
Total Knee Arthroplasty in People with Hemophilia: Higher Incidence of Periprosthetic Joint Infection and 1-Year Revision/Re-Operation than the General Population and Lower Prosthetic Survival When Early Postoperative Bleeding Complications Occurred: Current Literature Review

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Perioperative Hemostasis
3. Surgical Approach
4. Results and Complications
5. Prosthetic Survival
6. Discussion
7. Conclusions
8. Limitations and Future Direction
Author Contributions
Funding
Conflicts of Interest
References
- Rodriguez-Merchan, E.C.; Jimenez-Yuste, V. Pathophysiology of Hemophilia. In Advances in Hemophilia Treatment: From Genetics to Joint Health; Rodriguez-Merchan, E.C., Ed.; Springer Nature: Cham, Switzerland, 2022; pp. 1–9. [Google Scholar]
- Dolan, G.; Benson, G.; Duffy, A.; Hermans, C.; Jimenez-Yuste, V.; Lambert, T.; Ljung, R.; Morfini, M.; Šalek, S.Z. Haemophilia B: Where are we now and what does the future hold? Blood Rev. 2018, 32, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Valentino, L.A.; Khair, K. Prophylaxis for hemophilia A without inhibitors: Treatment options and considerations. Expert Rev. Hematol. 2020, 13, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Lambert, C.; Meité, N.; Sanogo, I.; Lobet, S.; Hermans, C. Feasibility and outcomes of low-dose and low-frequency prophylaxis with recombinant extended half-life products (Fc-rFVIII and Fc-rFIX) in Ivorian children with hemophilia: Two-year experience in the setting of World Federation of Haemophilia humanitarian aid programme. Haemophilia 2021, 27, 33–40. [Google Scholar] [PubMed]
- Jimenez-Yuste, V.; Auerswald, G.; Benson, G.; Dolan, G.; Hermans, C.; Lambert, T.; Ljung, R.; Morfini, M.; Santagostino, E.; Šalek, S.Z. Practical considerations for nonfactor-replacement therapies in the treatment of haemophilia with inhibitors. Haemophilia 2021, 27, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Carulli, C.; Civinini, R.; Martini, C.; Linari, S.; Morfini, M.; Tani, M.; Innocenti, M. Viscosupplementation in haemophilic arthropathy: A long-term follow-up study. Haemophilia 2012, 18, e210–e214. [Google Scholar] [CrossRef] [PubMed]
- De la Corte-Rodriguez, H.; Rodriguez-Merchan, E.C. The role of physical medicine and rehabilitation in haemophiliac patients. Blood Coagul. Fibrinolysis 2013, 24, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Stephensen, D.; Bladen, M.; McLaughlin, P. Recent advances in musculoskeletal physiotherapy for haemophilia. Ther. Adv. Hematol. 2018, 9, 227–237. [Google Scholar] [PubMed]
- McLaughlin, P.; Hurley, M.; Chowdary, P.; Khair, K.; Stephensen, D. Physiotherapy interventions for pain management in haemophilia: A systematic review. Haemophilia 2020, 26, 667–684. [Google Scholar] [CrossRef] [PubMed]
- Solimeno, L.P.; Mancuso, M.E.; Pasta, G.; Santagostino, E.; Perfetto, S.; Mannucci, P.M. Factors influencing the long-term outcome of primary total knee replacement in haemophiliacs: A review of 116 procedures at a single institution. Br. J. Haematol. 2009, 145, 227–234. [Google Scholar] [PubMed]
- Rodriguez-Merchan, E.C. Total knee arthroplasty in hemophilic arthropathy. Am. J. Orthop. Bellem Mead NJ 2015, 44, E503–E507. [Google Scholar]
- Pasta, G.; Vanelli, R.; Jannelli, E.; Castelli, A.; Mosconi, M.; Preti, P.S.; Ambaglio, C.; Benazzo, F. Primary total knee replacement in hemophiliacs: Experience of a single institution over fourteen years of surgical procedures. J. Biol. Regul. Homeost. Agents 2018, 32 (Suppl. S1), 145–150. [Google Scholar] [PubMed]
