
Extra-Corporeal Membrane Oxygenation in Pregnancy

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussions
4.1. Indications for ECMO Support
4.2. What Does the ECMO Circuit Consist of?
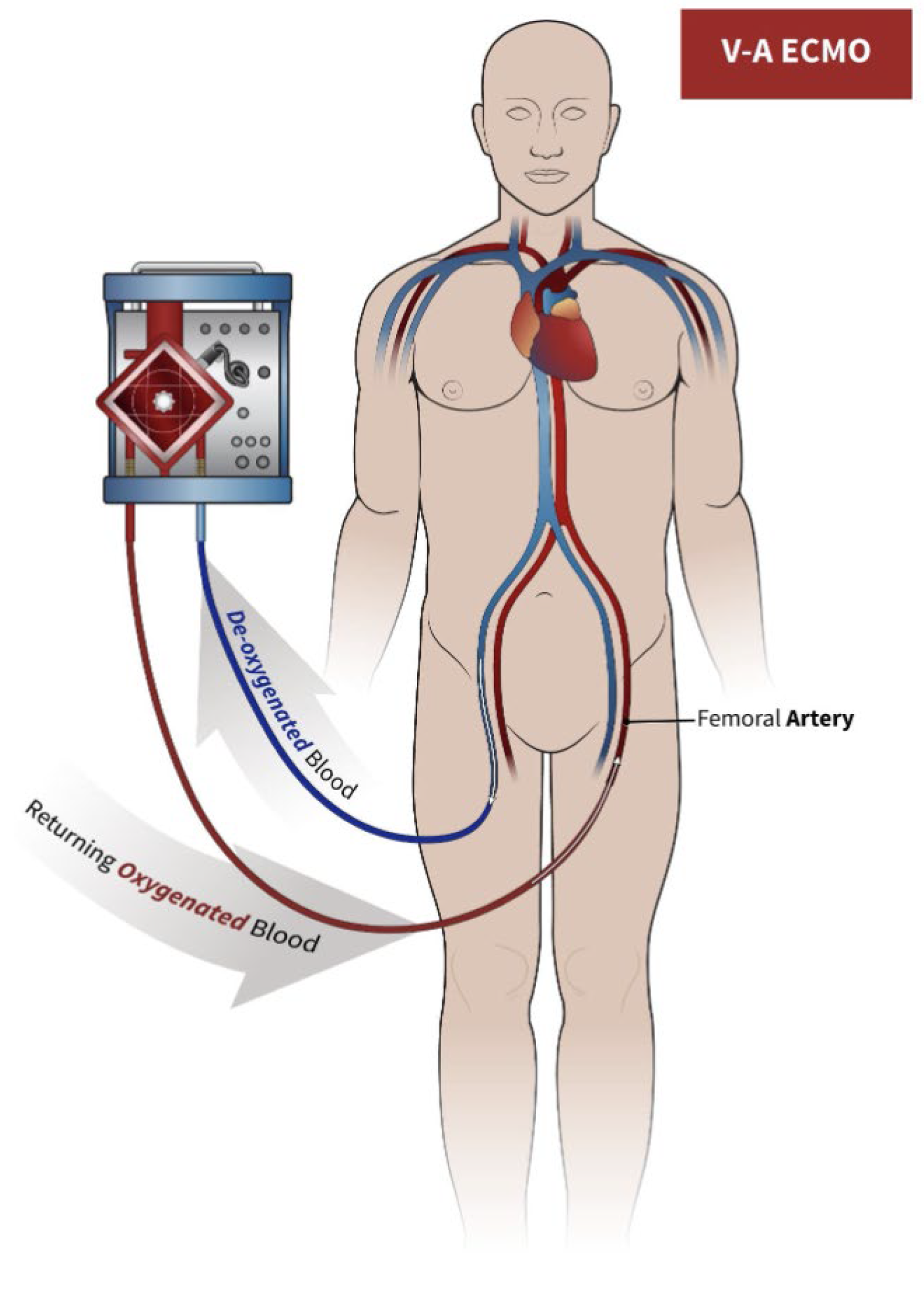
4.2.1. Veno-Arterial ECMO
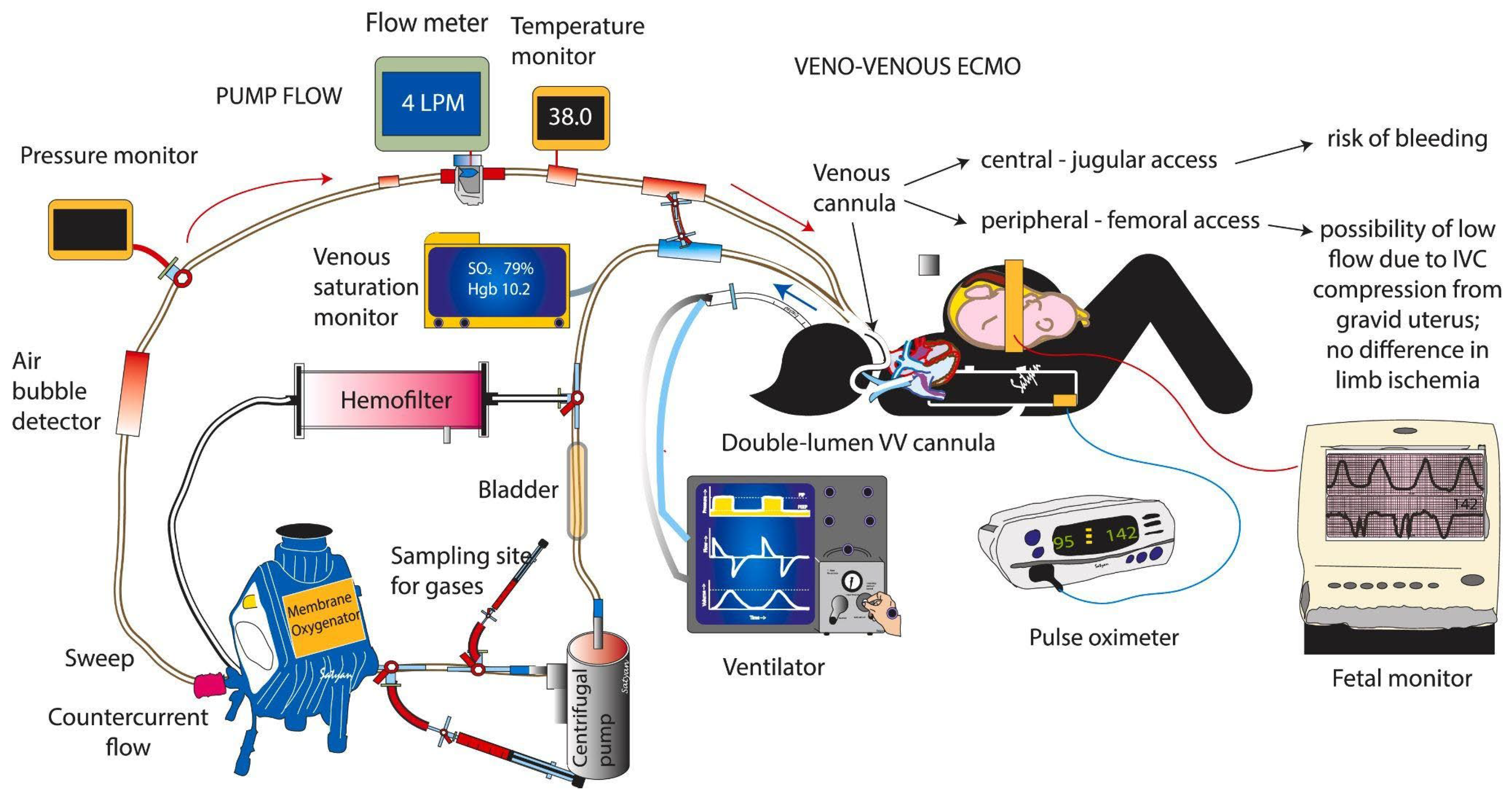
4.2.2. Veno-Venous ECMO
4.3. Weaning from ECMO
4.4. Complications & Contraindications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Makdisi, G.; Wang, I.-W. Extra Corporeal Membrane Oxygenation (ECMO) review of a lifesaving technology. J. Thorac. Dis. 2015, 7, E166–E176. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Dietl, C.A.; Coleman, D.M. Extracorporeal life support during pregnancy. J. Thorac. Cardiovasc. Surg. 2016, 151, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Frenckner, B. Extracorporeal membrane oxygenation: A breakthrough for respiratory failure. J. Intern. Med. 2015, 278, 586–598. [Google Scholar] [CrossRef]
- Pacheco, L.D.; Shamshirsaz, A.A. Extracorporeal Membrane Oxygenation During Pregnancy. Clin. Obstet. Gynecol. 2023, 66, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.S.; Wille, K.M.; Bellot, S.C.; Diaz-Guzman, E. Modern Use of Extracorporeal Life Support in Pregnancy and Postpartum. ASAIO J. 2015, 61, 110–114. [Google Scholar] [CrossRef]
- Palella, S.; Muscarà, L.; La Via, L.; Sanfilippo, F. Veno-venous extracorporeal membrane oxygenation for rescue support in pregnant patients with COVID-19: A systematic review. Br. J. Anaesth. 2023, 131, e130–e132. [Google Scholar] [CrossRef]
- Racca, F.; Longhitano, Y.; Zanza, C.; Balzanelli, M.G.; Draisci, G.; Stoia, P.A.; Gollo, E.; Maio, M.; Grattarola, C.; Astuto, M.; et al. Peri-partum respiratory management of pregnant women with neuro-muscular disorders: A prospective observational study (IT-NEUMA-Pregn study). BMC Anesthesiol. 2023, 23, 342. [Google Scholar] [CrossRef]
- Byrne, J.J.; Shamshirsaz, A.A.; Cahill, A.G.; Turrentine, M.A.; Seasely, A.R.; Eid, J.; Rouse, C.E.; Richley, M.; Raghuraman, N.; Naqvi, M.; et al. Outcomes Following Extracorporeal Membrane Oxygenation for Severe COVID-19 in Pregnancy or Post Partum. JAMA Netw. Open 2023, 6, e2314678. [Google Scholar] [CrossRef]
