


Parenteral Anticoagulation at First Medical Contact Improves Infarct Related Artery Patency in STEMI

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
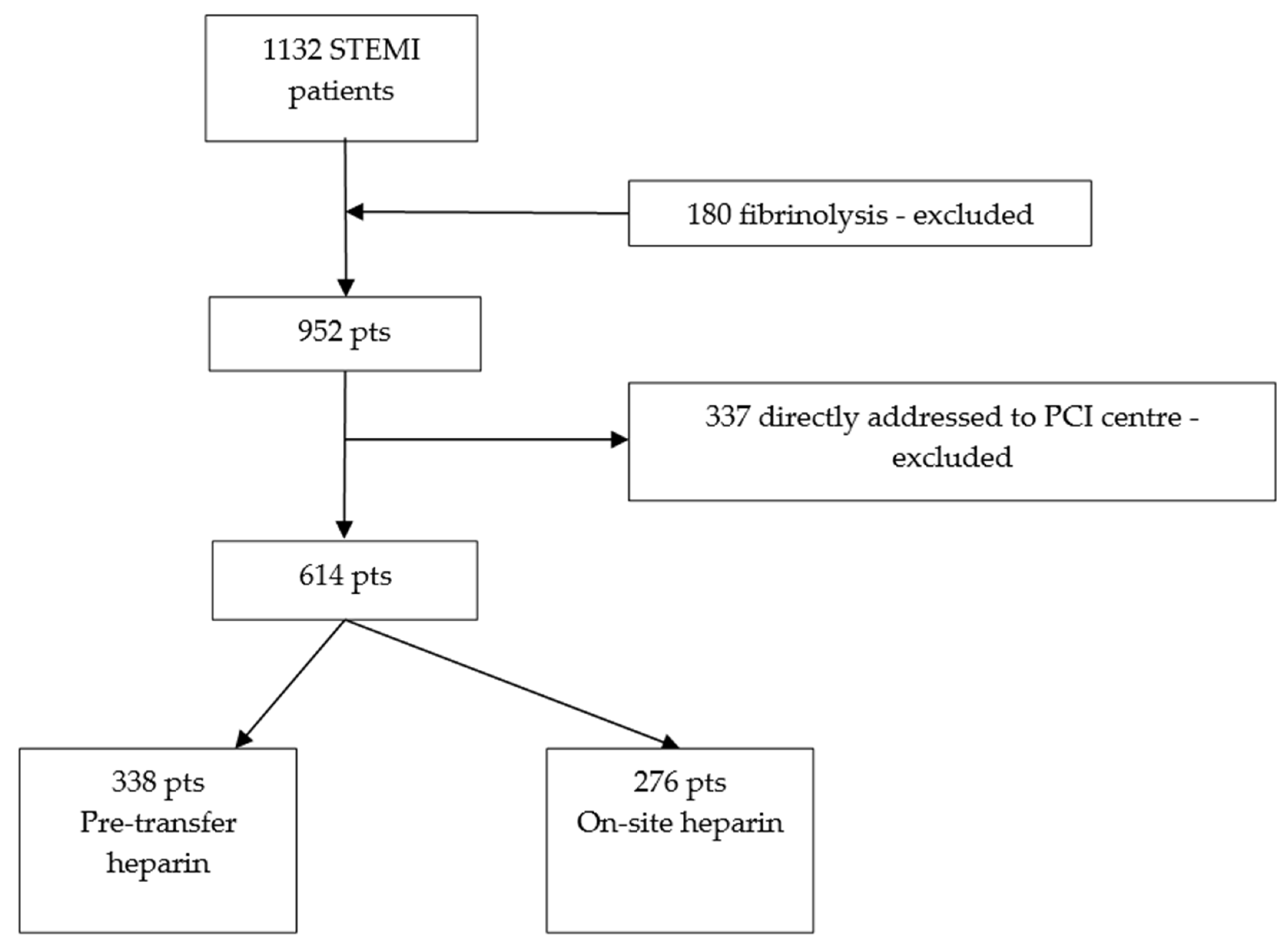
2.1. Patient Selection
2.2. Endpoints
- Rate of infarct-related artery (IRA) patency on coronary angiogram;
- Rate of in-hospital and post-discharge two-year mortality rates;
- Rate of in-hospital bleeding events from initial symptoms to discharge prior to the moment of discharge: major bleeding (Bleeding Academic Research Consortium (BARC) score > 2) any bleeding, access site-related bleeding;
- Stroke rate from initial symptoms prior to the moment of discharge.