- Lachiewicz, P.F.; Inglis, A.E.; Insall, J.N.; Sculco, T.P.; Hilgartner, M.W.; Bussel, J.B. Total knee arthroplasty in hemophilia. Bone Jt. Surg. Am. 1985, 67, 1361–13666. [Google Scholar] [CrossRef]
- Goldberg, V.M.; Heiple, K.G.; Ratnoff, O.D.; Kurczynski, E.; Arvan, G. Total knee arthroplasty in classic hemophilia. J. Bone Jt. Surg. Am. 1981, 63, 695–701. [Google Scholar] [CrossRef]
- Norian, J.M.; Ries, M.D.; Karp, S.; Hambleton, J. Total knee arthroplasty in hemophilic arthropathy. J. Bone Jt. Surg. Am. 2002, 84, 1138–1141. [Google Scholar] [CrossRef] [PubMed]
- Legroux-Gérot, I.; Strouk, G.; Parquet, A.; Goodemand, J.; Gougeon, F.; Duquesnoy, B. Total knee arthroplasty in hemophilic arthropathy. Jt. Bone Spine 2003, 70, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Sheth, D.S.; Oldfield, D.; Ambrose, C.; Clyburn, T. Total knee arthroplasty in hemophilic arthropathy. J. Arthroplast. 2004, 19, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Bae, D.K.; Yoon, K.H.; Kim, H.S.; Song, S.J. Total knee arthroplasty in hemophilic arthropathy of the knee. J. Arthroplast. 2005, 20, 664–668. [Google Scholar]
- Silva, M.; Luck, J.V., Jr. Long-term results of primary total knee replacement in patients with hemophilia. J. Bone Jt. Surg. Am. 2005, 87, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Solimeno, L.; Goddard, N.; Pasta, G.; Mohanty, S.; Mortazavi, S.; Pacheco, L.; Sohail, T.; Luck, J. Management of arthrofibrosis in haemophilic arthropathy. Haemophilia 2010, 16 (Suppl. S5), 115–120. [Google Scholar] [CrossRef] [PubMed]
- Rahmé, M.; Ehlinger, M.; Faradji, A.; Gengenwin, N.; Lecocq, J.; Sibilia, J.; Bonnomet, F. Total knee arthroplasty in severe haemophilic patients under continuous infusion of clotting factors. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 1781–1786. [Google Scholar] [CrossRef] [PubMed]
- Cho, K.Y.; Kim, K.I.; Khurana, S.; Cho, S.W.; Kang, D.G. Computer-navigated total knee arthroplasty in haemophilic arthropathy. Haemophilia 2013, 19, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Strauss, A.C.; Schmolders, J.; Friedrich, M.J.; Pflugmacher, R.; Müller, M.C.; Goldmann, G.; Oldenburg, J.; Pennekamp, P.H. Outcome after total knee arthroplasty in haemophilic patients with stiff knees. Haemophilia 2015, 21, e300–e305. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.M.; Haghpanah, B.; Ebrahiminasab, M.M.; Baghdadi, T.; Toogeh, G. Functional outcome of total knee arthroplasty in patients with haemophilia. Haemophilia 2016, 22, 919–924. [Google Scholar] [CrossRef] [PubMed]
- Mortazavi, S.M.J.; Haghpanah, B.; Ebrahiminasab, M.M.; Baghdadi, T.; Hantooshzadeh, R.; Toogeh, G. Simultaneous bilateral total knee arthroplasty in patients with haemophilia: A safe and cost-effective procedure? Haemophilia 2016, 22, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.I.; Kim, D.K.; Juh, H.S.; Khurana, S.; Rhyu, K.H. Robot-assisted total knee arthroplasty in haemophilic arthropathy. Haemophilia 2016, 22, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Ernstbrunner, L.; Hingsammer, A.; Catanzaro, S.; Sutter, R.; Brand, B.; Wieser, K.; Fucentese, S.F. Long-term results of total knee arthroplasty in haemophilic patients: An 18-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3431–3438. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.S.; Shin, W.J.; Kim, K.I. Comparison of continuous infusion versus bolus injection of factor concentrates for blood management after total knee arthroplasty in patients with hemophilia. BMC Musculoskelet. Disord. 2017, 18, 356. [Google Scholar] [CrossRef]