- Koons, B.; Siebert, J. Extracorporeal Membrane Oxygenation as a Bridge to Lung Transplant: Considerations for Critical Care Nursing Practice. Crit. Care Nurse 2020, 40, 49–57. [Google Scholar] [CrossRef]
- Dutta, S.; Hirani, S.; Heda, A.; Shaikh, M.Y.D.; Washani, S.; Hirani, S.; Prasad, R.; Wanjari, M. Extracorporeal Membrane Oxygenation (ECMO): A Lifeline for Pregnant and Postpartum Women. Cureus 2023, 15, e43586. [Google Scholar] [CrossRef] [PubMed]
- Banfi, C.; Pozzi, M.; Siegenthaler, N.; Brunner, M.-E.; Tassaux, D.; Obadia, J.-F.; Bendjelid, K.; Giraud, R. Veno-venous extracorporeal membrane oxygenation: Cannulation techniques. J. Thorac. Dis. 2016, 8, 3762–3773. [Google Scholar] [CrossRef]
- Vyas, A.; Bishop, M.A. Extracorporeal Membrane Oxygenation in Adults. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Pavlushkov, E.; Berman, M.; Valchanov, K. Cannulation techniques for extracorporeal life support. Ann. Transl. Med. 2017, 5, 70. [Google Scholar] [CrossRef] [PubMed]
- James, S.A.; Guervilly, C.; Lesouhaitier, M.; Coppens, A.; Haddadi, C.; Lebreton, G.; Nizard, J.; Brechot, N.; Assouline, B.; Saura, O.; et al. Delivery decision in pregnant women rescued by ECMO for severe ARDS: A retrospective multicenter cohort study. Crit. Care 2022, 26, 312. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.; Shiloh, A.L.; Carlese, A. Monitoring of the Adult Patient on Venoarterial Extracorporeal Membrane Oxygenation. Sci. World J. 2014, 2014, 393258. [Google Scholar] [CrossRef] [PubMed]
- Pandya, S.T.; Krishna, S.J. Acute Respiratory Distress Syndrome in Pregnancy. Indian J. Crit. Care Med. 2021, 25, S241–S247. [Google Scholar] [CrossRef] [PubMed]
- Sukhal, S.; Sethi, J.; Ganesh, M.; Villablanca, P.; Malhotra, A.; Ramakrishna, H. Extracorporeal membrane oxygenation in severe influenza infection with respiratory failure: A systematic review and meta-analysis. Ann. Card. Anaesth. 2017, 20, 14–21. [Google Scholar] [CrossRef]
