

Comparison of Fetal Crown-Rump Length Measurements between Thawed and Fresh Embryo Transfer

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McDonald, S.D.; Han, Z.; Mulla, S.; Murphy, K.E.; Beyene, J.; Ohlsson, A.; Knowledge Synthesis, G. Preterm birth and low birth weight among in vitro fertilization singletons: A systematic review and meta-analyses. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 146, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Shih, W.; Rushford, D.D.; Bourne, H.; Garrett, C.; McBain, J.C.; Healy, D.L.; Baker, H.W. Factors affecting low birthweight after assisted reproduction technology: Difference between transfer of fresh and cryopreserved embryos suggests an adverse effect of oocyte collection. Hum. Reprod. 2008, 23, 1644–1653. [Google Scholar] [CrossRef] [PubMed]
- Maheshwari, A.; Pandey, S.; Shetty, A.; Hamilton, M.; Bhattacharya, S. Obstetric and perinatal outcomes in singleton pregnancies resulting from the transfer of frozen thawed versus fresh embryos generated through in vitro fertilization treatment: A systematic review and meta-analysis. Fertil. Steril. 2012, 98, 368–377.e9. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, O.; Araki, R.; Kuwahara, A.; Itakura, A.; Saito, H.; Adamson, G.D. Impact of frozen-thawed single-blastocyst transfer on maternal and neonatal outcome: An analysis of 277,042 single-embryo transfer cycles from 2008 to 2010 in Japan. Fertil. Steril. 2014, 101, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, A.; Araki, R.; Tani, H.; Ishihara, O.; Kuwahara, A.; Irahara, M.; Yoshimura, Y.; Kuramoto, T.; Saito, H.; Nakaza, A.; et al. Implications of assisted reproductive technologies on term singleton birth weight: An analysis of 25,777 children in the national assisted reproduction registry of Japan. Fertil. Steril. 2013, 99, 450–455. [Google Scholar] [CrossRef]
- Syngelaki, A.; Chelemen, T.; Dagklis, T.; Allan, L.; Nicolaides, K.H. Challenges in the diagnosis of fetal non-chromosomal abnormalities at 11–13 weeks. Prenat. Diagn. 2011, 31, 90–102. [Google Scholar] [CrossRef]
- Santorum, M.; Wright, D.; Syngelaki, A.; Karagioti, N.; Nicolaides, K.H. Accuracy of first-trimester combined test in screening for trisomies 21, 18 and 13. Ultrasound Obstet. Gynecol. 2017, 49, 714–720. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T. Ethics, audit, and research: All shades of grey. BMJ 2005, 330, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Salomon, L.J.; Alfirevic, Z.; Bilardo, C.M.; Chalouhi, G.E.; Ghi, T.; Kagan, K.O.; Lau, T.K.; Papageorghiou, A.T.; Raine-Fenning, N.J.; Stirnemann, J.; et al. ISUOG practice guidelines: Performance of first-trimester fetal ultrasound scan. Ultrasound Obstet. Gynecol. 2013, 41, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Robinson, H.P.; Fleming, J.E. A critical evaluation of sonar “crown-rump length” measurements. Br. J. Obstet. Gynaecol. 1975, 82, 702–710. [Google Scholar] [CrossRef] [PubMed]
