
A Comparative Analysis of Liver Injury Markers in Post-COVID Syndrome among Elderly Patients: A Prospective Study


 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design and Ethical Considerations
2.2. Inclusion Criteria and Definitions
2.3. Variables
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Important Findings and Literature Review
4.2. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Meis-Pinheiro, U.; Lopez-Segui, F.; Walsh, S.; Ussi, A.; Santaeugenia, S.; Garcia-Navarro, J.A.; San-Jose, A.; Andreu, A.L.; Campins, M.; Almirante, B. Clinical characteristics of COVID-19 in older adults. A retrospective study in long-term nursing homes in Catalonia. PLoS ONE 2021, 16, e0255141. [Google Scholar] [CrossRef]
- Sawyers, A.; Chou, M.; Johannet, P.; Gulati, N.; Qian, Y.; Zhong, J.; Osman, I. Clinical outcomes in cancer patients with COVID-19. Cancer Rep. 2021, 4, e1413. [Google Scholar] [CrossRef]
- Ioan Faur, C.; Abu-Awwad, A.; Pop, D.L.; Zamfir, C.L.; Gurgus, D.; Hoinoiu, T.; Motoc, A.; Haivas, C.; Grigoraș, M.L.; Folescu, R. Liquid Nitrogen Efficiency in Treatment of Giant Cell Tumor of Bone and Prevention of Recurrence. Appl. Sci. 2020, 10, 6310. [Google Scholar] [CrossRef]
- Antinori, A.; Bausch-Jurken, M. The Burden of COVID-19 in the Immunocompromised Patient: Implications for Vaccination and Needs for the Future. J. Infect. Dis. 2023, 228 (Suppl. S1), S4–S12. [Google Scholar] [CrossRef] [PubMed]
- Virzob, C.R.B.; Poenaru, M.; Morar, R.; Horhat, I.D.; Balica, N.C.; Prathipati, R.; Moleriu, R.D.; Toma, A.-O.; Juganaru, I.; Bloanca, V.; et al. Efficacy of Bilateral Cochlear Implantation in Pediatric and Adult Patients with Profound Sensorineural Hearing Loss: A Retrospective Analysis in a Developing European Country. J. Clin. Med. 2023, 12, 2948. [Google Scholar] [CrossRef]
- Daitch, V.; Yelin, D.; Awwad, M.; Guaraldi, G.; Milić, J.; Mussini, C.; Falcone, M.; Tiseo, G.; Carrozzi, L.; Pistelli, F.; et al. Characteristics of long-COVID among older adults: A cross-sectional study. Int. J. Infect. Dis. 2022, 125, 287–293. [Google Scholar] [CrossRef]
- Huerne, K.; Filion, K.B.; Grad, R.; Ernst, P.; Gershon, A.S.; Eisenberg, M.J. Epidemiological and clinical perspectives of long COVID syndrome. Am. J. Med. Open 2023, 9, 100033. [Google Scholar] [CrossRef] [PubMed]
- Fericean, R.M.; Citu, C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Tudorache, E.; Oancea, C. Characterization and Outcomes of SARS-CoV-2 Infection in Overweight and Obese Patients: A Dynamic Comparison of COVID-19 Pandemic Waves. J. Clin. Med. 2022, 11, 2916. [Google Scholar] [CrossRef] [PubMed]
- Grigoras, M.L.; Citu, I.M.; Citu, C.; Chiriac, V.D.; Gorun, F.; Levai, M.C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Gurumurthy, S.; et al. Evaluation of FIB-4, NFS, APRI and Liver Function Tests as Predictors for SARS-CoV-2 Infection in the Elderly Population: A Matched Case-Control Analysis. J. Clin. Med. 2022, 11, 5149. [Google Scholar] [CrossRef]
- Tudorache, E.; Motoc, N.S.; Pescaru, C.; Crisan, A.; Ciumarnean, L. Impact of pulmonary rehabilitation programs in improving health status in COPD patients. Balneo Res. J. 2019, 10, 472–477. [Google Scholar] [CrossRef]
- Bugari, R.A.; Başchir, A.S.; Turcin, L.A.; Chioreanu, A.; Mihali, C.V.; Ilie, A.C.; Jompan, A.; Bălăşoiu, M. Adenoidal bacterial biofilm in pediatric rhinosinusitis. Rom. J. Morphol. Embryol. 2021, 62, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Hrubaru, I.; Motoc, A.; Bratosin, F.; Rosca, O.; Folescu, R.; Moise, M.L.; Neagoe, O.; Citu, I.M.; Feciche, B.; Gorun, F.; et al. Exploring Clinical and Biological Features of Premature Births among Pregnant Women with SARS-CoV-2 Infection during the Pregnancy Period. J. Pers. Med. 2022, 12, 1871. [Google Scholar] [CrossRef] [PubMed]
- Lenz, C.; Slack, M.P.E.; Shea, K.M.; Reinert, R.R.; Taysi, B.N.; Swerdlow, D.L. Long-Term effects of COVID-19: A review of current perspectives and mechanistic insights. Crit. Rev. Microbiol. 2023, 1–14. [Google Scholar] [CrossRef]
