
Application of Biomarkers in Obese Infertile Women: A Genetic Tool for a Personalized Treatment
 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Detection of Leptin and CART Gene Expression
4. Detection of FSHR Polymorphisms
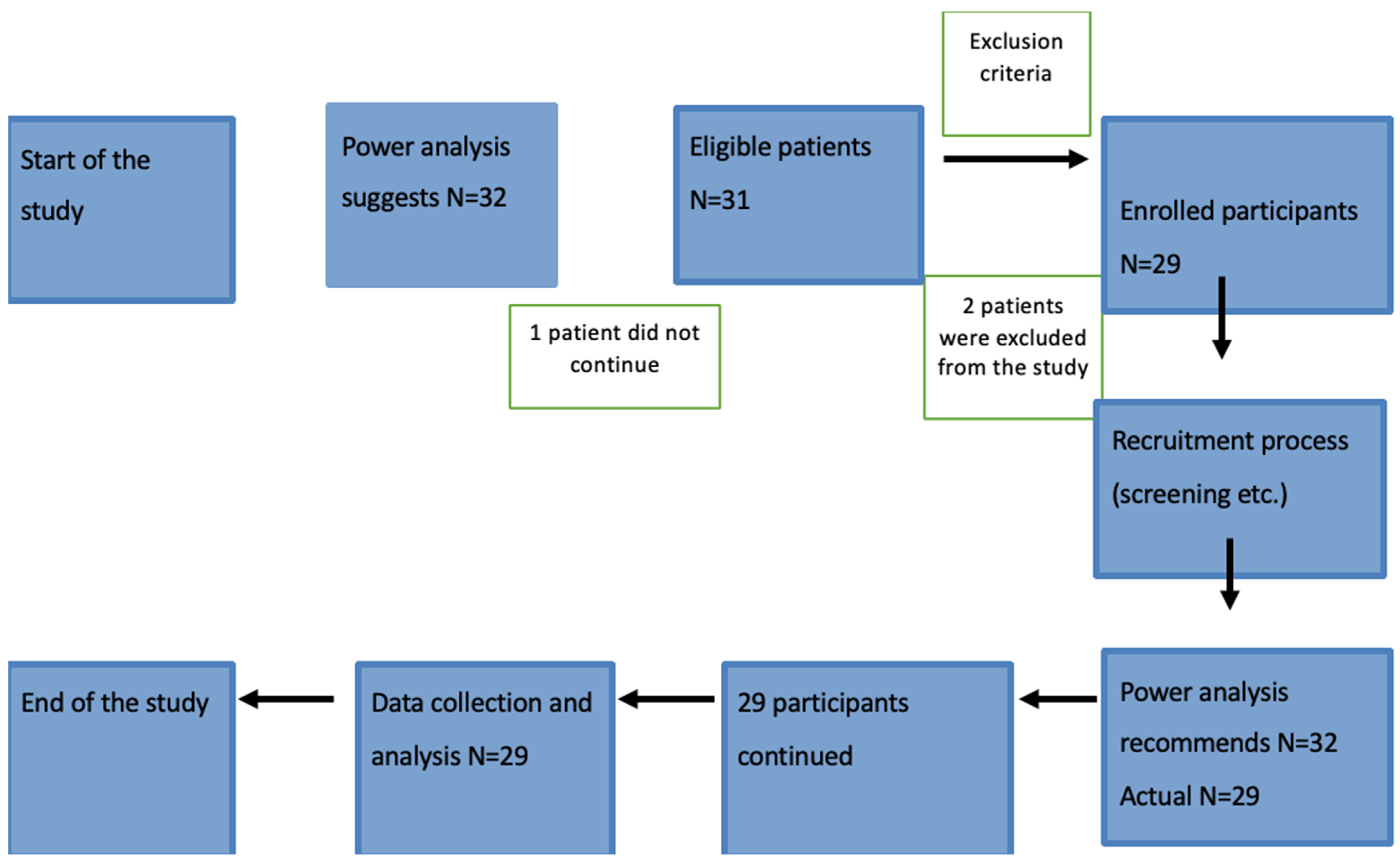
5. Sample Size Determination
6. Statistical Analysis (Methods)
7. Results
8. Discussion
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mechanick, J.I.; Kushner, R.F.; Sugerman, H.J.; Gonzalez-Campoy, J.M.; Collazo-Clavell, M.L.; Spitz, A.F.; Apovian, C.M.; Livingston, E.H.; Brolin, R.; Sarwer, D.B.; et al. American association of clinical endocrinologists, the obesity society, and american society for metabolic & bariatric surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Obesity 2009, 17, S3–S72. [Google Scholar] [CrossRef]
- Mechanick, J.I.; Youdim, A.; Jones, D.B.; Timothy Garvey, W.; Hurley, D.L.; Molly McMahon, M.; Heinberg, L.J.; Kushner, R.; Adams, T.D.; Shikora, S.; et al. Clinical Practice Guidelines for the Perioperative Nutritional, Metabolic, and Nonsurgical Support of the Bariatric Surgery Patient—2013 Update: Cosponsored by American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic & Bariatric Surgery. Surg. Obes. Relat. Dis. 2013, 9, 159–191. [Google Scholar] [CrossRef] [PubMed]
- Salminen, P.; Helmiö, M.; Ovaska, J.; Juuti, A.; Leivonen, M.; Peromaa-Haavisto, P.; Hurme, S.; Soinio, M.; Nuutila, P.; Victorzon, M. Effect of Laparoscopic Sleeve Gastrectomy vs Laparoscopic Roux-en-Y Gastric Bypass on Weight Loss at 5 Years Among Patients With Morbid Obesity: The SLEEVEPASS Randomized Clinical Trial. JAMA 2018, 319, 241. [Google Scholar] [CrossRef] [PubMed]
- Reges, O.; Greenland, P.; Dicker, D.; Leibowitz, M.; Hoshen, M.; Gofer, I.; Rasmussen-Torvik, L.J.; Balicer, R.D. Association of Bariatric Surgery Using Laparoscopic Banding, Roux-en-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management With All-Cause Mortality. JAMA 2018, 319, 279. [Google Scholar] [CrossRef] [PubMed]
- Davidson, L.E.; Adams, T.D.; Kim, J.; Jones, J.L.; Hashibe, M.; Taylor, D.; Mehta, T.; McKinlay, R.; Simper, S.C.; Smith, S.C.; et al. Association of Patient Age at Gastric Bypass Surgery With Long-term All-Cause and Cause-Specific Mortality. JAMA Surg. 2016, 151, 631. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Gromoll, J.; Nieschlag, E. The Follicle-Stimulating Hormone Receptor: Biochemistry, Molecular Biology, Physiology, and Pathophysiology. Endocr. Rev. 1997, 18, 739–773. [Google Scholar] [CrossRef] [PubMed]
