

Injection Site Matters: A Comparative Analysis of Transpulmonary Thermodilution via Simultaneous Femoral and Jugular Indicator Injections under Veno-Venous Extracorporeal Membrane Oxygenation Therapy

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Principle of TPTD Measurements with the PiCCO Device
2.3. Calculations
2.4. Statistical Analysis
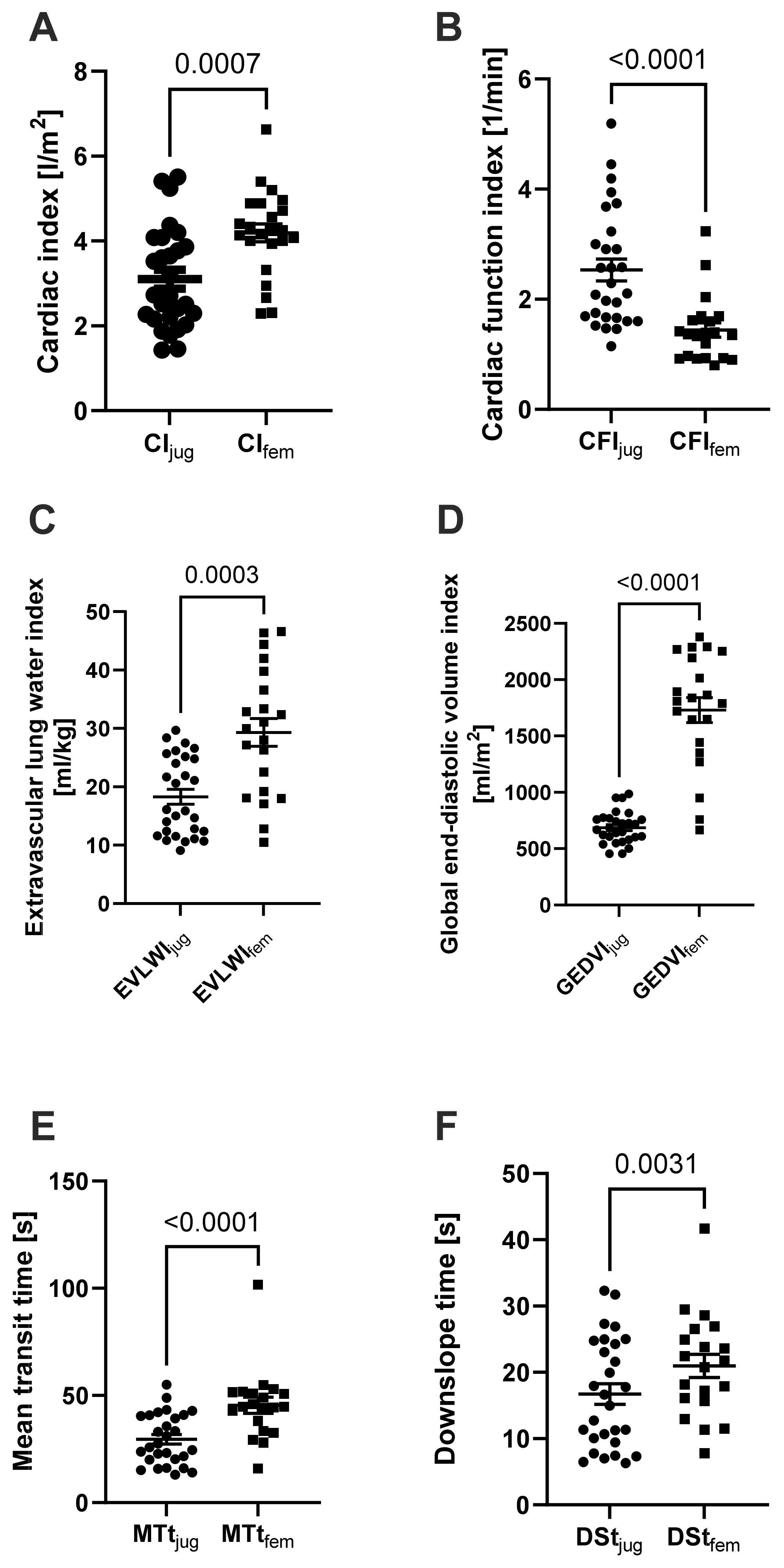
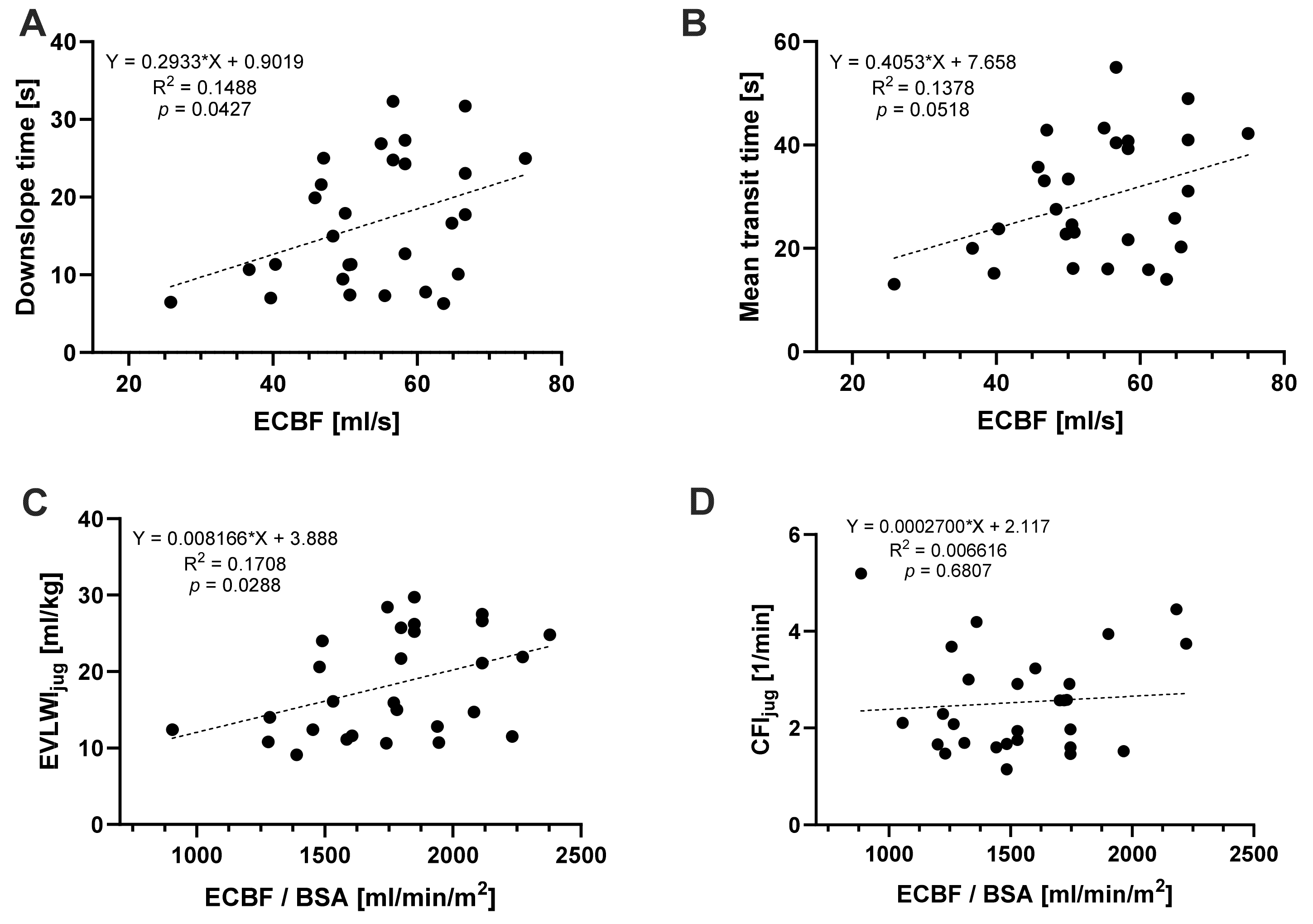
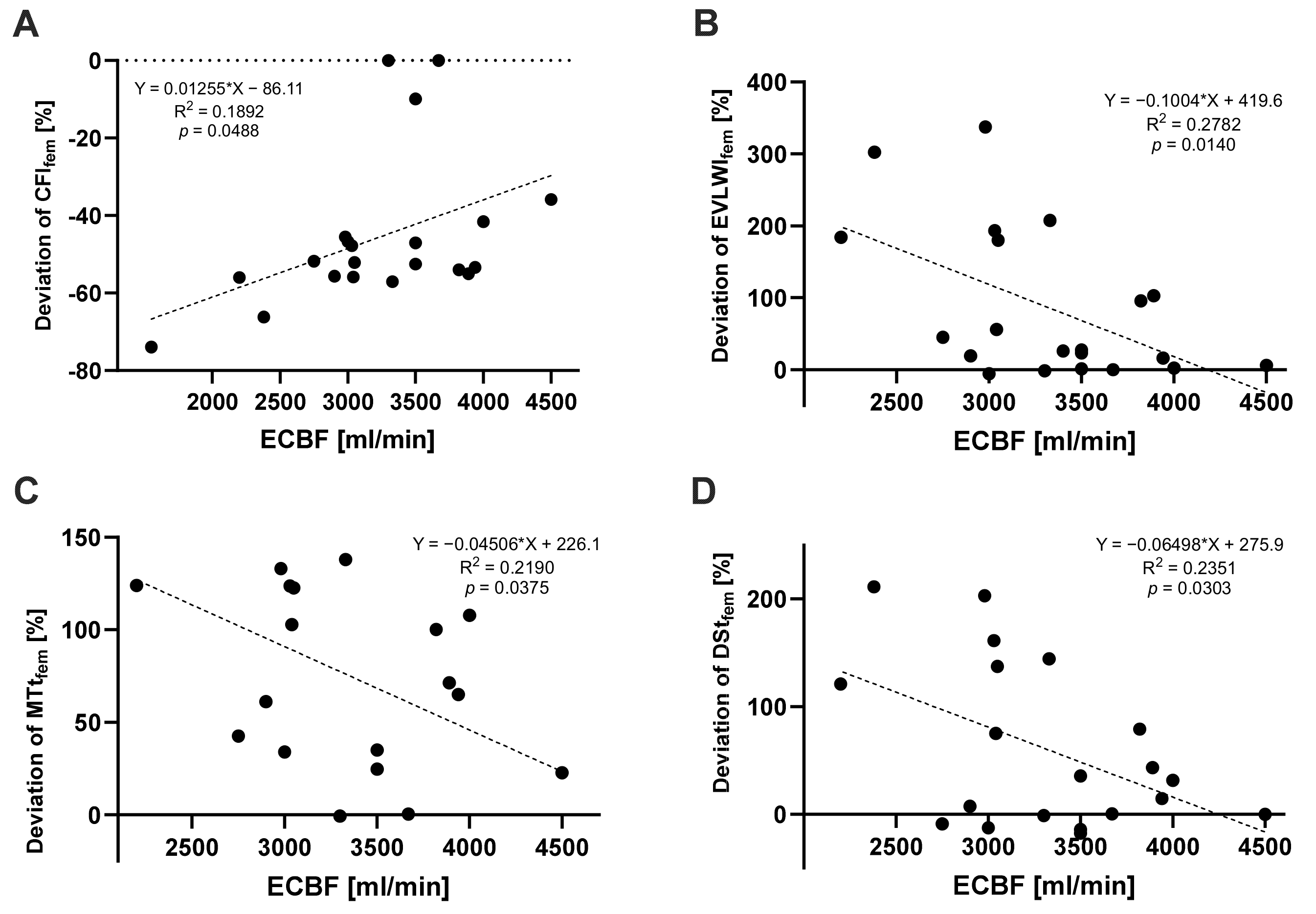
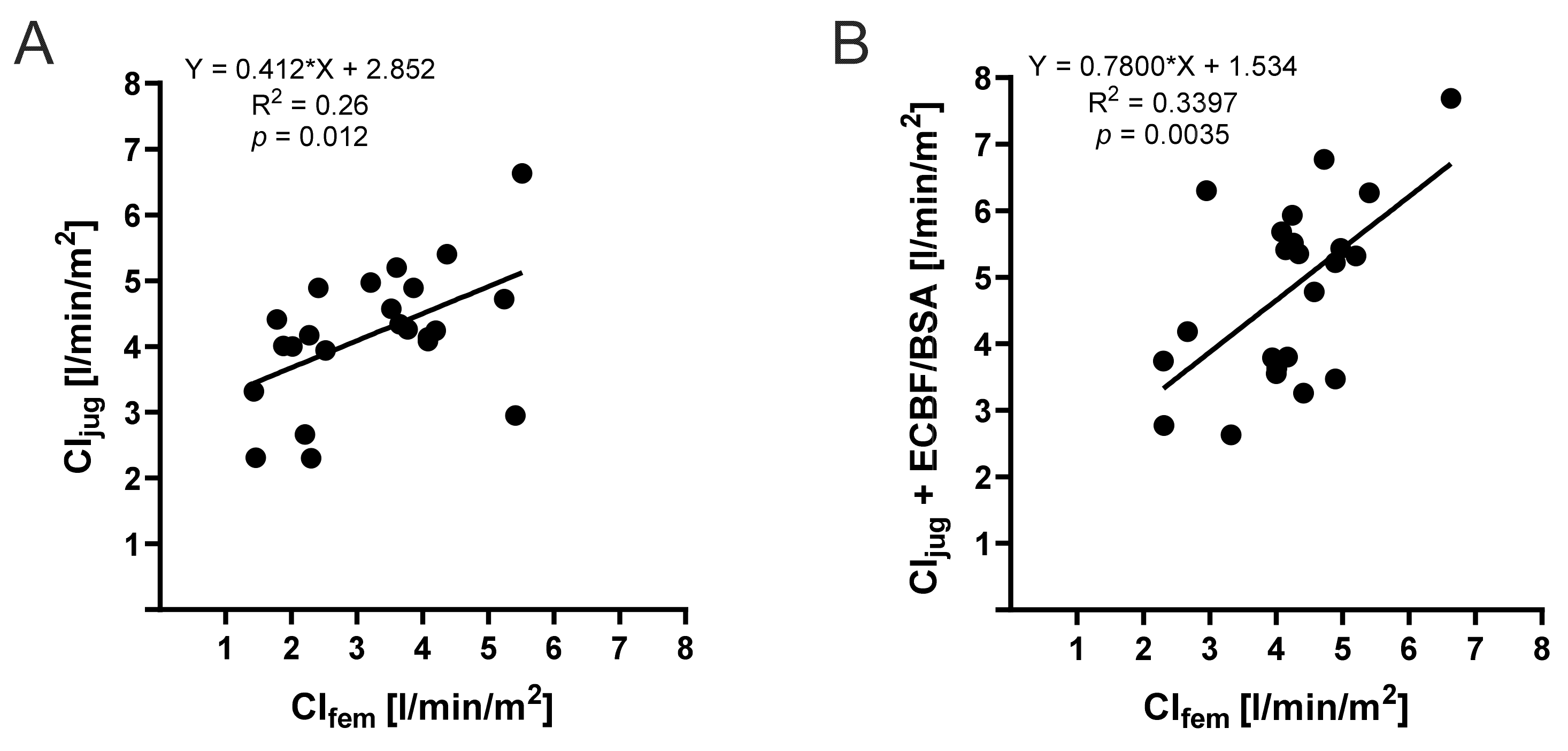
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Friedrichson, B.; Mutlak, H.; Zacharowski, K.; Piekarski, F. Insight into ECMO, mortality and ARDS: A nationwide analysis of 45,647 ECMO runs. Crit. Care 2021, 25, 38. [Google Scholar] [CrossRef] [PubMed]
- Karagiannidis, C.; Slutsky, A.S.; Bein, T.; Windisch, W.; Weber-Carstens, S.; Brodie, D. Complete countrywide mortality in COVID patients receiving ECMO in Germany throughout the first three waves of the pandemic. Crit. Care 2021, 25, 413. [Google Scholar] [CrossRef] [PubMed]
- Cecconi, M.; De Backer, D.; Antonelli, M.; Beale, R.; Bakker, J.; Hofer, C.; Jaeschke, R.; Mebazaa, A.; Pinsky, M.R.; Teboul, J.L.; et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014, 40, 1795–1815. [Google Scholar] [CrossRef] [PubMed]