- He, S.T.; Wu, K.; Cheng, Z.; He, M.; Hu, R.; Fan, N.; Shen, L.; Li, Q.; Fan, H.; Tong, Y. Long COVID: The latest manifestations, mechanisms, and potential therapeutic interventions. MedComm 2022, 3, e196. [Google Scholar] [CrossRef] [PubMed]
- Fericean, R.M.; Rosca, O.; Citu, C.; Manolescu, D.; Bloanca, V.; Toma, A.-O.; Boeriu, E.; Dumitru, C.; Ravulapalli, M.; Barbos, V.; et al. COVID-19 Clinical Features and Outcomes in Elderly Patients during Six Pandemic Waves. J. Clin. Med. 2022, 11, 6803. [Google Scholar] [CrossRef]
- Feier, C.V.I.; Faur, A.M.; Muntean, C.; Blidari, A.; Contes, O.E.; Streinu, D.R.; Olariu, S. The Challenges of Gastric Cancer Surgery during the COVID-19 Pandemic. Healthcare 2023, 11, 1903. [Google Scholar] [CrossRef]
- Fung, K.W.; Baye, F.; Baik, S.H.; Zheng, Z.; McDonald, C.J. Prevalence and characteristics of long COVID in elderly patients: An observational cohort study of over 2 million adults in the US. PLoS Med. 2023, 20, e1004194. [Google Scholar] [CrossRef]
- Hu, Y.; Liu, Y.; Zheng, H.; Liu, L. Risk Factors for Long COVID in Older Adults. Biomedicines 2023, 11, 3002. [Google Scholar] [CrossRef]
- Sadeghi Dousari, A.; Hosseininasab, S.S.; Sadeghi Dousari, F.; Fuladvandi, M.; Satarzadeh, N. The impact of COVID-19 on liver injury in various age. World J. Virol. 2023, 12, 91–99. [Google Scholar] [CrossRef]
- Merla, L.; Montesi, M.C.; Ticali, J.; Bais, B.; Cavarape, A.; Colussi, G. COVID-19 Accelerated Cognitive Decline in Elderly Patients with Pre-Existing Dementia Followed up in an Outpatient Memory Care Facility. J. Clin. Med. 2023, 12, 1845. [Google Scholar] [CrossRef]
- Liu, Y.H.; Wang, Y.R.; Wang, Q.H.; Chen, Y.; Chen, X.; Li, Y.; Cen, Y.; Xu, C.; Hu, T.; Liu, X.D.; et al. Post-infection cognitive impairments in a cohort of elderly patients with COVID-19. Mol. Neurodegener. 2021, 16, 48. [Google Scholar] [CrossRef] [PubMed]
- Enatescu, V.R.; Cozma, D.; Tint, D.; Enatescu, I.; Simu, M.; Giurgi-Oncu, C.; Lazar, M.A.; Mornos, C. The relationship between Type D personality and the complexity of coronary artery disease. Neuropsychiatr. Dis. Treat. 2021, 17, 809–820. [Google Scholar] [CrossRef] [PubMed]
- Oancea, R.; Timar, B.; Papava, I.; Cristina, B.A.; Ilie, A.C.; Dehelean, L. Influence of depression and self-esteem on oral health-related quality of life in students. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef] [PubMed]
- Túri, G.; Kassay, J.; Virág, A.; Dózsa, C.; Horváth, K.; Lorenzovici, L. Riding the Pandemic Waves-Lessons to Be Learned from the COVID-19 Crisis Management in Romania. Trop. Med. Infect. Dis. 2022, 7, 122. [Google Scholar] [CrossRef] [PubMed]
- Marc, M.S.; Rosca, D.; Bratosin, F.; Fira-Mladinescu, O.; Oancea, C.; Pescaru, C.C.; Velescu, D.; Wellmann, N.; Motofelea, A.C.; Ciuca, I.M.; et al. The Effect of Comorbidities and Complications on COVID-19 Mortality: A Detailed Retrospective Study in Western Romania. J. Pers. Med. 2023, 13, 1552. [Google Scholar] [CrossRef]
- Barbos, V.; Feciche, B.; Bratosin, F.; Bogdan, I.; Negrean, R.A.; Latcu, S.; Croitor, A.; Dema, V.; Bardan, R.; Cumpanas, A.A. A Retrospective Analysis of the Challenges of Urothelial Cancer Management during the COVID-19 Pandemic at a Single Academic Center in Romania. Healthcare 2023, 11, 812. [Google Scholar] [CrossRef]
- Enciu, B.G.; Tănase, A.A.; Drăgănescu, A.C.; Aramă, V.; Pițigoi, D.; Crăciun, M.D. The COVID-19 Pandemic in Romania: A Comparative Description with Its Border Countries. Healthcare 2022, 10, 1223. [Google Scholar] [CrossRef]
- Manole, C.; Baroiu, L.; Nechita, A.; Voinescu, D.C.; Ciubara, A.; Debita, M.; Tatu, A.L.; Ciubara, A.B.; Stefanopol, I.A.; Anghel, L.; et al. Comparative Evaluation of the Clinical Severity of COVID-19 of Vaccinated and Unvaccinated Patients in Southeastern Romania in the First 6 Months of 2022, during the Omicron Wave. Healthcare 2023, 11, 2184. [Google Scholar] [CrossRef]
- Mărcău, F.C.; Gheorghițoiu, R.; Bărbăcioru, I.C. Survey upon the Reasons of COVID-19 Vaccination Acceptance in Romania. Vaccines 2022, 10, 1679. [Google Scholar] [CrossRef]
- Chippa, V.; Aleem, A.; Anjum, F. Post-Acute Coronavirus (COVID-19) Syndrome. [Updated 3 February 2023]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK570608/ (accessed on 12 December 2023).