- Ulloa-Aguirre, A.; Reiter, E.; Crépieux, P. FSH Receptor Signaling: Complexity of Interactions and Signal Diversity. Endocrinology 2018, 159, 3020–3035. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Peng, Y.; Sharrow, A.C.; Iqbal, J.; Zhang, Z.; Papachristou, D.J.; Zaidi, S.; Zhu, L.-L.; Yaroslavskiy, B.B.; Zhou, H.; et al. FSH Directly Regulates Bone Mass. Cell 2006, 125, 247–260. [Google Scholar] [CrossRef] [PubMed]
- Conforti, A.; Vaiarelli, A.; Cimadomo, D.; Bagnulo, F.; Peluso, S.; Carbone, L.; Di Rella, F.; De Placido, G.; Ubaldi, F.M.; Huhtaniemi, I.; et al. Pharmacogenetics of FSH Action in the Female. Front. Endocrinol. 2019, 10, 398. [Google Scholar] [CrossRef]
- Lledo, B.; Ortiz, J.A.; Llacer, J.; Bernabeu, R. Pharmacogenetics of ovarian response. Pharmacogenomics 2014, 15, 885–893. [Google Scholar] [CrossRef]
- Mayorga, M.P.; Gromoll, J.; Behre, H.M.; Gassner, C.; Nieschlag, E.; Simoni, M. Ovarian Response to Follicle-Stimulating Hormone (FSH) Stimulation Depends on the FSH Receptor Genotype. J. Clin. Endocrinol. Metab. 2000, 85, 3365–3369. [Google Scholar] [CrossRef]
- Alviggi, C.; Conforti, A.; Caprio, F.; Gizzo, S.; Noventa, M.; Strina, I.; Pagano, T.; De Rosa, P.; Carbone, F.; Colacurci, N.; et al. In Estimated Good Prognosis Patients Could Unexpected “Hyporesponse” to Controlled Ovarian Stimulation be Related to Genetic Polymorphisms of FSH Receptor? Reprod. Sci. 2016, 23, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.K.; Yoon, J.S.; Ku, S.-Y.; Choi, Y.M.; Hwang, K.R.; Park, S.Y.; Lee, G.H.; Lee, W.D.; Kim, S.H.; Kim, J.G.; et al. Follicle-stimulating hormone receptor gene polymorphism and ovarian responses to controlled ovarian hyperstimulation for IVF-ET. J. Hum. Genet. 2006, 51, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Hausman, G.J.; Barb, C.R.; Lents, C.A. Leptin and reproductive function. Biochimie 2012, 94, 2075–2081. [Google Scholar] [CrossRef] [PubMed]
- Brannian, J.D.; Hansen, K.A. Leptin and Ovarian Folliculogenesis: Implications for Ovulation Induction and ART Outcomes. Semin. Reprod. Med. 2002, 20, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Galvão, A.; Henriques, S.; Pestka, D.; Lukasik, K.; Skarzynski, D.; Mateus, L.M.; Ferreira-Dias, G.M.L. Equine Luteal Function Regulation May Depend on the Interaction Between Cytokines and Vascular Endothelial Growth Factor: An In Vitro Study1. Biol. Reprod. 2012, 86, 187. [Google Scholar] [CrossRef] [PubMed]
