. 1994, 13, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Prospero International Prospective Register of Systematic Reviews. Available online: https://www.crd.york.ac.uk/prospero/ (accessed on 10 December 2022).
- Tufanaru, C. Chapter 3: Systematic reviews of effectiveness. In Joanna Briggs Institute Reviewer’s Manual; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Jauniaux, E.; Zucker, M.; Meuris, S.; Verhest, A.; Wilkin, P.; Hustin, J. Chorangiocarcinoma: An unusual tumour of the placenta. The missing link? Placenta 1988, 9, 607–613. [Google Scholar] [CrossRef]
- Ariel, I.; Boldes, R.; Weintraub, A.; Reinus, C.; Beller, U.; Arbel, R. Chorangiocarcinoma: A case report and review of the literature. Int. J. Gynecol. Pathol. 2009, 28, 267–271. [Google Scholar] [CrossRef]
- Huang, B.; Zhang, Y.-P.; Yuan, D.-F.; Yang, R.; Wang, C.; Wu, R.-F. Chorangiocarcinoma: A case report and clinical review. Int. J. Clin. Exp. Med. 2015, 8, 16798–16802. [Google Scholar] [PubMed]
- García-Molina, F.; Heredia-Oliva, L.; Castaño, M.D.; Andrada-Becerra, E. Corangiocarcinoma. A propósito de un caso. Rev. Española De Patol. 2016, 50, 229–233. [Google Scholar] [CrossRef]
- Sagar, N.; Tanwar, P.; Khurana, N.; Kashyap, P. Placental Chorangiocarcinoma: Case Report with Literature Review of a Rare Entity. Placental Chorangiocarcinoma: Case Report with Literature Review of a Rare Entity. Turk Patoloji Derg. 2022, 38, 292–296. [Google Scholar] [CrossRef]
- Benirschke, K.; Kaufmann, P.; Baergen, R.N. Pathology of the Human Placenta; Springer: New York, NY, USA, 2005. [Google Scholar]
- Ogino, S.; Redline, R.W. Villous capillary lesions of the placenta: Distinctions between chorangioma, chorangiomatosis, and chorangiosis. Hum Pathol. 2000, 31, 945–954. [Google Scholar] [CrossRef]
- Majlessi, H.F.; Wagner, K.M.; Brooks, J.J. Atypical cellular chorangioma of the placenta. Int. J. Gynecol. Pathol. 1983, 1, 403–408. [Google Scholar] [CrossRef]
- Mesia, A.F.; Mo, B.P.; Ylagan, L.R. Atypical cellular chorangioma. Arch. Pathol. Lab. Med. 1999, 123, 536–538. [Google Scholar] [CrossRef]
- Vellone, V.G.; Calamaro, P.; Vignale, C.; Novaro, G.; Penna, L.; Fulcheri, E. Atypical Cellular Chorangioma: A Potential Diagnostic Pitfall With Worrisome Aspects but a Favorable Prognosis. Int. J. Surg. Pathol. 2015, 23, 364–368. [Google Scholar] [CrossRef]
- Mao, T.-L.; Seidman, J.D.; Kurman, R.J.; Shih, I.-M. Cyclin E and p16 immunoreactivity in epithelioid trophoblastic tumor—An aid in differential diagnosis. Am. J. Surg. Pathol. 2006, 30, 1105–1110. [Google Scholar] [CrossRef]
- Benirschke, K.; Burton, G.J.; Baergen, R.N. Pathology of the Human Placenta, 6th ed.; Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Kurman, R.J.; Ellenson, L.H.; Ronnett, B.M. Blaustein’s Pathology of the Female Genital Tract, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Di Massa, G.; Stabile, G.; Romano, F.; Balduit, A.; Mangogna, A.; Belmonte, B.; Canu, P.; Bertucci, E.; Ricci, G.; Salviato, T. CD133 Expression in Placenta Chorioangioma Presenting as a Giant Asymptomatic Mass. Medicina 2021, 57, 162. [Google Scholar] [CrossRef] [PubMed]
- Mao, T.L.; Kurman, R.J.; Jeng, Y.M.; Huang, W.; Shih, I.M. HSD3B1 as a novel trophoblast-associated marker that assists in the differential diagnosis of trophoblastic tumors and tumorlike lesions. Am. J. Surg. Pathol. 2008, 32, 236–242. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Study Type | D1 | D2 | D3 | D4 | D5 | D6 | D7 | D8 |
|---|---|---|---|---|---|---|---|---|---|
| Jauniaux et al. (1988) [13] Placenta | Case report |  | | | | | | | |
| Trask C. et al. (1994) [9] Int J Gynecol Pathol | Case report | | | | | | | Not applicable | |
| Ariel I. et al. (2009) [14] Int J Gynecol Pathol | Case report | | Not applicable | | | | | | |
