
Sinonasal Malignancies Involving the Frontal Sinus: A Mono-Institutional Experience of 84 Cases and Systematic Literature Review

 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
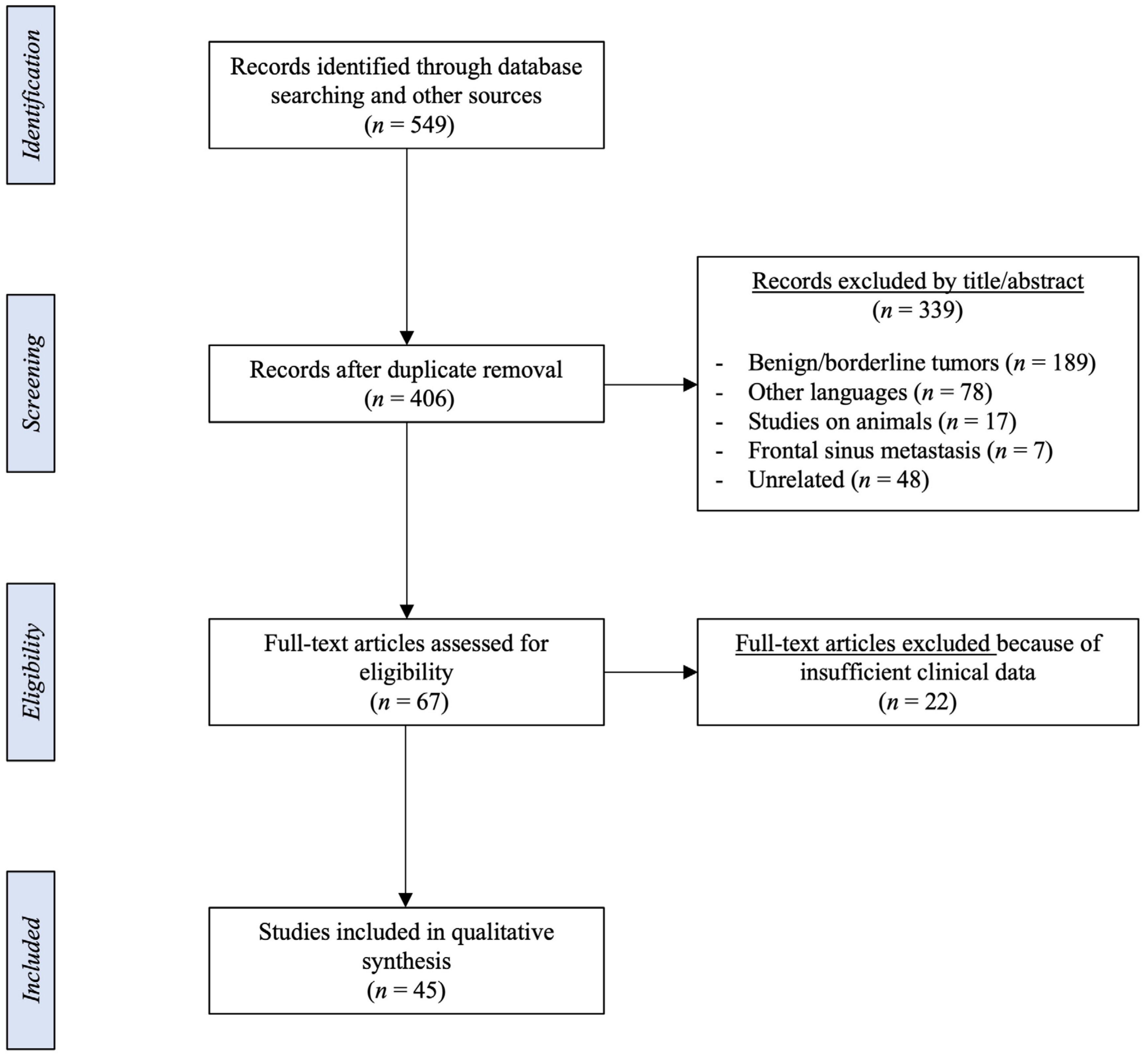
2.1. Systematic Literature Review
2.2. Mono-Institutional Cohort
2.3. Statistical Analysis
3. Results
3.1. Systematic Literature Review

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | N° of Cases | Age | Gender | Origin | Histology | T | N | M | Management | Complications | Follow-Up (Months) | Status | Recurrence (Where) | Months from Treatment | Recurrence Treatment |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abrahao [13] | 2000 | 1 | 59 | F | FS | ADC | 4b | NA | NA | CFR + CHRT | Cranioplasty infection | 10 | AWD | Nasal cavity | 10 | NA |
| Rodrigo [14] | 2000 | 1 | 53 | M | FS | Malignant fibrous histiocytoma | NA | NA | NA | CFR | - | 68 | AWD | FS + lung | 60 | CHT |
| Gallia [15] | 2005 | 1 | 44 | M | FS | Synovial sarcoma | 4b | 0 | 0 | CFR + CHRT | - | 2 | NED | - | - | - |
| Yoshida [16] | 2006 | 1 | 74 | M | FS | SCC | 4b | 0 | 0 | CFR + RT | - | 20 | DOD | FS + lung | 3 | CFR + CHRT |
| Nemet [17] | 2006 | 1 | 84 | M | FS | B-cell lymphoma | IE | - | - | RT | - | 9 | DOD | - | - | - |
| Ogunleye [18] | 2006 | 1 | 31 | F | FS | MPNST | 4b | 0 | 0 | CFR + RT | - | 24 | NED | - | - | - |
| Gerlinger [19] | 2007 | 1 | 60 | M | FS | SNUC | 4a | 0 | 0 | CFR + RT | - | 12 | NED | - | - | - |
| Chain [20] | 2007 | 1 | 55 | M | FS | B-cell lymphoma | IIE | - | - | CHRT | - | 18 | NED | - | - | - |
| Chu [21] | 2008 | 1 | 61 | M | FS | SNEC | 4a | 0 | 0 | ER | - | 14 | NED | - | - | - |
| Ichinose [22] | 2009 | 1 | 66 | M | FS | SCC | 4b | 0 | 0 | CFR | - | 48 | NED | - | - | - |
| Gray [23] | 2009 | 1 | 17 | M | ES | Ewing sarcoma | 4a | 0 | 0 | IMPT + CHT | Frontal mucocele | 7 | NED | - | - | - |
| Lazzeri [24] | 2010 | 1 | 78 | M | ES | MM | 4b | NA | NA | ER + RT | - | 1 | DOD | - | - | - |
| Ito [25] | 2010 | 2 | 43 (mean) | F | FS | Osteosarcoma | 4b | X | X | Best supportive care CER | - | 3 7 | DOD DOD | - | - | - |
| Kim [26] | 2011 | 3 | 69 (mean) | M | FS | SCC on IP | 4b 4a 4a | 0 2b 0 | 0 | CFR + RT RT CHT/RT | - | 3 5 23 | lost DOD DOD | - | - | - |
| Madana [27] | 2011 | 1 | 48 | F | FS | SCC | 4a | 0 | 0 | CFR + RT | - | 12 | NED | - | - | - |
| Wadhera [4] | 2011 | 1 | 53 | M | FS | ADC | 4b | 0 | 0 | CHRT | - | 12 | AWD | - | - | - |
| Bercin [28] | 2011 | 1 | 47 | F | ES | Fibrosarcoma | 4b | 0 | 0 | CER | - | 24 | NED | - | - | - |
| Soyka [29] | 2011 | 1 | 43 | F | FS | Malignant solitary fibrous tumor | 4a/4b | NA | NA | CER + RT | Osteomyelitis | 36 | NED | - | - | - |
| Kim [30] | 2011 | 1 | 42 | M | FS | B-cell lymphoma | IVE | - | - | CHT | - | 50 | NED | - | - | - |
| Hosokawa [31] | 2012 | 1 | 71 | M | FS | SCC | 4b | 0 | 0 | CER | - | 40 | NED | - | - | - |
| Fukumitsu [32] | 2012 | 1 | 71 | M | FS | SCC | 4b | X | X | IMPT | Brain necrosis | 22 | DOC | - | - | - |
| Peregud-Pogorzelski [33] | 2012 | 1 | 11 | F | FS | Rhabdomyosarcoma | 4a/4b | 1 | 0 | iCHT + ER + CHRT | Mycotic sinusitis | 1 | NED | - | - | - |
| Zhang [34] | 2014 | 1 | 66 | M | FS | SCC | 4b | 0 | 0 | CFR + RT | - | 6 | NED | - | - | - |
| Lee [35] | 2014 | 1 | 74 | M | ES | MPNST | 4a | 0 | 0 | CFR | Skin flap necrosis | 6 | NED | - | - | - |
| Jankowski [36] | 2014 | 2 | 39.5 (mean) | M | ES | ONB | B C | 0 N1 | 0 | ER CHT + CFR + RT | - | 6 24 | NED NED | - | - | - |
| Verim [37] | 2014 | 1 | 69 | F | FS | Plasmacytoma | 4b | 0 | 0 | CFR + RT | - | 18 | NED | - | - | - |
| Tomovic [38] | 2014 | 1 | 21 | F | FS | Angiosarcoma | 4b | 1 | 1 | CHRT | - | 12 | NED | - | - | - |
| Khan [39] | 2015 | 1 | 69 | M | FS | B-cell lymphoma | IE | - | - | CFR + CHT | - | 36 | NED | - | - | - |
| Kieliszak [40] | 2015 | 1 | 63 | M | FS | Granulocytic sarcoma | 4a | 0 | 0 | CFR + CHT | Neutropenic fever | 1 | DOC | - | - | - |
