

Immediate Effect of Cryo-Compression Therapy on Biomechanical Properties and Perfusion of Forearm Muscles in Mixed Martial Arts Fighters

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.2.1. Measurements—Tissue Perfusion (PU)
2.2.2. Measurements—Myotonometry
2.2.3. Measurements—Pressure Pain Threshold (PPT)
2.2.4. Measurements—Maximum Forearm Muscle Strength (Fmax)
2.3. Statistical Methods
3. Results
4. Discussion
4.1. Perfusion
4.2. Biomechanical Properties
4.3. Muscle Pain
4.4. Isometric Muscular Strength
Limitations and Directions of Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, L.P.; Kelly, V.G.; Beckman, E.M. Periodization for Mixed Martial Arts. Strength Cond. J. 2013, 35, 34–45. [Google Scholar] [CrossRef]
- Andrade, A.; Flores, M.A.; Andreato, L.V.; Coimbra, D.R. Physical and training characteristics of mixed martial arts athletes: Systematic review. Strength Cond. J. 2019, 41, 51–63. [Google Scholar] [CrossRef]
- Zebrowska, A.; Trybulski, R.; Roczniok, R.; Marcol, W. Effect of Physical Methods of Lymphatic Drainage on Postexercise Recovery of Mixed Martial Arts Athletes. Clin. J. Sport Med. 2019, 29, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Holme, I. Risk factors for sports injuries—A methodological approach. Br. J. Sports Med. 2003, 37, 384–392. [Google Scholar] [CrossRef] [PubMed]
- Jensen, L.; Bangsbo, J.; Hellsten, Y. Effect of high intensity training on capillarization and presence of angiogenic factors in human skeletal muscle. J. Physiol. 2004, 557, 571–582. [Google Scholar] [CrossRef] [PubMed]
- Schaser, K.D.; Disch, A.C.; Stover, J.F.; Lauffer, A.; Bail, H.J.; Mittlmeier, T. Prolonged superficial local cryotherapy attenuates microcirculatory impairment, regional inflammation, and muscle necrosis after closed soft tissue injury in rats. Am. J. Sports Med. 2007, 35, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lu, H.; Li, S.; Zhang, Y.; Yan, F.; Huang, Y.; Chen, X.; Yang, A.; Han, L.; Ma, Y. Effect of cold and heat therapies on pain relief in patients with delayed onset muscle soreness: A network meta-analysis. J. Rehabil. Med. 2022, 54, 331. [Google Scholar] [CrossRef]
- Vieira Ramos, G.; Pinheiro, C.M.; Messa, S.P.; Delfino, G.B.; Marqueti, R.D.C.; Salvini, T.D.F.; Durigan, J.L.Q. Cryotherapy Reduces Inflammatory Response Without Altering Muscle Regeneration Process and Extracellular Matrix Remodeling of Rat Muscle. Sci. Rep. 2016, 6, 18525. [Google Scholar] [CrossRef]
- Trybulski, R.; Vovkanych, A.; Bas, O.; Tyravska, O. The low-temperature effect on sports regeneration. Fisioter. Mov. 2023, 36, e36204. [Google Scholar] [CrossRef]
- Myrer, J.W.; Draper, D.O.; Durrant, E. Contrast therapy and intramuscular temperature in the human leg. J. Athl. Train. 1994, 29, 318–322. [Google Scholar] [PubMed]
