
Ashamed and Afraid: A Scoping Review of the Role of Shame in Post-Traumatic Stress Disorder (PTSD)

Abstract
:1. Introduction
2. Experimental Section
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Results
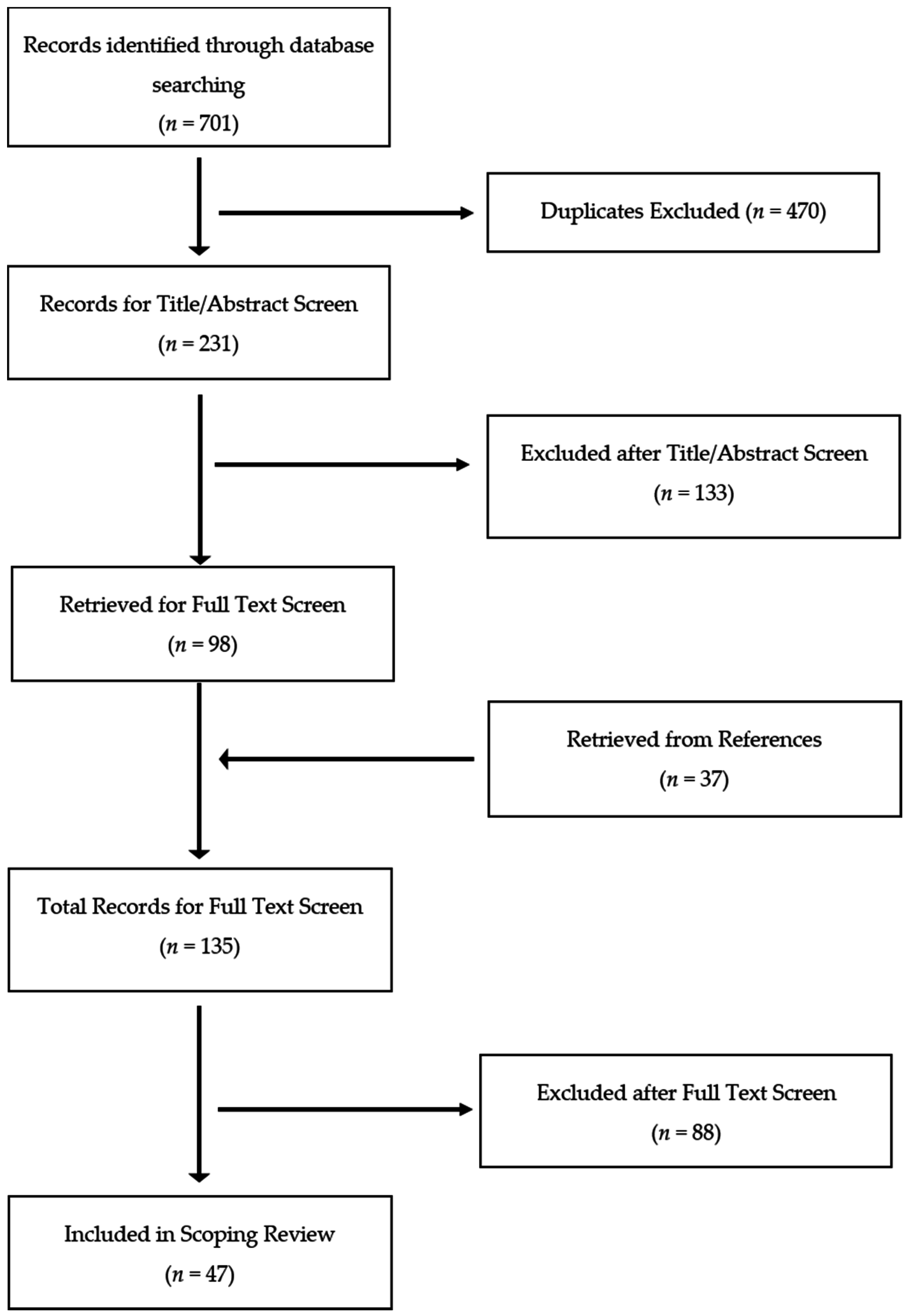
3.1. Overview of Results
3.2. Types of Trauma Exposure and Shame
3.3. The Association of Shame with PTSD
3.4. Shame in the Development and Maintenance of PTSS and PTSD
3.5. Shame as an Outcome and Mediator of PTSD Treatments
3.6. Nonsignificant Findings of Shame in PTSD
3.7. Shame Distinguished from Guilt in PTSD
3.8. Shame as a Mediator between PTSD and Negative Outcomes
4. Discussion
4.1. Implications of Research
4.2. Implications for Clinical Practice
4.3. Limitations of this Scoping Review & Future Directions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Schnurr, P.P.; Friedman, M.J.; Sengupta, A.; Jankowski, M.K.; Holmes, T. PTSD and utilization of medical treatment services among male Vietnam veterans. J. Nerv. Ment. Dis. 2000, 188, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Bradley, R.; Greene, J.; Russ, E.; Dutra, L.; Westen, D. A Multidimensional Meta-Analysis of Psychotherapy for PTSD. Am. J. Psychiatry 2005, 162, 214–227. [Google Scholar] [CrossRef] [PubMed]
- Badour, C.L.; Resnick, H.S.; Kilpatrick, D.G. Associations Between Specific Negative Emotions and DSM-5 PTSD Among a National Sample of Interpersonal Trauma Survivors. J. Interpers. Violence 2015, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Dalgleish, T.; Power, M.J. Emotion-specific and emotion-non-specific components of posttraumatic stress disorder (PTSD): Implications for a taxonomy of related psychopathology. Behav. Res. Ther. 2004, 42, 1069–1088. [Google Scholar] [CrossRef] [PubMed]
- Lewis, H.B. Shame and Guilt in Neurosis; International University Press: New York, NY, USA, 1971. [Google Scholar]
- Dahl, S. Acute response to rape—A PTSD variant. Acta Psychiatr. Scand. Suppl. 1989, 355, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Tracy, J.L.; Robins, R.W. Putting the self into self-conscious emotions: A theoretical model. Psychol. Inq. 2004, 15, 103–125. [Google Scholar] [CrossRef]
- Feiring, C.; Taska, L.; Lewis, M. A process model for understanding adaptation to sexual abuse: The role of shame in defining stigmatization. Child Abus. Negl. 1996, 20, 767–782. [Google Scholar] [CrossRef]
- Sippel, L.M.; Marshall, A.D. Posttraumatic stress disorder symptoms, intimate partner violence perpetration, and the mediating role of shame processing bias. J. Anxiety Disord. 2011, 25, 903–910. [Google Scholar] [CrossRef] [PubMed]
- Tangney, J.; Stuewig, J.; Mashek, D. Moral emotions and moral behavior. Annu. Rev. Psychol. 2007, 58, 345–372. [Google Scholar] [CrossRef] [PubMed]
- Wilson, J.P.; Drozdek, B.; Turkovic, S. Posttraumatic Shame and Guilt. Trauma Violence Abus. 2006, 7, 122–141. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.L. Trauma and Recovery; Basic Books: New York, NY, USA, 1992. [Google Scholar]
- Herman, J.L. Shattered shame states and their repair. In Shattered States: Disorganised Attachment and Its Repair; Karnac Books Ltd.: London, UK, 2012; pp. 157–170. [Google Scholar]
- Lee, D.A.; Scragg, P.; Turner, S. The role of shame and guilt in traumatic events: A clinical model of shame-based and guilt-based PTSD. Br. J. Med. Psychol. 2001, 74, 451–466. [Google Scholar] [CrossRef] [PubMed]
- Caspi, Y.; Slobodin, O.; Klein, E. Cultural Perspectives on the Aftereffects of Combat Trauma: Review of a Community Study of Bedouin IDF Servicemen and Their Families. Rambam Maimonides Med. J. 2015, 6, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Herman, J.L. Posttraumatic stress disorder as a shame disorder. In Shame in the Therapy Hour; Dearing, R.L., Tangney, J.P., Eds.; American Psychological Association: Washington, DC, USA, 2011; Volume 238, pp. 261–275. [Google Scholar]