| Kuan [41] | 2017 | 1 | 75 | M | FS | SCC on IP | 4a | 0 | 0 | CHT + ER | - | 12 | NED | - | - | - |
| Minato [42] | 2017 | 1 | 66 | F | FS | NUT carcinoma | 4b | 0 | 0 | CHT + RT | 13 | DOD | Bone + liver | NA | CHT | |
| Cannon [43] | 2017 | 3 | 69 (mean) | F | FS | Biphenotypic sarcoma | 4a 4b 4b | 0 | 0 | ERTC CFR + CER Awaiting surgery | - | 17 NA NA | NED NED AWD | ACF - - | 17 - - | Revision ERTC - - |
| Sienna [44] | 2018 | 1 | 80 | M | ES | SNUC | 4a | 2 | 0 | iCHT + CHRT | - | 17 | DOD | FS + brain | 4 | CHRT |
| Kim [45] | 2018 | 1 | 63 | M | FS | ITAC | 4a | 0 | 0 | CFR | - | 6 | NED | - | - | - |
| Nagafuji [46] | 2018 | 1 | 67 | M | FS | B-cell lymphoma | IIE | - | - | CHT | - | 12 | NED | - | - | - |
| Biswas [47] | 2019 | 1 | 21 | F | FS | ALCL | IE | - | - | CHRT | Cutaneous nasal fistula | 40 | NED | - | - | - |
| Tirelli [48] | 2019 | 1 | 45 | M | FS | ACC | 4a | 0 | 0 | CFR | Diplopia | 24 | NED | - | - | - |
| Alvi [49] | 2019 | 1 | 44 | F | FS | Biphenotypic sarcoma | 4a | 0 | 0 | CFR + RT | - | 360 | NED | FS + ES | 350 | CFR |
| Knudson [50] | 2019 | 1 | 11 | M | FS | B-cell lymphoma | IIE | - | - | CHT | Brain herniation | 12 | NED | - | - | - |
| Lee [51] | 2020 | 1 | 53 | M | FS | SCC | 4a | 0 | 0 | CER + CHRT | - | 36 | NED | - | - | - |
| Esteves Costa [52] | 2020 | 1 | 12 | F | FS | Ewing sarcoma | 4a | 0 | 0 | iCHT + RT | - | 17 | NED | - | - | - |
| Baudoin [53] | 2021 | 1 | 47 | M | MS | ACC | 4a | 0 | 0 | CFR + RT | - | NA | NED | FS | NA | CFR |
| Andron [54] | 2021 | 1 | 75 | F | FS | Plasmacytoma | 4a | 0 | 0 | CFR + RT | - | 22 | NED | - | - | - |
| Yoon [55] | 2021 | 1 | 46 | M | FS | B-cell lymphoma | IIE | - | - | CHT | Sepsis | 4 | DOC | - | - | - |
| Kieu [56] | 2021 | 1 | 65 | F | FS | MM | 4b | 0 | 0 | CFR + RT + immunotherapy | - | 3 | NED | - | - | - |
3.2. Mono-Institutional Cohort
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhojwani, A.; Unsal, A.; Dubal, P.M.; Echanique, K.A.; Baredes, S.; Liu, J.K.; Eloy, J.A. Frontal Sinus Malignancies: A Population-Based Analysis of Incidence and Survival. Otolaryngol. Neck Surg. 2016, 154, 735–741. [Google Scholar] [CrossRef]
- Gourin, C.G.; Terris, D.J. Frontal Sinus Malignancies. In The Frontal Sinus; Kountakis, S.E., Senior, B.A., Draf, W., Eds.; Springer: Berlin/Heidelberg, Germany, 2005. [Google Scholar]
- Dutta, R.; Dubal, P.M.; Svider, P.F.; Liu, J.K.; Baredes, S.; Eloy, J.A. Sinonasal malignancies: A population-based analysis of site-specific incidence and survival. Laryngoscope 2015, 125, 2491–2497. [Google Scholar] [CrossRef]
- Wadhera, R.; Gulati, S.P.; Garg, A.; Ghai, A.; Kumar, S. Primary Adenocarcinoma of the Frontal Sinus. Ear. Nose Throat J. 2011, 90, E23–E25. [Google Scholar] [CrossRef] [Green Version]
- Castelnuovo, P.; Turri-Zanoni, M.; Battaglia, P.; Antognoni, P.; Bossi, P.; Locatelli, D. Sinonasal Malignancies of Anterior Skull Base: Histology-Driven Treatment Strategies. Otolaryngol. Clin. N. Am. 2016, 49, 183–200. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ferrari, M.; Mattavelli, D.; Tomasoni, M.; Raffetti, E.; Bossi, P.; Schreiber, A.; Orlandi, E.; Taboni, S.; Rampinelli, V.; Gualtieri, T.; et al. The MUSES: A prognostic study on 1360 patients with sinonasal cancer undergoing endoscopic surgery-based treatment. Eur. J. Cancer 2022, 171, 161–182. [Google Scholar] [CrossRef]
- Arosio, A.D.; Bernasconi, D.P.; Valsecchi, M.G.; Pacifico, C.; Battaglia, P.; Bignami, M.; Ferrari, M.; Mattavelli, D.; Rampinelli, V.; Tomasoni, M.; et al. Patterns of recurrences in sinonasal cancers undergoing an endoscopic surgery-based treatment: Results of the MUSES on 940 patients. Oral Oncol. 2022, 134, 106123. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Bossi, P.; Orlandi, E.; Resteghini, C.; Vischioni, B.; Nicolai, P.; Castelnuovo, P.; Gambazza, S.; Locati, L.; Turri-Zanoni, M.; Ferrari, M.; et al. The SINTART 2 Study. A Phase II Nonrandomized Controlled Trial of Induction Chemotherapy, Photon-, Proton- and Carbon Ion-Based Radiotherapy Integration in Patients with Locally Advanced Unresectable Sinonasal Tumors. Eur. J. Cancer 2023, in press. [Google Scholar] [CrossRef]
