
The Benefit of Conserving and Gaining Resources after Trauma: A Systematic Review

Abstract
:1. Introduction
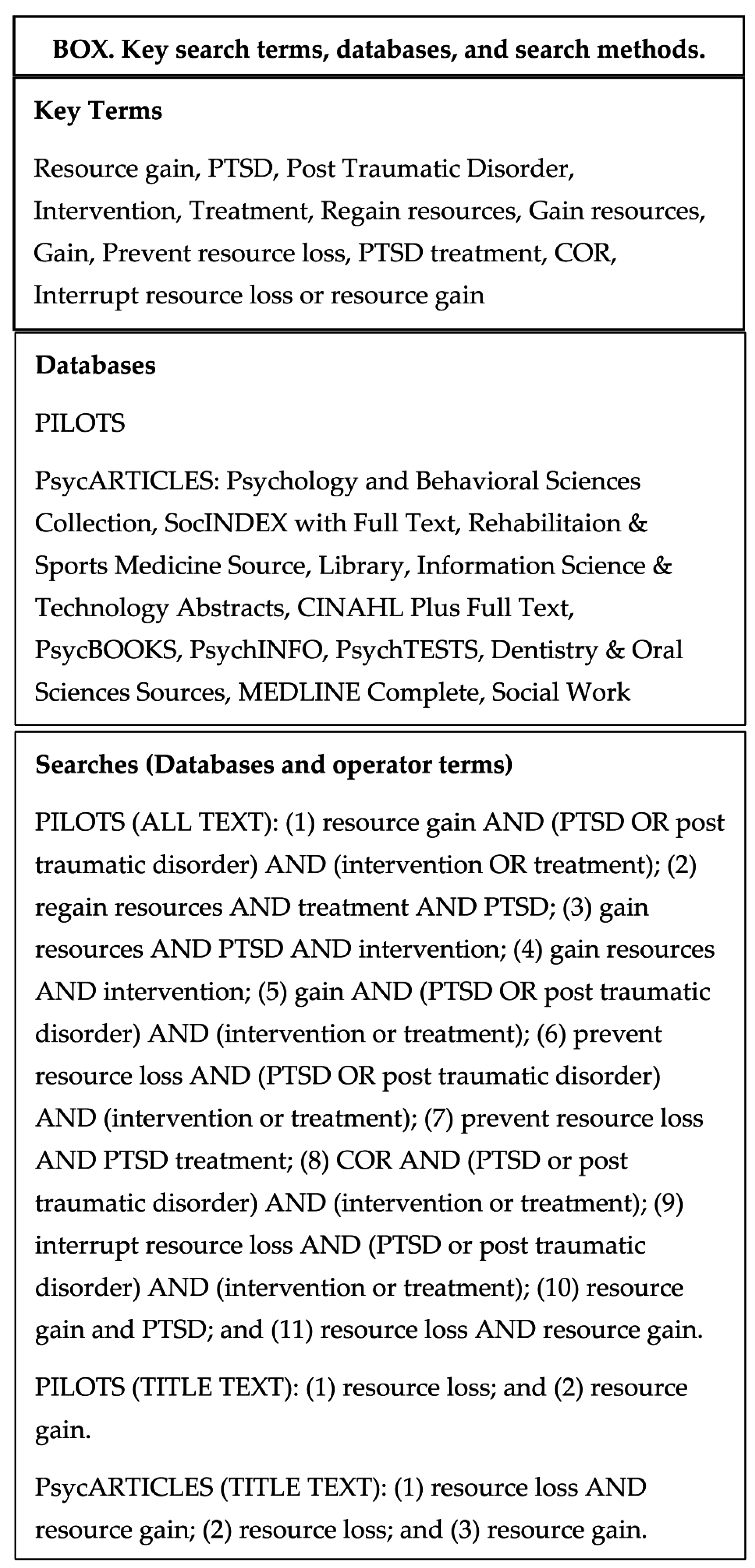
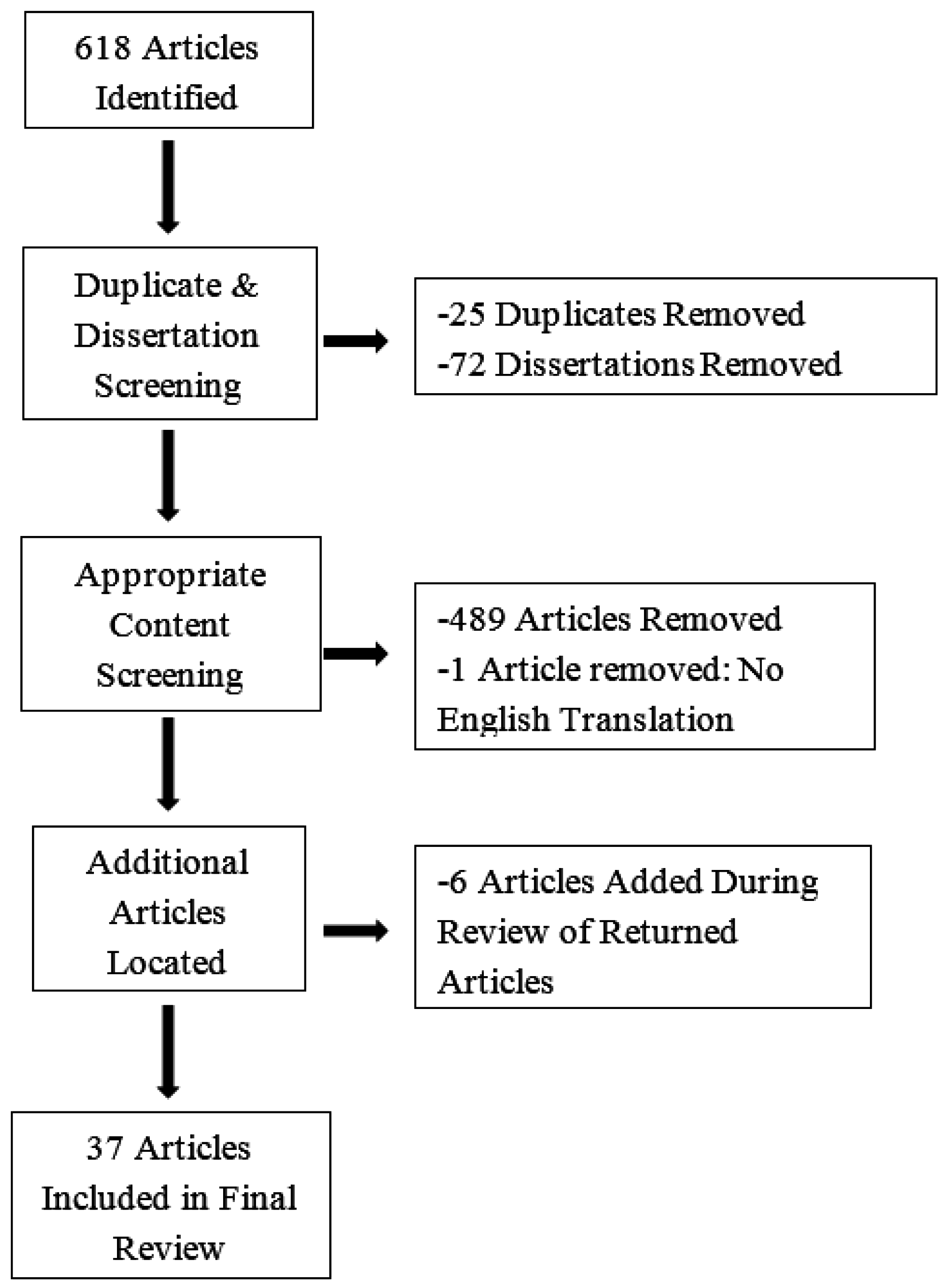
2. Methods
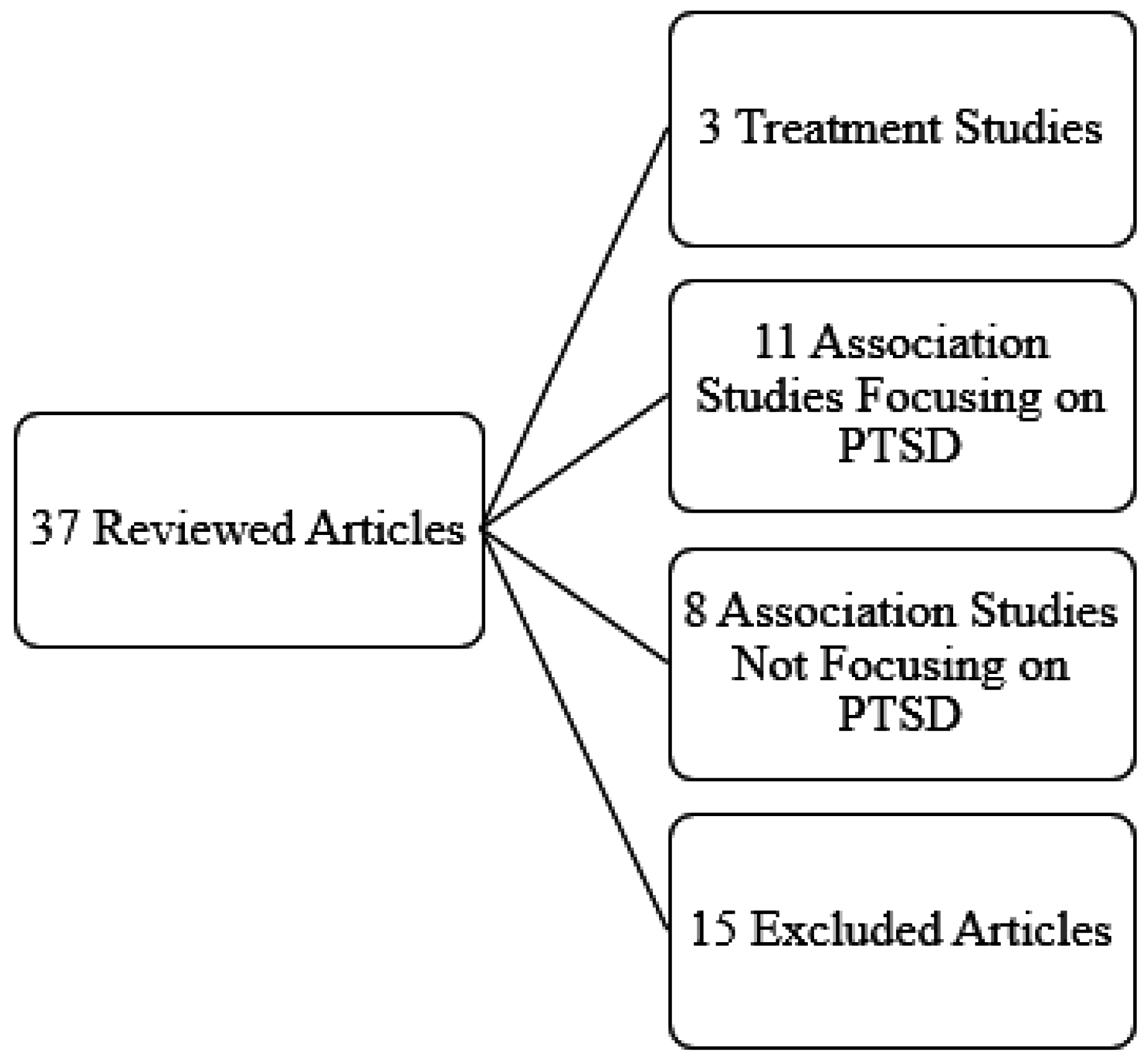
3. Results
3.1. Treatment Studies
3.2. Association Studies PTSD Focus
3.3. Association Studies No PTSD Focus
4. Discussion
Author Contributions
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Instrument | Construct Assessed | * Validated or Self-Made | |
|---|---|---|---|
| 1. | Objective and Subjective Index of Threat Questionnaire | Objective and Subject Threat | Self-Made |
| 2. | Changes in Life Domain Questionnaire | Subjective Evaluation of Changes In Life Domains and Coping Resources | Self-Made |
| 3. | The Posttraumatic Stress Reaction Index | Severity of Posttraumatic Symptoms | Validated |
| 4. | Coping Resources Questionnaire | Coping Resources | Self-Made |
| 5. | Conservation of Resources—Evaluation (COR-E) | Resources | Validated |
| 6. | Diagnostic and Statistical Manual of Mental Disorders (DSM) IV Criterion A for PTSD | Traumatic Events | Validated |
| 7. | Hopkins Symptom Checklist-25 (HSCL-25) | Anxiety and Depression | Validated |
| 8. | Demographic Questionnaire | Demographic Variables | Self-Made |
| 9. | Exposure to Terrorist or War-Related Event Questionnaire | Terrorist Attacks or War Related Events Since Beginning of Al Aqsa Intifada | Self-Made |
| 10. | Economic Resources Questionnaire | Loss of Economic Resources | Self-Made |
| 11. | COR Theory Questionnaire | Resources | Self-Made |
| 12. | Social Support Questionnaire | Support Satisfaction | Validated |
| 13. | Ethnocentrism, Political Violence, and Authoritarianism Questionnaire | Protective Attitudes | Self-Made |
| 14. | Public Health Questionnaire | Depressive Symptoms | Validated |
| 15. | Abbreviated Version of PTSD Symptom Scale | PTSD | Self-Made |
| 16. | PTSD Inventory | PTSD | Validated |
| 17. | PTSD Symptom Scale-Interview Format (PSS-I) | PTSD | Validated |
| 18. | Patient Health Questionnaire (PHQ-9) | Depressive Symptoms | Validated |
| 19. | Resource Loss Scale for Children (RLSC) | Resource Loss | Validated |
| 20. | Self-Esteem Inventory | Self-Esteem | Validated |
| 21. | Life Orientation Test | Optimism | Validated |
| 22. | General Health Questionnaire-12 | General Psychological Distress | Validated |
| 23. | Impact of Events Scale—Revised (IES-R) | Posttraumatic Stress | Validated |
| 24. | Multidimensional Scale of Perceived Social Support (MSPSS) | Social Support | Validated |
| 25. | PTSD Symptoms Scale—Self Report (PSS-SR) | PTSD | Validated |
| 26. | Center for Epidemiologic Studies Depression Scale (CES-D) | Depression | Validated |
| 27. | Four Dimension Anxiety Scale (FDAS) | Anxiety | Validated |
| 28. | September 11th Event Experiences Questionnaire | 9/11 Experiences | Self-Made |
| 29. | Lifetime Trauma Event Exposures Questionnaire | Lifetime Trauma Event Exposures | Self-Made |
| 30. | Social Support Questionnaire | Social Support | Self-Made |
| 31. | DSM IV Criteria for Panic Attacks | Panic Attack Symptoms | Validated |
| 32. | National Women’s Study (NWS) PTSD Module | PTSD | Validated |
| 33. | Major Depressive Scale from Structured Clinical Interview for DSM III—Revised | Depression | Validated |