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Effect of Pre-Transfer Heparin Effect on IRA Patency
4.2. Effect of Pre-Transfer Heparin Administration on Stent Diameter and Length
4.3. Risk of Pre-Transfer Heparin Administration Regarding Bleeding Events
5. Limitations
- Retrospective analysis with a relatively smaller sample compared to previously published registry analyses.
- Lack of routine evaluation of pre-angiography anticoagulation status which may impact both IRA patency and bleeding risk and is influenced by:
- Variable pre-transfer heparin dosing (5000 UI vs. weight-adjusted dose);
- Long time intervals from FMC (i.e., pre-transfer heparin administration) which may diminish residual anticoagulant effect at the time of coronary angiography.
- Confounding factors regarding antithrombotic therapy—antiplatelet therapy loading or omission of loading at FMC, type of antiplatelet therapy, simultaneous opioid administration.
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- OECD, on Health Systems EO, Policies. Romania: Country Health Profile 2017; OECD: Paris, France, 2017.
- Byrne, R.A.; Rossello, X.; Coughlan, J.J.; Barbato, E.; Berry, C.; Chieffo, A.; Claeys, M.J.; Dan, G.-A.; Dweck, M.R.; Galbraith, M.; et al. 2023 ESC Guidelines for the management of acute coronary syndromes: Developed by the task force on the management of acute coronary syndromes of the European Society of Cardiology (ESC). Eur. Heart J. 2023, 44, 3720–3826. [Google Scholar] [CrossRef]
- Emilsson, O.L.; Bergman, S.; Mohammad, M.A.; Olivecrona, G.K.; Götberg, M.; Erlinge, D.; Koul, S. Pretreatment with heparin in patients with ST-segment elevation myocardial infarction: A report from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR). EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2022, 18, 709–718. [Google Scholar] [CrossRef]
- Verheugt, F.W.; Liem, A.; Zijlstra, F.; Marsh, R.C.; Veen, G.; Bronzwaer, J.G. High dose bolus heparin as initial therapy before primary angioplasty for acute myocardial infarction: Results of the Heparin in Early Patency (HEAP) pilot study. J. Am. Coll. Cardiol. 1998, 31, 289–293. [Google Scholar] [CrossRef]
- Hirsh, J.; Anand, S.S.; Halperin, J.L.; Fuster, V. Mechanism of action and pharmacology of unfractionated heparin. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1094–1096. [Google Scholar] [CrossRef]
- Petersen, J.L.; Mahaffey, K.W.; Hasselblad, V.; Antman, E.M.; Cohen, M.; Goodman, S.G.; Langer, A.; Blazing, M.A.; Le-Moigne-Amrani, A.; de Lemos, J.A.; et al. Efficacy and Bleeding Complications Among Patients Randomized to Enoxaparin or Unfractionated Heparin for Antithrombin Therapy in Non–ST-Segment Elevation Acute Coronary Syndromes. JAMA 2004, 292, 89–96. [Google Scholar] [CrossRef]
- Franchini, M. Heparin-induced thrombocytopenia: An update. Thromb. J. 2005, 3, 14. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. Fourth universal definition of myocardial infarction. Eur. Heart J. 2019, 40, 237–269. [Google Scholar] [CrossRef] [PubMed]
- Giralt, T.; Carrillo, X.; Rodriguez-Leor, O.; Fernandez-Nofrerias, E.; Rueda, F.; Serra-Flores, J.; Viguer, J.M.; Mauri, J.; Curos, A.; Bayes-Genis, A. Time-dependent effects of unfractionated heparin in patients with ST-elevation myocardial infarction transferred for primary angioplasty. Int. J. Cardiol. 2015, 198, 70–74. [Google Scholar] [CrossRef]