| Guschmann M. et al. (2003) [8] Pathologe | Case report | | Unclear | | | | | | Unclear |
| Faes T. et al. (2012) [7] Placenta | Case report | | | | | | | | |
| Huang B. et al. (2015) [15] Int J Clin Exp Med | Case report | | Not applicable | | | | | | |
| Garcìa-Molina F. et al. (2016) [16] Patalogìa | Case report | | | | | | | Not applicable | Unclear |
| Sagar N. et al. (2021) [17] Turk Patoloji Derg | Case report | | | | | | | Not applicable | Unclear |
| Reference | Maternal Age | GA at Delivery (Weeks), Parity Singleton/Twin | Placental Weight (g) | Ultrasound Features | Macroscopic Examination Tumor Size | Microscopic Examination | Immunostaining | Maternal b-HCG (Baseline, Follow-Ups) | Fetal Assessment | Follow-Up | Maternal Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Jauniaux E. et al., 1988 [13] | 35 | 35 w, 3003 CS for shoulder presentation and vaginal bleeding Singleton | 600 | Not determined | Well-demarcated round nodule, multilobulated, limited by a white pseudocapsule 1.5 × 1.5 cm | Well-differentiated capillary pattern supported by chorionic stroma cells and fibrous tissue with an outer layer of syncytiotrophoblast and cytotrophoblast with nuclear atypia | -PAS-positive fibrin deposition in the area close to the tumor -hCG strongly positive in the trophoblastic layer and pseudocapsule -hPL positive to syncytium of the villi | -Not determined -Below detection 6 months after delivery | Normal | 9 months | Normal |
| Trask C. et al., 1994 [9] | 36 | 36 w, 1011 Spontaneous labor and delivery Twin BC/BA | 250 (presenting twin placenta) | Not determined | Firm lesion similar to an infarct 3 × 2.5 cm | Stem villi with pronounced proliferation of villous stromal vessels, circumferential proliferation of malignant trophoblast protruding in the intervillous space (nuclear atypia, high mitotic rate) | -keratin (E1/AE3, Boehringer-Mannheim, Indianapolis, IN, U.S.A.) reactivity in the abnormal trophoblast -hCG positive -hPL weak and focal at the malignant trophoblast, strong in the normal syncytiotrophoblast | -Not determined -698 mIU/mL 7 days after delivery -Below detection 29 days and 3 months after delivery | Normal | 7 days 29 days 3 months | Normal |
| Ariel I. et al., 2009 [14] | 23 | 37 w, 0000 Spontaneous labor and CS for condylomata Singleton | 678 | Thick lesion of 5–6 cm with hyperechogenic and hypoechogenic areas without hypervascularization | Well-demarcated mass with alternating red and yellowish tissue on cut sections 8 × 5 cm | Malignant epithelial tumor with central necrosis forming a complex branching structure within a chorangioma (mitotic rate >90%, pleomorphic nuclei) | -Panytokeratin positive -b-HCG positive -hsd3b1 focally positive -hPL weakly positive | -Consistent with GA at baseline -Below detection 1 month after delivery | Normal | 1 month after delivery | Normal |
| Guschmann M. et al., 2003 [8] | 31 | 34 w, 1001 CS for fetal distress and FGR Singleton | 496 | Not determined | Nodule with grey-yellow foci 3 cm | Villi surrounded by syncytiotrophoblast atypia and chorangiosis with adjacent areas of necrosis (nuclear atypia, mitoses) | -bHCG at the syncytiotrophoblast -hPL weak and prevalent at the intermediate trophoblast -VEGF, bFGF, Ang-1,2, PDGF expression at the trophoblast similar to normal villi | -Consistent with GA at baseline -Not determined | FGR | Not determined | Normal |