| 34. | Brief Symptom Inventory (BSI) | Psychiatric Symptoms | Validated |
| 35. | Social Constraints Scale (SCS) | Social Constraints | Validated |
| 36. | PTSD Stressor Criteria DSM-IV | Stressfulness of Events | Validated |
| 37. | Acceptance and Action Questionnaire (AAQ) | Acceptance and Action | Validated |
| 38. | Post-Traumatic Stress Disorder Checklist—Civilian (PCL-C) | PTSD | Validated |
| 39. | Life Trauma History | Traumatic Life Events Questionnaire (TLEQ) | Validated |
| 40. | Depression Anxiety Stress Scale 21 (DASS-21) | Psychological Distress | Validated |
| 41. | Exposure to Shooting Incident Questionnaire | Exposure To Shooting | Self-Made |
| 42. | Distressing Events Questionnaires (DEQ) | PTSD | Validated |
| 43. | Coping Strategies Inventory (CSI) | Coping Strategies | Validated |
| 44. | State Trait Anger Scale (STAS) | Anger | Validated |
| 45. | Mastery Scale | Mastery | Validated |
| 46. | Profile of Mood States (POMS) | Depressive Mood | Validated |
| 47. | State-Trait Expression Inventory (STAXI) | Anger | Validated |
| 48. | Family Environment Services (FES) | Family Support | Validated |
| 49. | Personality Characteristics Questionnaire | Personality Characteristics | Self-Made |
| 50. | Serious Negative Life Events Questionnaire | Life-Change Events | Validated |
| 51. | Research Diagnostic Criteria—Depressive Symptoms Index | Depressive Symptoms | Validated |
| 52. | Duke Religious Index (DRI) | General Religiousness | Validated |
| 53. | Religious Comfort and Strain Scale (RCSS) | General Religiousness | Validated |
| 54. | RAND Health Survey | Health and Adjustment | Validated |
| 55. | Posttraumatic Growth Inventory | Posttraumatic Growth | Validated |
| 56. | Resistance Deficit Variables | Generalized Resistance Resources | Self-Made |
| 57. | Sense of Coherence Scale | Sense of Coherence | Validated |
| 58. | Florida Health and Family Life Instrument | Psychological Dysfunction | Validated |
| 59. | K6 Scale | Psychological Distress | Validated |
| 60. | Social Provisions Scale | Social Support | Validated |
| 61. | Outlook and Sense of Identity Questionnaire | Goal Orientation | Self-Made |
| 62. | Reactive Responding—Short Form | Goal Orientation | Validated |
| 63. | Health and Hurricane Questionnaire | Health and Hurricane Exposure | Self-Made |
| 64. | Flood Exposure Questionnaire | Flood Exposure | Validated |
| 65. | Physical Symptoms Index | Physical Symptoms | Validated |
| 66. | Social Integration Questionnaire | Social Integration | Self-Made |
| 67. | Frequency of Social Interaction Questionnaire | Frequency of Social Interactions | Self-Made |
References
- Hobfoll, S.E.; Spielberger, C.D.; Breznitz, S.; Figley, C.; Folkman, S.; Lepper-Green, B.; Meichenbaum, D.; Milgram, N.A.; Sandler, I.; Sarason, I.; et al. War-related stress. Addressing the stress of war and other traumatic events. Am. Psychol. 1991, 46, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.J.; Hobfoll, S.E.; Palmieri, P.A.; Canetti-Nisim, D.; Shapira, O.; Johnson, R.J.; Galea, S. The psychological impact of impending forced settler disengagement in gaza: Trauma and posttraumatic growth. J. Trauma. Stress 2008, 21, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Palmieri, P.A.; Johnson, R.J.; Canetti-Nisim, D.; Hall, B.J.; Galea, S. Trajectories of resilience, resistance, and distress during ongoing terrorism: The case of jews and arabs in israel. J. Consult. Clin. Psychol. 2009, 77, 138–148. [Google Scholar] [CrossRef] [PubMed]