- Kakar, V.; Ahmed, I.; Ahmed, W.; Raposo, N.; Kumar, G.P. Peripartum veno-venous extracorporeal membrane oxygenation in patients with severe CoViD-19-related-ARDS. Perfusion 2024, 39, 426–432. [Google Scholar] [CrossRef]
- Urriago-Osorio, G.A.; Melo-Burbano, L.; Berghe, J.L.-V.D.; Muñoz-Córdoba, A.M.; Daza-Arana, J.E.; Contreras-Zúñiga, E. Pulmonary Thromboembolism in Pregnancy: A Case Report and Literature Review. Open Access Emerg. Med. 2023, 15, 217–225. [Google Scholar] [CrossRef]
- Zanza, C.; Saglietti, F.; Tesauro, M.; Longhitano, Y.; Savioli, G.; Balzanelli, M.G.; Romenskaya, T.; Cofone, L.; Pindinello, I.; Racca, G.; et al. Cardiogenic Pulmonary Edema in Emergency Medicine. Adv. Respir. Med. 2023, 91, 445–463. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.T.; Solnordal, C.B. Acute pulmonary oedema in pregnant women. Anaesthesia 2012, 67, 646–659. [Google Scholar] [CrossRef]
- Magley, M.; Hinson, M.R. Eclampsia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar] [PubMed]
- Velayudhareddy, S.; Kirankumar, H. Management of foetal asphyxia by intrauterine foetal resuscitation. Indian J. Anaesth. 2010, 54, 394–399. [Google Scholar] [CrossRef]
- Allen, K.A.; Brandon, D.H. Hypoxic Ischemic Encephalopathy: Pathophysiology and Experimental Treatments. Newborn Infant Nurs. Rev. 2011, 11, 125–133. [Google Scholar] [CrossRef]
- Borse, V.; Shanks, A.L. Twin-to-Twin Transfusion Syndrome. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Brogan, T.V.; Lequier, L.; Lorusso, R.; MacLaren, G.; Peek, G. Extracorporeal Life Support: The ELSO Red Book; AbeBooks: Victoria, BC, USA, 2017. [Google Scholar]
- Combes, A.; Hajage, D.; Capellier, G.; Demoule, A.; Lavoué, S.; Guervilly, C.; Da Silva, D.; Zafrani, L.; Tirot, P.; Veber, B.; et al. Extracorporeal Membrane Oxygenation for Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2018, 378, 1965–1975. [Google Scholar] [CrossRef]