- Janssens, U.; Jung, C.; Hennersdorf, M.; Ferrari, M.; Fuhrmann, J.; Buerke, M.; Ebelt, H.; Graf, T.; Thiele, H.; Kelm, M. Empfehlungen zum hämodynamischen Monitoring in der internistischen Intensivmedizin. Kardiologe 2016, 10, 149–169. [Google Scholar] [CrossRef]
- Herner, A.; Heilmaier, M.; Mayr, U.; Schmid, R.M.; Huber, W. Comparison of cardiac function index derived from femoral and jugular indicator injection for transpulmonary thermodilution with the PiCCO-device: A prospective observational study. PLoS ONE 2018, 13, e0200740. [Google Scholar] [CrossRef] [PubMed]
- Herner, A.; Heilmaier, M.; Mayr, U.; Schmid, R.M.; Huber, W. Comparison of global end-diastolic volume index derived from jugular and femoral indicator injection: A prospective observational study in patients equipped with both a PiCCO-2 and an EV-1000-device. Sci. Rep. 2020, 10, 20773. [Google Scholar] [CrossRef] [PubMed]
- Herner, A.; Lahmer, T.; Mayr, U.; Rasch, S.; Schneider, J.; Schmid, R.M.; Huber, W. Transpulmonary thermodilution before and during veno-venous extra-corporeal membrane oxygenation ECMO: An observational study on a potential loss of indicator into the extra-corporeal circuit. J. Clin. Monit. Comput. 2020, 34, 923–936. [Google Scholar] [CrossRef] [PubMed]
- Minini, A.; Raes, M.; Taccone, F.S.; Malbrain, M.L.N.G. Transpulmonary thermodilution during extracorporeal organ support (ECOS): Is it worth it?A brief commentary on the effects of the extracorporeal circuit on TPTD-derived parameters. J. Clin. Monit. Comput. 