- Lindhorst, T.; Oxford, M.; Gillmore, M.R. Longitudinal effects of domestic violence on employment and welfare outcomes. J. Interpers. Violence 2007, 22, 812–828. [Google Scholar] [CrossRef] [PubMed]
- Monnier, J.; Resnick, H.S.; Kilpatrick, D.G.; Seals, B. The relationship between distress and resource loss following rape. Violence Vict. 2002, 17, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Norris, F.H.; Friedman, M.J.; Watson, P.J. 60,000 disaster victims speak: Part ii. Summary and implications of the disaster mental health research. Psychiatry 2002, 65, 240–260. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, P.A.; Canetti-Nisim, D.; Galea, S.; Johnson, R.J.; Hobfoll, S.E. The psychological impact of the Israel-Hezbollah war on Jews and Arabs in Israel: The impact of risk and resilience factors. Soc. Sci. Med. 2008, 67, 1208–1216. [Google Scholar] [CrossRef] [PubMed]
- Silver, R.C.; Holman, E.A.; McIntosh, D.N.; Poulin, M.; Gil-Rivas, V. Nationwide longitudinal study of psychological responses to September 11. JAMA 2002, 288, 1235–1244. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Freedy, J.R. Psychosocial resource loss as a mediator of the effects of flood exposure on psychological distress and physical symptoms. J. Trauma. Stress 2000, 13, 349–357. [Google Scholar] [CrossRef] [PubMed]
- VA/DoD. Treatment Guidelines for Posttraumatic Stress Disorder; VA/DoD: Alexandria, VA, USA, 2011. [Google Scholar]
- Hobfoll, S.E. Conservation of resources. A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 13–24. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Stress, Culture, and Community: The Psychology and Physiology of Stress; Plenum Press: New York, NY, USA, 1998. [Google Scholar]
- Adeola, F.O. Mental health and psychosocial distress sequelae of katrina: An empirical study of survivors. Hum. Ecol. Rev. 2009, 16, 195–210. [Google Scholar]
- Paul, L.A.; Price, M.; Gros, D.F.; Gros, K.S.; McCauley, J.L.; Resnick, H.S.; Acierno, R.; Ruggiero, K.J. The associations between loss and posttraumatic stress and depressive symptoms following hurricane IKE. J. Clin. Psychol. 2014, 70, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Lilly, R.S. Resource conservation as a strategy for community psychology. J. Community Psychol. 1993, 21, 128–148. [Google Scholar] [CrossRef]
- Benotsch, E.G.; Brailey, K.; Vasterling, J.J.; Uddo, M.; Constans, J.I.; Sutker, P.B. War zone stress, personal and environmental resources, and PTSD symptoms in gulf war veterans: A longitudinal perspective. J. Abnorm. Psychol. 2000, 109, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Thrasher, S.; Power, M.; Morant, N.; Marks, I.; Dalgleish, T. Social support moderates outcome in a randomized controlled trial of exposure therapy and (or) cognitive restructuring for chronic posttraumatic stress disorder. Can. J. Psychiatry 2010, 55, 187–190. [Google Scholar] [PubMed]