- Budden, A. The role of shame in posttraumatic stress disorder: A proposal for a socio-emotional model for DSM-V. Soc. Sci. Med. 2009, 69, 1032–1039. [Google Scholar] [CrossRef] [PubMed]
- Taylor, T.F. The influence of shame on posttrauma disorders: have we failed to see the obvious? Eur. J. Psychotraumatol. 2015, 6, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Lanius, R.A.; Frewen, P.; Nazarov, A.; McKinnon, M.C. A Social—Cognitive—Neuroscience Approach to PTSD: Clinical and Research Perspectives. In Neurobiology and Treatment of Traumatic Dissociation: Towards an Embodied Self; Lanius, U.F., Corrigan, F.M., Paulsen, S.L., Eds.; Springer: Wien, Austria, 2013; Volume 18, pp. 69–80. [Google Scholar]
- Lawrence, A.E.; Taft, C.T. Shame, posttraumatic stress disorder, and intimate partner violence perpetration. Aggress. Violent Behav. 2013, 18, 191–194. [Google Scholar] [CrossRef]
- Scheff, T. A social/emotional theory of “mental illness”. Int. J. Soc. Psychiatry 2013, 59, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Velotti, P.; Elison, J.; Garofalo, C. Shame and aggression: Different trajectories and implications. Aggress. Violent Behav. 2014, 19, 454–461. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: towards a methodological framework. Int. J. Soc. Res. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Nazarov, A.; Jetly, R.; Mcneely, H.; Kiang, M.; Lanius, R.; Mc, M. Role of morality in the experience of guilt and shame within the armed forces. Acta Psychiatr. Scand. 2015, 132, 4–19. [Google Scholar] [CrossRef] [PubMed]
- Plana, I.; Lavoie, M.-A.; Battaglia, M.; Achim, A. A meta-analysis and scoping review of social cognition performance in social phobia, posttraumatic stress disorder and other anxiety disorders. J. Anxiety Disord. 2013, 28, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Aakvaag, H.F.; Thoresen, S.; Wentzel-Larsen, T.; Roysamb, E.; Dyb, G. Shame and guilt in the aftermath of terror: The Utoya Island study. J. Trauma. Stress 2014, 27, 618–621. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.S.; Hersh, J.; Herres, J.; Foster, J. HIV-Related Stigma, Shame, and Avoidant Coping: Risk Factors for Internalizing Symptoms Among Youth Living with HIV? Child Psychiatry Hum. Dev. 2016, 47, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Negrao, C.; Bonanno, G.A.; Noll, J.G.; Putnam, F.W.; Trickett, P.K. Shame, humiliation, and childhood sexual abuse: Distinct contributions and emotional coherence. Child Maltreat. 2005, 10, 350–363. [Google Scholar] [CrossRef] [PubMed]
- Uji, M.; Shikai, N.; Shono, M.; Kitamura, T. Contribution of shame and attribution style in developing PTSD among Japanese University women with negative sexual experiences. Arch. Women S Ment. Health 2007, 10, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Shin, K.M.; Cho, S.-M.; Lee, S.H.; Chung, Y.K. A pilot prospective study of the relationship among cognitive factors, shame, and guilt proneness on posttraumatic stress disorder symptoms in female victims of sexual violence. J. Korean Med. Sci. 2014, 29, 831–836. [Google Scholar] [CrossRef] [PubMed]
- Stotz, S.J.; Elbert, T.; Müller, V.; Schauer, M. The relationship between trauma, shame, and guilt: Findings from a community-based study of refugee minors in Germany. Eur. J. Psychotraumatol. 2015, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Andrews, B.; Brewin, C.R.; Rose, S.; Kirk, M. Predicting PTSD symptoms in victims of violent crime: The role of shame, anger, and childhood abuse. J. Abnorm. Psychol. 2000, 109, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Brewin, C.R.; Dalgleish, T.; Joseph, S. A dual representation theory of posttraumatic stress disorder. Psychol. Rev. 1996, 103, 670–686. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.A.; Deblinger, E.; Mannarino, A.P.; Steer, R.A. A multisite, randomized controlled trial for children with sexual abuse-related PTSD symptoms. J. Am. Acad. Child Adolesc. Psychiatry 2004, 43, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Deblinger, E.; Mannarino, A.P.; Cohen, J.A.; Steer, R.A. A follow-up study of a multisite, randomized, controlled trial for children with sexual abuse-related PTSD symptoms. J. Am. Acad. Child Adolesc. Psychiatry 2006, 45, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Feiring, C.; Taska, L.; Chen, K. Trying to understand why horrible things happen: Attribution, shame, and symptom development following sexual abuse. Child Maltreat. 2002, 7, 26–41. [Google Scholar] [CrossRef] [PubMed]
- Feiring, C.; Taska, L.; Lewis, M. Adjustment following sexual abuse discovery: The role of shame and attributional style. Dev. Psychol. 2002, 38, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Feiring, C.; Taska, L.S. The persistence of shame following sexual abuse: A longitudinal look at risk and recovery. Child Maltreat. 2005, 10, 337–349. [Google Scholar] [CrossRef] [PubMed]
- Ginzburg, K.; Butler, L.D.; Giese-Davis, J.; Cavanaugh, C.E.; Neri, E.; Koopman, C.; Classen, C.C.; Spiegel, D. Shame, guilt, and posttraumatic stress disorder in adult survivors of childhood sexual abuse at risk for human immunodeficiency virus: outcomes of a randomized clinical trial of group psychotherapy treatment. J. Nerv. Ment. Dis. 2009, 197, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Harned, M.S.; Korslund, K.E.; Linehan, M.M. A pilot randomized controlled trial of Dialectical Behavior Therapy with and without the Dialectical Behavior Therapy Prolonged Exposure protocol for suicidal and self-injuring women with borderline personality disorder and PTSD. Behav. Res. Ther. 2014, 55, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Layer, S.D.; Roberts, C.; Wild, K.; Walters, J. Postabortion Grief: Evaluating the Possible Efficacy of a Spiritual Group Intervention. Res. Soc. Work Pract. 2004, 14, 344–350. [Google Scholar] [CrossRef]
- Oktedalen, T.; Hoffart, A.; Langkaas, T.F. Trauma-related shame and guilt as time-varying predictors of posttraumatic stress disorder symptoms during imagery exposure and imagery rescripting—A randomized controlled trial. Psychother. Res. 2014, 25, 518–532. [Google Scholar] [CrossRef] [PubMed]
- Resick, P.A.; Galovski, T.E.; O’Brien Uhlmansiek, M.; Scher, C.D.; Clum, G.A.; Young-Xu, Y. A randomized clinical trial to dismantle components of cognitive processing therapy for posttraumatic stress disorder in female victims of interpersonal violence. J. Consult. Clin. Psychol. 2008, 76, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Tangney, J.P.; Dearing, R.L.; Wagner, P.E.; Gramzow, R. The Test of Self-Conscious Affect–3 (TOSCA-3); George Mason University: Fairfax, VA, USA, 2000. [Google Scholar]
- Cook, D.R. Internalized Shame Scale: Technical Manual; Multi-Health Systems, Inc.: North Tonawanda, NY, USA, 1994. [Google Scholar]
- Andrews, B.; Qian, M.; Valentine, J.D. Predicting depressive symptoms with a new measure of shame: The Experience of Shame Scale. Br. J. Clin. Psychol. 2002, 41, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Bockers, E.; Roepke, S.; Michael, L.; Renneberg, B.; Knaevelsrud, C. The role of generalized explicit and implicit guilt and shame in interpersonal traumatization and posttraumatic stress disorder. J. Nerv. Ment. Dis. 2015, 204, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.a.; Keane, T.M. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. Int. Soc. Trauma. Stress Stud. San Antonio TX. 1993, 2, 90–92. [Google Scholar]
- Ojserkis, R.; McKay, D.; Badour, C.L.; Feldner, M.T.; Arocho, J.; Dutton, C. Alleviation of moral disgust, shame, and guilt in posttraumatic stress reactions: An evaluation of comprehensive distancing. Behav. Modif. 2014, 38, 801–836. [Google Scholar] [CrossRef] [PubMed]
