

PlasmaBlade versus Electrocautery for Deep Inferior Epigastric Perforator Flap Harvesting in Autologous Breast Reconstruction: A Comparative Clinical Outcome Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Risk Factors
3.2. Postoperative Complications and Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Allen, R.J.; Treece, P. Deep Inferior Epigastric Perforator Flap for Breast Reconstruction. Ann. Plast. Surg. 1994, 32, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Healy, C.; Allen, R.J. The Evolution of Perforator Flap Breast Reconstruction: Twenty Years after the First DIEP Flap. J. Reconstr. Microsurg. 2014, 30, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Granzow, J.W.; Levine, J.L.; Chiu, E.S.; Allen, R.J. Breast Reconstruction with the Deep Inferior Epigastric Perforator Flap: History and an Update on Current Technique. J. Plast. Reconstr. Aesthetic Surg. 2006, 59, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Santosa, K.B.; Qi, J.; Kim, H.M.; Hamill, J.B.; Wilkins, E.G.; Pusic, A.L. Long-Term Patient-Reported Outcomes in Postmastectomy Breast Reconstruction. JAMA Surg. 2018, 153, 891. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.A.; Allen, R.J.; Polanco, T.; Shamsunder, M.; Patel, A.R.; McCarthy, C.M.; Matros, E.; Dayan, J.H.; Disa, J.J.; Cordeiro, P.G.; et al. Long-Term Patient-Reported Outcomes following Postmastectomy Breast Reconstruction: An 8-Year Examination of 3268 Patients. Ann. Surg. 2019, 270, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Miseré, R.M.; van Kuijk, S.M.; Claassens, E.L.; Heuts, E.M.; Piatkowski, A.A.; van der Hulst, R.R. Breast-Related and Body-Related Quality of Life Following Autologous Breast Reconstruction Is Superior to Implant-Based Breast Reconstruction—A Long-Term Follow-Up Study. Breast 2021, 59, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Messenger, D.; Carter, F.; Noble, E.; Francis, N. Electrosurgery and Energized Dissection. Surgery 2020, 38, 133–138. [Google Scholar] [CrossRef]
- Loh, S.A.; Carlson, G.A.; Chang, E.I.; Huang, E.; Palanker, D.; Gurtner, G.C. Comparative Healing of Surgical Incisions Created by the PEAK Plasmablade, Conventional Electrosurgery, and a Scalpel. Plast. Reconstr. Surg. 2009, 124, 1849–1859. [Google Scholar] [CrossRef] [PubMed]
- Palanker, D.V.; Vankov, A.; Huie, P. Electrosurgery with Cellular Precision. IEEE Trans. Biomed. Eng. 2008, 55, 838–841. [Google Scholar] [CrossRef]
- Ruidiaz, M.E.; Messmer, D.; Atmodjo, D.Y.; Vose, J.G.; Huang, E.J.; Kummel, A.C.; Rosenberg, H.L.; Gurtner, G.C. Comparative Healing of Human Cutaneous Surgical Incisions Created by the PEAK PlasmaBlade, Conventional Electrosurgery, and a Standard Scalpel. Plast. Reconstr. Surg. 2011, 128, 104–111. [Google Scholar] [CrossRef]