- Richley, M.; Rao, R. Extracorporeal membrane oxygenation in pregnancy during the SARS-CoV-2 pandemic. Semin. Fetal Neonatal Med. 2023, 28, 101435. [Google Scholar] [CrossRef]
- Donker, D.W.; Brodie, D.; Henriques, J.P.S.; Broomé, M. Left Ventricular Unloading During Veno-Arterial ECMO: A Simulation Study. ASAIO J. 2019, 65, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Magon, F.; Longhitano, Y.; Savioli, G.; Piccioni, A.; Tesauro, M.; Del Duca, F.; Napoletano, G.; Volonnino, G.; Maiese, A.; La Russa, R.; et al. Point-of-Care Ultrasound (POCUS) in Adult Cardiac Arrest: Clinical Review. Diagnostics 2024, 14, 434. [Google Scholar] [CrossRef] [PubMed]
- Nair, P.; Davies, A.R.; Beca, J.; Bellomo, R.; Ellwood, D.; Forrest, P.; Jackson, A.; Pye, R.; Seppelt, I.; Sullivan, E.; et al. Extracorporeal membrane oxygenation for severe ARDS in pregnant and postpartum women during the 2009 H1N1 pandemic. Intensive Care Med. 2011, 37, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Park, J.H.; Jang, J.H.; Kim, S.H.; Hong, S.Y.; Heo, W.; Lee, D.-H.; Choi, H.S.; Kim, K.H.; Jang, H.-J. The role of nafamostat mesilate as a regional anticoagulant during extracorporeal membrane oxygenation. Acute Crit. Care 2022, 37, 177–184. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, F.; La Via, L.; Murabito, P.; Pappalardo, F.; Astuto, M. More evidence available for the use of Bivalirudin in patients supported by extracorporeal membrane oxygenation. Thromb. Res. 2022, 211, 148–149. [Google Scholar] [CrossRef] [PubMed]
- Granja, T.; Hohenstein, K.; Schüssel, P.; Fischer, C.; Prüfer, T.; Schibilsky, D.; Wendel, H.P.; Jaschonek, K.; Serna-Higuita, L.; Schlensak, C.; et al. Multi-Modal Characterization of the Coagulopathy Associated with Extracorporeal Membrane Oxygenation. Crit. Care Med. 2020, 48, e400–e408. [Google Scholar] [CrossRef] [PubMed]
- Shoskes, A.D.; Migdady, I.; Rice, C.; Hassett, C.D.; Deshpande, A.; Price, C.M.; Hernandez, A.V.; Cho, S.-M.D. Brain Injury Is More Common in Venoarterial Extracorporeal Membrane Oxygenation Than Venovenous Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-Analysis. Crit. Care Med. 2020, 48, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Pasrija, C.; Bedeir, K.; Jeudy, J.; Kon, Z.N. Harlequin Syndrome during Venoarterial Extracorporeal Membrane Oxygenation. Radiol. Cardiothorac. Imaging 2019, 1, e190031. [Google Scholar] [CrossRef]