- Napodano, M.; Ramondo, A.; Tarantini, G.; Peluso, D.; Compagno, S.; Fraccaro, C.; Frigo, A.C.; Razzolini, R.; Iliceto, S. Predictors and time-related impact of distal embolization during primary angioplasty. Eur. Heart J. 2009, 30, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Berger, P.B.; Ting, H.H.; Rihal, C.S.; Wilson, S.H.; Lennon, R.J.; Reeder, G.S.; Bresnahan, J.F.; Holmes, D.R. Influence of coronary thrombus on outcome of percutaneous coronary angioplasty in the current era (the Mayo Clinic experience). Am. J. Cardiol. 2001, 88, 1091–1096. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Socie. Eur. Heart J. 2017, 39, 119–177. [Google Scholar] [CrossRef] [PubMed]
- Farag, M.; Spinthakis, N.; Gue, Y.X.; Srinivasan, M.; Sullivan, K.; Wellsted, D.; Gorog, D.A. Impaired endogenous fibrinolysis in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention is a predictor of recurrent cardiovascular events: The RISK PPCI study. Eur. Heart J. 2019, 40, 295–305. [Google Scholar] [CrossRef]
- McGinley, C.; Mordi, I.R.; Kell, P.; Currie, P.; Hutcheon, S.; Koch, S.; Martin, T.; Irving, J. Prehospital Administration of Unfractionated Heparin in ST-Segment Elevation Myocardial Infarction Is Associated With Improved Long-Term Survival. J. Cardiovasc. Pharmacol. 2020, 76, 159–163. [Google Scholar] [CrossRef]
- Giralt, T.; Ribas, N.; Freixa, X.; Sabaté, M.; Caldentey, G.; Tizón-Marcos, H.; Carrillo, X.; García-Picart, J.; Lidón, R.M.; Cárdenas, M.; et al. Impact of pre-angioplasty antithrombotic therapy administration on coronary reperfusion in ST-segment elevation myocardial infarction: Does time matter? Int. J. Cardiol. 2021, 325, 9–15. [Google Scholar] [CrossRef]
- Cantor, W.J.; Lavi, S.; Džavík, V.; Cairns, J.; Cheema, A.N.; Della Siega, A.; Moreno, R.; Stankovic, G.; Kedev, S.; Natarajan, M.K.; et al. Upstream anticoagulation for patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention: Insights from the TOTAL trial. Catheter. Cardiovasc. Interv. 2020, 96, 519–525. [Google Scholar] [CrossRef]
- Karlsson, S.; Andell, P.; Mohammad, M.A.; Koul, S.; Olivecrona, G.K.; James, S.K.; Fröbert, O.; Erlinge, D. Editor’s Choice- Heparin pre-treatment in patients with ST-segment elevation myocardial infarction and the risk of intracoronary thrombus and total vessel occlusion. Insights from the TASTE trial. Eur. Heart J. Acute Cardiovasc. Care 2019, 8, 15–23. [Google Scholar] [CrossRef]
- Montalescot, G.; van ’t Hof, A.W.; Lapostolle, F.; Silvain, J.; Lassen, J.F.; Bolognese, L.; Cantor, W.J.; Cequier, Á.; Chettibi, M.; Goodman, S.G.; et al. Prehospital Ticagrelor in ST-Segment Elevation Myocardial Infarction. N. Engl. J. Med. 2014, 371, 1016–1027. [Google Scholar] [CrossRef] [PubMed]
- Rakowski, T.; Dudek, D.; Dziewierz, A.; Yu, J.; Witzenbichler, B.; Guagliumi, G.; Kornowski, R.; Hartmann, F.; Lansky, A.J.; Brener, S.J.; et al. Impact of infarct-related artery patency before primary PCI on outcome in patients with ST-segment elevation myocardial infarction: The HORIZONS-AMI trial. EuroIntervention J. EuroPCR Collab. Work. Group Interv. Cardiol. Eur. Soc. Cardiol. 2013, 8, 1307–1314. [Google Scholar] [CrossRef] [PubMed]