- Rogge, G.; Jones, D.; Hubert, G.W.; Lin, Y.; Kuhar, M.J. CART peptides: Regulators of body weight, reward and other functions. Nat. Rev. Neurosci. 2008, 9, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, P.; Judge, M.E.; Thim, L.; Ribel, U.; Christjansen, K.N.; Wulff, B.S.; Clausen, J.T.; Jensen, P.B.; Madsen, O.D.; Vrang, N.; et al. Hypothalamic CART is a new anorectic peptide regulated by leptin. Nature 1998, 393, 72–76. [Google Scholar] [CrossRef]
- Hunter, E.; Avenell, A.; Maheshwari, A.; Stadler, G.; Best, D. The effectiveness of weight-loss lifestyle interventions for improving fertility in women and men with overweight or obesity and infertility: A systematic review update of evidence from randomized controlled trials. Obes. Rev. 2021, 22, e13325. [Google Scholar] [CrossRef]
- Yao, J.; Ren, X.; Ireland, J.J.; Coussens, P.M.; Smith, T.P.L.; Smith, G.W. Generation of a bovine oocyte cDNA library and microarray: Resources for identification of genes important for follicular development and early embryogenesis. Physiol. Genom. 2004, 19, 84–92. [Google Scholar] [CrossRef]
- Lv, L.; Jimenez-Krassel, F.; Sen, A.; Bettegowda, A.; Mondal, M.; Folger, J.K.; Lee, K.-B.; Ireland, J.J.; Smith, G.W. Evidence Supporting a Role for Cocaine- and Amphetamine-Regulated Transcript (CARTPT) in Control of Granulosa Cell Estradiol Production Associated with Dominant Follicle Selection in Cattle. Biol. Reprod. 2009, 81, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Sen, A.; Bettegowda, A.; Jimenez-Krassel, F.; Ireland, J.J.; Smith, G.W. Cocaine- and Amphetamine-Regulated Transcript Regulation of Follicle-Stimulating Hormone Signal Transduction in Bovine Granulosa Cells. Endocrinology 2007, 148, 4400–4410. [Google Scholar] [CrossRef] [PubMed]
- Courcoulas, A.P.; Christian, N.J.; Belle, S.H.; Berk, P.D.; Flum, D.R.; Garcia, L.; Horlick, M.; Kalarchian, M.A.; King, W.C.; Mitchell, J.E.; et al. Weight change and health outcomes at 3 years after bariatric surgery among individuals with severe obesity. JAMA 2013, 310, 2416–2425. [Google Scholar] [CrossRef] [PubMed]