- Zhang, J.J.Y.; Ong, J.A.-H.; Syn, N.L.; Lorusso, R.; Tan, C.S.; MacLaren, G.; Ramanathan, K. Extracorporeal Membrane Oxygenation in Pregnant and Postpartum Women: A Systematic Review and Meta-Regression Analysis. J. Intensive Care Med. 2021, 36, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Ong, J.; Zhang, J.; Lorusso, R.; MacLaren, G.; Ramanathan, K. Extracorporeal membrane oxygenation in pregnancy and the postpartum period: A systematic review of case reports. Int. J. Obstet. Anesth. 2020, 43, 106–113. [Google Scholar] [CrossRef]
- Naoum, E.E.; Chalupka, A.; Haft, J.; MacEachern, M.; Vandeven, C.J.M.; Easter, S.R.; Maile, M.; Bateman, B.T.; Bauer, M.E. Extracorporeal Life Support in Pregnancy: A Systematic Review. J. Am. Heart Assoc. 2020, 9, e016072. [Google Scholar] [CrossRef]
- Saad, A.F.; Rahman, M.; Maybauer, D.M.; Fraser, J.F.; Costantine, M.M.; Pacheco, L.D.; Maybauer, M.O. Extracorporeal Membrane Oxygenation in Pregnant and Postpartum Women with H1N1-Related Acute Respiratory Distress Syndrome: A Systematic Review and Meta-analysis. Obstet. Gynecol. 2016, 127, 241–247. [Google Scholar] [CrossRef]
- Conti, E.; Cascio, N.D.; Paluan, P.; Racca, G.; Longhitano, Y.; Savioli, G.; Tesauro, M.; Leo, R.; Racca, F.; Zanza, C. Pregnancy Arrhythmias: Management in the Emergency Department and Critical Care. J. Clin. Med. 2024, 13, 1095. [Google Scholar] [CrossRef]
- Pacheco, L.D.; Saade, G.R.; Hankins, G.D. Extracorporeal membrane oxygenation (ECMO) during pregnancy and postpartum. Semin. Perinatol. 2018, 42, 21–25. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Maternal Indication | Cardiogenic Shock | Acute Respiratory Distress | Eclampsia | Pulmonary Embolism |
| Fetal Indication | Twin to Twin Transfusion Syndrome | Hypoxic- Hischemic encephalopaty | Fetal Distress |