- Johnson, D.M.; Zlotnick, C. A cognitive-behavioral treatment for battered women with PTSD in shelters: Findings from a pilot study. J. Trauma. Stress 2006, 19, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Walter, K.H.; Hobfoll, S.E. Resource loss and naturalistic reduction of PTSD among inner-city women. J. Interpers. Violence 2009, 24, 482–498. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.C.; Hung, F.C.; Chen, S.H. “Changes or not” is the question: The meaning of posttraumatic stress reactions one year after the taiwan chi-chi earthquake. J. Chin. Inst. Eng. 2002, 25, 609–618. [Google Scholar] [CrossRef]
- Slobodin, O.; Caspi, Y.; Klein, E.; Berger, B.D.; Hobfoll, S.E. Resource loss and posttraumatic responses in bedouin members of the israeli defense forces. J. Trauma. Stress 2011, 24, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Hall, B.J.; Bonanno, G.A.; Bolton, P.A.; Bass, J.K. A longitudinal investigation of changes to social resources associated with psychological distress among Kurdish torture survivors living in northern Iraq. J. Trauma. Stress 2014, 27, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Zwiebach, L.; Rhodes, J.; Roemer, L. Resource loss, resource gain, and mental health among survivors of Hurricane Katrina. J. Trauma. Stress 2010, 23, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E.; Canetti-Nisim, D.; Johnson, R. Exposure to terrorism, stress-related mental health symptoms and defensive coping among Jews and Arabs in Israel. J. Consult. Clin. Psychol. 2006, 74, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Heath, N.M.; Hall, B.J.; Russ, E.U.; Hobfoll, S.E. Reciprocal relationships between resource loss and psychological distress following exposure to political violence: An empirical investigation of COR theory’s loss spirals. Anxiety Stress Coping 2012, 25, 679–695. [Google Scholar] [CrossRef] [PubMed]
- Blaze, J.T.; Shwalk, D.W. Resource loss and relocation: A follow-up study of adolescents two years after Hurricane Katrina. Psychol. Trauma 2009, 1, 312–322. [Google Scholar] [CrossRef]
- Littleton, H.; Grills-Taquechel, A.E.; Axsom, D. Resource loss as a predictor of posttrauma symptoms among college women following the mass shooting at Virginia Tech. Violence Vict. 2009, 5, 669–686. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Tracey, T.; Galea, S. The impact of resource loss and traumatic growth on probable PTSD and depression following terrorist attacks. J. Trauma. Stress 2006, 19, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Dekel, R.; Hobfoll, S.E. The impact of resource loss on Holocaust survivors facing war and terrorism in Israel. Aging Ment. Health 2007, 11, 159–167. [Google Scholar] [CrossRef] [PubMed]
- Cordova, M.J.; Walser, R.; Neff, J.; Ruzek, J.I. Predictors of emotional adjustment following traumatic injury: Personal, social and material resources. Prehosp. Disaster Med. 2005, 20, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Littleton, H.L.; Kumpula, M.; Orcutt, H. Posttraumatic symptoms following a campus shooting: The role of psychosocial resource loss. Violence Vict. 2011, 26, 461–476. [Google Scholar] [CrossRef] [PubMed]
- Littleton, H.L.; Axsom, D.; Grills-Taquechel, A.E. Adjustment following the mass shooting at Virginia Tech: The roles of resource loss and gain. Psychol. Trauma 2009, 1, 206–219. [Google Scholar] [CrossRef]