- Semb, O.; Stromsten, L.; Sundbom, E.; Fransson, P.; Henningsson, M. Distress after a single violent crime: How shame-proneness and event-related shame work together as risk factors for post-victimization symptoms. Psychol. Rep. 2011, 109, 3–23. [Google Scholar] [CrossRef] [PubMed]
- MacNair, R.M. Perpetration-induced traumatic stress in combat veterans. Peace Confl. 2002, 8, 63–72. [Google Scholar] [CrossRef]
- Lowinger, T.; Solomon, Z. PTSD, Guilt, and Shame Among Reckless Drivers. J. Loss Trauma 2004, 9, 327–344. [Google Scholar] [CrossRef]
- DePrince, A.P.; Chu, A.T.; Pineda, A.S. Links between specific posttrauma appraisals and three forms of trauma-related distress. Psychol. Trauma Theory Res. Pract. Policy 2011, 3, 430–441. [Google Scholar] [CrossRef]
- La Bash, H.; Papa, A. Shame and PTSD symptoms. Psychol. Trauma Theory Res. Pract. Policy 2014, 6, 159–166. [Google Scholar] [CrossRef]
- Hagenaars, M.A.; Fisch, I.; Van Minnen, A. The effect of trauma onset and frequency on PTSD-associated symptoms. J. Affect. Disord. 2011, 132, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Street, A.E.; Arias, I. Psychological abuse and posttraumatic stress disorder in battered women: Examining the roles of shame and guilt. Violence Vict. 2001, 16, 65–78. [Google Scholar] [PubMed]
- Ehlers, A.; Clark, D.M. A cognitive model of posttraumatic stress disorder. Behav. Res. Ther. 2000, 38, 319–345. [Google Scholar] [CrossRef]
- Brewin, C.R.; Andrews, B.; Rose, S. Fear, helplessness, and horror in posttraumatic stress disorder: Investigating. J. Trauma. Stress 2000, 13, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Leskela, J.; Dieperink, M.E.; Thuras, P. Shame and posttraumatic stress disorder. J. Trauma. Stress 2002, 15, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.G.; Reich, C.M.; Woodward, M.J.; Olsen, S.A.; Jones, J.M.; Patton, S.C. How do negative emotions relate to dysfunctional posttrauma cognitions? An examination of interpersonal trauma survivors. Psychol. Trauma 2015, 7, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Harman, R.; Lee, D. The role of shame and self-critical thinking in the development and maintenance of current threat in post-traumatic stress disorder. Clin. Psychol. Psychother. 2010, 17, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Dewey, D.; Schuldberg, D.; Madathil, R. Do peritraumatic emotions differentially predict PTSD symptom clusters? Initial evidence for emotion specificity. Psychol. Rep. 2014, 115, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Dyer, A.S.; Feldmann, R.E.J.; Borgmann, E. Body-related emotions in posttraumatic stress disorder following childhood sexual abuse. J. Child Sex. Abus. Res. Treat. Progr. Innov. Vict. Surviv. Offenders 2015, 24, 627–640. [Google Scholar] [CrossRef] [PubMed]
- Vidal, M.E.; Petrak, J. Shame and adult sexual assault: A study with a group of female survivors recruited from an East London population. Sex. Relatsh. Ther. 2007, 22, 159–171. [Google Scholar] [CrossRef]
- Freed, S.; Andrea, W.D. Autonomic Arousal and Emotion in Victims of Interpersonal Violence: Shame Proneness But Not Anxiety Predicts Vagal Tone. J. Trauma Dissociation 2015, 16, 367–383. [Google Scholar]
- Dorahy, M.J.; Corry, M.; Shannon, M.; Webb, K.; McDermott, B.; Ryan, M.; Dyer, K.F.W. Complex trauma and intimate relationships: the impact of shame, guilt and dissociation. J. Affect. Disord. 2013, 147, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Greenwald, A.G.; Mcghee, D.E.; Schwartz, J.L.K. Measuring Individual Differences in Implicit Cognition: The Implicit Association Test. J. Pers. Soc. Psychol. 1998, 74, 1464–1480. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.G.; McNiff, J.; Clapp, J.D.; Olsen, S.A.; Avery, M.L.; Hagewood, J.H. Exploring negative emotion in women experiencing intimate partner violence: shame, guilt, and PTSD. Behav. Ther. 2011, 42, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Barr, P. A dyadic analysis of negative emotion personality predisposition effects with psychological distress in neonatal intensive care unit parents. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 347–355. [Google Scholar] [CrossRef]