- Schlosshauer, T.; Kiehlmann, M.; Riener, M.O.; Rothenberger, J.; Sader, R.; Rieger, U.M. Effect of Low-Thermal Dissection Device versus Conventional Electrocautery in Mastectomy for Female-to-Male Transgender Patients. Int. Wound J. 2020, 17, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- Xiao, X.; Ye, L. Efficacy and Safety of Scarpa Fascia Preservation during Abdominoplasty: A Systematic Review and Meta-Analysis. Aesthetic Plast. Surg. 2017, 41, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Wormald, J.C.R.; Wade, R.G.; Figus, A. The Increased Risk of Adverse Outcomes in Bilateral Deep Inferior Epigastric Artery Perforator Flap Breast Reconstruction Compared to Unilateral Reconstruction: A Systematic Review and Meta-Analysis. J. Plast. Reconstr. Aesthetic Surg. 2014, 67, 143–156. [Google Scholar] [CrossRef] [PubMed]
- Salgarello, M.; Tambasco, D.; Farallo, E. DIEP Flap Donor Site Versus Elective Abdominoplasty Short-Term Complication Rates: A Meta-Analysis. Aesthetic Plast. Surg. 2012, 36, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.Y.L.; Onggo, J.; Serag, S.; Phan, K.; Dusseldorp, J.R. Deep Inferior Epigastric Perforator (DIEP) Flap Safety Profile in Slim versus Non-Slim BMI Patients: A Systematic Review and Meta-Analysis. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 2180–2189. [Google Scholar] [CrossRef] [PubMed]
- Mani, M.; Wang, T.; Harris, P.; James, S. Breast Reconstruction with the Deep Inferior Epigastric Perforator Flap is a Reliable Alternative In Slim Patients. Microsurgery 2016, 36, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Schlosshauer, T.; Kiehlmann, M.; Rothenberger, J.; Sader, R.; Rieger, U.M. Bilateral Reduction Mammaplasty with Pulsed Electron Avalanche Knife PlasmabladeTM and Conventional Electrosurgical Surgery: A Retrospective, Randomised Controlled Clinical Trial. Int. Wound J. 2020, 17, 1695–1701. [Google Scholar] [CrossRef]
- Schlosshauer, T.; Kiehlmann, M.; Riener, M.O.; Sader, R.; Rieger, U.M. Comparative Analysis on the Effect of Low-Thermal Plasma Dissection Device (PEAK PlasmaBlade) vs. Conventional Electrosurgery in Post-Bariatric Abdominoplasty: A Retrospective Randomised Clinical Study. Int. Wound J. 2019, 16, 1494–1502. [Google Scholar] [CrossRef]
- Sowa, Y.; Inafuku, N.; Kodama, T.; Morita, D.; Numajiri, T. Preventive Effect on Seroma of Use of Peak Plasmablade after Latissimus Dorsi Breast Reconstruction. Plast. Reconstr. Surg. Glob. Open 2018, 6, e2035. [Google Scholar] [CrossRef] [PubMed]
