

Really Asymptomatic? Health-Related Quality of Life and Objective Clinical Foot Characteristics among 5–10-Year-Old Children with a Flexible FlatFoot
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample and Procedure
2.2. Measures
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rungprai, C.; Maneeprasopchoke, P. A Clinical Approach to Diagnose Flatfoot Deformity. J. Foot Ankle Surg. 2021, 8, 48–54. [Google Scholar] [CrossRef]
- Halabchi, F.; Mazaheri, R.; Mirshahi, M.; Abbasian, L. Pediatric flexible flatfoot; Clinical aspects and algorithmic approach. Iran. J. Pediatr. 2013, 23, 247–260. [Google Scholar] [PubMed]
- Tang, S.F.T.; Chen, C.H.; Wu, C.K.; Hong, W.H.; Chen, K.J.; Chen, C.K. The effects of total contact insole with forefoot medial posting on rearfoot movement and foot pressure distributions in patients with flexible flatfoot. Clin. Neurol. Neurosurg. 2015, 129 (Suppl. S1), S8–S11. [Google Scholar] [CrossRef]
- Rome, K.; Ashford, R.L.; Evans, A. Non-surgical interventions for paediatric pes planus. Cochrane Database Syst. Rev. 2010, 7, 1–31. [Google Scholar] [CrossRef]
- Evans, A.M.; Rome, K.; Carroll, M.; Hawke, F. Foot orthoses for treating paediatric flat feet. Cochrane Database Syst. Rev. 2022, 1, 1–107. [Google Scholar] [CrossRef]
- Hawke, F.; Burns, J.; Radford, J.A.; du Toit, V. Foot Pain: Custom-made insoles offer relief After ankle surgery: Mobilise with care. Cochrane Database Syst. Rev. 2008, 3, 1–66. [Google Scholar]
- Rusu, L.; Marin, M.I.; Geambesa, M.M.; Rusu, M.R. Monitoring the Role of Physical Activity in Children with Flat Feet by Assessing Subtalar Flexibility and Plantar Arch Index. Children 2022, 9, 427. [Google Scholar] [CrossRef]
- Hung, N.N.; Duc, H.H.; Anh, L.T. Overview and Treatment for A Flatfoot in Children. Int. J. Orthop. 2022, 9, 1614–1631. [Google Scholar]
- Martínez-Nova, A.; Gijón-Noguerón, G.; Alfageme-García, P.; Montes-Alguacil, J.; Evans, A.M. Foot posture development in children aged 5 to11 years: A three-year prospective study. Gait Posture 2018, 62, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Böhm, H.; Oestreich, C.; Rethwilm, R.; Federolf, P.; Döderlein, L.; Fujak, A.; Dussa, C.U. Cluster analysis to identify foot motion patterns in children with flexible flatfeet using gait analysis—A statistical approach to detect decompensated pathology? Gait Posture 2019, 71, 151–156. [Google Scholar] [CrossRef]
- Bernasconi, A.; Lintz, F.; Sadile, F. The role of arthroereisis of the subtalar joint for flatfoot in children and adults. EFORT Open Rev. 2017, 2, 438. [Google Scholar] [CrossRef] [PubMed]
- Vulcano, E.; Maccario, C.; Myerson, M.S. How to approach the pediatric flatfoot. World J. Orthop. 2016, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Jane MacKenzie, A.; Rome, K.; Evans, A.M. The efficacy of nonsurgical interventions for pediatric flexible flat foot: A critical review. J. Pediatr. Orthop. 2012, 32, 830–834. [Google Scholar] [CrossRef]
- Camurcu, Y.; Ucpunar, H.; Karakose, R.; Ozcan, S.; Sahin, V. Foot orthoses use for pediatric flexible flatfoot: Comparative evaluation of quality of life for children and parents. J. Pediatr. Orthop. B 2021, 30, 282–286. [Google Scholar] [CrossRef]