- Rodriguez-Merchan, E.C.; Encinas-Ullan, C.A.; Gomez-Cardero, P. Intra-articular Tranexamic Acid in Primary Total Knee Arthroplasty Decreases the Rate of Post-operative Blood Transfusions in People with Hemophilia: A Retrospective Case-Control Study. HSS J. 2020, 16, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Santos Silva, M.; Rodrigues-Pinto, R.; Rodrigues, C.; Morais, S.; Costa E Castro, J. Long-term results of total knee arthroplasty in hemophilic arthropathy. J. Orthop. Surg. 2019, 27, 2309499019834337. [Google Scholar] [CrossRef]
- Oyarzun, A.; Barrientos, C.; Barahona, M.; Martinez, Á.; Soto-Arellano, V.; Courtin, C.; Cruz-Montecinos, C. Knee haemophilic arthropathy care in Chile: Midterm outcomes and complications after total knee arthroplasty. Haemophilia 2020, 26, e179–e186. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Feng, B.; Du, Y.; Wang, Y.; Bian, Y.; Weng, X. Complications of total knee arthroplasty in patients with haemophilia compared with osteoarthritis and rheumatoid arthritis: A 20-year single-surgeon cohort. Haemophilia 2020, 26, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Takedani, H. Risk of deep venous thrombosis after total knee arthroplasty in patients with haemophilia A. Haemophilia 2020, 26, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Rosas, S.; Buller, L.T.; Plate, J.; Higuera, C.; Barsoum, W.K.; Emory, C. Total knee arthroplasty among Medicare beneficiaries with hemophilia A and B is associated with increased complications and higher costs. J. Knee Surg. 2021, 34, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.F.; Yu, Y.B.; Tsai, S.W.; Chiu, J.W.; Hsiao, L.T.; Gau, J.P.; Hsu, H.-C. Total knee replacement for patients with severe hemophilic arthropathy in Taiwan: A nationwide population-based retrospective study. J. Chin. Med. Assoc. 2022, 85, 228–232. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Kim, J.H.; Kim, K.I. Risk factors for increased perioperative blood loss during total knee arthroplasty in patients with haemophilia. Haemophilia 2022, 28, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.N.; Wu, D.X.; Lv, S.J.; Tong, P.J. Hidden blood loss of total knee arthroplasty in hemophilia arthritis: An analysis of influencing factors. BMC Musculoskelet. Disord. 2022, 23, 587. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Wang, Z.; Gu, Y.; Zhang, J.; Wang, P.; Tong, P.; Lv, S. Total knee arthroplasty in patients with haemophilic arthropathy is effective and safe according to the outcomes at a mid-term follow-up. J. Orthop. Traumatol. 2022, 23, 31. [Google Scholar] [CrossRef]
- Canbolat, N.; Dinç, T.; Koltka, K.; Zulfikar, B.; Koç, B.; Kılıçoğlu, Ö.İ.; Buget, M.I. Comparison of analgesic consumption of hemophilic and non-hemophilic patients in knee arthroplasty. Turk. J. Trauma Emerg. Surg. 2022, 28, 1616–1621. [Google Scholar] [CrossRef]
- Goker, B.; Caglar, O.; Kinikli, G.I.; Aksu, S.; Tokgozoglu, A.M.; Atilla, B. Postoperative bleeding adversely affects total knee arthroplasty outcomes in hemophilia. Knee 2022, 39, 261–268. [Google Scholar] [CrossRef]
- Fenelon, C.; Murphy, E.P.; Fahey, E.J.; Murphy, R.P.; O’Connell, N.M.; Queally, J.M. Total knee arthroplasty in hemophilia: Survivorship and outcomes-A systematic review and meta-analysis. J. Arthroplast. 2022, 37, 581–592.e1. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Wang, Y.; Dong, X.; Li, Z.; Lin, J.; Weng, X. Long-term clinical outcomes following total knee arthroplasty in patients with hemophilic arthropathy: A single-surgeon cohort after a 10- to 17-year follow-up. Chin. Med. J. 2023, 136, 1478–1484. [Google Scholar] [CrossRef] [PubMed]