- Dogan, L.; Gulcelik, M.A.; Yuksel, M.; Uyar, O.; Erdogan, O.; Reis, E. The Effect of Plasmakinetic Cautery on Wound Healing and Complications in Mastectomy. J. Breast Cancer 2013, 16, 198–201. [Google Scholar] [CrossRef]
- Friebel, T.R.; Narayan, N.; Ramakrishnan, V.; Morgan, M.; Cellek, S.; Griffiths, M. Comparison of PEAK PlasmaBladeTM to Conventional Diathermy in Abdominal-Based Free-Flap Breast Reconstruction Surgery—A Single-Centre Double-Blinded Randomised Controlled Trial. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1731–1742. [Google Scholar] [CrossRef] [PubMed]
- Chiappa, C.; Fachinetti, A.; Boeri, C.; Arlant, V.; Rausei, S.; Dionigi, G.; Rovera, F. Wound Healing and Postsurgical Complications in Breast Cancer Surgery: A Comparison between PEAK PlasmaBlade and Conventional Electrosurgery—A Preliminary Report of a Case Series. Ann. Surg. Treat. Res. 2018, 95, 129–134. [Google Scholar] [CrossRef]
- Clavien, P.A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-Year Experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef]
- Yilmaz, K.B.; Dogan, L.; Nalbant, H.; Akinci, M.; Karaman, N.; Ozaslan, C.; Kulacoglu, H. Comparing Scalpel, Electrocautery and Ultrasonic Dissector Effects: The Impact on Wound Complications And Pro-Inflammatory Cytokine Levels in Wound Fluid from Mastectomy Patients. J. Breast Cancer 2011, 14, 58. [Google Scholar] [CrossRef]
- Duscher, D.; Aitzetmüller, M.M.; Shan, J.J.; Wenny, R.; Brett, E.A.; Staud, C.J.; Kiesl, D.; Huemer, G.M. Comparison of Energy-Based Tissue Dissection Techniques in Abdominoplasty: A Randomized, Open-Label Study Including Economic Aspects. Aesthetic Surg. J. 2019, 39, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Chow, W.T.H.; Oni, G.; Ramakrishnan, V.V.; Griffiths, M. The Use of Plasmakinetic Cautery Compared to Conventional Electrocautery for Dissection of Abdominal Free Flap for Breast Reconstruction: Single-Centre, Randomized Controlled Study. Gland Surg. 2019, 8, 242–248. [Google Scholar] [CrossRef]
- Chen, A.W.G.; Chen, M.K. Comparison of Post-Tonsillectomy Hemorrhage between Monopolar and Plasma Blade Techniques. J. Clin. Med. 2021, 10, 2051. [Google Scholar] [CrossRef] [PubMed]
- Lane, J.C.; Dworkin-Valenti, J.; Chiodo, L.; Haupert, M. Postoperative Tonsillectomy Bleeding Complications in Children: A Comparison of Three Surgical Techniques. Int. J. Pediatr. Otorhinolaryngol. 2016, 88, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Thottam, P.J.; Christenson, J.R.; Cohen, D.S.; Metz, C.M.; Saraiya, S.S.; Haupert, M.S. The Utility of Common Surgical Instruments for Pediatric Adenotonsillectomy. Laryngoscope 2015, 125, 475–479. [Google Scholar] [CrossRef] [PubMed]