- Zeymer, U.; Huber, K.; Fu, Y.; Ross, A.; Granger, C.; Goldstein, P.; van de Werf, F.; Armstrong, P. Impact of TIMI 3 patency before primary percutaneous coronary intervention for ST-elevation myocardial infarction on clinical outcome: Results from the ASSENT-4 PCI study. Eur. Heart J. Acute Cardiovasc. Care 2012, 1, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Stone, G.W.; Cox, D.; Garcia, E.; Brodie, B.R.; Morice, M.C.; Griffin, J.; Mattos, L.; Lansky, A.J.; O’Neill, W.W.; Grines, C.L. Normal flow (TIMI-3) before mechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction: Analysis from the Primary Angioplasty in Myocardial Infarction Trials. Circulation 2001, 104, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Calmac, L.; Popa-Fotea, N.M.; Bataila, V.; Ploscaru, V.; Turea, A.; Tache, I.A.; Stoian, D.; Itu, L.; Badila, E.; Scafa-Udriste, A.; et al. Importance of Visual Estimation of Coronary Artery Stenoses and Use of Functional Evaluation for Appropriate Guidance of Coronary Revascularization—Multiple Operator Evaluation. Diagnostics 2021, 11, 2241. [Google Scholar] [CrossRef] [PubMed]
- Shin, E.-S.; Ann, S.H.; Singh, G.B.; Lim, K.H.; Yoon, H.-J.; Hur, S.-H.; Her, A.-Y.; Koo, B.-K.; Akasaka, T. OCT-Defined Morphological Characteristics of Coronary Artery Spasm Sites in Vasospastic Angina. JACC Cardiovasc. Imaging 2015, 8, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Shirai, S.; Kimura, T.; Nobuyoshi, M.; Morimoto, T.; Ando, K.; Soga, Y.; Yamaji, K.; Kondo, K.; Sakai, K.; Arita, T.; et al. Impact of Multiple and Long Sirolimus-Eluting Stent Implantation on 3-Year Clinical Outcomes in the j-Cypher Registry. JACC Cardiovasc. Interv. 2010, 3, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Hara, H.; Ono, M.; Kawashima, H.; Kogame, N.; Mack, M.J.; Holmes, D.R.; Morice, M.C.; Davierwala, P.M.; Mohr, F.W.; Thuijs, D.J.F.M.; et al. Impact of stent length and diameter on 10-year mortality in the SYNTAXES trial. Catheter. Cardiovasc. Interv. 2021, 98, E379–E387. [Google Scholar] [CrossRef] [PubMed]
- Wykrzykowska, J.J.; Serruys, P.W.; Onuma, Y.; de Vries, T.; van Es, G.A.; Buszman, P.; Linke, A.; Ischinger, T.; Klauss, V.; Corti, R.; et al. Impact of vessel size on angiographic and clinical outcomes of revascularization with biolimus-eluting stent with biodegradable polymer and sirolimus-eluting stent with durable polymer the LEADERS trial substudy. JACC Cardiovasc. Interv. 2009, 2, 861–870. [Google Scholar] [CrossRef]


{kind=link}
| Group A (Early Heparin) (n = 338) | Group B (Heparin On Site) (n = 276) | p | |
|---|---|---|---|
| Age, years | 62.3 ± 12.9 | 63.1 ± 14.0 | 0.45 |
| Female sex, n% | 91 (26.9%) | 79 (28.6%) | 0.64 |
| Smoking, n% | 205 (62.1%) | 175 (65.1%) | 0.45 |
| Hypertension, n % | 252 (74.6%) | 208 (75.4%) | 0.71 |
| Dyslipidemia, n % | 184 (54.5%) | 154 (55.8%) | 0.54 |
| Diabetes mellitus, n % | 77 (23.3%) | 39 (29.2%) | 0.10 |
| Previous MI, n% | 25 (7.4%) | 22 (8.0%) | 0.79 |
| Previous angina, n % | 176 (52.1%) | 139 (50.4%) | 0.67 |
| Previous PCI, n% | 15 (4.5%) | 17 (6.2%) | 0.09 |
| Previous stroke, n % | 27 (8%) | 26 (9.4%) | 0.53 |
| Cancer, n % | 13 (3.9%) | 21 (7.6%) | 0.15 |
| Anterior MI, n % | 144 (42.6%) | 114 (41.3%) | 0.74 |
| Radial procedure, n % | 293 (86.7%) | 237 (85.9%) | 0.39 |