- Papageorghiou, A.T.; Kennedy, S.H.; Salomon, L.J.; Ohuma, E.O.; Cheikh Ismail, L.; Barros, F.C.; Lambert, A.; Carvalho, M.; Jaffer, Y.A.; Bertino, E.; et al. International standards for early fetal size and pregnancy dating based on ultrasound measurement of crown-rump length in the first trimester of pregnancy. Ultrasound Obstet. Gynecol. 2014, 44, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Zaat, T.; Zagers, M.; Mol, F.; Goddijn, M.; van Wely, M.; Mastenbroek, S. Fresh versus frozen embryo transfers in assisted reproduction. Cochrane Database Syst. Rev. 2021, 2, CD011184. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Reschke, L.; Segars, J.; Baker, V.L. Frozen-thawed embryo transfer: The potential importance of the corpus luteum in preventing obstetrical complications. Fertil. Steril. 2020, 113, 252–257. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharya, S. Maternal and perinatal outcomes after fresh versus frozen embryo transfer-what is the risk-benefit ratio? Fertil. Steril. 2016, 106, 241–243. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Du, M.; Li, Z.; Wang, L.; Hu, J.; Zhao, B.; Feng, Y.; Chen, X.; Sun, L. Fresh versus frozen embryo transfer for full-term singleton birth: A retrospective cohort study. J. Ovarian Res. 2018, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Spijkers, S.; Lens, J.W.; Schats, R.; Lambalk, C.B. Fresh and Frozen-Thawed Embryo Transfer Compared to Natural Conception: Differences in Perinatal Outcome. Gynecol. Obstet. Investig. 2017, 82, 538–546. [Google Scholar] [CrossRef] [PubMed]
- De Geyter, C.; Calhaz-Jorge, C.; Kupka, M.S.; Wyns, C.; Mocanu, E.; Motrenko, T.; Scaravelli, G.; Smeenk, J.; Vidakovic, S.; Goossens, V.; et al. ART in Europe, 2014: Results generated from European registries by ESHRE: The European IVF-monitoring Consortium (EIM) for the European Society of Human Reproduction and Embryology (ESHRE). Hum. Reprod. 2018, 33, 1586–1601. [Google Scholar] [CrossRef] [PubMed]
- Kawwass, J.F.; Monsour, M.; Crawford, S.; Kissin, D.M.; Session, D.R.; Kulkarni, A.D.; Jamieson, D.J.; National ART Surveillance System (NASS) Group. Trends and outcomes for donor oocyte cycles in the United States, 2000–2010. JAMA 2013, 310, 2426–2434. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.M.; van Wely, M.; Mol, F.; Repping, S.; Mastenbroek, S. Fresh versus frozen embryo transfers in assisted reproduction. Cochrane Database Syst. Rev. 2017, 3, CD011184. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, B.S.; Daneshmand, S.T.; Restrepo, H.; Garner, F.C.; Aguirre, M.; Hudson, C. Matched-cohort comparison of single-embryo transfers in fresh and frozen-thawed embryo transfer cycles. Fertil. Steril. 2013, 99, 389–392. [Google Scholar] [CrossRef]
- Laval, M.; Garlantezec, R.; Guivarc’h-Leveque, A. Birthweight difference of singletons conceived through in vitro fertilization with frozen versus fresh embryo transfer: An analysis of 5406 embryo transfers in a retrospective study 2013–2018. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101644. [Google Scholar] [CrossRef] [PubMed]