- Mumith, A.; Pavlou, P.; Barrett, M.; Thurston, B.; Garrett, S. Enhancing Postoperative Rehabilitation Following Knee Arthroplasty Using a New Cryotherapy Product: A Prospective Study. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 316. [Google Scholar] [CrossRef] [PubMed]
- Theurot, D.; Dugué, B.; Douzi, W.; Guitet, P.; Louis, J.; Dupuy, O. Impact of acute partial-body cryostimulation on cognitive performance, cerebral oxygenation, and cardiac autonomic activity. Sci. Rep. 2021, 11, 7793. [Google Scholar] [CrossRef] [PubMed]
- Knobloch, K.; Grasemann, R.; Jagodzinski, M.; Richter, M.; Zeichen, J.; Krettek, C. Changes of Achilles midportion tendon microcirculation after repetitive simultaneous cryotherapy and compression using a Cryo/Cuff. Am. J. Sports Med. 2006, 34, 1953–1959. [Google Scholar] [CrossRef]
- White, G.E.; Wells, G.D. Cold-water immersion and other forms of cryotherapy: Physiological changes potentially affecting recovery from high-intensity exercise. Extrem. Physiol. Med. 2013, 2, 26. [Google Scholar] [CrossRef]
- Hodges, G.J.; Johnson, J.M. Adrenergic control of the human cutaneous circulation. Appl. Physiol. Nutr. Metab. 2009, 34, 829–839. [Google Scholar] [CrossRef]
- Selkow, N.M.; Herman, D.C.; Liu, Z.; Hertel, J.; Hart, J.M.; Saliba, S.A. Microvascular perfusion increases after eccentric exercise of the gastrocnemius. J. Ultrasound Med. 2013, 32, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Nadler, S.; Weingand, K.; Kruse, R. The physiologic basis and clinical applications of cryotherapy and thermotherapy for the pain practitioner. Pain Physician 2004, 7, 395. [Google Scholar] [CrossRef]
- Kang, J.I.; Jeong, D.K.; Choi, H. Effects of microcurrent and cryotherapy on C-reactive protein levels andmuscle tone of patients with rotator cuff reconstruction. J. Phys. Ther. Sci. 2018, 30, 37. [Google Scholar] [CrossRef]
- Alaca, N.; Kablan, N. Acute effects of cold spray application on mechanical properties of the rectus femoris muscle in athletes. J. Bodyw. Mov. Ther. 2022, 30, 100–104. [Google Scholar] [CrossRef]
- French, D.N.; Thompson, K.G.; Garland, S.W.; Barnes, C.A.; Portas, M.D.; Hood, P.E.; Wilkes, G. The effects of contrast bathing and compression therapy on muscular performance. Med. Sci. Sports Exerc. 2008, 40, 1297–1306. [Google Scholar] [CrossRef]
- Dupont, W.H.; Meuris, B.J.; Hardesty, V.H.; Barnhart, E.C.; Tompkins, L.H.; Golden, M.J.P.; Usher, C.J.; Spence, P.A.; Caldwell, L.K.; Post, E.M.; et al. The effects combining cryocompression therapy following an acute bout of resistance exercise on performance and recovery. J. Sport. Sci. Med. 2017, 16, 333–342. [Google Scholar]
- Allan, R.; Malone, J.; Alexander, J.; Vorajee, S.; Ihsan, M.; Gregson, W.; Kwiecien, S.; Mawhinney, C. Cold for centuries: A brief history of cryotherapies to improve health, injury and post-exercise recovery. Eur. J. Appl. Physiol. 2022, 122, 1153. [Google Scholar] [CrossRef]