| Manual thrombectomy, n % | 107 (31.7%) | 87 (31.5%) | 0.97 |
| Aspirin on FMC or pretreatment, n % | 338 (100%) | 276 (100%) | 0.73 |
| DAPT (Aspirin + P2Y12 inhibitors) on FMC, n % | 328 (97.0%) | 221 (80.1%) | <0.001 |
| Time from symptoms to FMC, minutes | 290.6 ± 310.1 | 341.1 ± 460.2 | 0.31 |
| Time FMC to balloon, minutes | 206.6 ± 256.3 | 187.7 ± 165.0 | 0.30 |
| Group A (Pre-Transfer) (n = 338) | Group B (Heparin on-Site) (n = 276) | p | |
|---|---|---|---|
| Patent infarct related artery, n % | 151 (44.7%) | 103 (37.3%) | 0.04 |
| Major bleeding (requiring transfusion), n % | 1 (0.3%) | 0 | 0.45 |
| Any bleeding, n % | 11 (3.2%) | 7 (2.0%) | 0.70 |
| Minimum hemoglobin, g/dl | 12.8 ± 2.2 | 12.9 ± 2.3 | 0.63 |
| Vascular access complications, n % | 3 (0.9%) | 8 (2.9%) | 0.06 |
| Periprocedural stroke, n (%) | 0 (%) | 1 (0.4%) | 0.26 |
| pPCI during index procedure, n (%) | 295 (87.3%) | 252 (91.3%) | 0.12 |
| LAD, n (%) | 152 (45%) | 127 (45.5%) | 0.36 |
| LCX, n (%) | 49 (14.5%) | 47 (17%) | |
| LM, n (%) | 6 (1.8%) | 1 (0.4%) | |
| RCA, n (%) | 131 (38.8%) | 101 (36.6%) | |
| Stent diameter, mm | 3.15 ± 0.66 | 3.06 ± 0.76 | 0.03 |
| Stent length, mm | 22.4 ± 11.2 | 26.6 ± 10.1 | 0.04 |
| In-hospital mortality, n (%) | 31 (9.2%) | 30 (10.9%) | 0.48 |
| Two-year total mortality, n % | 58 (17.1%) | 54 (19.5%) | 0.40 |
| Variable | Odds Ratio | CI 95% | p |
|---|---|---|---|
| Age, years | 1.00 | 0.99–1.01 | 0.507 |
| Gender, male | 1.17 | 0.79–1.72 | 0.412 |
| Smoking | 1.23 | 0.86–1.76 | 0.256 |
| Hypertension | 0.81 | 0.54–1.22 | 0.329 |
| Diabetes mellitus | 1.59 | 1.10–2.28 | 0.012 |
| Anterior STEMI | 1.45 | 1.04–2.03 | 0.026 |
| Early P2Y2 inhibitor administration | 0.67 | 0.38–1.16 | 0.160 |
| Heparin administration at FMC | 1.50 | 1.06–2.13 | 0.019 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bataila, V.; Popa-Fotea, N.-M.; Cojocaru, C.; Calmac, L.; Mihai, C.; Dragoescu, M.-B.; Ploscaru, V.; Marinescu, M.; Iliese, V.; Avram, A.-G.; et al. Parenteral Anticoagulation at First Medical Contact Improves Infarct Related Artery Patency in STEMI. J. Clin. Med. 2024, 13, 1710. https://doi.org/10.3390/jcm13061710
Bataila V, Popa-Fotea N-M, Cojocaru C, Calmac L, Mihai C, Dragoescu M-B, Ploscaru V, Marinescu M, Iliese V, Avram A-G, et al. Parenteral Anticoagulation at First Medical Contact Improves Infarct Related Artery Patency in STEMI. Journal of Clinical Medicine. 2024; 13(6):1710. https://doi.org/10.3390/jcm13061710
Chicago/Turabian StyleBataila, Vlad, Nicoleta-Monica Popa-Fotea, Cosmin Cojocaru, Lucian Calmac, Cosmin Mihai, Marian-Bogdan Dragoescu, Vlad Ploscaru, Mugur Marinescu, Vasile Iliese, Anamaria-Georgiana Avram, and et al. 2024. "Parenteral Anticoagulation at First Medical Contact Improves Infarct Related Artery Patency in STEMI" Journal of Clinical Medicine 13, no. 6: 1710. https://doi.org/10.3390/jcm13061710
APA StyleBataila, V., Popa-Fotea, N. -M., Cojocaru, C., Calmac, L., Mihai, C., Dragoescu, M. -B., Ploscaru, V., Marinescu, M., Iliese, V., Avram, A. -G., Mitran, R. -E., & Vatasescu, R. -G. (2024). Parenteral Anticoagulation at First Medical Contact Improves Infarct Related Artery Patency in STEMI. Journal of Clinical Medicine, 13(6), 1710. https://doi.org/10.3390/jcm13061710