- Pineles, S.L.; Street, A.E.; Koenen, K.C. The Differential Relationships of Shame–Proneness and Guilt–Proneness to Psychological and Somatization Symptoms. J. Soc. Clin. Psychol. 2006, 25, 688–704. [Google Scholar] [CrossRef]
- Robinaugh, D.J.; McNally, R.J. Autobiographical memory for shame or guilt provoking events: Association with psychological symptoms. Behav. Res. Ther. 2010, 48, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Kaysen, D.; Scher, C.D.; Mastnak, J.; Resick, P. Depression in Recent Crime Victims. Behav. Ther. 2006, 36, 235–244. [Google Scholar] [CrossRef]
- Ferguson, T.J.; Crowley, S.L. Measure for Measure: A Multitrait-Multimethod Analysis of Guilt and Shame. J. Pers. Assess. 1997, 69, 425–441. [Google Scholar] [CrossRef]
- Luyten, P.; Fontaine, J.R.J.; Corveleyn, J. Does the Test of Self-Conscious Affect (TOSCA) measure maladaptive aspects of guilt and adaptive aspects of shame? An empirical investigation. Pers. Individ. Dif. 2002, 33, 1373–1387. [Google Scholar] [CrossRef]
- Crocker, L.D.; Haller, M.; Norman, S.B.; Angkaw, A.C. Shame versus trauma-related guilt as mediators of the relationship between PTSD symptoms and aggression among returning veterans. Psychol. Trauma Theory Res. Pract. Policy 2016, 8, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Schoenleber, M.; Sippel, L.M.; Jakupcak, M.; Tull, M.T. Role of trait shame in the association between posttraumatic stress and aggression among men with a history of interpersonal trauma. Psychol. Trauma 2015, 7, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Bryan, C.J.; Morrow, C.E.; Etienne, N.; Ray-Sannerud, B. Guilt, shame, and suicidal ideation in a military outpatient clinical sample. Depress. Anxiety 2013, 30, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Held, P.; Owens, G.P.; Anderson, S.E. The interrelationships among trauma-related guilt and shame, disengagement coping, and PTSD in a sample of treatment-seeking substance users. Traumatology 2015, 21, 285–292. [Google Scholar] [CrossRef]
- Hundt, N.E.; Holohan, D.R. The role of shame in distinguishing perpetrators of intimate partner violence in U.S. veterans. J. Trauma. Stress 2012, 25, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Dunmore, E.; Clark, D.M.; Ehlers, A. A prospective investigation of the role of cognitive factors in persistent posttraumatic stress disorder (PTSD) after physical or sexual assault. Behav. Res. Ther. 2001, 39, 1063–1084. [Google Scholar] [CrossRef]
- Stuewig, J.; Tangney, J.P.; Heigel, C.; Harty, L.; McCloskey, L. Shaming, blaming, and maiming: Functional links among the moral emotions, externalization of blame, and aggression. J. Res. Pers. 2010, 44, 91–102. [Google Scholar] [CrossRef] [PubMed]
- Green, B.L.; Goodman, L.A.; Krupnick, J.L.; Corcoran, C.B.; Petty, R.M.; Stockton, P.; Stern, N.M. Outcomes of Single Versus Multiple Trauma Exposure in a Screening Sample. J. Trauma. Stress 2000, 13, 271–286. [Google Scholar] [CrossRef] [PubMed]
- Foa, E.B.; Riggs, D.S.; Gershuny, B.S. Arousal, numbing, and intrusion: Symptom structure of PTSD following assault. Am. J. Psychiatry 1995, 152, 116–120. [Google Scholar] [PubMed]
- Schore, A.N. The Effects of Early Relational Trauma on Right Brain Development, Affect Regulation, and Infant Mental Health. Infant Ment. Health J. 2001, 22, 201–269. [Google Scholar] [CrossRef]
- Taft, C.T.; Schumm, J.A.; Marshall, A.D.; Panuzio, J.; Holtzworth-munroe, A. Family-of-Origin Maltreatment, Posttraumatic Stress Disorder Symptoms, Social Information Processing Deficits, and Relationship Abuse Perpetration. J. Abnorm. Psychol. 2008, 117, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Rizvi, S.L.; Linehan, M.M. The treatment of maladaptive shame in borderline personality disorder: A pilot study of “opposite action”. Cogn. Behav. Pract. 2005, 12, 437–447. [Google Scholar] [CrossRef]