- Leitner, D.R.; Frühbeck, G.; Yumuk, V.; Schindler, K.; Micic, D.; Woodward, E.; Toplak, H. Obesity and Type 2 Diabetes: Two Diseases with a Need for Combined Treatment Strategies—EASO Can Lead the Way. Obes. Facts 2017, 10, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Hannah, W.N.; Harrison, S.A. Effect of Weight Loss, Diet, Exercise, and Bariatric Surgery on Nonalcoholic Fatty Liver Disease. Clin. Liver Dis. 2016, 20, 339–350. [Google Scholar] [CrossRef] [PubMed]
- Asnicar, M.A.; Smith, D.P.; Yang, D.D.; Heiman, M.L.; Fox, N.; Chen, Y.F.; Hsiung, H.M.; Köster, A. Absence of cocaine- and amphetamine-regulated transcript results in obesity in mice fed a high caloric diet. Endocrinology 2001, 142, 4394–4400. [Google Scholar] [CrossRef] [PubMed]
- Gumbs, A.A.; Gagner, M.; Dakin, G.; Pomp, A. Sleeve Gastrectomy for Morbid Obesity. Obes. Surg. 2007, 17, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Zhao, G.; Wen, J.; Tong, W. Follicle-stimulating hormone promotes the transformation of cholesterol to estrogen in mouse adipose tissue. Biochem. Biophys. Res. Commun. 2018, 495, 2331–2337. [Google Scholar] [CrossRef] [PubMed]
- Anagnostou, E.; Drakakis, P.; Marinopoulos, S.; Mavrogianni, D.; Loutradis, D. The Impact of Genetics Profile (Gene Polymorphisms) in Obese Non- PCOS Women Entering an IVF/ICSI Program. Curr. Drug Targets 2013, 14, 850–855. [Google Scholar] [CrossRef]
- Sudo, S. Genetic and functional analyses of polymorphisms in the human FSH receptor gene. Mol. Hum. Reprod. 2002, 8, 893–899. [Google Scholar] [CrossRef]
- De Castro, F.; Ruiz, R.; Montoro, L.; Pérez-Hernández, D.; Sánchez-Casas Padilla, E.; Real, L.M.; Ruiz, A. Role of follicle-stimulating hormone receptor Ser680Asn polymorphism in the efficacy of follicle-stimulating hormone. Fertil. Steril. 2003, 80, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Chou, S.H.; Mantzoros, C. 20 YEARS OF LEPTIN: Role of leptin in human reproductive disorders. J. Endocrinol. 2014, 223, T49–T62. [Google Scholar] [CrossRef] [PubMed]
- Wertel, I.; Gogacz, M.; Polak, G.; Jakowicki, J.; Kotarski, J. Leptin is not involved in the pathophysiology of endometriosis-related infertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 119, 206–209. [Google Scholar] [CrossRef]
- Kitawaki, J. Leptin directly stimulates aromatase activity in human luteinized granulosa cells. Mol. Hum. Reprod. 1999, 5, 708–713. [Google Scholar] [CrossRef]