- Wells, J.D.; Hobfoll, S.E.; Lavin, J. Resource loss, resource gain, and communal coping during pregnancy women with multiple roles. Psychol. Women Q. 1997, 21, 645–662. [Google Scholar] [CrossRef]
- Hobfoll, S.E.; Johnson, R.J.; Ennis, N.; Jackson, A.P. Resource loss, resource gain and emotional outcomes among inner city women. J. Pers. Soc. Psychol. 2003, 84, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Holahan, C.J.; Moos, R.H.; Holahan, C.K.; Cronkite, R.C. Resource loss, resource gain, and depressive symptoms: A 10-year model. J. Pers. Soc. Psychol. 1999, 77, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.W.; Aten, J.D.; Moore, M.; Hook, J.; Davis, D.E. Resource loss, religiousness, health and posttraumatic growth following Hurricane Katrina. Ment. Heath Relig. Cult. 2013, 16, 352–366. [Google Scholar] [CrossRef]
- Ying, Y.; Akutsu, P.D.; Zhang, X.; Huang, L.N. Psychological dysfunction in Southeast Asian refugees as mediated by sense of coherence. Community Psychol. 1997, 25, 839–859. [Google Scholar] [CrossRef]
- Bisson, J.; Andrew, M. Psychological treatment of post-traumatic stress disorder (PTSD). Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef]
- Hollifield, M. Acupuncture for posttraumatic stress disorder: Conceptual, clinical, and biological data support further research. CNS Neurosci. Ther. 2011, 17, 769–779. [Google Scholar] [CrossRef] [PubMed]
- Kar, N. Cognitive behavioral therapy for the treatment of post-traumatic stress disorder: A review. Neuropsychiatr. Disease Treat. 2011, 7, 167–181. [Google Scholar] [CrossRef] [PubMed]
- Frueh, B.C.; Turner, S.M.; Beidel, D.C. Exposure therapy for combat-related PTSD: A critical review. Clin. Psychol. Rev. 1995, 15, 799–817. [Google Scholar] [CrossRef]
- Turner, S.M.; Beidel, D.C.; Frueh, B.C. Multicomponent behavioral treatment for chronic combat-related posttraumatic stress disorder: Trauma management therapy. Behav. Modif. 2005, 29, 39–69. [Google Scholar] [CrossRef] [PubMed]
- Hollifield, M.; Sinclair-Lian, N.; Warner, T.D.; Hammerschlag, R. Acupuncture for posttraumatic stress disorder: A randomized controlled pilot trial. J. Nerv. Ment. Disease 2007, 195, 504–513. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Rush, A.J.; Shaw, B.F. Cognitive Therapy of Depresson; Guilford: New York, NY, USA, 1979. [Google Scholar]
- Krakow, B.; Hollifield, M.; Johnston, L.; Koss, M.; Schrader, R.; Warner, T.D.; Tandberg, D.; Lauriello, J.; McBride, L.; Cutchen, L.; et al. Imagery rehearsal therapy for chronic nightmares in sexual assault survivors with posttraumatic stress disorder. A randomized controlled trial. JAMA 2001, 286, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Wolpe, J. Psychotherapy by Reciprocal Inhibition; Stanford University Press: Stanford, CA, USA, 1958. [Google Scholar]
- Salter, A. Conditioned Reflex Therapy; Creative Age: New York, NY, USA, 1949. [Google Scholar]
- Hobfoll, S.E.; Watson, P.; Bell, C.C.; Bryant, R.A.; Brymer, M.J.; Friedman, M.J.; Friedman, M.; Gersons, B.P.; de Jong, J.T.; Layne, C.M.; et al. Five essential elements of immediate and mid-term mass trauma intervention: Empirical evidence. Psychiatry 2007, 70, 283–315. [Google Scholar] [CrossRef] [PubMed]