- Kypta, A.; Blessberger, H.; Saleh, K.; Hönig, S.; Kammler, J.; Neeser, K.; Steinwender, C. An Electrical Plasma Surgery Tool for Device Replacement—Retrospective Evaluation of Complications and Economic Evaluation of Costs and Resource Use. Pacing Clin. Electrophysiol. 2015, 38, 28–34. [Google Scholar] [CrossRef]
- Decker, M.R.; Greenblatt, D.Y.; Havlena, J.; Wilke, L.G.; Greenberg, C.C.; Neuman, H.B. Impact of Neoadjuvant Chemotherapy on Wound Complications after Breast Surgery. Surgery 2012, 152, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Azzawi, K.; Ismail, A.; Earl, H.; Forouhi, P.; Malata, C.M. Influence of Neoadjuvant Chemotherapy on Outcomes of Immediate Breast Reconstruction. Plast. Reconstr. Surg. 2010, 126, 22. [Google Scholar] [CrossRef] [PubMed]
- Bowen, M.E.; Mone, M.C.; Buys, S.S.; Sheng, X.; Nelson, E.W. Surgical Outcomes for Mastectomy Patients Receiving Neoadjuvant Chemotherapy. Ann. Surg. 2017, 265, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.; Gohari, S.S.; Rizki, H.; Faheem, I.; Langridge, B.; Kümmel, S.; Johnson, L.; Schmid, P. A Systematic Review and Meta-Analysis on the Effect of Neoadjuvant Chemotherapy on Complications Following Immediate Breast Reconstruction. Breast 2021, 55, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Zhang, X.; Liu, Q.; Peng, J.; Liang, X.; Shen, Y.; Liu, H.; Li, H. Impact of Neoadjuvant Chemotherapy on Immediate Breast Reconstruction: A Meta-Analysis. PLoS ONE 2014, 9, e98225. [Google Scholar] [CrossRef] [PubMed]
- Heidekrueger, P.I.; Fritschen, U.; Moellhoff, N.; Germann, G.; Giunta, R.E.; Zeman, F.; Prantl, L. Impact of Body Mass Index on Free DIEP Flap Breast Reconstruction: A Multicenter Cohort Study. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 1718–1724. [Google Scholar] [CrossRef] [PubMed]
- Kearns, S.R.; Connolly, E.M.; Mcnally, S.; Mcnamara, D.A.; Deasy, J. Randomized Clinical Trial of Diathermy versus Scalpel Incision in Elective Midline Laparotomy. Br. J. Surg. 2000, 88, 41–44. [Google Scholar] [CrossRef]
- Chrysos, E.; Athanasakis, E.; Antonakakis, S.; Zoras, O. A Prospective Study Comparing Diathermy and Scalpel Incisions in Tension-Free Inguinal Hernioplasty. Am. Surg. 2005, 71, 326–329. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PPB | MPE | ||
|---|---|---|---|
| n | 56 | 72 | |
| Mean (±std) | Mean (±std) | p-Value | |
| Age | 49.68 (±10.50) | 48.67 (±9.56) | 0.5733 |
| BMI | 25.37 (±3.85) | 25.33 (±4.01) | 0.9612 |