- An, Y.W.; Song, S.; Li, W.X.; Chen, Y.X.; Hu, X.P.; Zhao, J.; Li, Z.W.; Jiang, G.Y.; Wang, C.; Wang, J.C.; et al. Liver function recovery of COVID-19 patients after discharge, a follow-up study. Int. J. Med. Sci. 2021, 18, 176–186. [Google Scholar] [CrossRef]
- Gameil, M.A.; Marzouk, R.E.; Elsebaie, A.H.; Rozaik, S.E. Long-term clinical and biochemical residue after COVID-19 recovery. Egypt. Liver J. 2021, 11, 74. [Google Scholar] [CrossRef] [PubMed]
- Patterson, B.K.; Francisco, E.B.; Yogendra, R.; Long, E.; Pise, A.; Rodrigues, H.; Hall, E.; Herrera, M.; Parikh, P.; Guevara-Coto, J.; et al. Persistence of SARS CoV-2 S1 protein in CD16+ monocytes in post-acute sequelae of COVID-19 (PASC) up to 15 months post-infection. Front. Immunol. 2022, 12, 746021. [Google Scholar] [CrossRef] [PubMed]
- de Lima, I.C.; de Menezes, D.C.; Uesugi, J.H.E.; Bichara, C.N.C.; da Costa Vasconcelos, P.F.; Quaresma, J.A.S.; Falcão, L.F.M. Liver Function in Patients with Long-Term Coronavirus Disease 2019 of up to 20 Months: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 5281. [Google Scholar] [CrossRef] [PubMed]
- Bloom, P.P.; Meyerowitz, E.A.; Reinus, Z.; Daidone, M.; Gustafson, J.; Kim, A.Y.; Schaefer, E.; Chung, R.T. Liver biochemistries in hospitalized patients with COVID-19. Hepatology 2021, 73, 890–900. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef]
- Marjot, T.; Webb, G.J.; Barritt, A.S., IV; Moon, A.M.; Stamataki, Z.; Wong, V.W.; Barnes, E. COVID-19 and liver disease: Mechanistic and clinical perspectives. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 348–364. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef]
- Olry, A.; Meunier, L.; Délire, B.; Larrey, D.; Horsmans, Y.; Le Louët, H. Drug-induced liver injury and COVID-19 infection: The rules remain the same. Drug Saf. 2020, 43, 615–617. [Google Scholar] [CrossRef]
- Nevola, R.; Criscuolo, L.; Beccia, D.; Delle Femine, A.; Ruocco, R.; Imbriani, S.; Alfano, M.; Villani, A.; Russo, A.; Perillo, P.; et al. Impact of chronic liver disease on SARS-CoV-2 infection outcomes: Roles of stage, etiology and vaccination. World J. Gastroenterol. 2023, 29, 800–814. [Google Scholar] [CrossRef]
- Kovalic, A.J.; Satapathy, S.K.; Thuluvath, P.J. Prevalence of chronic liver disease in patients with COVID-19 and their clinical outcomes: A systematic review and meta-analysis. Hepatol. Int. 2020, 14, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Ozkurt, Z.; Çınar Tanrıverdi, E. COVID-19: Gastrointestinal manifestations, liver injury and recommendations. World J. Clin. Cases 2022, 10, 1140–1163. [Google Scholar] [CrossRef]