- Ono, K.; Hirose, J.; Noguchi, M.; Asano, K.; Yasuda, M.; Takedani, H. Extension contracture stiff knee in haemophilia: Surgical timing and procedure for total knee arthroplasty. Mod. Rheumatol. 2023, 33, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Carulli, C.; Innocenti, M.; Tambasco, R.; Perrone, A.; Civinini, R. Total knee arthroplasty in haemophilia: Long-term results and survival rate of a modern knee implant with an oxidized zirconium femoral component. J. Clin. Med. 2023, 12, 4356. [Google Scholar] [CrossRef] [PubMed]
- Challoumas, D.; Munn, D.; Jeyakumar, G.; Bagot, C.; Rodgers, R.; Kearns, R.; Jones, B. Outcomes of total hip and knee arthroplasty in patients with haemophilia: A meta-analysis of comparative studies and clinical practice recommendations. Haemophilia 2024, 30, 180–194. [Google Scholar] [CrossRef] [PubMed]
- Poston, J.N.; Kruse-Jarres, R. Perioperative hemostasis for patients with hemophilia. Hematol. Am. Soc. Hematol. Educ. Program 2022, 2022, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Roman, M.T. Hemostatic cover in orthopedic surgery. Blood Coagul. Fibrinolysis 2023, 34, S22–S25. [Google Scholar] [CrossRef] [PubMed]
- Hermans, C.; Apte, S.; Santagostino, E. Invasive procedures in patients with haemophilia: Review of low-dose protocols and experience with extended half-life FVIII and FIX concentrates and non-replacement therapies. Haemophilia 2021, 27 (Suppl. S3), 46–52. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.E.; Apte, S.; Hermans, C. Managing invasive procedures in haemophilia patients with limited resources, extended half-life concentrates or non-replacement therapies in 2022. Haemophilia 2022, 28 (Suppl. S4), 93–102. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Hemophilia A | Hemophilia B | |
|---|---|---|
| Preoperative peak factor activity objective | 80–100% | 60–80% |
| Postoperative peak factor activity objective | 60–80% (days 1–3) | 40–60% (days 1–3) |
| 40–60% (days 4–6) | 30–50% (days 4–6) | |
| 30–50% (days 7–14) | 20–40% (days 7–14) |
| Clotting Factor Concentrate (CFC) | Multiple CFC products are available for hemophilia A and B that can be used in the perioperative setting. The CFC product should be readily available at the site of surgery and postoperatively if needed, depending on the severity of the patient’s hemophilia and anticipated surgical risk. Most patients with hemophilia require CFC support in the perioperative setting. A preoperative bolus of CFC should be administered 30 to 60 min prior to the procedure. For patients without a history of an inhibitor, CFC dosing should be based on the patient’s weight, baseline factor levels, target factor level, and volume of distribution. Postoperative factor levels should be obtained depending on the half-life of the CFC: 8 to 12 h after the last dose of standard half-life FVIII CFCs and 12 to 24 h after the last dose of standard half-life FIX CFCs. If atypical or unexpected bleeding occurs, a stat factor level should be obtained to confirm sufficient levels, and alternative causes of bleeding should be considered, including anatomical drivers. |