- Gilbert, P.; Procter, S. Compassionate mind training for people with high shame and self-criticism: Overview and pilot study of a group therapy approach. Clin. Psychol. Psychother. 2006, 13, 353–379. [Google Scholar] [CrossRef]
- Hoffart, A.; Øktedalen, T.; Langkaas, T.F. Self-compassion influences PTSD symptoms in the process of change in trauma-focused cognitive-behavioral therapies: A study of within-person processes. Front. Psychol. 2015, 6, 1273. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Sample Type (n) | Design | PTSS/PTSD Measure 2 | Shame Measure 2 | Findings |
|---|---|---|---|---|---|
| Aakvaag et al. (2014) | Adolescent and adult survivors of terrorism (n = 325) | Cross-sectional | PTSD-RI | PTSD-RI (2 items) | Past month trauma-related shame and guilt associated with PTS 1 in mass-trauma survivors. Greater severity of trauma-related shame or guilt associated with greater PTS severity. |
| Andrews et al. (2000) | Adult victims of violent crime (n = 157) | Longitudinal | PSS-SR | Study-designed semi-structured interview (single item) | Post-traumatic shame and anger predicted PTS at 1-month after crime victimization. Post-traumatic shame and 1-month PTS predicted 6-months PTS. Post-traumatic shame mediated childhood abuse and 6-months PTS. |
| Badour et al. (2015) | Adult survivors of interpersonal trauma (n = 1522) | Cross-sectional | NSES | NSES | Peritraumatic anger, shame, and fear, in order, predicted assault related-PTSD (AR-PTSD). Peritraumatic shame was more associated with AR-PTSD in women; peritraumatic fear was more associated with AR-PTSD in men. |
| Barr (2011) | Couples with sick newborn infants (n = 67) | Cross-sectional | PCL-S | TOSCA | Shame-proneness predicted depression, but not PTS or anxiety. Guilt was a significant predictor of PTS symptoms, depression, and anxiety. |
| Beck et al. (2011) | Female IPV 1 survivors (n = 63) | Cross-sectional | CAPS | ISS | Trait shame, guilt-related distress, and guilt cognitions positively correlated with PTSD. Shame was positively correlated with higher levels of emotional and verbal abuse. Women with IPV marked by high dominance/isolation or emotional/verbal abuse and high shame had higher PTSD severity. Guilt was not a significant moderator. |
| Beck et al. (2015) | Female IPV survivors (n = 109) | Cross-sectional | CAPS | ISS | Trait shame and depression predicted negative thoughts of the self; shame had a larger effect size. Higher guilt associated with negative thoughts of the world. Higher levels of trait shame and guilt but lower levels of depression associated with greater self-blame. |
| Bennett et al. (2016) | Adolescent and young adults living with HIV (n = 88) | Cross-sectional | CPSS | TOSCA-A | Shame-proneness was positively associated with higher levels of PTSD and depression symptoms. Depression was predicted by shame-proneness and HIV-related stigma whereas PTSD was predicted by HIV-related stigma and avoidant coping. |
| Bockers et al. (2015) | Inpatient sample of female survivors of interpersonal trauma: with PTSD (n = 28), without PTSD (n = 32), non-traumatized (n = 92) | Cross-sectional | MINI | TOSCA and IAT (implicit) | Explicit shame and guilt were significantly different across groups; PTSD group had the highest and the non-traumatized group had the lowest. No differences in implicit shame between PTSD group and traumatized/no PTSD group. |
| Brewin et al. (2000) | Adult victims of violent crime (n = 138) | Longitudinal | PSS-SR | Semi-structured interview (single item) | Trauma-related shame experienced by a subset of participants and significant predictor of PTSD. |