- Alexander, J.; Jeffery, J.; Rhodes, D. Recovery profiles of eccentric hamstring strength in response to cooling and compression. J. Bodyw. Mov. Ther. 2021, 27, 9–15. [Google Scholar] [CrossRef]
- Nabıyev, V.N.; Ayhan, S.; Adhıkarı, P.; Cetın, E.; Palaoglu, S.; Acaroglu, R.E. Cryo-Compression Therapy After Elective Spinal Surgery for Pain Management: A Cross-Sectional Study With Historical Control. Neurospine 2018, 15, 348–352. [Google Scholar] [CrossRef] [PubMed]
- Schinsky, M.F.; McCune, C.; Bonomi, J. Multifaceted Comparison of Two Cryotherapy Devices Used After Total Knee Arthroplasty: Cryotherapy Device Comparison. Orthop. Nurs. 2016, 35, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Hohenauer, E.; Taeymans, J.; Baeyens, J.P.; Clarys, P.; Clijsen, R. The Effect of Post-Exercise Cryotherapy on Recovery Characteristics: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0139028. [Google Scholar] [CrossRef] [PubMed]
- Swenson, C.; Swärd, L.; Karlsson, J. Cryotherapy in sports medicine. Scand. J. Med. Sci. Sports 1996, 6, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Szyguła, R.; Wierzbicka, M.; Sondel, G. Influence of 8-Week Aerobic Training on the Skin Microcirculation in Patients with Ischaemic Heart Disease. J. Aging Res. 2020, 2020, 4602067. [Google Scholar] [CrossRef] [PubMed]
- Albin, S.R.; Koppenhaver, S.L.; MacDonald, C.W.; Capoccia, S.; Ngo, D.; Phippen, S.; Pineda, R.; Wendlandt, A.; Hoffman, L.R. The effect of dry needling on gastrocnemius muscle stiffness and strength in participants with latent trigger points. J. Electromyogr. Kinesiol. 2020, 55, 102479. [Google Scholar] [CrossRef]
- Liana, R.; Chudański, M.; Katedra, I.P. Standarisation of laser Doppler flowmetry-own standards. Clin. Diabetol. 2009, 10, 58–64. [Google Scholar]
- Chen, G.; Wu, J.; Chen, G.; Lu, Y.; Ren, W.; Xu, W.; Xu, X.; Wu, Z.; Guan, Y.; Zheng, Y.; et al. Reliability of a portable device for quantifying tone and stiffness of quadriceps femoris and patellar tendon at different knee flexion angles. PLoS ONE 2019, 14, e0220521. [Google Scholar] [CrossRef] [PubMed]
- Kisilewicz, A.; Madeleine, P.; Ignasiak, Z.; Ciszek, B.; Kawczynski, A.; Larsen, R.G. Eccentric Exercise Reduces Upper Trapezius Muscle Stiffness Assessed by Shear Wave Elastography and Myotonometry. Front. Bioeng. Biotechnol. 2020, 8, 928. [Google Scholar] [CrossRef] [PubMed]
- Melo, A.S.C.; Cruz, E.B.; Vilas-Boas, J.P.; Sousa, A.S.P. Scapular Dynamic Muscular Stiffness Assessed through Myotonometry: A Narrative Review. Sensors 2022, 22, 2565. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, K.; Brandl, A.; Weber, P.; Wilke, J.; Bensamoun, S.F.; Bauermeister, W.; Klingler, W.; Schleip, R. Assessing reliability and validity of different stiffness measurement tools on a multi-layered phantom tissue model. Sci. Rep. 2023, 13, 815. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.N.; Li, Y.P.; Liu, C.L.; Zhang, Z.J. Assessing the elastic properties of skeletal muscle and tendon using shearwave ultrasound elastography and MyotonPRO. Sci. Rep. 2018, 8, 17064. [Google Scholar] [CrossRef] [PubMed]