| Indications for Veno-Venous-Extra Corporeal Membrane Oxygenation Support during Pregnancy in Case of Respiratory Failure/Acute Respiratory Distress Syndrome |
|---|
|
| Bleeding | Due to “ECMO-Associated Coagulopathy” the Etiology Is Multifactorial, Including Anticoagulation, Thrombocytopenia and Acquired Von Willebrand Disease |
|---|---|
| Infection | Should be administered a prophylactic antibiotic (low evidence). |
| Thrombo- cytopenia | The goal is to maintain hemoglobin above 7 to 8 g/dL and platelets above >50,000/mm3. |
| Neurological complications | Ischemic and hemorrhagic strokes and anoxic brain injury. It is more common in Veno-Arterial Extra Corporeal Membrane Oxygenation than in Veno-Venous Extra Corporeal Membrane Oxygenation (19% vs. 11%, respectively). |
| Harlequin syndrome | Regional changes in skin coloration, with cyanosis of the upper portions of the body and a pinkish complexion of the lower regions. |
| Thrombosis of ECMO circuit | Can be prevented with systemic anticoagulation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romenskaya, T.; Longhitano, Y.; Mahajan, A.; Savioli, G.; Voza, A.; Tesauro, M.; Zanza, C. Extra-Corporeal Membrane Oxygenation in Pregnancy. J. Clin. Med. 2024, 13, 1634. https://doi.org/10.3390/jcm13061634
Romenskaya T, Longhitano Y, Mahajan A, Savioli G, Voza A, Tesauro M, Zanza C. Extra-Corporeal Membrane Oxygenation in Pregnancy. Journal of Clinical Medicine. 2024; 13(6):1634. https://doi.org/10.3390/jcm13061634
Chicago/Turabian StyleRomenskaya, Tatsiana, Yaroslava Longhitano, Aman Mahajan, Gabriele Savioli, Antonio Voza, Manfredi Tesauro, and Christian Zanza. 2024. "Extra-Corporeal Membrane Oxygenation in Pregnancy" Journal of Clinical Medicine 13, no. 6: 1634. https://doi.org/10.3390/jcm13061634
APA StyleRomenskaya, T., Longhitano, Y., Mahajan, A., Savioli, G., Voza, A., Tesauro, M., & Zanza, C. (2024). Extra-Corporeal Membrane Oxygenation in Pregnancy. Journal of Clinical Medicine, 13(6), 1634. https://doi.org/10.3390/jcm13061634