- Marjot, T.; Moon, A.M.; Cook, J.A.; Abd-Elsalam, S.; Aloman, C.; Armstrong, M.J.; Pose, E.; Brenner, E.J.; Cargill, T.; Catana, M.A.; et al. Outcomes following SARS-CoV-2 infection in patients with chronic liver disease: An international registry study. J. Hepatol. 2021, 74, 567–577. [Google Scholar] [CrossRef]
- Mahamid, M.; Nseir, W.; Khoury, T.; Mahamid, B.; Nubania, A.; Sub-Laban, K.; Schifter, J.; Mari, A.; Sbeit, W.; Goldin, E. Nonalcoholic fatty liver disease is associated with COVID-19 severity independently of metabolic syndrome: A retrospective case-control study. Eur. J. Gastroenterol. Hepatol. 2021, 33, 1578–1581. [Google Scholar] [CrossRef]
- Hashemi, N.; Viveiros, K.; Redd, W.D.; Zhou, J.C.; McCarty, T.R.; Bazarbashi, A.N.; Hathorn, K.E.; Wong, D.; Njie, C.; Shen, L.; et al. Impact of chronic liver disease on outcomes of hospitalized patients with COVID-19: A multicentre United States experience. Liver Int. 2020, 40, 2515–2521. [Google Scholar] [CrossRef]
- Kim, D.; Adeniji, N.; Latt, N.; Kumar, S.; Bloom, P.P.; Aby, E.S.; Perumalswami, P.; Roytman, M.; Li, M.; Vogel, A.S.; et al. Predictors of Outcomes of COVID-19 in Patients With Chronic Liver Disease: US Multi-center Study. Clin. Gastroenterol. Hepatol. 2021, 19, 1469–1479.e19. [Google Scholar] [CrossRef]
- Sugiyama, A.; Kurisu, A.; Bunthen, E.; Ouoba, S.; Ko, K.; Rakhimov, A.; Akita, T.; Harakawa, T.; Sako, T.; Koshiyama, M.; et al. Distribution of FIB-4 index in the general population: Analysis of 75,666 residents who underwent health checkups. BMC Gastroenterol. 2022, 22, 241. [Google Scholar] [CrossRef]
- Okada, S.; Kashima, K.; Okada, K.; Okada, J.; Kikkawa, K.; Yamada, E.; Saito, T.; Ohshima, K. Aging affects FIB-4 index in the general population without pre-existing diseases: Analysis of a cohort of healthy individuals who underwent annual health checkups for 10 consecutive years. Clin. Res. Hepatol. Gastroenterol. 2023, 47, 102058. [Google Scholar] [CrossRef]
- van Kleef, L.A.; Sonneveld, M.J.; de Man, R.A.; de Knegt, R.J. Poor performance of FIB-4 in elderly individuals at risk for chronic liver disease—Implications for the clinical utility of the EASL NIT guideline. J. Hepatol. 2022, 76, 245–246. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | Long COVID <65 Years (n = 117) | Long COVID ≥65 Years (n = 71) | No Long COVID (n = 50) | p-Value |
|---|---|---|---|---|
| Background data | ||||
| BMI, kg/m2 (mean ± SD) | 24.2 ± 4.9 | 24.8 ± 5.7 | 23.9 ± 5.5 | 0.618 |
| Gender (men) | 65 (55.6%) | 37 (52.1%) | 27 (54.0%) | 0.899 |
| Smoking | 45 (38.5%) | 20 (28.2%) | 22 (44.0%) | 0.171 |
| Frequent alcohol use | 8 (6.8%) | 8 (11.3%) | 7 (14.0%) | 0.307 |