- Zuhair Abdul-Majeed Alkhwaja, S.; Jabir Edan, B.; Raad Muhi, Z. Role of Serum Leptin Level in Primary Sub-Fertile Women. Arch. Razi Inst. 2022, 77, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Fang, Q.; Wang, M.; Wang, Y.; Zhu, X.; Fang, Z.; Lu, F.; Xu, B.; Jin, R.; Han, H.; et al. Effect of weight loss on pregnancy outcomes, neuronal-reproductive-metabolic hormones and gene expression profiles in granulosa cells in obese infertile PCOS patients undergoing IVF-ET. Front. Endocrinol. 2022, 13, 954428. [Google Scholar] [CrossRef]
- Kaur, M.; Singh, S.; Kaur, R.; Beri, A.; Kaur, A. Analyzing the Impact of FSHR Variants on Polycystic Ovary Syndrome—A Case-Control Study in Punjab. Reprod. Sci. 2023, 30, 2563–2572. [Google Scholar] [CrossRef]
- Chu, G.; Ma, G.; Sun, J.; Zhu, Y.; Xiang, A.; Yang, G.; Sun, S. Leptin Receptor Mediates Bmal1 Regulation of Estrogen Synthesis in Granulosa Cells. Animals 2019, 9, 899. [Google Scholar] [CrossRef]
- Ma, X.; Hayes, E.; Prizant, H.; Srivastava, R.K.; Hammes, S.R.; Sen, A. Leptin-Induced CART (Cocaine- and Amphetamine-Regulated Transcript) Is a Novel Intraovarian Mediator of Obesity-Related Infertility in Females. Endocrinology 2016, 157, 1248–1257. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Mean ± SD |
|---|---|
| Age (years) | 33.0 ± 4.1 (26, 39) |
| Weight (kg) | 109.89 ± 19.28 |
| Height (m) | 1.53 ± 0.21 |
| BMI (kg/m2) | 41.94 ± 3.98 |
| LH (mIU/mL) | 6.35 ± 0.67 |
| E2 (pg/mL) | 29.81 ± 2.65 |
| SHBG (nmol/L) | 36.24 ± 7.58 |
| Free testosterone (ng/dL) | 28.72 ± 9.35 |
| AMH (ng/mL) | 2.14 ± 0.24 |
| Duration of infertility (years) | 3 (2, 5) |
| Cpt0 CART (adjusted) | 0.3 ± 4.41 |
| Cpt0 leptin (adjusted) | −1.81 ± 1.82 |
| Homozygotes without the Polymorphism (N = 8) | Heterozygotes for the Polymorphism (N = 13) | Homozygotes for the Polymorphism (N = 8) | p-Value between the Three Groups | p-Value between Homozygotes without the Polymorphism and Heterozygotes with the Polymorphism | p-Value between Homozygotes without the Polymorphism and Homozygotes with the Polymorphism | p-Value between Heterozygotes and Homozygotes with the Polymorphism | |
|---|---|---|---|---|---|---|---|
| Characteristic | Median (Q1–Q3) | Median (Q1–Q3) | Median (Q1–Q3) | p | p | p | p |
| AFC—Left ovary—before surgery | 10 (8.5–11) | 8 (7–10) | 10 (8–12.5) | 0.1775 | 0.1775 | 0.8738 | 0.1252 |
| AFC—Left ovary—post surgery | 7 (5.5–8.5) | 7 (6–7) | 6.5 (6–8) | 0.7730 | 0.5016 | 0.8724 | 0.6258 |