| Flap volume (mL) | 617.16 (±283.66) | 608.27 (±322.90) | 0.8572 |
| n (%) | n% | p-value | |
| Female | 56 (100) | 72 (100) | >0.999 |
| Indication | |||
| Carcinoma | 53 (94.64) | 71 (98.61) | 0.2005 |
| Prophylactic | 3 (5.36) | 1 (1.39) | |
| Breast reconstruction | |||
| Unilateral | 34 (60.7) | 55 (76.4) | 0.0560 |
| Bilateral | 22 (39.3) | 17 (23.6) | |
| Nicotine | |||
| Yes | 6 (10.71) | 12 (16.67) | 0.3366 |
| No | 50 (89.29) | 60 (83.33) | |
| Diabetes | |||
| Yes | 1 (1.79) | 0 (0.00) | 0.3918 |
| No | 55 (98.21) | 72 (100.00) | |
| Neoadjuvant chemotherapy | |||
| Yes | 21 (37.50) | 24 (33.33) | 0.6243 |
| No | 35 (62.50) | 48 (66.67) | |
| BMI | 0.9692 | ||
| BMI < 25 kg/m2 | 32 (57.14) | 40 (55.55) | |
| BMI 25–30 kg/m2 | 15 (26.79) | 21 (29.17) | |
| BMI > 30 kg/m2 | 9 (16.07) | 11 (15.28) |
| PPB | MPE | ||
|---|---|---|---|
| Outcome | Mean (±std) | Mean (±std) | p-Value |
| Number of suction drainages | 2.00 (±0.00) | 1.99 (±0.12) | 0.3799 |
| Duration of draining (days) | 6.18 (±1.69) | 6.29 (±1.72) | 0.7128 |
| Hospitalization (days) | 10.86 (±2.29) | 11.13 (±3.00) | 0.5828 |
| Total wound fluid quantity (mL) | 279.38 (±183.38) | 351.11 (±185.96) | 0.0324 * |
| Seroma (mL) and risk factors | |||
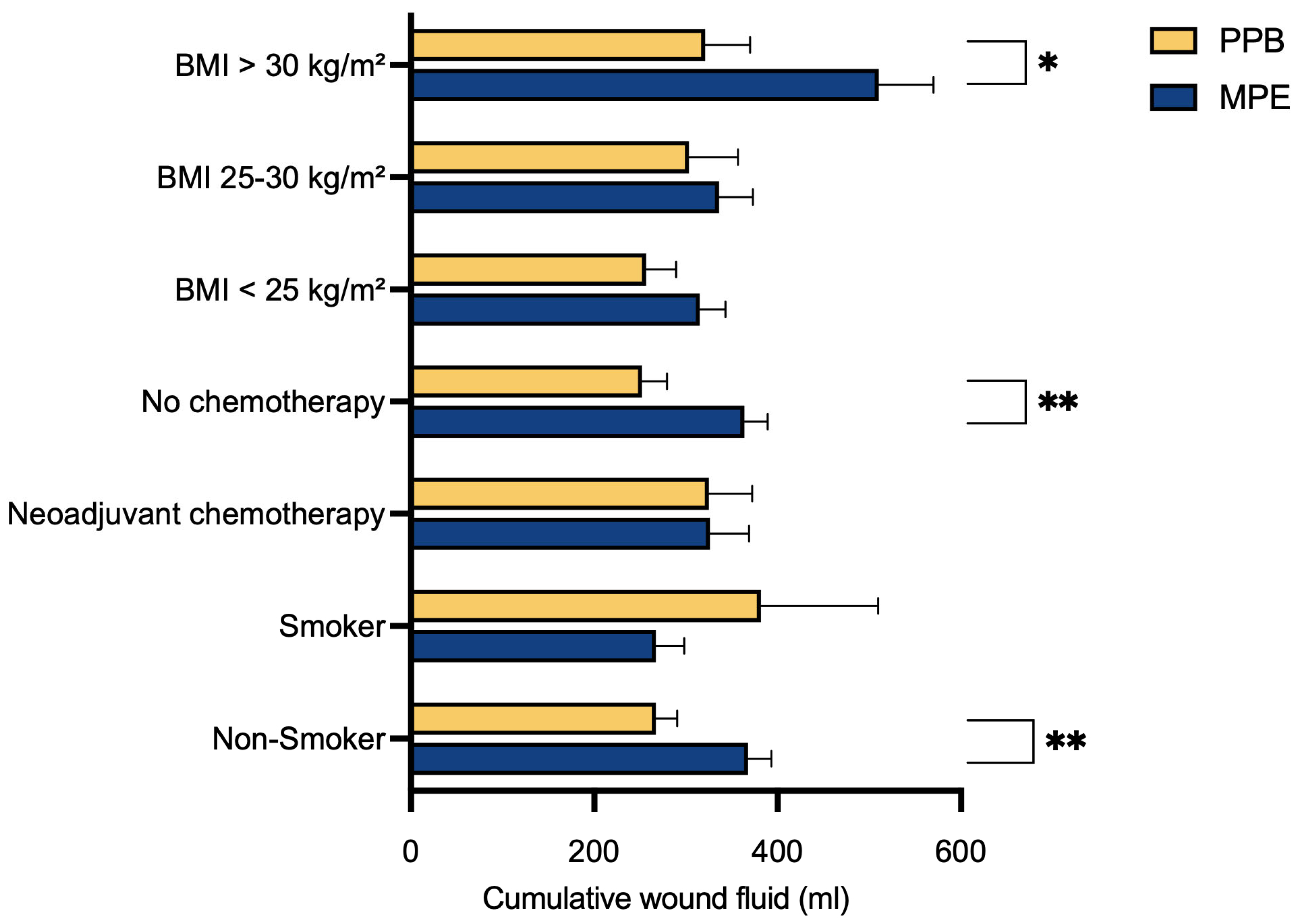
| Non-Smoker | 267.10 (±164.21) | 367.92 (±195.73) | 0.0046 ** |
| Smoker | 381.67 (±313.52) | 267.08 (±107.84) | 0.2612 |
| Adjuvant Chemotherapy | 325.00 (±215.56) | 326.04 (±209.19) | 0.9870 |
| No Chemotherapy | 252.00 (±161.23) | 363.65 (±176.29) | 0.0041 ** |
| BMI < 25 kg/m2 | 256.41 (±186.32) | 315.25 (±175.01) | 0.1727 |
| BMI 25–30 kg/m2 | 303.33 (±206.08) | 335.95 (±168.64) | 0.6053 |
| BMI > 30 kg/m2 | 321.11 (±146.33) | 510.45 (±197.74) | 0.0284 * |
| PPB | MPE | ||
|---|---|---|---|
| Drain Dwelling Time (d) | Mean (±std) | Mean (±std) | p-Value |
| Non-Smoker | 6.10 (±1.50) | 6.35 (±1.71) | 0.4210 |
| No chemotherapy | 6.09 (±1.50) | 6.35 (±1.62) | 0.4440 |
| BMI > 30 kg/m2 | 6.67 (±1.87) | 7.55 (±1.75) | 0.2933 |
| Hospitalization (d) | |||
| Non-Smoker | 10.86 (±2.35) | 11.00 (±2.26) | 0.7513 |
| No chemotherapy | 10.94 (±2.71) | 11.02 (±3.22) | 0.9077 |
| BMI > 30 kg/m2 | 11.44 (±4.03) | 11.73 (±1.19) | 0.8267 |
| PPB | MPE | ||
|---|---|---|---|
| Mean (±std) | Mean (±std) | p-Value | |
| Unilateral | 248.53 (±177.81) | 357.09 (±184.89) | 0.0077 ** |
| Bilateral | 327.05 (±189.92) | 331.76 (±199.31) | 0.9404 |
| Unilateral reconstruction | Bilateral reconstruction | ||
| mean (±std) | mean (±std) | p-value | |
| All patients (n = 128) | 315.62 (±188.80) | 329.10 (±191.48) | 0.7118 |