- Kothari, A.; Dixon, P.C.; Stebbins, J.; Zavatsky, A.B.; Theologis, T. The relationship between quality of life and foot function in children with flexible flatfeet. Gait Posture 2015, 41, 786–790. [Google Scholar] [CrossRef]
- Indino, C.; Villafañe, J.H.; D’Ambrosi, R.; Manzi, L.; Maccario, C.; Berjano, P.; Usuelli, F.G. Effectiveness of subtalar arthroereisis with endorthesis for pediatric flexible flat foot: A retrospective cross-sectional study with final follow up at skeletal maturity. Foot Ankle Surg. 2020, 26, 98–104. [Google Scholar] [CrossRef]
- Sterian, A.G.; Ulici, A. Quality of Life after Flatfoot Surgery in the Pediatric Population. J. Med. Life 2020, 13, 356. [Google Scholar] [CrossRef]
- Bok, S.K.; Lee, H.; Kim, B.O.; Ahn, S.; Song, Y.; Park, I. The effect of different foot orthosis inverted angles on plantar pressure in children with flexible flatfeet. PLoS ONE 2016, 11, e0159831. [Google Scholar] [CrossRef]
- Hsieh, R.L.; Peng, H.L.; Lee, W.C. Short-term effects of customized arch support insoles on symptomatic flexible flatfoot in children. Medicine 2018, 97, e10655. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Shin, H.S.; Ko, J.H.; Cha, Y.H.; Ahn, J.H.; Hwang, J.Y. Gait analysis of symptomatic flatfoot in children: An observational study. CiOS Clin. Orthop. Surg. 2017, 9, 363–373. [Google Scholar] [CrossRef]
- Martinelli, N.; Bianchi, A.; Martinkevich, P.; Sartorelli, E.; Romeo, G.; Bonifacini, C.; Malerba, F. Return to sport activities after subtalar arthroereisis for correction of pediatric flexible flatfoot. J. Pediatr. Orthop. B 2018, 27, 82–87. [Google Scholar] [CrossRef]
- Vescio, A.; Testa, G.; Amico, M.; Lizzio, C.; Sapienza, M.; Pavone, P.; Pavone, V. Arthroereisis in juvenile flexible flatfoot: Which device should we implant? A systematic review of literature published in the last 5 years. World J. Orthop. 2021, 12, 433–444. [Google Scholar] [CrossRef]
- Li, B.; He, W.; Yu, G.; Zhou, H.; Xia, J.; Zhao, Y.; Zhu, H.; Yu, T.; Yang, Y. Treatment for Flexible Flatfoot in Children With Subtalar Arthroereisis and Soft Tissue Procedures. Front. Pediatr. 2021, 9, 656178. [Google Scholar] [CrossRef] [PubMed]
- Wen, X.; Nie, G.; Liu, C.; Zhao, H.; Lu, J.; Liang, X.; Wang, X.; Liang, J.; Guo, R.; Li, Y. Osteotomies combined with soft tissue procedures for symptomatic flexible flatfoot deformity in children. Am. J. Transl. Res. 2020, 12, 6921. [Google Scholar]
- Kothari, A.; Theologis, T.; Bhuva, S.; Stebbins, J.; Zavatsky, A.B. An investigation into the aetiology of flexible flat feet: The role of subtalar joint morphology. Bone Jt. J. 2016, 98B, 564–568. [Google Scholar] [CrossRef]
- Hösl, M.; Böhm, H.; Multerer, C.; Döderlein, L. Does excessive flatfoot deformity affect function? A comparison between symptomatic and asymptomatic flatfeet using the Oxford Foot Model. Gait Posture 2014, 39, 23–28. [Google Scholar] [CrossRef]