| Comorbidities | ||||
| Cardiovascular disease | 43 (36.8%) | 31 (43.7%) | 22 (44.0%) | 0.540 |
| Metabolic disease | 18 (15.4%) | 12 (16.9%) | 13 (26.0%) | 0.251 |
| Autoimmune disease | 4 (3.4%) | 2 (2.8%) | 3 (6.0%) | 0.637 |
| Chronic kidney disease | 5 (4.3%) | 7 (9.9%) | 5 (10.0%) | 0.239 |
| Others | 6 (5.1%) | 5 (7.0%) | 6 (12.0%) | 0.287 |
| CCI score (≥2) | 26 (22.2%) | 25 (35.2%) | 16 (32.0%) | 0.222 |
| Oxygen supplementation | 0.055 | |||
| No supplementation | 11 (9.4%) | 3 (4.2%) | 7 (14.0%) | |
| Non-invasive ventilation | 88 (75.2%) | 46 (64.8%) | 33 (66.0%) | |
| Invasive ventilation | 18 (15.4%) | 22 (31.0%) | 10 (20.0%) | |
| COVID-19 severity | 0.506 | |||
| Mild | 40 (34.2%) | 18 (25.4%) | 15 (30.0%) | |
| Moderate | 43 (36.8%) | 25 (35.2%) | 21 (42.0%) | |
| Severe | 34 (29.1%) | 28 (39.4%) | 14 (28.0%) | |
| Disease outcomes | ||||
| Days of hospitalization (mean ± SD) | 11.3 ± 6.9 | 15.8 ± 8.2 | 13.2 ± 8.0 | <0.001 |
| ICU admission | 14 (12.0%) | 14 (19.7%) | 12 (10.0%) | 0.221 |
| Variables (Median IQR) | Normal Range | Long COVID <65 Years (n = 117) | Long COVID ≥65 Years (n = 71) | No Long COVID (n = 50) | p-Value |
|---|---|---|---|---|---|
| Fasting glucose (mmol/L) | 60–125 | 132.4 (121.3–143.7) | 147.8 (136.5–158.2) | 112.5 (101.9–123.4) | <0.001 |
| ALT (U/L) | 7–35 | 61.7 (51.2–72.9) | 82.3 (71.8–93.1) | 47.4 (37.6–56.5) | 0.006 |
| AST (U/L) | 10–40 | 71.2 (61.4–81.9) | 92.5 (82.7–103.6) | 52.3 (42.1–61.8) | <0.001 |
| ALP (U/L) | 40–130 | 163.5 (152.3–175.8) | 194.7 (182.4–207.9) | 143.2 (131.7–154.3) | <0.001 |
| Serum albumin (g/dL) | 3.4–5.4 | 2.6 (2.4–2.9) | 2.1 (1.9–2.4) | 3.2 (2.9–3.5) | 0.044 |
| Total proteins (g/dL) | 6.0–8.3 | 6.7 (6.3–7.2) | 5.9 (5.4–6.5) | 7.3 (6.8–7.9) | 0.020 |
| Total bilirubin (g/dL) | 0.3–1.2 | 1.8 (1.5–2.2) | 2.4 (2.0–2.9) | 1.1 (0.9–1.3) | 0.002 |
| GGT (U/L) | 0–30 | 45.3 (39.8–52.1) | 58.6 (51.9–66.4) | 31.5 (25.7–38.2) | <0.001 |
| LDH (U/L) | 140–280 | 312.4 (295.1–331.7) | 364.5 (345.9–384.8) | 265.3 (248.6–283.7) | <0.001 |
| PT (seconds) | 11.0–13.5 | 15.2 (14.6–15.9) | 16.7 (16.0–17.5) | 13.4 (12.8–14.1) | 0.039 |
| APTT (seconds) | 30–40 | 43.8 (41.5–46.4) | 49.3 (46.9–52.1) | 36.7 (34.3–39.2) | 0.010 |
| FIB-4 | 1.45–3.25 | 3.3 (2.0–4.7) | 3.9 (2.5–4.4) | 1.7 (1.4–2.0) | <0.001 |
| NFS | ≤1.5 | −0.4 (−0.7–−0.1) | 0.2 (-0.1–0.6) | −1.6 (−1.9–−1.3) | <0.001 |
| APRI | 0.5–1.5 | 1.8 (1.0–2.5) | 2.6 (1.3–3.9) | 0.8 (0.6–1.0) | <0.001 |
| Variables (Median IQR) | Normal Range | Long COVID <65 Years (n = 117) | Long COVID ≥65 Years (n = 71) | No Long COVID (n = 50) | p-Value |