| PPB | MPE | ||
|---|---|---|---|
| n (%) | n% | p-Value | |
| Complications | 13 (23.21) | 23 (31.94) | 0.2758 |
| Bleeding/Hematoma | 4 (7.14) | 4 (5.56) | 0.7128 |
| Clavien–Dindo | |||
| 1 | 5 (8.93) | 10 (13.89) | |
| Bleeding/Hematoma | 2 (3.57) | 1 (1.39) | |
| Wound healing complications | 3 (5.36) | 7 (9.72) | |
| Seroma | 0 (0.00) | 2 (2.78) | |
| 2 | 0 (0.00) | 0 (0.00) | |
| 3a | 0 (0.00) | 2 (2.78) | |
| Wound healing complications | 0 (0.00) | 2 (2.78) | |
| 3b | 8 (14.29) | 11 (15.28) | |
| Bleeding/Hematoma | 2 (3.57) | 3 (4.17) | |
| Wound healing complications | 6 (10.71) | 8 (11.11) |
| PPB | MPE | ||
|---|---|---|---|
| Mean (±std) | Mean (±std) | p-Value | |
| Day 1 | 2.36 (±1.52) | 2.00 (±1.81) | 0.4994 |
| Day 2 | 2.23 (±1.47) | 3.09 (±1.73) | 0.0080 ** |
| Day 3 | 2.08 (±1.62) | 2.67 (±1.71) | 0.0683 |
| Day 4 | 1.71 (±1.18) | 2.27 (±1.70) | 0.0512 |
| Day 5 | 1.73 (±1.59) | 1.65 (±1.50) | 0.7855 |
| Day 6 | 1.29 (±1.12) | 1.82 (±1.87) | 0.0729 |
| Day 7 | 0.88 (±0.93) | 1.55 (±1.52) | 0.0065 ** |
| Day 8 | 1.27 (±1.35) | 1.49 (±1.66) | 0.4455 |
| Day 9 | 1.07 (±1.18) | 1.89 (±1.78) | 0.0153 ** |
| Day 10 | 1.23 (±1.34) | 1.61 (±1.48) | 0.2928 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustin, A.; Schoberleitner, I.; Unterhumer, S.-M.; Krapf, J.; Bauer, T.; Wolfram, D. PlasmaBlade versus Electrocautery for Deep Inferior Epigastric Perforator Flap Harvesting in Autologous Breast Reconstruction: A Comparative Clinical Outcome Study. J. Clin. Med. 2024, 13, 2388. https://doi.org/10.3390/jcm13082388
Augustin A, Schoberleitner I, Unterhumer S-M, Krapf J, Bauer T, Wolfram D. PlasmaBlade versus Electrocautery for Deep Inferior Epigastric Perforator Flap Harvesting in Autologous Breast Reconstruction: A Comparative Clinical Outcome Study. Journal of Clinical Medicine. 2024; 13(8):2388. https://doi.org/10.3390/jcm13082388
Chicago/Turabian StyleAugustin, Angela, Ines Schoberleitner, Sophie-Marie Unterhumer, Johanna Krapf, Thomas Bauer, and Dolores Wolfram. 2024. "PlasmaBlade versus Electrocautery for Deep Inferior Epigastric Perforator Flap Harvesting in Autologous Breast Reconstruction: A Comparative Clinical Outcome Study" Journal of Clinical Medicine 13, no. 8: 2388. https://doi.org/10.3390/jcm13082388
APA StyleAugustin, A., Schoberleitner, I., Unterhumer, S. -M., Krapf, J., Bauer, T., & Wolfram, D. (2024). PlasmaBlade versus Electrocautery for Deep Inferior Epigastric Perforator Flap Harvesting in Autologous Breast Reconstruction: A Comparative Clinical Outcome Study. Journal of Clinical Medicine, 13(8), 2388. https://doi.org/10.3390/jcm13082388