- Moraleda, L.; Mubarak, S.J. Flexible flatfoot: Differences in the relative alignment of each segment of the foot between symptomatic and asymptomatic patients. J. Pediatr. Orthop. 2011, 31, 421–428. [Google Scholar] [CrossRef]
- Lee, E.C.; Kim, M.O.; Kim, H.S.; Hong, S.E. Changes in resting calcaneal stance position angle following insole fitting in children with flexible flatfoot. Ann. Rehabil. Med. 2017, 41, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Langley, B.; Cramp, M.; Morrison, S.C. Clinical measures of static foot posture do not agree. J. Foot Ankle Res. 2016, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Zuil-Escobar, J.C.; Martínez-Cepa, C.B.; Martín-Urrialde, J.A.; Gómez-Conesa, A. Evaluating the Medial Longitudinal Arch of the Foot: Correlations, Reliability, and Accuracy in People with a Low Arch. Phys. Ther. 2019, 99, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Welton, E.A. The Harris and Beath footprint: Interpretation and clinical value. Foot Ankle 1992, 13, 462–468. [Google Scholar] [CrossRef]
- Chang, C.H.; Chen, Y.C.; Yang, W.T.; Ho, P.C.; Hwang, A.W.; Chen, C.H.; Chang, J.H.; Chang, L.W. Flatfoot diagnosis by a unique bimodal distribution of footprint index in children. PLoS ONE 2014, 9, e115808. [Google Scholar] [CrossRef]
- Onodera, A.N.; Sacco, I.C.N.; Morioka, E.H.; Souza, P.S.; de Sá, M.R.; Amadio, A.C. What is the best method for child longitudinal plantar arch assessment and when does arch maturation occur? Foot 2008, 18, 142–149. [Google Scholar] [CrossRef]
- Lee, J.H.; Sung, I.Y.; Yoo, J.Y. Clinical or radiologic measurements and 3-D gait analysis in children with pes planus. Pediatr. Int. 2009, 51, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, S.A.; Bowling, F.L.; Baltzopoulos, V.; Maganaris, C.; Reeves, N.D. The reliability of measurements taken from radiographs in the assessment of paediatric flat foot deformity. Foot 2012, 22, 156–162. [Google Scholar] [CrossRef]
- Romeo, D.M.; Lucibello, S.; Musto, E.; Brogna, C.; Ferrantini, G.; Velli, C.; Cota, F.; Ricci, D.; Mercuri, E. Assessing Joint Hypermobility in Preschool-Aged Children. J. Pediatr. 2016, 176, 162–166. [Google Scholar] [CrossRef]
- Carr, J.B.; Yang, S.; Lather, L.A. Pediatric pes planus: A stateofthe-art review. Pediatrics 2016, 137, e20151230. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Limbers, C.A.; Burwinkle, T.M. Parent proxy-report of their children’s health-related quality of life: An analysis of 13,878 parents’ reliability and validity across age subgroups using the PedsQLTM 4.0 Generic Core Scales. Health Qual. Life Outcomes 2007, 5, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PedsQL 4.0: Reliability and validity of the Pediatric Quality of Life Inventory version 4.0 generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef] [PubMed]
- Podolak, O.E.; Arbogast, K.B.; Master, C.L.; Sleet, D.; Grady, M.F. Pediatric Sports-Related Concussion: An Approach to Care. Am. J. Lifestyle Med. 2021, 16, 469–484. [Google Scholar] [CrossRef]
- PedsQLTM (Pediatric Quality of Life InventoryTM). Available online: http://www.pedsql.org/score.html (accessed on 26 July 2022).