- Park, G.; Kim, C.W.; Park, S.B.; Kim, M.J.; Jang, S.H. Reliability and Usefulness of the Pressure Pain Threshold Measurement in Patients with Myofascial Pain. Ann. Rehabil. Med. 2011, 35, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Hohenauer, E.; Costello, J.T.; Stoop, R.; Küng, U.M.; Clarys, P.; Deliens, T.; Clijsen, R. Cold-water or partial-body cryotherapy? Comparison of physiological responses and recovery following muscle damage. Scand. J. Med. Sci. Sport. 2018, 28, 1252–1262. [Google Scholar] [CrossRef]
- Nogueira, N.M.; Felappi, C.J.; Lima, C.S.; Medeiros, D.M. Effects of local cryotherapy for recovery of delayed onset muscle soreness and strength following exercise-induced muscle damage: Systematic review and meta-analysis. Sport Sci. Health 2020, 16, 1–11. [Google Scholar] [CrossRef]
- Bieles, J.S.; Bruce, S.A.; Newham, D.J.; Green, D.A. Dorsiflexion But Not Plantarflexion Force Declines At Lower Foot Skin Temperatures. Int. J. Ther. Rehabil. 2019, 26, 13. [Google Scholar] [CrossRef]
- Otte, J.W.; Merrick, M.A.; Ingersoll, C.D.; Cordova, M.L. Subcutaneous adipose tissue thickness alters cooling time during cryotherapy. Arch. Phys. Med. Rehabil. 2002, 83, 1501–1505. [Google Scholar] [CrossRef]
- Khoshnevis, S.; Craik, N.K.; Diller, K.R. Cold-induced vasoconstriction may persist long after cooling ends: An evaluation of multiple cryotherapy units. Knee Surg. Sports Traumatol. Arthrosc. 2015, 23, 2475–2483. [Google Scholar] [CrossRef]
- Karunakara, R.G.; Lephart, S.M.; Pincivero, D.M. Changes in forearm blood flow during single and intermittent cold application. J. Orthop. Sports Phys. Ther. 1999, 29, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Wegmann, M.; Faude, O.; Poppendieck, W.; Hecksteden, A.; Fröhlich, M.; Meyer, T. Pre-Cooling and sports performance: A meta-analytical review. Sport. Med. 2012, 42, 545–564. [Google Scholar] [CrossRef] [PubMed]
- Petersen, A.C.; Fyfe, J.J. Post-exercise Cold Water Immersion Effects on Physiological Adaptations to Resistance Training and the Underlying Mechanisms in Skeletal Muscle: A Narrative Review. Front. Sport. Act. Living 2021, 3, 660291. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, C.M.; Costello, J.T. Do thermal agents affect range of movement and mechanical properties in soft tissues? A systematic review. Arch. Phys. Med. Rehabil. 2013, 94, 149–163. [Google Scholar] [CrossRef]
- Kalli, K.; Fousekis, K. The effects of cryotherapy on athletes’ muscle strength, flexibility, and neuromuscular control: A systematic review of the literature. J. Bodyw. Mov. Ther. 2020, 24, 175–188. [Google Scholar] [CrossRef]