| Authors and Year | Research Question | Sample size, Population, and Trauma Experience | Resources Measured | Other Measured Clinical Symptoms | Experienced Resource Gain | Positive Associations with Resource Gain | Associations with Resource Loss |
|---|---|---|---|---|---|---|---|
| Wu, Hung, Chen, 2002 [20] | Is there a positive relationship between changes of health conditions/social relationships and the state of possessed resources? | 556 adults Taiwan Chi-Chi Earthquake | Objective and Subjective Threat 1 Subjective Evaluation of changes in life domains and coping resources 2 Coping Resources 4 | Severity of Posttraumatic Symptoms 3 | Socio-economic Domain Social-interpersonal Domain Personal health Domain Overall Condition | Groups that experience “better” or “no change” in resources displayed fewer PTSD symptoms. | “Worse” group reported more posttraumatic symptoms. |
| Slobodin, Caspi, Klein, Berger and Hobfoll, 2011 [21] | Does loss of resources mediate the relationship between trauma and posttraumatic responses? | 317 Bedouin servicemen Israeli Defense Forces | COR-E 5 Traumatic Events 6 | Depression 7 Anxiety 7 | Trauma-related gains in object resources Trauma-related gains in material resources | Gains reflected the ability to use defensive and avoidant strategies effectively. | Loss of personal resources negatively mediates the impact of trauma on development of psychological symptoms. |
| Hall, Bonanno, Bolton and Bass, 2014 [22] | Does baseline psychological distress symptoms and changes in these symptoms were associated with changes in social resources? | 96 male and female adults Torture survivors | Social Support 30 Social Integration 66 Frequency of Social Contact 67 Demographic Variables 8 | Depression 7 Anxiety 7 Posttraumatic Stress Symptoms Traumatic Grief | Social Support Social Integration Frequency of Social Contact | Decreased depression, anxiety and PTSD symptoms was significantly associated to gaining social integration. Decreased depression and PTSD was associated to gaining social contact. | Depression symptoms, PTSD symptoms and traumatic grief were associated with losses to social integration. |
| Hobfoll, Canetti-Nisim and Johnson, 2006 [24] | What is the impact of terrorism on PTSD symptoms and depressive symptoms? | 905 Jewish and Palestinian citizens of Israel Al Aqsa Intifada acts of terrorism | Demographic Variables 8 Terrorism Exposure 9 Economic Resources 10 Psychological Resources 11 Support Satisfaction 12 Protective Attitudes 13 | Depressive Symptoms 14 PTSD 15 | Psychological Resource Gain | Psychosocial resource loss is strongly related to PTSD symptoms and depressive symptoms. | |
| Heath, Hall, Russ, Canetti and Hobfoll, 2012 [25] | What are the transitional relationships among resource loss and psychological distress? | 752 Palestinian adults Political Violence | Intrapersonal and Interpersonal Resources 5 | PTSD 17 Depressive Symptoms 18 | Psychological resource loss and psychological distress predicted each other over time. | ||
| Blaze and Shwalb, 2009 [26] | What are the long term psychological impacts of Hurricane Katrina? | 636 high school aged students Hurricane Katrina | Resource Loss 19 Self-Esteem 20 Optimism 21 | General Psychological Distress (GPD) 22 Posttraumatic Stress (PTS) 23 | Self-esteem scores predicted posttraumatic stress. Lower self-esteem, lower optimism, and greater relocation strongly predicted GPD. | ||