| AFC—Left difference | −3 (−4–−2) | −2 (−3–0) | −3.5 (−4.5–−1.5) | 0.3088 | 0.2000 | 0.7889 | 0.2145 |
| AFC—Right ovary—before surgery | 12 (10–12.5) | 9 (8–12) | 10.5 (9–11.5) | 0.4466 | 0.3240 | 0.3105 | 0.4005 |
| AFC—Right ovary—post surgery | 6 (5–9.5) | 8 (7–8) | 7.5 (7–9) | 0.5267 | 0.5086 | 0.2875 | 0.5027 |
| AFC—Right difference | −3.5 (−7–−1.5) | −2 (−4–0) | −2 (−4.5–−0.5) | 0.4693 | 0.2744 | 0.2897 | 0.9127 |
| AMH (ng/mL)—before surgery | 2.2 (1.9–2.3) | 2.2 (2–2.4) | 2.2 (1.9–2.4) | 0.8592 | 0.6081 | 0.8727 | 0.7155 |
| AMH (ng/mL)—post surgery | 3 (2.9–3.1) | 3 (2.8–3.1) | 2.9 (2.8–3) | 0.4507 | 0.9408 | 0.1957 | 0.3323 |
| AMH difference | 3.9 (2.7–4.4) | 3.2 (2.7–3.8) | 2.7 (2–3.4) | 0.3460 | 0.3454 | 0.1886 | 0.4039 |
| Age | 31 (28–35.5) | 36 (35–37) | 31.5 (27.5–34.5) | 0.0318 | 0.0680 | 0.5237 | 0.0163 |
| BMI (before surgery) | 41.8 (39.2–42.7) | 41.2 (38.9–44.5) | 40.7 (37.9–45.6) | 0.9464 | 0.7173 | 0.8336 | 0.8563 |
| BMI (after 6 months) | 26.1 (25.3–26.9) | 25.7 (24.8–26.2) | 26.5 (25.3–27.2) | 0.4375 | 0.6892 | 0.5271 | 0.1792 |
| BMI difference | −14.8 (−16.7–−13.8) | −15.3 (−18.8–−14.3) | −13.6 (−19–−11.3) | 0.2578 | 0.4913 | 0.3446 | 0.1111 |
| Cpt1-Cpt0 CART | −1.7 (−2.4–−1.3) | −2.1 (−2.6–−1.8) | −1.5 (−12.7–−1.3) | 0.6387 | 0.3848 | 1.0000 | 0.5006 |
| Cpt1—Cpt0 leptin | 2 (1.6–2.6) | 2 (1.4–2.3) | 1.7 (0.7–1.9) | 0.4275 | 0.5623 | 0.2030 | 0.3832 |
| E2 (pg/mL)—before surgery | 29.6 (29.5–32.7) | 29.8 (27.1–32) | 29.6 (27.7–31.4) | 0.6834 | 0.5141 | 0.3713 | 0.9134 |
| E2 (pg/mL)—post surgery | 51.2 (44.4–54.6) | 47.8 (44.8–50.7) | 47 (45.1–51.9) | 0.8078 | 0.6121 | 0.5286 | 0.7720 |
| E2 difference | 19.7 (15.7–21.8) | 17.7 (15.2–22.3) | 18.2 (13.7–22.5) | 0.9014 | 0.8563 | 0.5995 | 0.8280 |
| FSH (mIU/mL)—before surgery | 8.1 (7.6–10.1) | 9.5 (8.8–11.2) | 10.3 (8.1–11.9) | 0.0408 | 0.0362 | 0.0292 | 0.0515 |
| FSH (mIU/mL)—post surgery | 5.8 (5–6.7) | 7.1(5.6–7.8) | 8.2(4.7–9.1) | 0.0356 | 0.0458 | 0.0484 | 0.0685 |
| FSH difference | 2.6 (2.1–4.0) | 2.4 (1.7–3.8) | 2.1 (1.6–3.1) | 0.3460 | 0.1454 | 0.0886 | 0.2039 |
| Free testo (ng/dL)—before surgery | 32.4 (21.2–37.5) | 31.5 (27.3–34.3) | 25.6 (19.1–29.5) | 0.3107 | 0.6639 | 0.2936 | 0.1281 |
| Free testo (ng/dL)—post surgery | 9.3 (6.4–11.7) | 9.3 (7.4–11.2) | 8.9 (8.4–10.7) | 0.9431 | 0.6638 | 0.9157 | 0.9133 |