- Abaïdia, A.E.; Lamblin, J.; Delecroix, B.; Leduc, C.; McCall, A.; Nédélec, M.; Dawson, B.; Baquet, G.; Dupont, G. Recovery from exercise-induced muscle damage: Cold-water immersion versus whole-body cryotherapy. Int. J. Sports Physiol. Perform. 2017, 12, 402–409. [Google Scholar] [CrossRef]
- Albracht, K.; Arampatzis, A. Exercise-induced changes in triceps surae tendon stiffness and muscle strength affect running economy in humans. Eur. J. Appl. Physiol. 2013, 113, 1605–1615. [Google Scholar] [CrossRef]
- Bohm, S.; Mersmann, F.; Santuz, A.; Arampatzis, A. Enthalpy efficiency of the soleus muscle contributes to improvements in running economy. Proceedings. Biol. Sci. 2021, 288, 20202784. [Google Scholar] [CrossRef]
- Morgan, D.L. Separation of active and passive components of short-range stiffness of muscle. Am. J. Physiol. 1977, 232, 45–49. [Google Scholar] [CrossRef]
- Konrad, A.; Tilp, M.; Mehmeti, L.; Mahnič, N.; Seiberl, W.; Paternoster, F.K. The Relationship Between Lower Limb Passive Muscle and Tendon Compression Stiffness and Oxygen Cost During Running. J. Sports Sci. Med. 2023, 22, 28–35. [Google Scholar] [CrossRef]
- Mac Auley, D.C. Ice therapy: How good is the evidence? Int. J. Sports Med. 2001, 22, 379–384. [Google Scholar] [CrossRef]
- Sleboda, D.A.; Wold, E.S.; Roberts, T.J. Passive muscle tension increases in proportion to intramuscular fluid volume. J. Exp. Biol. 2019, 222, jeb209668. [Google Scholar] [CrossRef] [PubMed]
- Sleboda, D.A.; Roberts, T.J. Incompressible fluid plays a mechanical role in the development of passive muscle tension. Biol. Lett. 2017, 13, 20160630. [Google Scholar] [CrossRef] [PubMed]
- Joyner, M.J.; Casey, D.P. Regulation of increased blood flow (hyperemia) to muscles during exercise: A hierarchy of competing physiological needs. Physiol. Rev. 2015, 95, 549–601. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.W.; Tsai, H.Y.; Lin, F.S.; Lin, Y.H.; Chiang, C.Y.; Lu, Z.L.; Tseng, M.T. Effects of positive and negative expectations on human pain perception engage separate but interrelated and dependently regulated cerebral mechanisms. J. Neurosci. 2019, 39, 1261–1274. [Google Scholar] [CrossRef] [PubMed]
- Jepma, M.; Koban, L.; van Doorn, J.; Jones, M.; Wager, T.D. Behavioural and neural evidence for self-reinforcing expectancy effects on pain. Nat. Hum. Behav. 2018, 2, 838–855. [Google Scholar] [CrossRef] [PubMed]
- Gatewood, C.T.; Tran, A.A.; Dragoo, J.L. The efficacy of post-operative devices following knee arthroscopic surgery: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 501–516. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.G.; Brown, J.N.; Hammond, J.M. Cryotherapy for the prevention of chemotherapy-induced peripheral neuropathy: A systematic review. J. Oncol. Pharm. Pract. 2021, 27, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Bleakley, C.M.; McDonough, S.M.; MacAuley, D.C. Cryotherapy for acute ankle sprains: A randomised controlled study of two different icing protocols. Br. J. Sports Med. 2006, 40, 700–705. [Google Scholar] [CrossRef]