2021, 35, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Fichtner, F.; Mörer, O.; Laudi, S.; Weber-Carstens, S.; Kaisers, U. Webinar zur S3-Leitlinie Invasive Beatmung und Einsatz extrakorporaler Verfahren bei akuter respiratorischer Insuffizienz. Chirurg 2021, 92, 851–852. [Google Scholar] [CrossRef]
- Tonna, J.E.; Abrams, D.; Brodie, D.; Greenwood, J.C.; Rubio Mateo-Sidron, J.A.; Usman, A.; Fan, E. Management of Adult Patients Supported with Venovenous Extracorporeal Membrane Oxygenation (VV ECMO): Guideline from the Extracorporeal Life Support Organization (ELSO). Asaio J. 2021, 67, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Oren-Grinberg, A. The PiCCO Monitor. Int. Anesthesiol. Clin. 2010, 48, 57–85. [Google Scholar] [CrossRef] [PubMed]
- Saugel, B.; Umgelter, A.; Schuster, T.; Phillip, V.; Schmid, R.M.; Huber, W. Transpulmonary thermodilution using femoral indicator injection: A prospective trial in patients with a femoral and a jugular central venous catheter. Crit. Care 2010, 14, R95. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, S.; Westhoff, T.H.; Hofmann, C.; Schaefer, J.-H.; Zidek, W.; Compton, F.; van der Giet, M. Effect of the venous catheter site on transpulmonary thermodilution measurement variables. Crit. Care Med. 2007, 35, 783–786. [Google Scholar] [CrossRef] [PubMed]