- Desai, A.D.; Zhou, C.; Stanford, S.; Haaland, W.; Varni, J.W.; Mangione-Smith, R.M. Validity and responsiveness of the pediatric quality of life inventory (PedsQL) 4.0 generic core scales in the pediatric inpatient setting. JAMA Pediatr. 2014, 168, 1114–1121. [Google Scholar] [CrossRef]
- Kothari, A.; Stebbins, J.; Zavatsky, A.B.; Theologis, T. Health-related quality of life in children with flexible flatfeet: A cross-sectional study. J. Child. Orthop. 2014, 8, 489–496. [Google Scholar] [CrossRef]
- Cheng, K.-W.; Peng, Y.; Chen, T.L.-W.; Zhang, G.; Cheung, J.C.-W.; Lam, W.-K.; Wong, D.W.-C.; Zhang, M. A Three-Dimensional Printed Foot Orthosis for Flexible Flatfoot: An Exploratory Biomechanical Study on Arch Support Reinforcement and Undercut. Materials 2021, 14, 5297. [Google Scholar] [CrossRef]
- Hösl, M.; Böhm, H.; Oestreich, C.; Dussa, C.U.; Schäfer, C.; Döderlein, L.; Nader, S.; Fenner, V. Self-perceived foot function and pain in children and adolescents with flexible flatfeet—Relationship between dynamic pedobarography and the foot function index. Gait Posture 2020, 77, 225–230. [Google Scholar] [CrossRef]
- Jafarnezhadgero, A.A.; Majlesi, M.; Madadi-Shad, M. The effects of low arched feet on lower limb joints moment asymmetry during gait in children: A cross sectional study. Foot 2018, 34, 63–68. [Google Scholar] [CrossRef]
- Kerr, C.M.; Zavatsky, A.B.; Theologis, T.; Stebbins, J. Kinematic differences between neutral and flat feet with and without symptoms as measured by the Oxford foot model. Gait Posture 2019, 67, 213–218. [Google Scholar] [CrossRef]
- Parsons, S.; Naim, S.; Richards, P.J.; McBride, D. Correction and prevention of deformity in type II tibialis posterior dysfunction. Clin. Orthop. Relat. Res. 2010, 468, 1025–1032. [Google Scholar] [CrossRef]
- Kosashvili, Y.; Fridman, T.; Backstein, D.; Safir, O.; Ziv, Y.B. The correlation between pes planus and anterior knee or intermittent low back pain. Foot Ankle Int. 2008, 29, 910–913. [Google Scholar] [CrossRef] [PubMed]