- Brierley, T.N.M. Classification of Malignant Tumours, 8th ed.; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA.
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours; International Agency for Research on Cancer: Lion, France, 2017; Available online: https://books.google.it/books?id=EDo5MQAACAAJ (accessed on 10 January 2023).
- Abrahão, M.; Gonçalves, A.P.V.; Yamashita, R.; Dedivitis, R.A.; Santos, R.O.; Nascimento, L.A.; Mudo, M.L.; Ferraz, F.A.P.; Cervantes, O. Frontal sinus adenocarcinoma. Sao Paulo Med. J. 2000, 118, 118–120. [Google Scholar] [CrossRef] [Green Version]
- Rodrigo, J.P.; Fernáandez, J.A.; Suárez, C.; Gómez, J.; Llorente, J.L.; Herrero, A. Malignant Fibrous Histiocytoma of the Nasal Cavity and Paranasal Sinuses. Am. J. Rhinol. 2000, 14, 427–432. [Google Scholar] [CrossRef]
- Gallia, G.L.; Sciubba, D.M.; Hann, C.L.; Raman, S.P.; Westra, W.H.; Tufaro, A.P.; Olivi, A. Synovial sarcoma of the frontal sinus: Case report. J. Neurosurg. 2005, 103, 1077–1080. [Google Scholar] [CrossRef]
- Yoshida, N.; Kanekura, T.; Hashiguchi, T.; Nagayama, T.; Hamada, H.; Kanzaki, T. Primary squamous cell carcinoma of the frontal sinus. J. Dermatol. 2006, 33, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Nemet, A.Y.; Deckel, Y.; Kourt, G. Orbital Invasion of Frontal Sinus Lymphoma. Orbit 2006, 25, 149–151. [Google Scholar] [CrossRef] [PubMed]
- Ogunleye, A.; Ijaduola, G.; Malomo, A.; Oluwatosin, O.; Oluwasola, A.; Shokunbi, W.; Akinyemi, O.; Oluwasola, A.; Akang, E. Malignant schwannoma of the nasal cavity and paranasal sinuses in a Nigerian. Afr. J. Med. Med Sci. 2006, 35, 489–493. [Google Scholar]
- Gerlinger, I.; Gőbel, G.; Tóth, E.; Szanyi, I.; Weninger, C. Primary carcinoma of the frontal sinus: A case report and a review of literature. Eur. Arch. Otorhinolaryngol. 2008, 265, 593–597. [Google Scholar] [CrossRef]
- Chain, J.R.; Kingdom, T.T. Non-Hodgkin’s lymphoma of the frontal sinus presenting as osteomyelitis. Am. J. Otolaryngol. 2007, 28, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.W.; Karakla, D.W.; Silverberg, M.; Han, J.K. Primary Carcinoid Tumor of the Frontal Sinus: A Case Report. Ear. Nose Throat J. 2010, 89, E13–E16. [Google Scholar] [CrossRef] [Green Version]
- Ichinose, T.; Goto, T.; Motomura, H.; Terakawa, Y.; Ohata, K. Primary Squamous Cell Carcinoma of the Frontal Sinus Treated with En Bloc Resection. Neurol. Med. Chir. 2009, 49, 481–483. [Google Scholar] [CrossRef] [Green Version]
- Gray, S.; Chen, Y.-L.; Lin, D. Efficacy of Proton Beam Therapy in the Treatment of Ewing’s Sarcoma of the Paranasal Sinuses and Anterior Skull Base. J. Neurol. Surg. Part B Skull Base 2009, 19, 409–416. [Google Scholar] [CrossRef] [Green Version]
- Lazzeri, D.; Agostini, T.; Giacomina, A.; Giannotti, G.; Colizzi, L.; Rosa, M.D.; Massei, P.; Pantaloni, M. Malignant Melanoma of the Nasal Septum. J. Craniofac. Surg. 2010, 21, 1957–1960. [Google Scholar] [CrossRef]
- Ito, T.; Ozaki, Y.; Sato, K.; Oikawa, M.; Tanino, M.; Nakamura, H.; Tanaka, S. Radiation-Induced osteosarcomas after treatment for frontal gliomas: A report of two cases. Brain Tumor Pathol. 2010, 27, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Kim, D.; Koo, Y.; Kim, C.-H.; Choi, E.C.; Lee, J.-G.; Yoon, J.-H. Sinonasal carcinoma associated with inverted papilloma: A report of 16 cases. J. Cranio-Maxillofac. Surg. 2012, 40, e125–e129. [Google Scholar] [CrossRef]
- Madana, J.; Yolmo, D.; Gopalakrishnan, S.; Saxena, S.K. Primary Frontal Sinus Carcinoma with Extradural Anterior Cranial Fossa Involvement. Ear. Nose Throat J. 2011, 90, E4–E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bercin, S.; Muderris, T.; Kiris, M.; Kanmaz, A.; Kandemir, O. A Rare Sinonasal Neoplasm: Fibrosarcoma. Ear. Nose Throat J. 2011, 90, E6–E8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soyka, M.B.; Annen, A.; Holzmann, D. Where endoscopy fails: Indications and experience with the frontal sinus fat obliteration. Rhinology 2009, 47, 136–140. [Google Scholar]