|---|---|---|---|---|---|
| Fasting glucose (mmol/L) | 60–125 | 119.2 (109.3–129.8) | 126.7 (116.9–137.2) | 97.8 (88.1–107.9) | <0.001 |
| ALT (U/L) | 7–35 | 49.7 (40.2–60.1) | 58.2 (48.9–68.4) | 28.5 (19.1–38.6) | <0.001 |
| AST (U/L) | 10–40 | 51.8 (42.5–62.4) | 62.3 (53.1–72.8) | 33.9 (24.7–44.6) | <0.001 |
| ALP (U/L) | 40–130 | 145.9 (135.7–157.6) | 164.3 (153.8–176.5) | 110.2 (100.1–121.8) | <0.001 |
| Serum albumin (g/dL) | 3.4–5.4 | 3.7 (3.5–3.9) | 3.3 (3.1–3.6) | 4.2 (4.0–4.5) | 0.038 |
| Total proteins (g/dL) | 6.0–8.3 | 7.2 (6.9–7.6) | 6.7 (6.3–7.1) | 7.8 (7.5–8.2) | 0.022 |
| Total bilirubin (g/dL) | 0.3–1.2 | 1.3 (1.1–1.6) | 1.6 (1.3–1.9) | 0.8 (0.6–1.0) | 0.064 |
| GGT (U/L) | 0–30 | 36.4 (31.1–42.8) | 41.9 (36.3–48.2) | 24.6 (19.4–30.5) | <0.001 |
| LDH (U/L) | 140–280 | 292.7 (276.4–310.3) | 315.8 (299.2–333.9) | 210.4 (194.1–228.2) | <0.001 |
| PT (seconds) | 11.0–13.5 | 14.3 (13.7–15.0) | 15.4 (14.8–16.1) | 12.6 (12.0–13.3) | <0.001 |
| APTT (seconds) | 30–40 | 39.5 (37.2–41.9) | 42.8 (40.4–45.3) | 33.1 (30.8–35.6) | <0.001 |
| FIB-4 | 1.45–3.25 | 1.9 (1.6–2.3) | 2.7 (1.9–3.6) | 1.4 (1.1–1.8) | 0.010 |
| NFS | ≤1.5 | −0.9 (−1.3–−0.6) | −0.5 (−0.9–−0.2) | −1.7 (−2.0–−1.5) | 0.073 |
| APRI | 0.5–1.5 | 1.1 (0.9–1.4) | 1.5 (1.1–1.9) | 0.7 (0.5–0.9) | 0.055 |
| Variables (Median IQR) | Normal Range | Initial Measurement | Second Measurement | p-Value |
|---|---|---|---|---|
| Long COVID <65 years (n = 117) | ||||
| Fasting glucose (mmol/L) | 60–125 | 132.4 (121.3–143.7) | 119.2 (109.3–129.8) | <0.001 |
| ALT (U/L) | 7–35 | 61.7 (51.2–72.9) | 49.7 (40.2–60.1) | <0.001 |
| AST (U/L) | 10–40 | 71.2 (61.4–81.9) | 51.8 (42.5–62.4) | <0.001 |
| ALP (U/L) | 40–130 | 163.5 (152.3–175.8) | 145.9 (135.7–157.6) | 0.004 |
| Serum albumin (g/dL) | 3.4–5.4 | 2.6 (2.4–2.9) | 3.7 (3.5–3.9) | <0.001 |
| Total proteins (g/dL) | 6.0–8.3 | 6.7 (6.3–7.2) | 7.2 (6.9–7.6) | 0.058 |
| Total bilirubin (g/dL) | 0.3–1.2 | 1.8 (1.5–2.2) | 1.3 (1.1–1.6) | 0.106 |
| GGT (U/L) | 0–30 | 45.3 (39.8–52.1) | 36.4 (31.1–42.8) | 0.001 |
| LDH (U/L) | 140–280 | 312.4 (295.1–331.7) | 292.7 (276.4–310.3) | 0.042 |
| PT (seconds) | 11.0–13.5 | 15.2 (14.6–15.9) | 14.3 (13.7–15.0) | 0.094 |
| APTT (seconds) | 30–40 | 43.8 (41.5–46.4) | 39.5 (37.2–41.9) | 0.010 |
| FIB-4 | 1.45–3.25 | 3.3 (2.0–4.7) | 1.9 (1.6–2.3) | <0.001 |
| NFS | <-1.5 | −0.4 (−0.7–−0.1) | −0.9 (−1.3–−0.6) | <0.001 |
| APRI | 0.5–1.5 | 1.8 (1.0–2.5) | 1.1 (0.9–1.4) | 0.003 |
| Long COVID ≥65 years (n = 71) | ||||
| Fasting glucose (mmol/L) | 60–125 | 147.8 (136.5–158.2) | 126.7 (116.9–137.2) | <0.001 |
| ALT (U/L) | 7–35 | 82.3 (71.8–93.1) | 58.2 (48.9–68.4) | <0.001 |