- Garrow, A.P.; Silman, A.J.; Macfarlane, G.J. The cheshire foot pain and disability survey: A population survey assessing prevalence and associations. Pain 2004, 110, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Mølgaard, C.; Lundbye-Christensen, S.; Simonsen, O. High prevalence of foot problems in the Danish population: A survey of causes and associations. Foot 2010, 20, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, U.S.D.T.; Hillstrom, H.J.; Li, W.; Dufour, A.B.; Kiel, D.P.; Procter-Gray, E.; Gagnon, M.M.; Hannan, M.T. Factors associated with hallux valgus in a population-based study of older women and men: The MOBILIZE Boston Study. Osteoarthr. Cartil. 2010, 18, 41–46. [Google Scholar] [CrossRef]
- Dibello, D.; Dallan, G.; Di Carlo, V.; Pederiva, F. Quality of life in flexible painful flatfoot treated by anterograde calcaneo-stop procedure: The patient’s and family’s perspective. PLoS ONE 2023, 18, e0263763. [Google Scholar] [CrossRef] [PubMed]
- Caravaggi, P.; Lullini, G.; Berti, L.; Giannini, S.; Leardini, A. Functional evaluation of bilateral subtalar arthroereisis for the correction of flexible flatfoot in children: 1-year follow-up. Gait Posture 2018, 64, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Gijon-Nogueron, G.; Martinez-Nova, A.; Alfageme-Garcia, P.; Montes-Alguacil, J.; Evans, A.M. International normative data for paediatric foot posture assessment: A cross-sectional investigation. BMJ Open 2019, 9, e023341. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Gu, H.; Zhang, Y.; Sun, T.; Yu, J. Risk Factors of Flatfoot in Children: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 8247. [Google Scholar] [CrossRef] [PubMed]
- Dabholkar, T.; Agarwal, A. Quality of Life in Adult Population with Flat Feet. Int. J. Health Sci. Res. 2020, 10, 193. [Google Scholar]
- Almutairi, A.F.; Mustafa, A.B.; Bin Saidan, T.; Alhizam, S.; Salam, M. The prevalence and factors associated with low back pain among people with flat feet. Int. J. Gen. Med. 2021, 14, 3677–3685. [Google Scholar] [CrossRef]
- Hagedorn, T.J.; Dufour, A.B.; Riskowski, J.L.; Hillstrom, H.J.; Menz, H.B.; Casey, V.A.; Hannan, M.T. Foot disorders, foot posture, and foot function: The Framingham foot study. PLoS ONE 2013, 8, e74364. [Google Scholar] [CrossRef]
- Smith, C.; Zaidi, R.; Bhamra, J.; Bridgens, A.; Wek, C.; Kokkinakis, M. Subtalar arthroereisis for the treatment of the symptomatic paediatric flexible pes planus: A systematic review. EFORT Open Rev. 2021, 6, 118–129. [Google Scholar] [CrossRef]