| Bryan et al. (2013) | Active duty military personnel (n = 69) | Cross-sectional | PCL | PFQ2 | Guilt and trait shame are higher in military personnel with history of suicidal ideation. Both guilt and trait shame mediated the relationship between PTSD or depression and suicidal ideation; guilt had a stronger relationship with suicidal ideation. |
| Cohen et al. (2004) | Sexually abused children (n = 203) | Longitudinal; RCT 1 | K-SADS-PL | CAPS | Children randomized to TF-CBT showed greater reductions in shame attributions and PTSD from baseline to post-treatment in comparison to children in CCT 1. |
| Crocker et al. (2016) | Returning veterans, primarily male (n = 127) | Cross-sectional | PCL-S | ISS | PTSD predicted trait shame and global guilt. When controlling for global guilt, shame partially mediated PTSD symptoms and verbal aggression. |
| Dahl (1989) | Young adult and adult survivors of rape and attempted rape, primarily female (n = 55) | Cross-sectional | IES and semi-structured interview | CPRS (single item) | Assault-related shame, guilt, and suicidal ideation present in the majority of rape survivors. |
| Deblinger et al. (2006) | Child survivors of sexual abuse (n = 183) | Longitudinal; RCT | K-SADS-PL | TSQ and CAPS | Children in TF-CBT 1 showed significant decrease in trauma-related shame during post-treatment, 6-month, and 12-month follow ups in comparison to children in Child-Centered Therapy. |
| DePrince et al. (2011) | College students with at least one traumatic event (n = 98); Adult female survivors of child abuse/interpersonal crime (n = 94); Adult female survivors of nonsexual IPV (n = 236) | Cross-sectional | RCMS and PDS | TAQ | Posttraumatic shameful appraisals predicted PTSD in college students and female survivors of child abuse or interpersonal crime. Posttraumatic shameful appraisals did not predict PTSD in the nonsexual IPV sample. |
| Dewey et al. (2014) | College students (n = 144) | Cross-sectional | PCL-S | TEQ (subscales: anger, fear, guilt, shame, disgust) | In order, peritraumatic fear, anger, and shame were the top three predictors of avoidance and numbing symptoms. Peritraumatic guilt, fear, and anger predicted re-experiencing; shame did not. Peritraumatic guilt and shame were the strongest predictors of hyperarousal symptoms. |
| Dorahy et al. (2013) | Treatment-receiving adult survivors of Northern Irish conflict exposure with PTSD (n = 65) | Cross-sectional | SRC and clinical interview | CoSS, SSGS, and PFQ-2 | Clinical dissociation group had significantly higher levels of (a) trait shame and guilt and (b) state shame, guilt, and pride than the subclinical dissociation group. Dissociation, trait/state shame, and trait/state guilt significantly predicted complex PTSD. |
| Dorahy et al. (2016) | Adults with Dissociative Disorders (n = 39); Two comparison groups: adults with child abuse-related chronic PTSD (n = 13) & adults with mixed psychiatric diagnoses and child abuse histories (n = 21) | Cross-sectional | CTQ and clinical interview | PFQ-2 | Child maltreatment significantly contributed to trait shame and child abuse and neglect significantly contributed to trait guilt. Emotional abuse was the strongest predictor of both trait shame and trait guilt. |
| Dyer et al. (2015) | Adult female German inpatients/outpatients with PTSD from CSA 1 (n = 23), BPD (n = 25), BPD and PTSD after CSA (n = 22), and healthy controls (n = 27) | Cross-sectional | SCID-I | SBA and BIGSS | Participants with child sexual abuse identified more body areas as associated with traumatic experiences. Psychiatrically diagnosed groups rated trauma-related body areas to have more body-related shame, guilt, and disgust compared to the healthy controls. |
| Feiring et al. (2002) | Child and adolescent survivors of CSA (n = 137) | Longitudinal | IAE and CITES-R | Study-designed measure | Trauma-related shame was a significant mediator between abuse attributions both after the traumatic event and one year later with both PTSD and depression symptoms. |