| Bypassing Agents for Inhibitor Patients | Patients with FVIII or FIX inhibitors are typically treated with bypassing agents. The WFH recommends against the use of activated prothrombin complex concentrates (aPCCs; FVIII inhibitor bypass activity; FEIBA) for patients with congenital hemophilia B and inhibitors due to the risk of accumulation of clotting factors II, VII, and X, which can be associated with a higher risk of thrombotic complications. Rarely, patients with inhibitors may receive FVIII or FIX CFC when the inhibitor titer is negligible or low (<5 Bethesda units; BU), and CFC support is anticipated for a short duration with the understanding that reexposure to FVIII or FIX CFC results in an anamnestic response with a rise in the inhibitor titer and a loss of response to the CFC product. |
| Antifibrinolytics | The antifibrinolytics, tranexamic acid (TXA) and epsilon-aminocaproic acid, can be used as adjuvants for hemostatic support; these are particularly effective for mucosal bleeding. Overall, the use of TXA during major surgeries has not been shown to increase the risk of thromboembolism. |
| Authors [Reference] | Year | Methods | Results | Conclusions |
|---|---|---|---|---|
| Santos Silva et al. [30] | 2019 | Eighteen TKAs (15 PWH) during a 24-year period. Mean follow-up: 11.3 years. Mean age not available. | Ten-year survival rate with prosthesis removal as end point was 94.3%. Complication rate was 27.8% (two infections, two postoperative stiff knees, one instance of recurrent intra-articular bleeding). | TKA in PWH gave good clinical outcomes and survivor rates comparable to those of non-hemophilic patients. |
| Oyarzun et al. [31] | 2020 | 41 TKA (19 cases were bilateral). | Six individuals needed revision (6.66%) due to infection. TKA survival at 5 years was 92%. | TKA improved function and ROM. |
| Li et al. [32] | 2020 | 1515 individuals who experienced 2083 TKAs for osteoarthritis (OA), hemophilic arthropathy (HA), or rheumatoid arthritis (RA). | The overall complication rate in the HA cohort was 21.8%, which was much higher than the OA or RA group (7.1% and 8.7%, respectively). | Patients with hemophilia B and severe hemophilia had substantially higher complication rates. |
| Ono and Takedani [33] | 2020 | Eleven TKAs in PWH. Mean age: 50.5 years. | DVT was not encountered on either pre- or postoperative examinations by US, but contrast-enhanced CT detected DVT in two cases. No patients showed clinical signs of VTE during hospitalization. | Contrast-enhanced CT detected DVT in 18% of PWH A who experienced TKA despite no detection of DVT on US. |
| Rosas et al. [34] | 2021 | 4034 TKAs in PWH A and B were matched to controls using a 1:1 random matching process based on age, gender, CCI, and select comorbidity burden. | Hemophilia was associated with higher odds of PJI (1.78 versus 0.98%). | PWH experienced more frequent postoperative complications than matched controls after TKA. |
| Chen et al. [35] | 2022 | 103 primary TKAs (75 PWH). Unilateral TKA was performed on 47 individuals and bilateral TKAs on the remaining 28 patients, including 12 simultaneous and 16 staged surgeries. The mean age was 32.3 years, and the mean follow-up was 77.9 months. | Failure was found in 8 individuals (8.5%) at mean 32.8 months after surgery. Four individuals suffered aseptic loosening, whereas infection in 4. The 10-year prosthesis survivorship was 88.6% | In terms of cost-effectiveness, bilateral simultaneous TKA was preferable to staged procedures. |