- Kim, K.; Kim, M.J.; Ahn, S.; Bae, S.Y.; Kim, W.S.; Yoon, J.-H. Frontal Sinus Lymphoma Presenting As Progressive Multiple Cranial Nerve Palsy. Yonsei Med. J. 2011, 52, 1044–1047. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, S.; Okamura, J.; Sakai, N.; Mineta, H. Primary Spindle Cell Carcinoma of the Frontal Sinus. J. Oral Maxillofac. Surg. 2012, 70, e674–e678. [Google Scholar] [CrossRef]
- Fukumitsu, N.; Okumura, T.; Mizumoto, M.; Oshiro, Y.; Hashimoto, T.; Kanemoto, A.; Hashii, H.; Ohkawa, A.; Moritake, T.; Tsuboi, K.; et al. Outcome of T4 (International Union against Cancer Staging System, 7th edition) or Recurrent Nasal Cavity and Paranasal Sinus Carcinoma Treated with Proton Beam. Int. J. Radiat. Oncol. 2012, 83, 704–711. [Google Scholar] [CrossRef]
- Peregud-Pogorzelski, J.; Wawrykow, P.; Wozniak, S.; Zakowska, A.; Brodkiewicz, A. Highly effective unconventional management of aspergillosis of the left maxillary sinus in an 11-year-old girl with rhabdomyosarcoma embryonale of the frontal sinus. J. Med. Microbiol. 2013, 62, 652–654. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.-Z.; Li, Y.-P.; She, L.; Wang, X.-D.; Yan, Z.-C.; Zhang, N.; Xu, E.-X. Primary carcinoma of the frontal sinus with extensive intracranial invasion: A case report and review of the literature. Oncol. Lett. 2014, 7, 1915–1918. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.H.; Kim, N.G.; Lee, K.S.; Kim, J.S. Malignant Peripheral Nerve Sheath Tumor in Frontal Sinus, Orbital Cavity and Ethmoid Cavity. Arch. Craniofac. Surg. 2014, 15, 125–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankowski, R.; Russel, A.; Gallet, P.; Henrot, P.; Vignaud, J.M.; Nguyen, D.T. Olfactory neuroblastoma behavior inside and outside the olfactory cleft. Surg. Radiol. Anat. 2015, 37, 507–515. [Google Scholar] [CrossRef]
- Verim, A.; Sheidaii, S.; Bilaç, Ö.; Tepe Karaca, Ç.; Naiboğlu, B. Extramedullary Plasmacytoma of the Frontal Sinus: Case Report and Turkish Literature Review. Turk. J. Hematol. 2014, 31, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Tomovic, S.; Kalyoussef, E.; Mirani, N.M.; Baredes, S.; Eloy, J.A. Angiosarcoma arising from the frontal sinus. Am. J. Otolaryngol. 2014, 35, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.; Lakičević, G.; Callihan, T.; Burruss, G.; Arnautović, K. Diffuse Large B-Cell Lymphoma of the Frontal Sinus Presenting as a Pott Puffy Tumor: Case Report. J. Neurol. Surg. Rep. 2015, 76, e23–e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kieliszak, C.R.; Cosenza, M.J. Granulocytic Sarcoma of the Frontal Sinuses. Otolaryngol. Neck Surg. 2015, 153, 691–692. [Google Scholar] [CrossRef]
- Kuan, E.C.; Frederick, J.W.; Diaz, M.F.P.; Lim, D.W.; Suh, J.D. Complete Response of Skull Base Inverted Papilloma to Chemotherapy: Case Report. Allergy Rhinol. 2017, 8, e105–e108. [Google Scholar] [CrossRef] [Green Version]
- Minato, H.; Kobayashi, E.; Nakada, S.; Kurose, N.; Tanaka, M.; Tanaka, Y.; Suzuki, S.; Tanioka, F.; Saikawa, Y.; Miwa, T.; et al. Sinonasal NUT carcinoma: Clinicopathological and cytogenetic analysis with autopsy findings. Hum. Pathol. 2018, 71, 157–165. [Google Scholar] [CrossRef]
- Cannon, R.; Wiggins, R.; Witt, B.; Dundar, Y.; Johnston, T.; Hunt, J.; Iii, R.H.W.; Wu, A.W.; Suh, J.D.; Metson, R.; et al. Imaging and Outcomes for a New Entity: Low-Grade Sinonasal Sarcoma with Neural and Myogenic Features. J. Neurol. Surg. Rep. 2017, 78, e15–e19. [Google Scholar] [CrossRef] [Green Version]
- Sienna, J.; Nguyen, N.-T.; Arsenault, J.; Hodson, I.; Meyers, B. A Case of Sinonasal Undifferentiated Carcinoma with Brain Metastases. Cureus. 2018. Available online: https://www.cureus.com/articles/7176-a-case-of-sinonasal-undifferentiated-carcinoma-with-brain-metastases (accessed on 20 February 2023).