| Littleton, Grills-Taquechel and Axsom, 2009 [27] | What are the risk factors for posttraumatic symptomatology? | 293 female university students Mass shooting at Virginia Tech | Social Support 24 Resource Loss 5 | PTSD 25 Depression 26 Anxiety 27 | Resource loss in the time after shootings predicted experienced trauma. | ||
| Hobfoll, Tracey and Galea, 2006 [28] | Does resource loss predict PTSD and depression? | 2752 random individuals in New York City 11 September 2001 World Trade Center | Sociodemographic characteristics 8 9/11 experiences 28 Lifetime Trauma Event Exposures 29 Social Support 30 Resource Loss and Resource Gain 5 | Panic Attack Symptoms 31 PTSD 32 Depression 33 | Critical role of resource loss in predicting PTSD and depression following terrorism. | ||
| Dekel and Hobfoll, 2007 [29] | Examine emotional adjustment of Holocaust survivors when facing new stressors (Intifada). | 102 Holocaust survivors of Israel Terror and threat of missile attack | Loss of Personal Resources 11 Loss of Interpersonal Resources 11 | PTSD 16 Psychiatric Symptoms 34 | During Holocaust those who lost a spouse or child had higher PTSD symptoms During Intifada higher loss of interpersonal psychological and person resources was strongly associated with higher PTSD. | ||
| Cordova, Walser, Neff and Ruzek, 2005 [30] | To identify factors that influence emotional adjustment after injury to prevent future psychological impairment. | 47 emergency room admitted patients Traumatic Experience | COR-E 5 Social Constraints 35 Stressfulness of Event 36 Acceptance and Action 37 Demographics 8 | PTSD 38 Depression 26 | Greater social constraints were associated with greater PTSD symptoms. | ||
| Littleton, Kumpula and Orcutt, 2011 [31] | Do psychosocial resources predict PTSD symptoms? | 691 college women Mass shooting at Northern Illinois University | Life Trauma History 39 Exposure to Shooting 41 Resource Loss 5 | PTSD 42 Psychological Distress 40 | Resource loss experienced in the aftermath of the campus shooting predicted PTSD symptoms. |
| Authors and Year | Study | Sample Population and Trauma Experienced | Resources Measured | Other Measured Clinical Symptoms | Experienced Resource Gain | Associations of Resource Gain |
|---|---|---|---|---|---|---|
| Littleton, Axsom and Grills-Taquechel, 2009 [32] | Longitudinally examine interpersonal and interpersonal resource loss and gain in relation to college students’ psychological distress. | 193 College Women; ages 18–27 Virginia Tech mass shooting | Resource Loss and Resource Gain 5 Social Support 24 Coping Strategies 43 Exposure to Shooting Incident 41 | Depression 26 Anxiety 27 | Social Support Active Coping | Decrease in depression and anxiety symptoms. |
| Wells, Hobfoll and Lavin, 1999 [33] | Pattern of resource loss and resource gain in pregnant women during pregnancy and following pregnancy. | 71 women Pregnancy | COR-E 5 | Depressive Mood 26 Anger 44 | Gains during and after pregnancy include increase in self pride, optimism, and better relationship with others | Decrease in anger and depressed mood. |