- Block, J.E. Cold and compression in the management of musculoskeletal injuries and orthopedic operative procedures: A narrative review. Open Access J. Sport. Med. 2010, 1, 105. [Google Scholar] [CrossRef] [PubMed]
- Shibaguchi, T.; Hoshi, M.; Yoshihara, T.; Naito, H.; Goto, K.; Yoshioka, T.; Sugiura, T. Impact of different temperature stimuli on the expression of myosin heavy chain isoforms during recovery from bupivacaine-induced muscle injury in rats. J. Appl. Physiol. 2019, 127, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Tomchuk, D.; Rubley, M.D.; Holcomb, W.R.; Guadagnoli, M.; Tarno, J.M. The magnitude of tissue cooling during cryotherapy with varied types of compression. J. Athl. Train. 2010, 45, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Ostrowski, J.; Purchio, A.; Beck, M.; Leisinger, J.L. Effectiveness of Salted Ice Bag Versus Cryocompression on Decreasing Intramuscular and Skin Temperature. J. Sport Rehabil. 2019, 28, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, J.; Shurtz, J.; Spears, C. Traditional Cryotherapy Treatments are More Effective than Game Ready® on Medium Setting at Decreasing Sinus Tarsi Tissue Temperatures in Uninjured Subjects. J. Athl. Enhanc. 2012, 1, 1–5. [Google Scholar] [CrossRef]
- Holwerda, S.W.; Trowbridge, C.A.; Womochel, K.S.; Keller, D.M. Effects of cold modality application with static and intermittent pneumatic compression on tissue temperature and systemic cardiovascular responses. Sports Health 2013, 5, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Ohnishi, N.; Yamane, M.; Uchiyama, N.; Shirasawa, S.; Kosaka, M.; Shiono, H.; Okada, T. Adaptive changes in muscular performance and circulation by resistance training with regular cold application. J. Therm. Biol. 2004, 29, 839–843. [Google Scholar] [CrossRef]
- Aoki, H.; O’Hata, N.; Kohno, T.; Morikawa, T.; Seki, J. A 15-year prospective epidemiological account of acute traumatic injuries during official professional soccer league matches in Japan. Am. J. Sports Med. 2012, 40, 1006–1014. [Google Scholar] [CrossRef]
- Taber, C.B.; Vigotsky, A.; Nuckols, G.; Haun, C.T. Exercise-Induced Myofibrillar Hypertrophy is a Contributory Cause of Gains in Muscle Strength. Sports Med. 2019, 49, 993–997. [Google Scholar] [CrossRef]