| AST (U/L) | 10–40 | 92.5 (82.7–103.6) | 62.3 (53.1–72.8) | <0.001 |
| ALP (U/L) | 40–130 | 194.7 (182.4–207.9) | 164.3 (153.8–176.5) | <0.001 |
| Serum albumin (g/dL) | 3.4–5.4 | 2.1 (1.9–2.4) | 3.3 (3.1–3.6) | <0.001 |
| Total proteins (g/dL) | 6.0–8.3 | 5.9 (5.4–6.5) | 6.7 (6.3–7.1) | 0.040 |
| Total bilirubin (g/dL) | 0.3–1.2 | 2.4 (2.0–2.9) | 1.6 (1.3–1.9) | 0.033 |
| GGT (U/L) | 0–30 | 58.6 (51.9–66.4) | 41.9 (36.3–48.2) | <0.001 |
| LDH (U/L) | 140–280 | 364.5 (345.9–384.8) | 315.8 (299.2–333.9) | 0.002 |
| PT (seconds) | 11.0–13.5 | 16.7 (16.0–17.5) | 15.4 (14.8–16.1) | 0.065 |
| APTT (seconds) | 30–40 | 49.3 (46.9–52.1) | 42.8 (40.4–45.3) | 0.001 |
| FIB-4 | 1.45–3.25 | 3.9 (2.5–4.4) | 2.7 (1.9 −3.6) | <0.001 |
| NFS | ≤1.5 | 0.2 (−0.1–0.6) | −0.5 (−0.9–−0.2) | 0.010 |
| APRI | 0.5–1.5 | 2.6 (1.3–3.9) | 1.5 (1.1–1.9) | <0.001 |
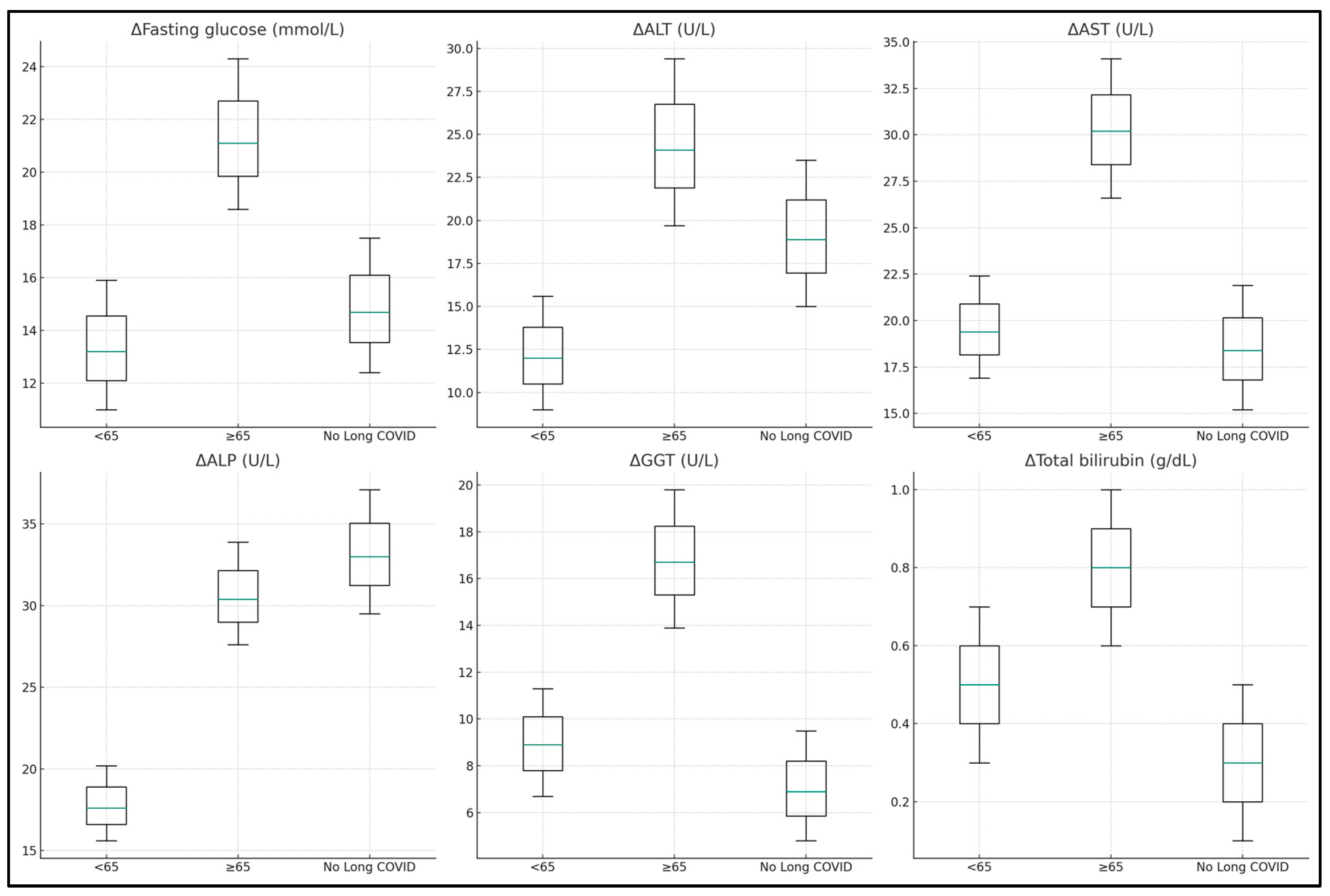
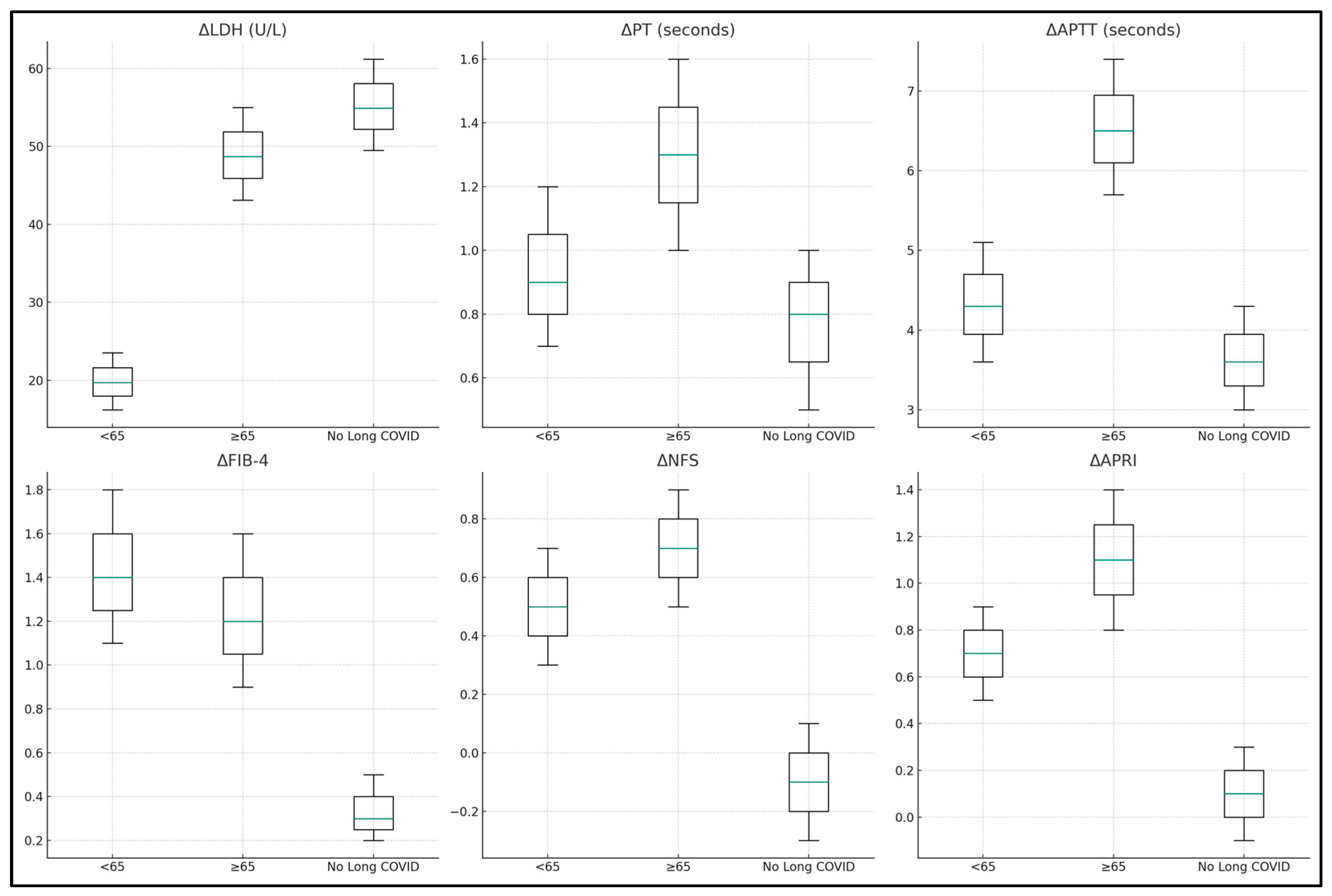
| Variables (Median-IQR) | Long COVID <65 Years (n = 117) | Long COVID ≥65 Years (n = 71) | No Long COVID (n = 50) | p-Value |
|---|---|---|---|---|
| ΔFasting glucose (mmol/L) | 13.2 (11.0–15.9) | 21.1 (18.6–24.3) | 14.7 (12.4–17.5) | <0.001 |
| ΔALT (U/L) | 12.0 (9.0–15.6) | 24.1 (19.7–29.4) | 18.9 (15.0–23.5) | <0.001 |
| ΔAST (U/L) | 19.4 (16.9–22.4) | 30.2 (26.6–34.1) | 18.4 (15.2–21.9) | <0.001 |
| ΔALP (U/L) | 17.6 (15.6–20.2) | 30.4 (27.6–33.9) | 33.0 (29.5–37.1) | <0.001 |
| ΔSerum albumin (g/dL) | −1.1 (−1.3–−0.9) | −1.2 (−1.4–−1.0) | −1.0 (−1.2–−0.8) | 0.092 |
| ΔTotal proteins (g/dL) | −0.5 (−0.7–−0.3) | −0.8 (−1.0–−0.6) | −0.5 (−0.7–−0.3) | 0.059 |
| ΔTotal bilirubin (g/dL) | 0.5 (0.3–0.7) | 0.8 (0.6–1.0) | 0.3 (0.1–0.5) | 0.034 |
| ΔGGT (U/L) | 8.9 (6.7–11.3) | 16.7 (13.9–19.8) | 6.9 (4.8–9.5) | <0.001 |
| ΔLDH (U/L) | 19.7 (16.2–23.5) | 48.7 (43.1–55.0) | 54.9 (49.5–61.2) | <0.001 |
| ΔPT (seconds) | 0.9 (0.7–1.2) | 1.3 (1.0–1.6) | 0.8 (0.5–1.0) | 0.009 |
| ΔAPTT (seconds) | 4.3 (3.6–5.1) | 6.5 (5.7–7.4) | 3.6 (3.0–4.3) | <0.001 |
| ΔFIB-4 | 1.4 (1.1–1.8) | 1.2 (0.9–1.6) | 0.3 (0.2–0.5) | 0.010 |
| ΔNFS | 0.5 (0.3–0.7) | 0.7 (0.5–0.9) | −0.1 (−0.3–0.1) | 0.041 |
| ΔAPRI | 0.7 (0.5–0.9) | 1.1 (0.8–1.4) | 0.1 (−0.1–0.3) | <0.001 |
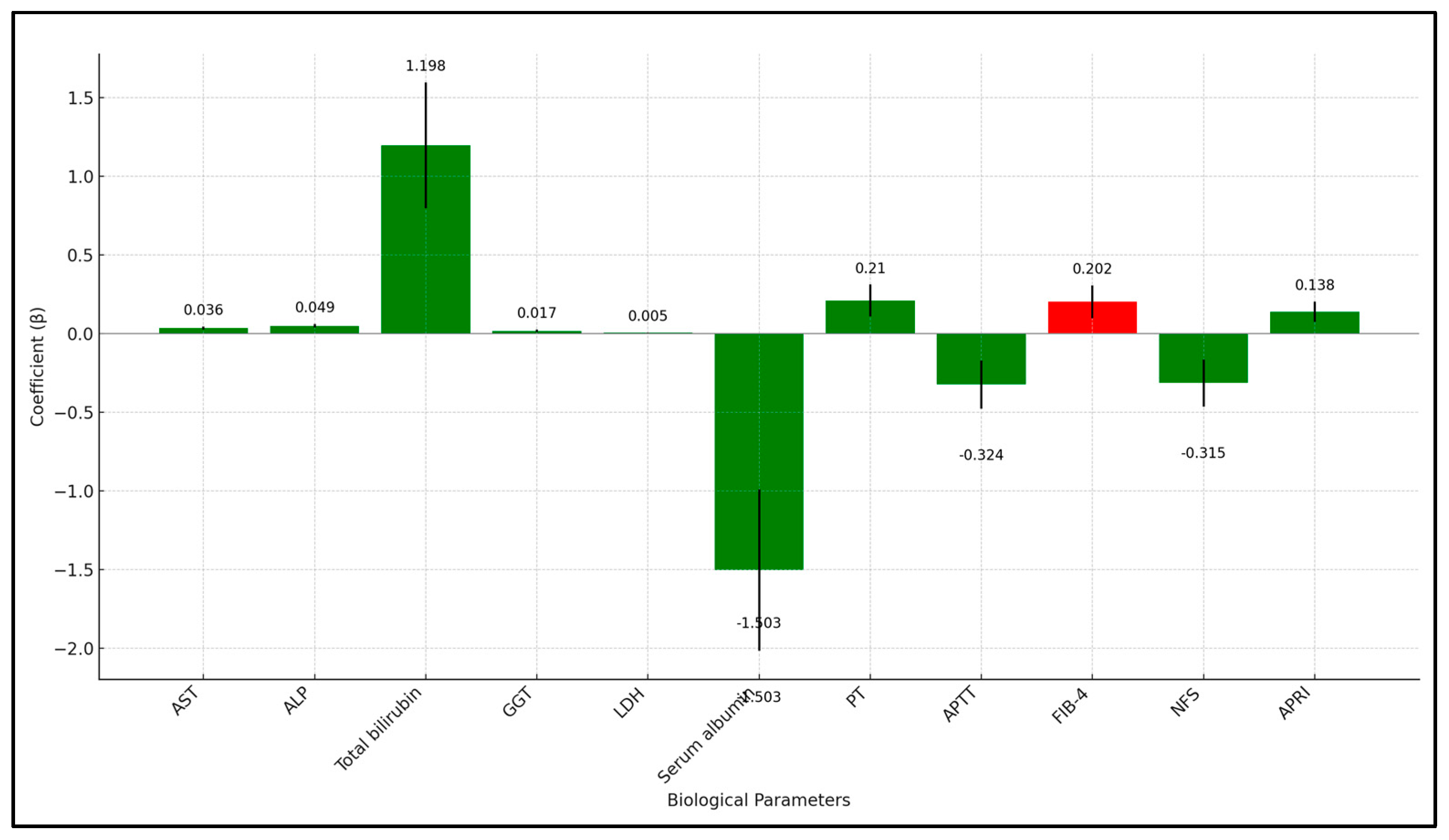
| Independent Variables | Coefficient (β) | Std. Error | p-Value | 95% CI |
|---|---|---|---|---|
| Demographic Factors | ||||
| Age (years) | 0.048 | 0.014 | <0.001 | [0.021, 0.075] |
| Gender (1 = Male, 0 = Female) | −0.107 | 0.192 | 0.558 | [−0.484, 0.270] |
| BMI (kg/m²) | 0.023 | 0.015 | 0.148 | [−0.007, 0.053] |
| Clinical Factors | ||||