- Morrison, S.C.; Tait, M.; Bong, E.; Kane, K.J.; Nester, C. Symptomatic pes planus in children: A synthesis of allied health professional practices. J. Foot Ankle Res. 2020, 13, 1–7. [Google Scholar] [CrossRef]
- Hegazy, F.A.; Aboelnasr, E.A.; Salem, Y.; Zaghloul, A.A. Validity and diagnostic accuracy of foot posture Index-6 using radiographic findings as the gold standard to determine paediatric flexible flatfoot between ages of 6–18 years: A cross-sectional study. Musculoskelet. Sci. Pract. 2020, 46, 102107. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | AFF 1 | Controls | Total | |||
|---|---|---|---|---|---|---|
| Boys | Girls | Boys | Girls | |||
| Age, years | 5 | 20 | 20 | 21 | 20 | 81 |
| 6 | 20 | 20 | 15 | 15 | 70 | |
| 7 | 20 | 20 | 15 | 15 | 70 | |
| 8 | 20 | 20 | 15 | 15 | 70 | |
| 9 | - | - | 15 | 15 | 30 | |
| 10 | - | - | 15 | 15 | 30 | |
| Subtotal | 80 | 80 | 96 | 95 | 351 | |
| Total | 160 | 191 | ||||
| Quality of Life 1 | AFFF | Controls | Difference | Cohen’s Delta | t | p | |
|---|---|---|---|---|---|---|---|
| Children | total | 56.67 | 81.60 | −24.92 | −2.38 | −21.45 | <0.001 |
| physical | 53.84 | 85.93 | −32.09 | −2.37 | −22.08 | <0.001 | |
| emotional | 49.90 | 82.91 | −33.00 | −1.80 | −16.72 | <0.001 | |
| social | 66.09 | 84.29 | −18.20 | −0.98 | −8.72 | <0.001 | |
| school | 60.03 | 70.65 | −10.62 | −0.57 | −5.34 | <0.001 | |
| Parents | total | 27.62 | 84.63 | −57.01 | −5.77 | −50.38 | <0.001 |
| physical | 21.72 | 86.14 | −64.42 | −5.22 | −46.04 | <0.001 | |
| emotional | 25.63 | 83.09 | −57.46 | −3.84 | −34.58 | <0.001 | |
| social | 35.28 | 84.11 | −48.83 | −3.21 | −28.44 | <0.001 | |
| school | 31.38 | 84.27 | −52.89 | −3.76 | −33.65 | <0.001 | |
| Foot | Indicator | B | Beta | p | R2 |
|---|---|---|---|---|---|
| Left | Age | 0.73 | 0.30 | <0.001 | 0.86 |
| Gender | −0.47 | −0.06 | 0.007 | ||
| assessed by parents | −0.10 | −0.82 | <0.001 | ||
| assessed by children | −0.04 | −0.17 | <0.001 | ||
| Right | Age | 0.68 | 0.28 | <0.001 | 0.86 |
| Gender | −0.23 | −0.03 | 0.179 | ||
| assessed by parents | −0.10 | −0.82 | <0.001 | ||
| assessed by children | −0.04 | −0.18 | <0.001 |
| Indicator | Foot | AFF 1 | Controls | Difference | Cohen’s Delta | t | p |
|---|---|---|---|---|---|---|---|
| Clinical measurements | |||||||
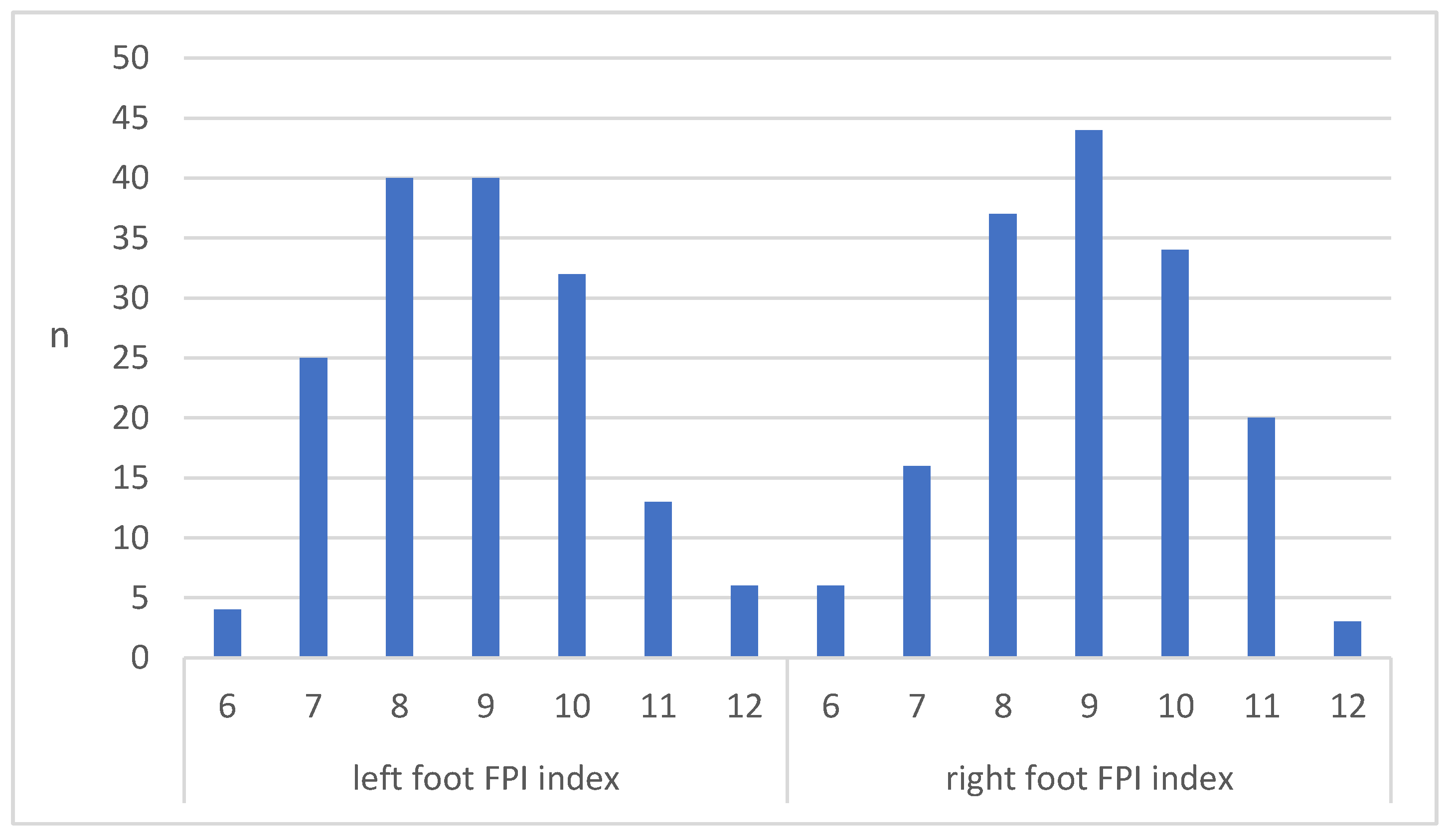
| Foot Posture Index-6 (FPI) | Left | 8.84 | 0.57 | 7.27 | 6.36 | 58.81 | <0.001 |