| Hobfoll, Johnson, Ennis and Jackson, 2003 [34] | Study how economic stress (material loss) alters women’s personal and social resources and how changes in the resources impact anger and depressive mood. | 714 women Inner City | Material Loss 5 Mastery 45 Social Support 12 | Depressive Mood 46 Anger 47 | Mastery Gain Material Gain Social Support | Mastery gain has less depressive mood. Decrease of material loss experienced lower depressed mood and anger. |
| Holahan, Moos, Holahan and Cronkite, 1999 [35] | Better understand the role of psychosocial resources in the stress and coping process. | 326 Individuals Community Sample | Sociodemographics 8 Family Support 48 Personality Characteristics 49 Life-Change Events 50 | Depressive Symptoms 51 | Psychosocial Resources | Decrease of depressive symptoms Decrease of excess negative life events. |
| Cook, Aten, Moore, Hook and Davis, 2013 [36] | Examine associations among resource loss, religiousness, posttraumatic growth, and physical and mental health. | 189 college students Hurricane Katrina | Resource Loss 11 General Religiousness 52, 53 Health and Adjustment 54 Posttraumatic Growth 55 | Religious Comfort | Positive adjustment Buffered negative effects of resource loss on emotional health. | |
| Ying, Akutsu, Zhang and Huang, 1997 [37] | Test if sense of coherence serves as a mediator between stressors, resources, and psychological functioning. | 2234 Vietnamese, Cambodian, Laotian, Hmong, and Chinese-Vietnamese refugees | Resistance Deficit Variables 56 Sense of Coherence 57 Psychological Dysfunction 58 | Depression 58 Anxiety 58 | Sense of Cohesion | Lower rates of depression, anxiety and psychosocial dysfunction. |
| Zwieback and et al., 2010 [23] | Analyzed patterns of loss, and gain and subsequent mental health. | 402 survivors of Hurricane Katrina | Social Support 60 Participants Outlook Goal Orientation 61, 62 Health and Hurricane Exposure 63 | Psychological Distress 59 | Social Support Future Orientation Physical Health Insurance | Resource gain showed no effect. |
| Smith and Freedy, 2000 [9] | Examine the role of psychosocial resource loss after the Midwest Flood. The studied resources fully mediated flood effects. | 131 adults Midwest Flood | Flood Exposure 64 Psychosocial Resources 11 Psychological Distress 22 Physical Symptoms 65 | Resource gain was explained. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollifield, M.; Gory, A.; Siedjak, J.; Nguyen, L.; Holmgreen, L.; Hobfoll, S. The Benefit of Conserving and Gaining Resources after Trauma: A Systematic Review. J. Clin. Med. 2016, 5, 104. https://doi.org/10.3390/jcm5110104
Hollifield M, Gory A, Siedjak J, Nguyen L, Holmgreen L, Hobfoll S. The Benefit of Conserving and Gaining Resources after Trauma: A Systematic Review. Journal of Clinical Medicine. 2016; 5(11):104. https://doi.org/10.3390/jcm5110104
Chicago/Turabian StyleHollifield, Michael, Andrea Gory, Jennifer Siedjak, Linda Nguyen, Lucie Holmgreen, and Stevan Hobfoll. 2016. "The Benefit of Conserving and Gaining Resources after Trauma: A Systematic Review" Journal of Clinical Medicine 5, no. 11: 104. https://doi.org/10.3390/jcm5110104
APA StyleHollifield, M., Gory, A., Siedjak, J., Nguyen, L., Holmgreen, L., & Hobfoll, S. (2016). The Benefit of Conserving and Gaining Resources after Trauma: A Systematic Review. Journal of Clinical Medicine, 5(11), 104. https://doi.org/10.3390/jcm5110104