- Beitz, A.; Berbara, H.; Mair, S.; Henschel, B.; Lahmer, T.; Rasch, S.; Schmid, R.; Huber, W. Consistency of cardiac function index and global ejection fraction with global end-diastolic volume in patients with femoral central venous access for transpulmonary thermodilution: A prospective observational study. J. Clin. Monit. Comput. 2017, 31, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Haller, M.; Zöllner, C.; Manert, W.; Briegel, J.; Kilger, E.; Polasek, J.; Hummel, T.; Forst, H.; Peter, K. Thermodilution cardiac output may be incorrect in patients on venovenous extracorporeal lung assist. Am. J. Respir. Crit. Care Med. 1995, 152, 1812–1817. [Google Scholar] [CrossRef] [PubMed]
- Sreenan, C.; Osiovich, H.; Cheung, P.Y.; Lemke, R.P. Quantification of recirculation by thermodilution during venovenous extracorporeal membrane oxygenation. J. Pediatr. Surg. 2000, 35, 1411–1414. [Google Scholar] [CrossRef] [PubMed]
- Sakka, S.G.; Hanusch, T.; Thuemer, O.; Wegscheider, K. The influence of venovenous renal replacement therapy on measurements by the transpulmonary thermodilution technique. Anesth. Analg. 2007, 105, 1079–1082. [Google Scholar] [CrossRef] [PubMed]
- Huber, W.; Fuchs, S.; Minning, A.; Küchle, C.; Braun, M.; Beitz, A.; Schultheiss, C.; Mair, S.; Phillip, V.; Schmid, S.; et al. Transpulmonary thermodilution (TPTD) before, during and after Sustained Low Efficiency Dialysis (SLED). A Prospective Study on Feasibility of TPTD and Prediction of Successful Fluid Removal. PLoS ONE 2016, 11, e0153430. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Cao, Y.; Lu, W.; Li, J. CRRT influences PICCO measurements in febrile critically ill patients. Open Med. 2022, 17, 245–252. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | (Mean ± SD, Percentages) |
|---|---|
| Sex [male:female, n] | 0:2 |
| Age [years] | 57.50 ± 3.54 |
| Weight [kg] | 87.50 ± 31.82 |
| BMI [kg/m2] | 28.22 ± 8.10 |
| BSA [m2] | 2.02 ± 0.38 |
| Measurements (n = 28) | |
| ABPs [mmHg] | 101.00 ± 36.77 |
| ABPd [mmHg] | 47.47 ± 18.03 |
| HR [bpm] | 67.07 ± 26.47 |
| sinus rhythm [%] | 100 |
| mCVP [cmH2O] | 8.37 ± 4.36 |
| ECBF [L/min] | 3.24 ± 0.65 |
| Mechanical ventilation [%] | 100 |
| Norepinephrine [%] | 74.19 |
| Norepinephrine [µg/kg/h] | 5.26 ± 19.43 |
| Comorbidities | |
| Renal replacement therapy [n] | 0/2 |
| Valvular diseases [n] | 0/2 |
| Coronary heart disease [n] | 0/2 |
| Peripheral artery disease [n] | 0/2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopp, S.; Windschmitt, J.; Schnauder, L.; Münzel, T.; Keller, K.; Karbach, S.; Hobohm, L.; Lurz, P.; Sagoschen, I.; Wild, J. Injection Site Matters: A Comparative Analysis of Transpulmonary Thermodilution via Simultaneous Femoral and Jugular Indicator Injections under Veno-Venous Extracorporeal Membrane Oxygenation Therapy. J. Clin. Med. 2024, 13, 2334. https://doi.org/10.3390/jcm13082334