| Kim et al. [36] | 2022 | A total of 92 TKA (78 hemophilia A and 14 hemophilia B). Perioperative blood loss (PBL) was calculated. Patients were categorized into two groups: group H (higher blood loss than the mean PBL, n = 36) and group L (lower blood loss than the mean PBL, n = 56). | The mean PBL volume during TKA for hemophilic arthropathy of the knee was 542.3 mL. Lower hematocrit on the operation day and coagulation factor level were independent risk factors for increased PBL. | A FVIII level < 93.5% or hematocrit level of <38.2% are significant risk factors for increasing PBL. |
| Shen et al. [37] | 2022 | This study explored factors affecting hidden blood loss (92 TKAs in PWH). Mean age not available. | The hidden blood loss was 1069.51 mL, and the age was positively correlated with the hidden blood loss. However, tranexamic acid, FVIII prophylaxis, and incremental in vivo recovery were negatively correlated with hidden blood loss. | Intraoperative intra-articular injection of tranexamic acid diminished hidden blood loss. |
| Wang et al. [38] | 2022 | Twenty-eight patients (32 TKAs). Mean follow-up: 69.1 months. Mean age not available. | The rate of complications was 15.6%. | The rate of satisfaction was 100%. |
| Cambolat et al. [39] | 2022 | 73 TKAs (36 PWH and 37 patients without hemophilia). Mean age not available. | Postoperative tramadol consumption and pethidine consumption were substantially higher in PWH. | The length of stay in the hospital was also substantially longer in PWH. |
| Goker et al. [40] | 2022 | Forty-five TKAs in 29 PWH. This study assessed the effects of early major postoperative bleeding (MPOB) on the final functional result, complications, and implant survival of TKA. Mean age not available. | Ten patients (10 TKAs) experienced major bleeding during the postoperative period. Three of these patients had hemarthroses, one patient had a hematoma, one patient had hemorrhagic bullae formation, and five had excessive/prolonged bleeding from the wound. The bleeding group had significantly worse HSS, KSS, and KSS-F scores compared with controls. | In this study, MPOB after TKA in PWH was common and led to substantially worse function. MPOB after TKA in PWH was associated with a higher rate of complications and lower survival rates, although the differences were not statistically significant. Prosthetic survival was 17.04 years for the bleeding group and 22.15 years for the control group. Survival rates were 80% for the bleeding group and 96.4% for the control group. |
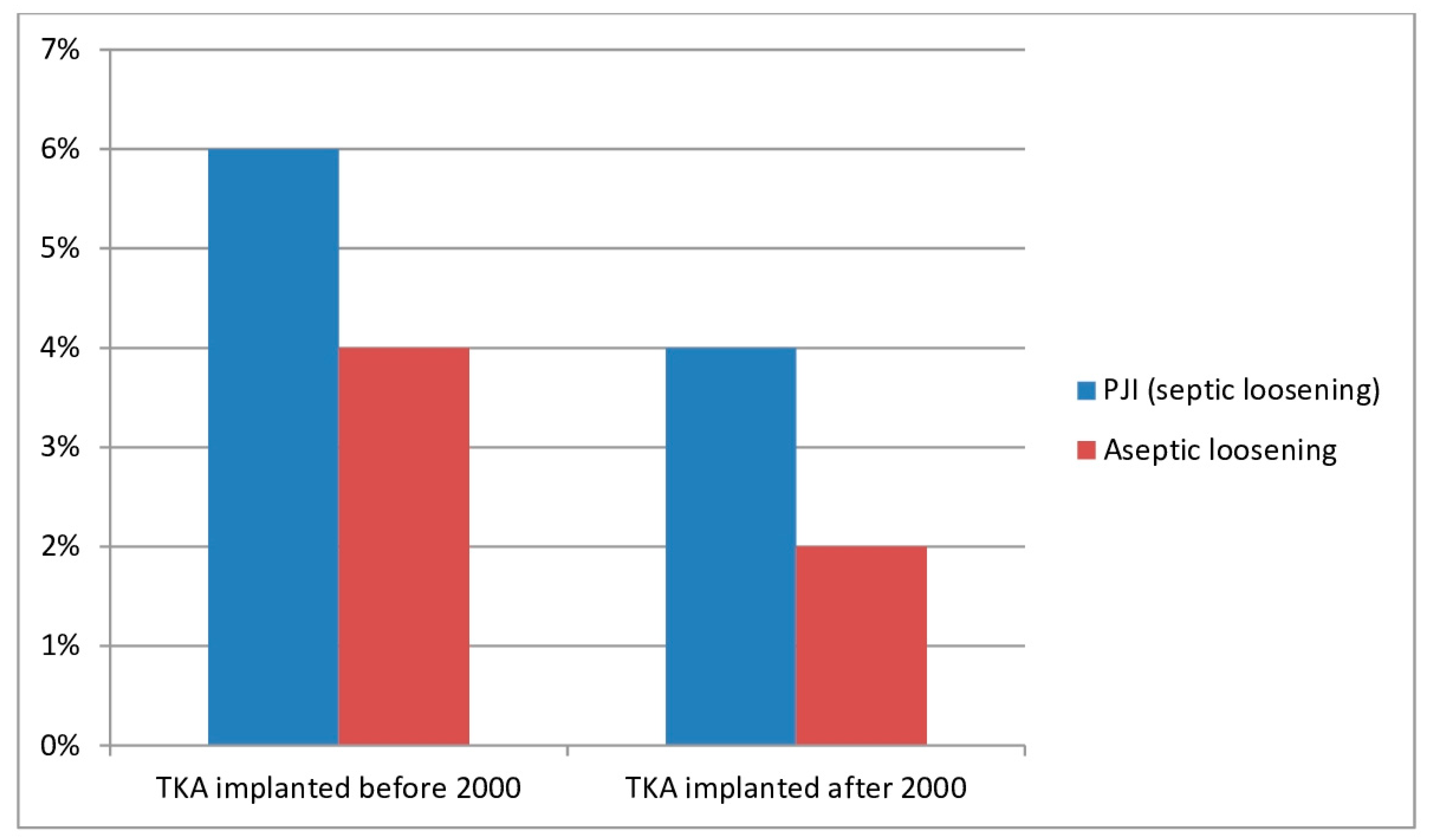
| Fenelon et al. [41] | 2022 | Systematic review and meta-analysis. A total of 1210 TKAs were carried out in 917 PWHs. The mean age of patients was 38.5 years with a mean length of follow-up of 7.1 years. | The complication rate was 28.7%, with 19.3% needing a further procedure. The HSS Knee Score improved by 44.6 points and KSS-F improved by 35.9 points. Total ROM improved by 22.3°. The most common complication was postoperative hemarthrosis (7.6%, 92 TKAs). PJI (6.2% versus 3.9%) and aseptic loosening (3.8% versus 2.1%) rates fell between period B (before the year 2000) and period A (after the year 2000). | TKA in PWHs is a successful procedure, improving function, alleviating pain, and improving ROM. PWHs underwent TKA at a younger age and had a higher risk of complications, though contemporary treatment diminished these risks. |
| Feng et al. [42] | 2023 | Twenty-six PWH with 36 TKAs were followed up for an average of 12.4 years. Mean age not available. | Mild and enduring anterior knee pain was reported in 7 knees (19%). Revision surgery was carried out in 7 knees, with 10- and 15-year prosthesis survival rates of 85.8% and 75.7%, respectively. | TKA alleviated pain, improved knee functions, reduced flexion contracture, and provided a high rate of satisfaction after more than 10 years of follow-up. |