- Kim, J.; Chang, H.; Jeong, E.C. Sinonasal intestinal-type adenocarcinoma in the frontal sinus. Arch. Craniofacial Surg. 2018, 19, 210–213. [Google Scholar] [CrossRef]
- Nagafuji, H.; Yokoi, H.; Ohara, A.; Fujiwara, M.; Takayama, N.; Saito, K. Primary diffuse large B-cell lymphoma of the frontal sinus: A case report and literature review. Radiol. Case Rep. 2018, 13, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Biswas, A.; Devnani, B.; Agarwal, S.; Sharma, M.C.; Sharma, A. Combined Modality Management of Sinonasal Anaplastic Lymphoma Kinase-Positive Anaplastic Large Cell Lymphoma in a Young Adult—Report of a Rare Case. J. Adolesc. Young Adult Oncol. 2019, 8, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Tirelli, G.; Capriotti, V.; Sartori, G.; Tofanelli, M.; Marcuzzo, A.V. Primary Adenoid Cystic Carcinoma of the Frontal Sinus: Case Description of a Previously Unreported Entity and Literature Review. Ear. Nose Throat J. 2019, 98, E8–E12. [Google Scholar] [CrossRef] [PubMed]
- Alvi, M.I.U.R.; Pathmanaban, O.; Bhalla, R.; Mani, N. Recurrence of a complex anterior skull base tumour managed with an uncommon surgical approach. BMJ Case Rep. 2019, 12, e228622. [Google Scholar] [CrossRef]
- Knudson, S.A.; Day, K.M.; Harshbarger, R.J. Pediatric Diffuse Large B-Cell Lymphoma of the Frontal Sinus: A Case Report. Cleft Palate. Craniofac. J. 2019, 56, 1089–1095. [Google Scholar] [CrossRef]
- Lee, Y.-M.; Park, H.-J.; Kim, S.-D.; Cho, K.-S. Mini Osteoplastic Flap Through Supra-Eyebrow Incision for Primary Frontal Sinus Squamous Cell Carcinoma. J. Craniofac. Surg. 2020, 31, 517–519. [Google Scholar] [CrossRef]
- Costa, I.E.; Sousa Menezes, A.; Lima, A.F.; Rodrigues, B. Extra-skeletal Ewing’s sarcoma of the frontal sinus: A rare disorder in pediatric age. BMJ Case Rep. 2020, 13, e232460. [Google Scholar] [CrossRef]
- Baudoin, M.E.; Palines, P.A.; Stalder, M.W. Frontal Cranioplasty with Vascularized Split-Iliac Crest Bone Flap. Plast. Reconstr. Surg.-Glob. Open 2021, 9, e3934. [Google Scholar] [CrossRef]
- Andron, A.; Peleg, U.; Genzel, C.; Drabkin, E. Masquerading solitary plasmacytoma; an eyelid lump in disguise. Oman J. Ophthalmol. 2021, 14, 42–44. [Google Scholar] [CrossRef]
- Yoon, S.; Ryu, K.H.; Baek, H.J.; An, H.J.; Joo, Y.-H. Epstein-Barr virus-positive diffuse large B-cell lymphoma with human immunodeficiency virus mimicking complicated frontal sinusitis: A case report. World J. Clin. Cases 2021, 9, 1654–1660. [Google Scholar] [CrossRef]
- Kieu, H.D.; Le, T.D.; Nguyen, V.; Tran, T.Q. Malignant mucosal melanoma of paranasal sinuses: A case report. Int. J. Surg. Case Rep. 2021, 87, 106450. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.S.; Porter, K.; Mallin, K.; Hoffman, H.T.; Weber, R.S.; Ang, K.K.; Gay, E.G.; Langer, C.J. National Cancer Database report on cancer of the head and neck: 10-Year update. Head Neck 2009, 31, 748–758. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Orlandi, E.; Bossi, P. Sinonasal cancers treatments: State of the art. Curr. Opin. Oncol. 2021, 33, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Osguthorpe, J.D.; Richardson, M. Frontal Sinus Malignancies. Otolaryngol. Clin. N. Am. 2001, 34, 269–281. [Google Scholar] [CrossRef]
- Lydiatt, W.M.; Patel, S.G.; Ridge, J.A.; O’Sullivan, B.; Shah, J.P. Staging Head and Neck Cancers. In AJCC Cancer Staging Manual; Amin, M.B., Edge, S.B., Greene, F.L., Byrd, D.R., Brookland, R.K., Washington, M.K., Gershenwald, J.E., Compton, C.C., Hess, K.R., Sullivan, D.C., et al., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 55–65. Available online: http://link.springer.com/10.1007/978-3-319-40618-3_561 (accessed on 4 January 2023).