| Faes T. et al., 2012 [7] | 36 | 40 w, 2002 Spontaneous labor and delivery Singleton | 812 | Nodule of 8 × 7 cm with hyperechogenic and hypoechogenic areas with hypervascularisation at the border. Supplying artery PI 0.87, RI 0.58, PSF 39.34 cm/s. | Firm reddish-brown tumor with a lobulated appearance on section with multiple small white nodules 8 × 7 cm | Dilated angiomatous vessels filled up with neoplastic cell proliferation and separated by fibrous septa containing numerous capillary-type blood vessels; extensive central necrosis with dystrophic calcification (nuclei pleomorphism, multinucleation, high mitotic rate). | -AE1/AE3 cytoplasmic positivity -p63 nuclear staining -inhibin-alfa focal positivity -b-HCG strong positivity at the margins -Ki-67 high proliferation index | -Not determined -Below detection 1 month after delivery | Normal | 1 month after delivery | Normal |
| Huang B. et al., 2015 [15] | 27 | 39 w, 0000 Spontaneous labor and CS for suspicious of Macrosomia Singleton | 500 | Not determined | Firm grayish yellow-white mass with the consistency of an infarct. 5 × 4.5 cm | Abnormal trophoblastic proliferation in conjunction with a chorangioma in the stroma of chorionic villi. Cells forming solid masses with massive central coagulation necrosis surrounded by three to six layers of epithelial tumor cells (high proliferation index, mitoses) | -strong intensity for hCG, PLAP, CK, CD31 (+) and CD34 (+) in the lesion. -Ki67 high proliferation index | -Consistent with GA at baseline -Increase at 6 weeks after delivery -Below detection after 3 cycles of chemotherapy | Normal | -6 weeks after delivery -3 months after delivery | Lung metastasis at 3 months after delivery |
| Garcìa-Molina F. et al. (2016) Patalogìa [16] | 36 | 41 3013 Elective C section Twin BC/BA | 587 (fused bichorial placenta) | Not determined | Small irregular whitish area | Abnormal trophoblastic proliferation, with cellular atypia and arborescent proliferation through stromal cells and abundant vessels (cellular mitoses, coagulation necrosis, pleomorfism) | -Positivity for bHCG, CK 8–18, PAN CK -vascular proliferation vimentina and CD-34 (+) -High Ki-67 at the area of trophoblastic proliferation | -Not determined -negative at one month after delivery | Normal | 1 month after delivery | Normal |
| Sagar N. et al., 2021 [17] | 29 | 30 w, 1021 pProm, Chorionamnionitis CS Singleton | Not determined | Small hypoechoic lesion in relation to the uterine fundus with maintained uterine contour | Grey-white nodule, solid-cystic at cut section with friable areas 5.5 × 4.5 × 3 cm | Multiple well-circumscribed cellular nests with central necrosis dispersed in a chorangiomatous stroma (mitoses, apoptotic bodies, multinucleation) | -AE1/AE3, PathnSitu, U.S.A. cytokeratin positivity -b-HCH positivity -PLAP and Ki-67 | -Consistent with GA at baseline -Not determined | Normal | Not determined | Normal |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stabile, G.; Scalia, M.S.; Stampalija, T.; Bruno, M.; Laganà, A.S.; Sartore, A.; Mangogna, A.; Carlucci, S. Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. J. Clin. Med. 2023, 12, 3065. https://doi.org/10.3390/jcm12093065
Stabile G, Scalia MS, Stampalija T, Bruno M, Laganà AS, Sartore A, Mangogna A, Carlucci S. Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. Journal of Clinical Medicine. 2023; 12(9):3065. https://doi.org/10.3390/jcm12093065
Chicago/Turabian StyleStabile, Guglielmo, Maria Sole Scalia, Tamara Stampalija, Matteo Bruno, Antonio Simone Laganà, Andrea Sartore, Alessandro Mangogna, and Stefania Carlucci. 2023. "Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature" Journal of Clinical Medicine 12, no. 9: 3065. https://doi.org/10.3390/jcm12093065
APA StyleStabile, G., Scalia, M. S., Stampalija, T., Bruno, M., Laganà, A. S., Sartore, A., Mangogna, A., & Carlucci, S. (2023). Placental Chorangiocarcinoma a Specific Histological Pattern of Uncertain Incidence and Clinical Impact: Systematic Review of the Literature. Journal of Clinical Medicine, 12(9), 3065. https://doi.org/10.3390/jcm12093065