Kopp S, Windschmitt J, Schnauder L, Münzel T, Keller K, Karbach S, Hobohm L, Lurz P, Sagoschen I, Wild J. Injection Site Matters: A Comparative Analysis of Transpulmonary Thermodilution via Simultaneous Femoral and Jugular Indicator Injections under Veno-Venous Extracorporeal Membrane Oxygenation Therapy. Journal of Clinical Medicine. 2024; 13(8):2334. https://doi.org/10.3390/jcm13082334
Chicago/Turabian StyleKopp, Sabrina, Johannes Windschmitt, Lena Schnauder, Thomas Münzel, Karsten Keller, Susanne Karbach, Lukas Hobohm, Philipp Lurz, Ingo Sagoschen, and Johannes Wild. 2024. "Injection Site Matters: A Comparative Analysis of Transpulmonary Thermodilution via Simultaneous Femoral and Jugular Indicator Injections under Veno-Venous Extracorporeal Membrane Oxygenation Therapy" Journal of Clinical Medicine 13, no. 8: 2334. https://doi.org/10.3390/jcm13082334
APA StyleKopp, S., Windschmitt, J., Schnauder, L., Münzel, T., Keller, K., Karbach, S., Hobohm, L., Lurz, P., Sagoschen, I., & Wild, J. (2024). Injection Site Matters: A Comparative Analysis of Transpulmonary Thermodilution via Simultaneous Femoral and Jugular Indicator Injections under Veno-Venous Extracorporeal Membrane Oxygenation Therapy. Journal of Clinical Medicine, 13(8), 2334. https://doi.org/10.3390/jcm13082334