| Ono et al. [43] | 2023 | This study proposed a threshold angle of extension contracture in treating hemophilic knee joints, retrospectively. Mean age 48 years. | Sixty-seven primary TKAs for PWH (mean age, 48 years) were performed, and incisional approaches to the joint included standard (58 cases) and V-Y quadricepsplasty (V-Y) (9 cases). The preoperative ROM and flexion were substantially associated with V-Y. | Primary TKA for PWH using a standard approach might be carried out before the stage preoperative flexion < 45° and ROM < 35°. |
| Carulli et al. [44] | 2023 | This study assessed the long-run results and survival rates of TKA in a series of consecutive PWH affected by severe knee arthropathy. Mean age not available. | These authors followed 65 PWH undergoing 91 TKAs, implanted using the same implant, characterized by an oxidized zirconium femoral component, coupled with a titanium tibial component and highly crosslinked polyethylene. | The study showed a high survival rate: 97.5% at a mean follow-up of 12.3 years. |
| Challoumas et al. [45] | 2024 | This study compared the results of TKA in PWH versus matched controls. Mean age not available. | PWH had a significantly higher incidence of PJI and 1-year revision/re-operation. | The odds of 1-year revision/re-operation after TKA in PWH were 1.4 times greater than the odds of 1-year revision/re-operation in people without hemophilia. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Merchan, E.C.; Mosconi, M.; De la Corte-Rodriguez, H.; Jannelli, E.; Pasta, G. Total Knee Arthroplasty in People with Hemophilia: Higher Incidence of Periprosthetic Joint Infection and 1-Year Revision/Re-Operation than the General Population and Lower Prosthetic Survival When Early Postoperative Bleeding Complications Occurred: Current Literature Review. J. Clin. Med. 2024, 13, 2447. https://doi.org/10.3390/jcm13082447
Rodriguez-Merchan EC, Mosconi M, De la Corte-Rodriguez H, Jannelli E, Pasta G. Total Knee Arthroplasty in People with Hemophilia: Higher Incidence of Periprosthetic Joint Infection and 1-Year Revision/Re-Operation than the General Population and Lower Prosthetic Survival When Early Postoperative Bleeding Complications Occurred: Current Literature Review. Journal of Clinical Medicine. 2024; 13(8):2447. https://doi.org/10.3390/jcm13082447
Chicago/Turabian StyleRodriguez-Merchan, Emerito Carlos, Mario Mosconi, Hortensia De la Corte-Rodriguez, Eugenio Jannelli, and Gianluigi Pasta. 2024. "Total Knee Arthroplasty in People with Hemophilia: Higher Incidence of Periprosthetic Joint Infection and 1-Year Revision/Re-Operation than the General Population and Lower Prosthetic Survival When Early Postoperative Bleeding Complications Occurred: Current Literature Review" Journal of Clinical Medicine 13, no. 8: 2447. https://doi.org/10.3390/jcm13082447
APA StyleRodriguez-Merchan, E. C., Mosconi, M., De la Corte-Rodriguez, H., Jannelli, E., & Pasta, G. (2024). Total Knee Arthroplasty in People with Hemophilia: Higher Incidence of Periprosthetic Joint Infection and 1-Year Revision/Re-Operation than the General Population and Lower Prosthetic Survival When Early Postoperative Bleeding Complications Occurred: Current Literature Review. Journal of Clinical Medicine, 13(8), 2447. https://doi.org/10.3390/jcm13082447