- Katz, T.S.; Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Hinerman, R.W.; Villaret, D.B. Malignant tumors of the nasal cavity and paranasal sinuses. Head Neck 2002, 24, 821–829. [Google Scholar] [CrossRef]
- Pietrobon, G.; Karligkiotis, A.; Turri-Zanoni, M.; Fazio, E.; Battaglia, P.; Bignami, M.; Castelnuovo, P. Surgical management of inverted papilloma involving the frontal sinus: A practical algorithm for treatment planning. Acta Otorhinolaryngol. Ital. 2019, 39, 28–39. [Google Scholar] [CrossRef] [Green Version]





| Variable | n | % | |
|---|---|---|---|
| Age (years) | Mean | 60 | / |
| Median | 62 | / | |
| Range | 17–83 | / | |
| Gender | Male | 48 | 57.1% |
| Female | 36 | 42.9% | |
| Presentation | Naive | 56 | 66.7% |
| Relapse/persistence | 28 | 33.3% | |
| Origin | Frontal sinus | 24 | 28.6% |
| Other sinuses | 60 | 71.4% | |
| T classification | T3 | 5 | 6.0% |
| T4a | 30 | 35.7% | |
| T4b | 49 | 58.3% | |
| N classification | N0 | 82 | 97.6% |
| N+ | 2 | 2.4% | |
| M classification | M0 | 81 | 96.4% |
| M1 | 3 | 3.6% | |
| Histotype | Carcinoma | 21 | 25.0% |
| Mucosal melanoma | 14 | 16.7% | |
| SNEC/SNUC | 13 | 15.5% | |
| Adenocarcinoma | 12 | 14.3% | |
| ITAC | 9 | 75.0% | |
| non-ITAC | 2 | 16.7% | |
| NOS | 1 | 8.3% | |
| Soft tissue tumors | 10 | 11.9% | |
| ONB | 7 | 8.3% | |
| Salivary gland cancer | 5 | 5.9% | |
| ACC | 3 | 60.0% | |
| Acinic cell | 1 | 20.0% | |
| Salivary | 1 | 20.0% | |
| Lymphatic tumors | 2 | 2.4% | |
| Surgical treatment | EER/ERTC | 43 | 51.2% |
| EER + OPF | 6 | 7.1% | |
| CER/CFR | 35 | 41.7% | |
| Dural resection | Yes | 52 | 61.9% |
| No | 32 | 38.1% | |
| Margins status | R0 | 53 | 63.1% |
| R1 | 31 | 36.9% | |
| Adjuvant treatments | Yes | 61 | 72.6% |
| No | 23 | 27.4% | |
| Complications | Yes | 16 | 19.0% |
| No | 68 | 81.0% | |
| Follow-up | Mean | 39 | / |
| Range | 6–149 | / | |
| Recurrence | Yes | 33 | 39.3% |
| No | 51 | 60.7% | |
| Status | NED | 33 | 39.3% |
| AWD | 16 | 19.0% | |
| DOC | 7 | 8.3% | |
| DOD | 28 | 33.4% |
| Variable | OS | DSS | DFS | RFS | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 3-y (%) | 5-y (%) | p-Value | 3-y (%) | 5-y (%) | p-Value | 3-y (%) | 5-y (%) | p-Value | 3-y (%) | 5-y (%) | p-Value | ||
| Age | ≤60 years | 76.2 ± 8.2 | 71.1 ± 9.1 | 0.005 | 82.6 ± 7.4 | 82.6 ± 7.4 | 0.003 | 46.6 ± 8.8 | 46.6 ± 8.8 | 0.163 | 72.9 ± 8.3 | 65.6 ± 10.2 | 0.522 |
| >60 years | 49.2 ± 7.9 | 38.7 ± 8.2 | 56.6 ± 7.8 | 44.6 ± 8.7 | 30.7 ± 7.2 | 25.1 ± 6.9 | 63.5 ± 8.6 | 57.7 ± 9.6 | |||||
| Presentation | Naive | 56.5 ± 7.4 | 49.7 ± 7.9 | 0.469 | 65.4 ± 6.9 | 57.5 ± 8.0 | 0.566 | 39.7 ± 7.1 | 36.8 ± 7.1 | 0.658 | 80.3 ± 6.3 | 80.3 ± 6.3 | <0.0005 |