- Cavoretto, P.I.; Farina, A.; Girardelli, S.; Gaeta, G.; Spinillo, S.; Morano, D.; Amodeo, S.; Galdini, A.; Vigano, P.; Candiani, M. Greater fetal crown-rump length growth with the use of in vitro fertilization or intracytoplasmic sperm injection conceptions after thawed versus fresh blastocyst transfers: Secondary analysis of a prospective cohort study. Fertil. Steril. 2021, 116, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Pinborg, A.; Henningsen, A.A.; Loft, A.; Malchau, S.S.; Forman, J.; Andersen, A.N. Large baby syndrome in singletons born after frozen embryo transfer (FET): Is it due to maternal factors or the cryotechnique? Hum. Reprod. 2014, 29, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Ishii, R.; Shoda, A.; Kubo, M.; Okazaki, S.; Suzuki, M.; Okawa, R.; Enomoto, M.; Shitanaka, M.; Fujita, Y.; Nakao, K.; et al. Identifying a possible factor for the increased newborn size in singleton pregnancies after assisted reproductive technology using cryopreserved embryos, in comparison with fresh embryos. Reprod. Med. Biol. 2018, 17, 307–314. [Google Scholar] [CrossRef]
- Senapati, S.; Wang, F.; Ord, T.; Coutifaris, C.; Feng, R.; Mainigi, M. Superovulation alters the expression of endometrial genes critical to tissue remodeling and placentation. J. Assist. Reprod. Genet. 2018, 35, 1799–1808. [Google Scholar] [CrossRef] [PubMed]
- Conrad, K.P.; Baker, V.L. Corpus luteal contribution to maternal pregnancy physiology and outcomes in assisted reproductive technologies. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2013, 304, R69–R72. [Google Scholar] [CrossRef] [PubMed]
- Conrad, K.P.; Petersen, J.W.; Chi, Y.Y.; Zhai, X.; Li, M.; Chiu, K.H.; Liu, J.; Lingis, M.D.; Williams, R.S.; Rhoton-Vlasak, A.; et al. Maternal Cardiovascular Dysregulation During Early Pregnancy After In Vitro Fertilization Cycles in the Absence of a Corpus Luteum. Hypertension 2019, 74, 705–715. [Google Scholar] [CrossRef]
- Weinerman, R. Growth differences after fresh and frozen embryo transfers: When do they begin? Fertil. Steril. 2021, 116, 75–76. [Google Scholar] [CrossRef]
- Bilagi, A.; Burke, D.L.; Riley, R.D.; Mills, I.; Kilby, M.D.; Katie Morris, R. Association of maternal serum PAPP-A levels, nuchal translucency and crown-rump length in first trimester with adverse pregnancy outcomes: Retrospective cohort study. Prenat. Diagn. 2017, 37, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Ubaldi, F.M.; Cimadomo, D.; Vaiarelli, A.; Fabozzi, G.; Venturella, R.; Maggiulli, R.; Mazzilli, R.; Ferrero, S.; Palagiano, A.; Rienzi, L. Advanced Maternal Age in IVF: Still a Challenge? The Present and the Future of Its Treatment. Front. Endocrinol. 2019, 10, 94. [Google Scholar] [CrossRef]
- Leon, G.; Papetta, A.; Spiliopoulou, C. Overview of the Greek legislation regarding assisted reproduction and comparison with the EU legal framework. Reprod. Biomed. Online 2011, 23, 820–823. [Google Scholar] [CrossRef]
- van Loendersloot, L.L.; Moolenaar, L.M.; van Wely, M.; Repping, S.; Bossuyt, P.M.; Hompes, P.G.A.; van der Veen, F.; Mol, B.W.J. Cost-effectiveness of single versus double embryo transfer in IVF in relation to female age. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 214, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Medical Advisory, S. In vitro fertilization and multiple pregnancies: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2006, 6, 1–63. [Google Scholar]
- Veleva, Z.; Vilska, S.; Hyden-Granskog, C.; Tiitinen, A.; Tapanainen, J.S.; Martikainen, H. Elective single embryo transfer in women aged 36-39 years. Hum. Reprod. 2006, 21, 2098–2102. [Google Scholar] [CrossRef] [PubMed]