| Right | 8.98 | 0.55 | 7.32 | 6.61 | 61.06 | <0.001 | |
| Navicular drop test | Left | 15.54 | 1.41 | 10.31 | 6.07 | 53.02 | <0.001 |
| Right | 15.57 | 1.20 | 10.35 | 6.24 | 55.35 | <0.001 | |
| Footprints | |||||||
| Chippaux–Smirak index (CSI) | Left | 78.74 | 3.87 | 40.85 | 6.81 | 61.12 | <0.001 |
| Right | 78.76 | 3.82 | 41.23 | 6.74 | 60.66 | <0.001 | |
| Staheli’s Index | Left | 1.36 | 0.54 | 0.68 | 4.10 | 36.41 | <0.001 |
| Right | 1.36 | 0.52 | 0.68 | 4.10 | 36.33 | <0.001 | |
| Hyperlaxity | |||||||
| Beighton scale | 4.37 | 1.71 | 0.68 | 0.42 | 3.53 | <0.001 | |
| X-ray measurements | |||||||
| Calcaneal pitch angle | Left | 11.56 | 3.05 | −10.70 | −3.19 | −27.49 | <0.001 |
| Right | 11.74 | 2.96 | −10.67 | −3.48 | −29.53 | <0.001 | |
| Talocalcaneal angle | Left | 70.69 | 4.37 | 0.58 | 0.14 | 1.16 | 0.246 |
| Right | 70.58 | 5.15 | 0.96 | 0.19 | 1.61 | 0.108 | |
| Talo-1st metatarsal angle | Left | 12.51 | 3.53 | 1.55 | 2.66 | 22.54 | <0.001 |
| Right | 12.79 | 3.95 | 1.60 | 2.74 | 23.26 | <0.001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Žukauskas, S.; Barauskas, V.; Degliūtė-Muller, R.; Čekanauskas, E. Really Asymptomatic? Health-Related Quality of Life and Objective Clinical Foot Characteristics among 5–10-Year-Old Children with a Flexible FlatFoot. J. Clin. Med. 2023, 12, 3331. https://doi.org/10.3390/jcm12093331
Žukauskas S, Barauskas V, Degliūtė-Muller R, Čekanauskas E. Really Asymptomatic? Health-Related Quality of Life and Objective Clinical Foot Characteristics among 5–10-Year-Old Children with a Flexible FlatFoot. Journal of Clinical Medicine. 2023; 12(9):3331. https://doi.org/10.3390/jcm12093331
Chicago/Turabian StyleŽukauskas, Saidas, Vidmantas Barauskas, Ramunė Degliūtė-Muller, and Emilis Čekanauskas. 2023. "Really Asymptomatic? Health-Related Quality of Life and Objective Clinical Foot Characteristics among 5–10-Year-Old Children with a Flexible FlatFoot" Journal of Clinical Medicine 12, no. 9: 3331. https://doi.org/10.3390/jcm12093331
APA StyleŽukauskas, S., Barauskas, V., Degliūtė-Muller, R., & Čekanauskas, E. (2023). Really Asymptomatic? Health-Related Quality of Life and Objective Clinical Foot Characteristics among 5–10-Year-Old Children with a Flexible FlatFoot. Journal of Clinical Medicine, 12(9), 3331. https://doi.org/10.3390/jcm12093331