| Relapse | 67.9 ± 10.2 | 56.0 ± 11.4 | 71.9 ± 10.0 | 64.7 ± 11.3 | 32.6 ± 9.4 | 28.5 ± 9.1 | 45.3 ± 10.5 | 31.7 ± 11.1 | |||||
| pT | pT3 | 50.0 ± 35.4 | 50.0 ± 35.4 | 0.612 | 50.0 ± 35.4 | 50.0 ± 35.4 | 0.810 | 21.4 ± 18.8 | NA | 0.290 | 50.0 ± 25.0 | NA | 0.112 |
| pT4a-4b | 59.8 ± 6.1 | 51.0 ± 6.6 | 66.4 ± 5.8 | 59.4 ± 6.7 | 38.4 ± 5.9 | 36.5 ± 5.9 | 68.8 ± 6.1 | 65.0 ± 6.9 | |||||
| Tumor epicenter | Frontal | 68.5 ± 11.1 | 68.5 ± 11.1 | 0.097 | 73.0 ± 10.9 | 73.0 ± 10.9 | 0.164 | 43.9 ± 10.4 | 36.5 ± 10.9 | 0.678 | 62.2 ± 10.6 | 42.7 ± 13.7 | 0.146 |
| Other | 56.6 ± 7.1 | 45.7 ± 7.6 | 64.5 ± 6.8 | 54.5 ± 7.9 | 35.1 ± 6.7 | 32.9 ± 6.6 | 69.7 ± 7.4 | 69.7 ± 7.4 | |||||
| Histology | SGC | 53.3 ± 24.8 | NA | 0.206 | 66.7 ± 27.2 | NA | 0.232 | NA | NA | 0.049 | NA | NA | 0.347 |
| MM | 39.2 ± 16.4 | 39.2 ± 16.4 | 39.2 ± 16.4 | 39.2 ± 16.4 | 18.5 ± 11.6 | 9.3 ± 8.8 | 80.0 ± 12.6 | 53.3 ± 23.3 | |||||
| SNEC/SNUC | 34.6 ± 15.1 | 34.6 ± 15.1 | 34.6 ± 15.1 | 34.6 ± 15.1 | 28.0 ± 13.6 | 28.0 ± 13.6 | 77.9 ± 14.1 | 77.9 ± 14.1 | |||||
| ADC | 54.7 ± 15.4 | 32.8 ± 15.1 | 72.9 ± 13.5 | 54.7 ± 18.8 | 22.2 ± 12.8 | 22.2 ± 12.8 | 51.6 ± 15.8 | 51.6 ± 15.8 | |||||
| SCC | 72.2 ± 10.7 | 64.2 ± 12.1 | 78.2 ± 9.7 | 69.5 ± 11.9 | 40.7 ± 11.7 | 40.7 ± 11.7 | 60.0 ± 12.0 | 60.0 ± 12.0 | |||||
| Lymphatic tumor | 100 | 100 | 100 | 100 | 50.0 ± 35.4 | 50.0 ± 35.4 | 50.0 ± 35.4 | 50.0 ± 35.4 | |||||
| Soft tissue tumor | 80.0 ± 12.6 | 80.0 ± 12.6 | 80.0 ± 12.6 | 80.0 ± 12.6 | 70.0 ± 14.5 | 70.0 ± 14.5 | 77.8 ± 13.9 | 77.8 ± 13.9 | |||||
| ONB | 80.0 ± 17.9 | 60.0 ± 21.9 | 100 | 75.0 ± 21.7 | 80.0 ± 17.9 | 60.0 ± 21.9 | 100 | 50.0 ± 35.4 | |||||
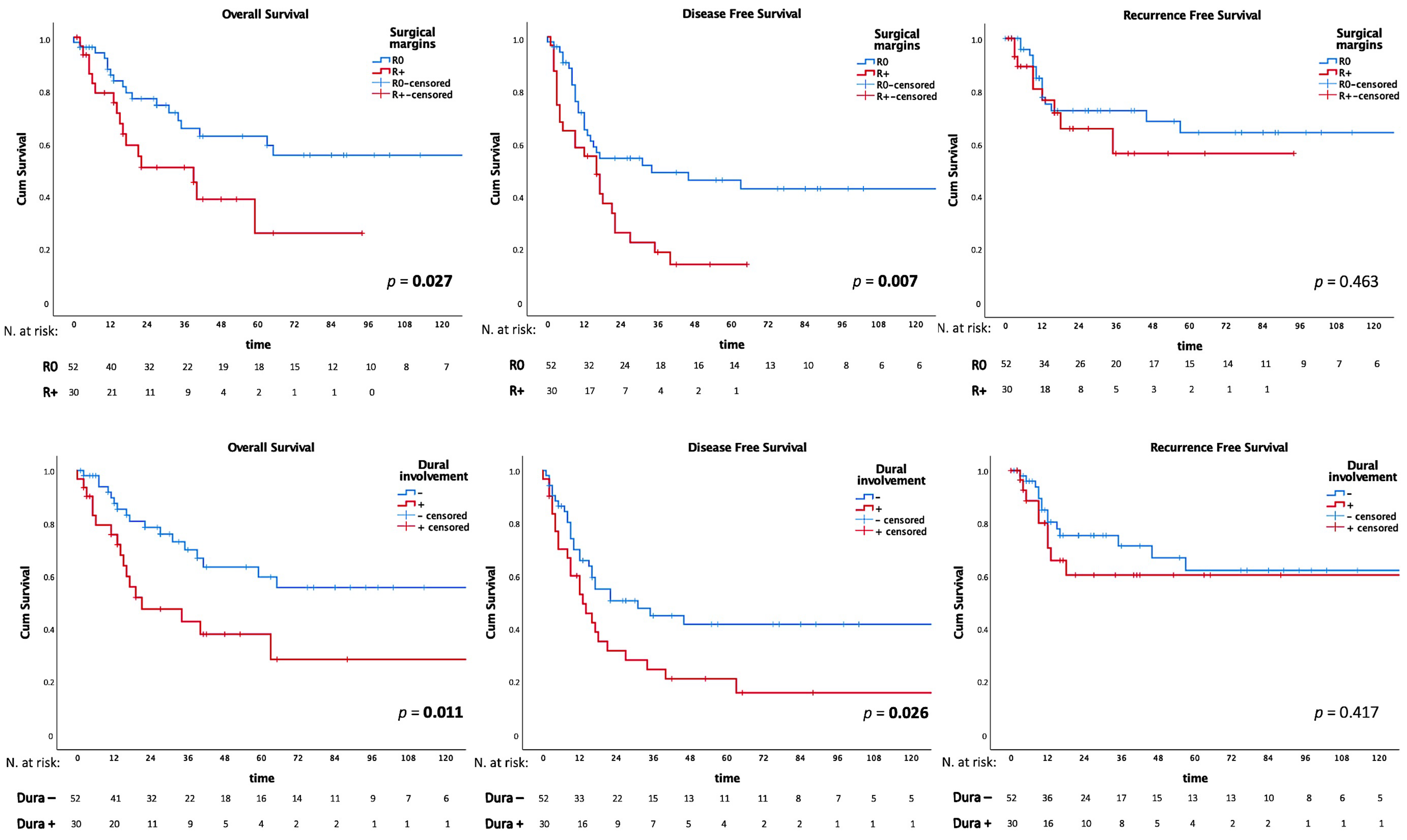
| Dural involvement | yes | 42.9 ± 10.0 | 38.1 ± 9.9 | 0.011 | 53.7 ± 9.9 | 47.8 ± 10.5 | 0.045 | 24.8 ± 8.1 | 21.3 ± 7.7 | 0.026 | 60.5 ± 10.5 | 60.5 ± 10.5 | 0.417 |
| no | 70.0 ± 7.1 | 59.7 ± 8.2 | 74.9 ± 6.7 | 66.9 ± 8.0 | 45.1 ± 7.4 | 41.9 ± 7.6 | 71.5 ± 7.3 | 62.2 ± 8.8 | |||||
| Surgery | EER | 61.2 ± 8.7 | 53.6 ± 9.1 | 0.093 | 66.3 ± 8.3 | 58.9 ± 9.2 | 0.231 | 37.9 ± 8.0 | 30.8 ± 7.9 | 0.023 | 79.8 ± 6.9 | 71.8 ± 9.8 | 0.009 |
| EER/OPF | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | |||||
| CER/CFR | 51.9 ± 9.1 | 42.6 ± 9.1 | 60.9 ± 8.9 | 54.1 ± 10.2 | 27.1 ± 7.9 | 27.1 ± 7.9 | 47.1 ± 10.1 | 47.1 ± 10.1 | |||||
| Surgical Margins | R0 | 65.5 ± 7.4 | 62.5 ± 7.7 | 0.027 | 74.5 ± 6.8 | 71.1 ± 7.3 | 0.015 | 48.6 ± 7.5 | 45.8 ± 7.6 | 0.007 | 72.7 ± 6.8 | 64.3 ± 8.2 | 0.436 |
| R1/2 | 50.7 ± 9.9 | 25.7 ± 12.7 | 54.6 ± 9.9 | 31.2 ± 14.7 | 18.5 ± 7.3 | 13.8 ± 6.8 | 56.4 ± 12.3 | 56.4 ± 12.3 | |||||