- Simopoulou, M.; Sfakianoudis, K.; Maziotis, E.; Tsioulou, P.; Grigoriadis, S.; Rapani, A.; Giannelou, P.; Asimakopoulou, M.; Kokkali, G.; Pantou, A.; et al. PGT-A: Who and when? Alpha systematic review and network meta-analysis of RCTs. J. Assist. Reprod. Genet. 2021, 38, 1939–1957. [Google Scholar] [CrossRef] [PubMed]
- Iuculano, A.; Stagnati, V.; Serrenti, M.; Peddes, C.; Monni, G.; Sole, G.; Cucca, F. Crown-rump length: Are they different or similar after homologous vs heterologous oocyte/embryo donation? Am. J. Obstet. Gynecol. 2017, 217, 224–225. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| (a) | |||||
| Characteristics | Thawed Cycles | Fresh Cycles | p-Value | ||
| Number of embryos | 1618 (40%) | 2426 (60%) | N/A | ||
| Maternal age (mean/SD) | 39.8 (5.7) | 35.8 (4.3) | <0.001 | ||
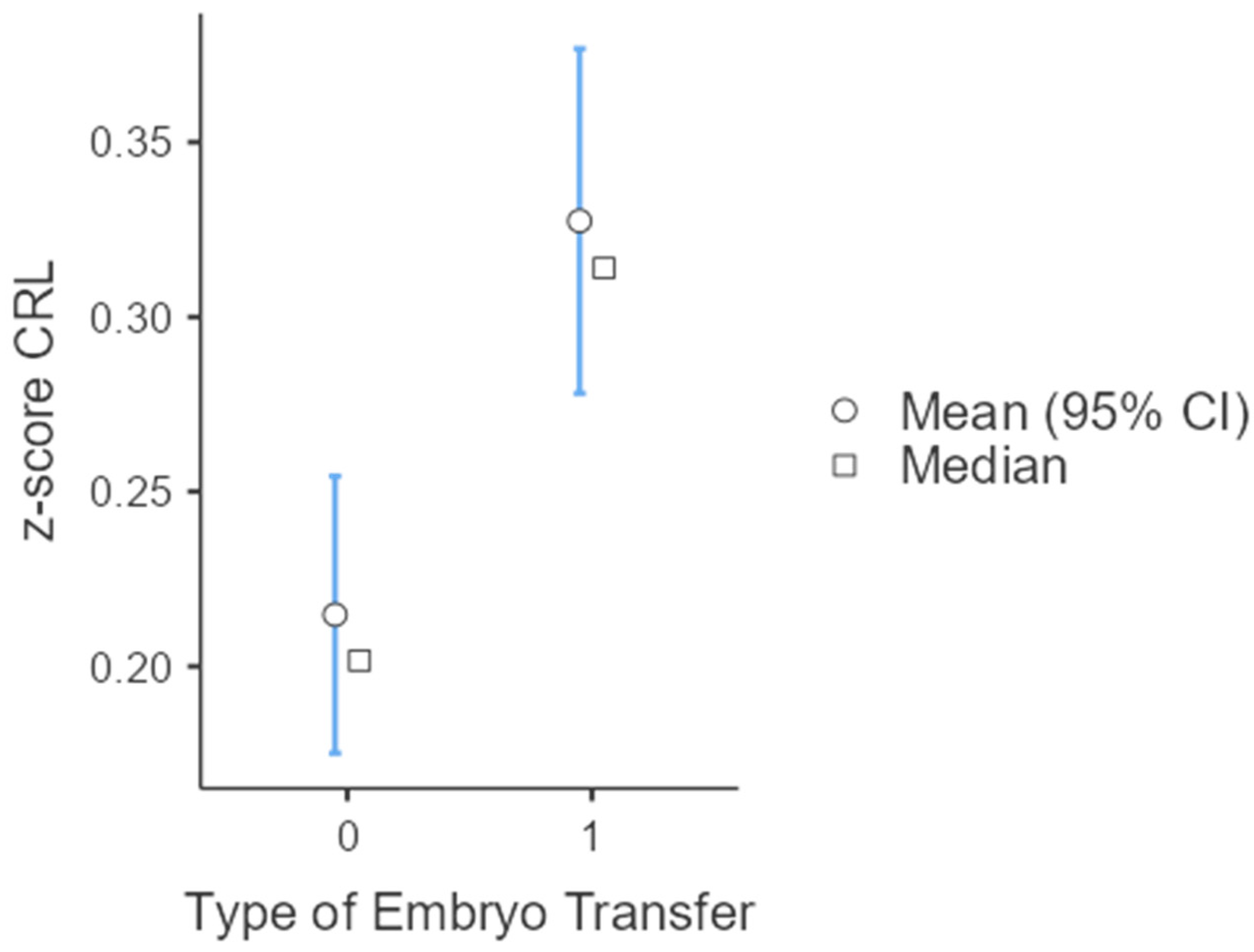
| CRL z-score (mean/SD) | 0.309 (0.806) | 0.199 (0.805) | <0.001 | ||
| (b) | |||||
| Characteristics | Thawed Cycles | Fresh Cycles | p-Value | OR | 95% CI |
| Number of singleton gestations | 892 (71%) | 1228 (67.2%) | |||
| Number of twin gestations | 363 (29%) | 599 (32.8%) | 0.005 | 1.20 | 1.06–1.36 |
| Characteristics | Thawed Cycles | Fresh Cycles | p-Value |
| Maternal age (mean/SD) | 40.1 (6.1) | 35.1 (4.3) | <0.001 |
| CRL z-score (mean/SD) | 0.285 (0.869) | 0.184 (0.893) | 0.015 |
| Characteristics | Own Oocytes | Donor Oocytes | p-Value |
| Maternal age (mean/SD) | 37.5 (5.1) | 43.5 (4.7) | <0.001 |
| CRL z-score (mean/SD) | 0.191 (1.05) | 0.431 (0.813) | 0.002 |
| Characteristics | Thawed Cycles | Fresh Cycles | p-Value |
| Maternal age (mean/SD) | 39.6 (5.3) | 36.4 (4.3) | <0.001 |
| CRL z-score (mean/SD) | 0.327 (0.751) | 0.215 (0.709) | <0.001 |
| Characteristics | Own Oocytes | Donor Oocytes | p-Value |
| Maternal age (mean/SD) | 37.6 (4.5) | 43.7 (4.1) | <0.001 |
| CRL z-score (mean/SD) | 0.455 (1.17) | 0.314 (0.919) | 0.412 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitta, K.; Tsakiridis, I.; Giougi, E.; Mamopoulos, A.; Kalogiannidis, I.; Dagklis, T.; Athanasiadis, A. Comparison of Fetal Crown-Rump Length Measurements between Thawed and Fresh Embryo Transfer. J. Clin. Med. 2024, 13, 2575. https://doi.org/10.3390/jcm13092575
Mitta K, Tsakiridis I, Giougi E, Mamopoulos A, Kalogiannidis I, Dagklis T, Athanasiadis A. Comparison of Fetal Crown-Rump Length Measurements between Thawed and Fresh Embryo Transfer. Journal of Clinical Medicine. 2024; 13(9):2575. https://doi.org/10.3390/jcm13092575
Chicago/Turabian StyleMitta, Kyriaki, Ioannis Tsakiridis, Evaggelia Giougi, Apostolos Mamopoulos, Ioannis Kalogiannidis, Themistoklis Dagklis, and Apostolos Athanasiadis. 2024. "Comparison of Fetal Crown-Rump Length Measurements between Thawed and Fresh Embryo Transfer" Journal of Clinical Medicine 13, no. 9: 2575. https://doi.org/10.3390/jcm13092575
APA StyleMitta, K., Tsakiridis, I., Giougi, E., Mamopoulos, A., Kalogiannidis, I., Dagklis, T., & Athanasiadis, A. (2024). Comparison of Fetal Crown-Rump Length Measurements between Thawed and Fresh Embryo Transfer. Journal of Clinical Medicine, 13(9), 2575. https://doi.org/10.3390/jcm13092575