- Broatch, J.R.; Petersen, A.; Bishop, D.J. Cold-water immersion following sprint interval training does not alter endurance signaling pathways or training adaptations in human skeletal muscle. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2017, 313, R372–R384. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, C.J.; Kouw, I.W.K.; Churchward-Venne, T.A.; Smeets, J.S.J.; Senden, J.M.; van Marken Lichtenbelt, W.D.; Verdijk, L.B.; van Loon, L.J.C. Postexercise cooling impairs muscle protein synthesis rates in recreational athletes. J. Physiol. 2020, 598, 755–772. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
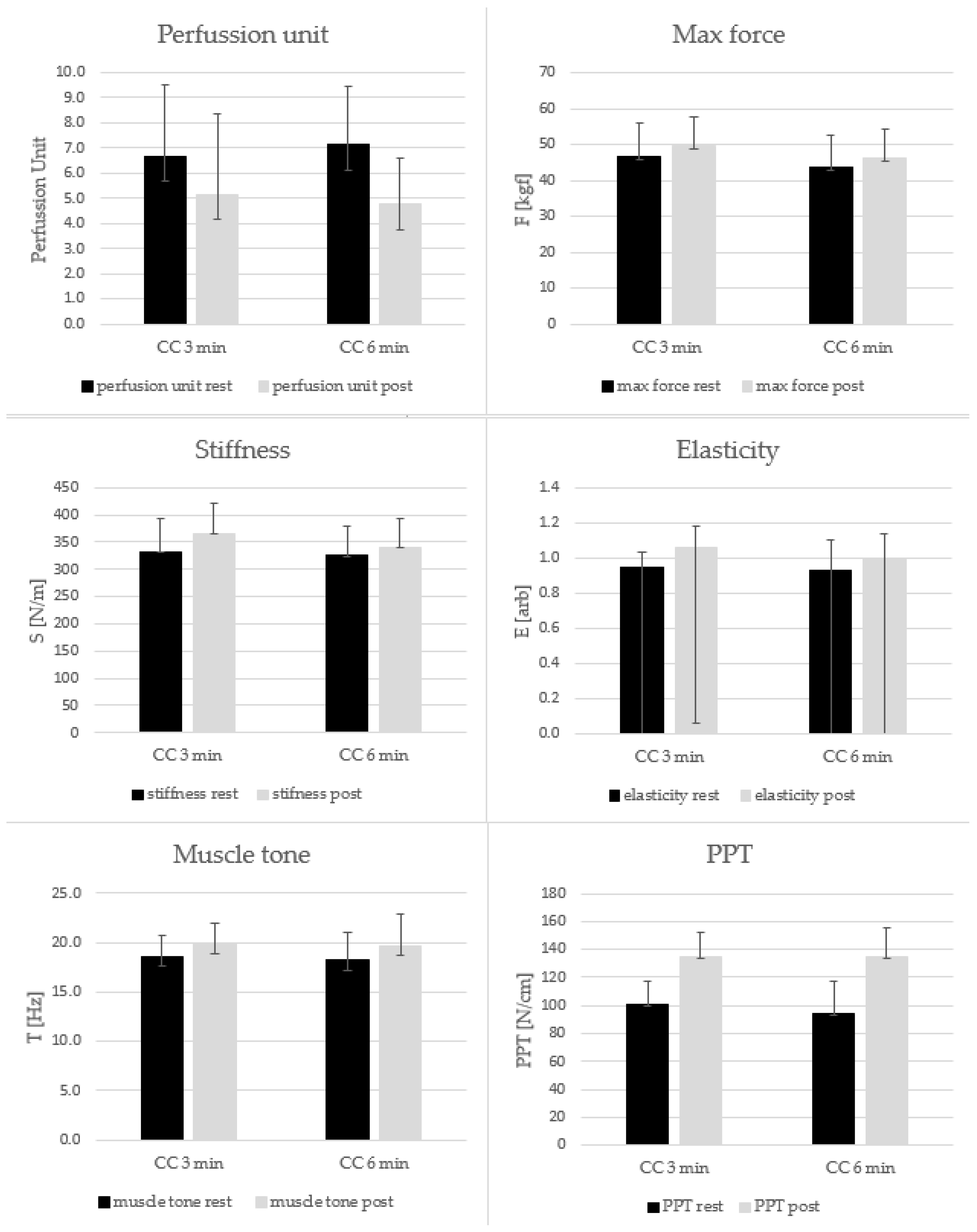
| Condition | Rest | Post |
|---|---|---|
| Perfusion Unit | ||
| CC3 | 6.67 ± 2.84 (5.34 to 8.00) | 5.15 ± 2.34 (4.05 to 6.24) |
| CC6 | 7.13 ± 3.21 (5.62 to 8.63) | 4.76 ± 1.82 (3.91 to 5.61) |
| Maximum forearm muscle strength [kgf] | ||
| CC3 | 46.61 ± 9.18 (42.31 to 50.91) | 49.55 ± 8.85 (45.41 to 53.69) |
| CC6 | 43.74 ± 8.07 (39.96 to 47.51) | 46.20 ± 8.04 (42.44 to 49.96) |
| Muscle Tone [Hz] | ||
| CC3 | 18.58 ± 2.06 (17.61 to 19.54) | 19.90 ± 2.79 (18.59 to 21.20) |
| CC6 | 18.19 ± 1.98 (17.26 to 19.11) | 19.66 ± 3.27 (18.13 to 21.19) |
| Stiffness [N/m] | ||
| CC3 | 332.5 ± 60.7 (304.1 to 360.9) | 366.2 ± 54.4 (340.7 to 391.6) |
| CC6 | 325.2 ± 55.0 (299.4 to 350.9) | 339.6 ± 53.2 (314.6 to 364.5) |
| Elasticity [arb] | ||
| CC3 | 0.95 ± 0.08 (0.92 to 0.99) | 1.06 ± 0.17 (0.98 to 1.14) |
| CC6 | 0.93 ± 0.12 (0.87 to 0.99) | 1.00 ± 0.14 (0.93 to 1.07) |
| Pressure pain threshold [N/cm] | ||
| CC3 | 101.1 ± 16.0 (93.6 to 108.6) | 134.6 ± 23.3 (123.7 to 145.5) |
| CC6 | 94.1 ± 18.0 (85.6 to 102.5) | 135.0 ± 21.0 (125.2 to 144.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trybulski, R.; Kużdżał, A.; Bichowska-Pawęska, M.; Vovkanych, A.; Kawczyński, A.; Biolik, G.; Muracki, J. Immediate Effect of Cryo-Compression Therapy on Biomechanical Properties and Perfusion of Forearm Muscles in Mixed Martial Arts Fighters. J. Clin. Med. 2024, 13, 1177. https://doi.org/10.3390/jcm13041177
Trybulski R, Kużdżał A, Bichowska-Pawęska M, Vovkanych A, Kawczyński A, Biolik G, Muracki J. Immediate Effect of Cryo-Compression Therapy on Biomechanical Properties and Perfusion of Forearm Muscles in Mixed Martial Arts Fighters. Journal of Clinical Medicine. 2024; 13(4):1177. https://doi.org/10.3390/jcm13041177
Chicago/Turabian StyleTrybulski, Robert, Adrian Kużdżał, Marta Bichowska-Pawęska, Andriy Vovkanych, Adam Kawczyński, Grzegorz Biolik, and Jarosław Muracki. 2024. "Immediate Effect of Cryo-Compression Therapy on Biomechanical Properties and Perfusion of Forearm Muscles in Mixed Martial Arts Fighters" Journal of Clinical Medicine 13, no. 4: 1177. https://doi.org/10.3390/jcm13041177
APA StyleTrybulski, R., Kużdżał, A., Bichowska-Pawęska, M., Vovkanych, A., Kawczyński, A., Biolik, G., & Muracki, J. (2024). Immediate Effect of Cryo-Compression Therapy on Biomechanical Properties and Perfusion of Forearm Muscles in Mixed Martial Arts Fighters. Journal of Clinical Medicine, 13(4), 1177. https://doi.org/10.3390/jcm13041177