| Grading | G1–2 | 76.1 ± 9.6 | 56.4 ± 12.1 | 0.287 | 90.9 ± 6.1 | 67.3 ± 12.6 | 0.130 | 54.7 ± 10.8 | 49.2 ± 11.0 | 0.104 | 76.8 ± 9.1 | 67.2 ± 12.0 | 0.369 |
| G3 | 51.2 ± 9.8 | 46.6 ± 10.0 | 59.2 ± 9.6 | 59.2 ± 9.6 | 29.1 ± 8.7 | 29.1 ± 8.7 | 60.7 ± 10.0 | 60.7 ± 10.0 | |||||
| Adjuvant treatment | yes | 60.4 ± 7.0 | 53.7 ± 7.7 | 0.902 | 67.1 ± 6.6 | 59.6 ± 7.8 | 0.818 | 39.4 ± 6.7 | 34.1 ± 6.7 | 0.820 | 69.6 ± 6.7 | 64.7 ± 7.8 | 0.519 |
| no | 59.9 ± 11.3 | 47.2 ± 12.0 | 68.3 ± 11.0 | 59.8 ± 12.5 | 33.0 ± 10.6 | 33.0 ± 10.6 | 62.6 ± 12.6 | 52.2 ± 14.2 | |||||
| Variable | OS | DSS | DFS | RFS | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HR | HR CI 95% | p-Value | HR | HR CI 95% | p-Value | HR | HR CI 95% | p-Value | HR | HR CI 95% | p-Value | |
| Age (>60 year vs. ≤60 year) | 2.5 | 1.1–5.7 | 0.028 | 3.3 | 1.2–8.9 | 0.019 | 1.6 | 0.6–2.2 | 0.542 | 1.3 | 0.5–3.1 | 0.616 |
| Dural involvement (yes vs. no) | 1.8 | 0.8–3.6 | 0.103 | 1.5 | 0.7–3.3 | 0.333 | 1.5 | 0.8–2.7 | 0.184 | 1.3 | 0.5–3.1 | 0.590 |
| Surgery (CER/CFR vs. EER/OPF) | 1.7 | 0.8–3.4 | 0.117 | 1.4 | 0.6–2.9 | 0.396 | 1.6 | 0.9–2.7 | 0.108 | 3.3 | 1.4–7.9 | 0.006 |
| Margins (R1/2 vs. R0) | 1.4 | 0.6–2.9 | 0.354 | 1.7 | 0.8–3.9 | 0.174 | 1.7 | 0.9–3.2 | 0.062 | 1.1 | 0.4–2.8 | 0.802 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sileo, G.; Valentini, M.; Gravante, G.; Monti, G.; Arosio, A.D.; Bignami, M.; Battaglia, P.; Castelnuovo, P.; Turri-Zanoni, M. Sinonasal Malignancies Involving the Frontal Sinus: A Mono-Institutional Experience of 84 Cases and Systematic Literature Review. J. Clin. Med. 2023, 12, 3186. https://doi.org/10.3390/jcm12093186
Sileo G, Valentini M, Gravante G, Monti G, Arosio AD, Bignami M, Battaglia P, Castelnuovo P, Turri-Zanoni M. Sinonasal Malignancies Involving the Frontal Sinus: A Mono-Institutional Experience of 84 Cases and Systematic Literature Review. Journal of Clinical Medicine. 2023; 12(9):3186. https://doi.org/10.3390/jcm12093186
Chicago/Turabian StyleSileo, Giorgio, Marco Valentini, Giacomo Gravante, Giulia Monti, Alberto D. Arosio, Maurizio Bignami, Paolo Battaglia, Paolo Castelnuovo, and Mario Turri-Zanoni. 2023. "Sinonasal Malignancies Involving the Frontal Sinus: A Mono-Institutional Experience of 84 Cases and Systematic Literature Review" Journal of Clinical Medicine 12, no. 9: 3186. https://doi.org/10.3390/jcm12093186
APA StyleSileo, G., Valentini, M., Gravante, G., Monti, G., Arosio, A. D., Bignami, M., Battaglia, P., Castelnuovo, P., & Turri-Zanoni, M. (2023). Sinonasal Malignancies Involving the Frontal Sinus: A Mono-Institutional Experience of 84 Cases and Systematic Literature Review. Journal of Clinical Medicine, 12(9), 3186. https://doi.org/10.3390/jcm12093186