| Free testo difference | −25.4 (−27.7–−10.4) | −21.8 (−26.3–−15.3) | −17.7 (−20.6–−10.1) | 0.3548 | 0.7171 | 0.2476 | 0.1922 |
| LH (mIU/mL)—before surgery) | 6.4 (6.2–6.7) | 6.8 (6.3–7) | 6.3 (5.9–6.4) | 0.3440 | 0.3627 | 0.3963 | 0.2016 |
| LH (mIU/mL)—post surgery | 9.4 (8.9–9.9) | 8.9 (8.6–9.5) | 8.4 (7.7–9) | 0.1011 | 0.2609 | 0.0325 | 0.1466 |
| LH difference | 2.9 (2.1–3.7) | 2.7 (2–3.3) | 2.5 (1.2–2.9) | 0.4172 | 0.3848 | 0.2936 | 0.3462 |
| SHBG (nmol/L)—before surgery | 40.4 (27.9–46.4) | 39.1 (34.5–41.3) | 32 (25.9–38) | 0.1106 | 0.8563 | 0.1415 | 0.0357 |
| SHBG (nmol/L)—post surgery | 69.7 (58.9–81.3) | 65.3 (58.7–72.3) | 58.2 (49.5–67) | 0.2383 | 0.5380 | 0.1415 | 0.1688 |
| SHBG difference | 30.9 (23.4–36.6) | 28.3 (21.2–34.9) | 27.4 (21.9–31.7) | 0.7953 | 0.7172 | 0.4623 | 0.7720 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voros, C.; Bananis, K.; Papapanagiotou, A.; Pouliakis, A.; Mavriki, K.; Gkaniatsos, I.; Daskalaki, M.A.; Prokopakis, I.; Tsimpoukelis, C.; Koulakmanidis, A.-M.; et al. Application of Biomarkers in Obese Infertile Women: A Genetic Tool for a Personalized Treatment. J. Clin. Med. 2024, 13, 2261. https://doi.org/10.3390/jcm13082261
Voros C, Bananis K, Papapanagiotou A, Pouliakis A, Mavriki K, Gkaniatsos I, Daskalaki MA, Prokopakis I, Tsimpoukelis C, Koulakmanidis A-M, et al. Application of Biomarkers in Obese Infertile Women: A Genetic Tool for a Personalized Treatment. Journal of Clinical Medicine. 2024; 13(8):2261. https://doi.org/10.3390/jcm13082261
Chicago/Turabian StyleVoros, Charalampos, Kyriakos Bananis, Angeliki Papapanagiotou, Abraham Pouliakis, Konstantina Mavriki, Ioannis Gkaniatsos, Maria Anastasia Daskalaki, Ioannis Prokopakis, Charalampos Tsimpoukelis, Aristotelis-Marios Koulakmanidis, and et al. 2024. "Application of Biomarkers in Obese Infertile Women: A Genetic Tool for a Personalized Treatment" Journal of Clinical Medicine 13, no. 8: 2261. https://doi.org/10.3390/jcm13082261
APA StyleVoros, C., Bananis, K., Papapanagiotou, A., Pouliakis, A., Mavriki, K., Gkaniatsos, I., Daskalaki, M. A., Prokopakis, I., Tsimpoukelis, C., Koulakmanidis, A. -M., Darlas, M., Anysiadou, S., Daskalakis, G., & Domali, E. (2024). Application of Biomarkers in Obese Infertile Women: A Genetic Tool for a Personalized Treatment. Journal of Clinical Medicine, 13(8), 2261. https://doi.org/10.3390/jcm13082261