| Smoking (1 = Yes, 0 = No) | 0.293 | 0.244 | 0.223 | [−0.186, 0.772] |
| Cardiovascular disease (1 = Yes, 0 = No) | 0.429 | 0.217 | 0.046 | [0.004, 0.854] |
| Chronic kidney disease (1 = Yes, 0 = No) | 0.574 | 0.307 | 0.069 | [−0.028, 1.176] |
| CCI score (≥2) | 0.149 | 0.074 | 0.041 | [0.004, 0.294] |
| Biological Parameters Change (Δ) | ||||
| AST (U/L) | 0.036 | 0.009 | <0.001 | [0.018, 0.054] |
| ALP (U/L) | 0.049 | 0.012 | <0.001 | [0.036, 0.075] |
| Total bilirubin (g/dL) | 1.198 | 0.400 | 0.003 | [0.413, 1.983] |
| GGT (U/L) | 0.017 | 0.007 | 0.028 | [0.003, 0.031] |
| LDH (U/L) | 0.005 | 0.002 | 0.012 | [0.001, 0.009] |
| Serum albumin (g/dL) | −1.503 | 0.513 | 0.005 | [−2.509, −0.497] |
| PT (seconds) | 0.210 | 0.101 | 0.037 | [0.012, 0.408] |
| APTT (seconds) | −0.324 | 0.153 | 0.034 | [−0.624, −0.024] |
| FIB-4 | 0.202 | 0.104 | 0.053 | [0.001, 0.403] |
| NFS | −0.315 | 0.150 | 0.032 | [−0.609, −0.021] |
| APRI | 0.138 | 0.065 | 0.038 | [0.010, 0.266] |
| Treatment Variables | ||||
| Oxygen supplementation (1 = Yes, 0 = No) | −0.140 | 0.203 | 0.489 | [−0.538, 0.258] |
| ICU admission (1 = Yes, 0 = No) | 0.483 | 0.235 | 0.042 | [0.022, 0.944] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bota, A.V.; Bratosin, F.; Bandi, S.S.S.; Bogdan, I.; Razvan, D.V.; Toma, A.-O.; Indries, M.F.; Csep, A.N.; Cotoraci, C.; Prodan, M.; et al. A Comparative Analysis of Liver Injury Markers in Post-COVID Syndrome among Elderly Patients: A Prospective Study. J. Clin. Med. 2024, 13, 1149. https://doi.org/10.3390/jcm13041149
Bota AV, Bratosin F, Bandi SSS, Bogdan I, Razvan DV, Toma A-O, Indries MF, Csep AN, Cotoraci C, Prodan M, et al. A Comparative Analysis of Liver Injury Markers in Post-COVID Syndrome among Elderly Patients: A Prospective Study. Journal of Clinical Medicine. 2024; 13(4):1149. https://doi.org/10.3390/jcm13041149
Chicago/Turabian StyleBota, Adrian Vasile, Felix Bratosin, Satya Sai Sri Bandi, Iulia Bogdan, David Vladut Razvan, Ana-Olivia Toma, Mirela Florica Indries, Andrei Nicolae Csep, Coralia Cotoraci, Mihaela Prodan, and et al. 2024. "A Comparative Analysis of Liver Injury Markers in Post-COVID Syndrome among Elderly Patients: A Prospective Study" Journal of Clinical Medicine 13, no. 4: 1149. https://doi.org/10.3390/jcm13041149
APA StyleBota, A. V., Bratosin, F., Bandi, S. S. S., Bogdan, I., Razvan, D. V., Toma, A. -O., Indries, M. F., Csep, A. N., Cotoraci, C., Prodan, M., Marc, F., Ignuta, F., & Marincu, I. (2024). A Comparative Analysis of Liver Injury Markers in Post-COVID Syndrome among Elderly Patients: A Prospective Study. Journal of Clinical Medicine, 13(4), 1149. https://doi.org/10.3390/jcm13041149