| Feiring et al. (2002) | Child and adolescent survivors of CSA (n = 147) | Longitudinal | CITES-R and TSI | Study-designed measure | Trauma-related shame at abuse discovery was a small predictor of PTSD, depression, and self-esteem, but trauma-related shame one year after abuse was a strong predictor of PTSD, depression, and low self-esteem. Girls showed more shame than boys at the time of abuse, but decreased in shame over a year. Boys did not show a significant decrease in shame from abuse discovery to one year later. |
| Feiring and Taska (2005) | Adolescent survivors of CSA (n = 118) | Longitudinal | CITES-R and TSI | TOSCA and study-designed measure | Trauma-related shame experienced one year after CSA predicted high trauma-related shame six years after CSA and symptoms of hyperarousal, intrusive recollections, and avoidance. Children low in trauma-related shame have better treatment prognosis. |
| Freed and D’Andrea (2015) | Adult female survivors of interpersonal violence with PTSD (n = 27) | Cross-sectional | PCL-IV | PANAS (single-item) and study-designed adjective list | Shame-proneness was the only predictor of autonomic arousal in a trauma reminder task. Inactivation of the peripheral nervous system in PTSD patients was associated with fear and shame at baseline, anxiety and shame during the task, and shame during recovery period. Trait shame predicted lower respiratory sinus arrhythmia during recovery suggesting difficulty regulating affect after trauma reminders. State shame was the only predictor of lower RSA during the task, more than fear and anxiety. |
| Ginzburg et al. (2009) | Adult female CSA survivors (n = 166) | Longitudinal; RCT | PCL-S | ARBQ (Shame subscale) | Both treatment conditions demonstrated reductions in PTSD, abuse-related shame, and guilt. Improvement in shame mediated treatment effect on PTSD. No mediating effect found for guilt. |
| Hagenaars et al. (2011) | Treatment-seeking adults (n = 110) | Cross-sectional | CAPS | Study-designed single item | Multiple trauma group reported more recent shame experiences than single trauma group, independent of PTSD severity. Association between shame and childhood versus adult trauma group did not hold after controlling for PTSD severity. |
| Harman and Lee (2010) | Treatment-seeking adults (n = 49) | Cross-sectional | PDS | ESS | Shame-proneness positively correlated with self-criticizing thinking style, above and beyond contributions of PTSD and depressive symptoms. |
| Harned et al. (2014) | Adult females with comorbid BPD 1 (n = 26) | Longitudinal; RCT | PSS-I | ESS | Clinically significant and reliable improvement in shame-proneness and PTSD after one year of both tested therapies, DBT and DBT + DBT PE 1. |
| Held et al. (2015) | Treatment-seeking substance users (n = 72) | Cross-sectional | PCL-S | SSGS | Trauma-related shame provided direct and indirect (through avoidant coping) pathways for the relationship between trauma-related guilt and PTSD severity. |
| Hundt and Holohan (2012) | Treatment-seeking adult male veterans (n = 264) | Cross-sectional | PCL-C | ISS | Trait shame mediation of PTSD and IPV perpetration relationship not significant when depression taken into account. |
| La Bash and Papa (2014) | College students (n = 99) | Cross-sectional | PCL | Modified TLEQ | Peritraumatic shame mediated relationship between risk factors (trauma type and number of potentially traumatic events) and PTSD symptoms. |
| Layer et al. (2004) | Adult females (n = 35) | Longitudinal | IES-R | ISS | Spiritually-based group intervention associated with improvement in trait shame and PTSD symptoms in women suffering from post-abortion grief. |
| Leskela et al. (2002) | Adult male veterans (n = 107) | Cross-sectional | PCL-M and CES | TOSCA | Shame-proneness, not guilt-proneness, positively correlated with PTSD severity. |
| Lowinger and Solomon (2004) | Adult males convicted of reckless driving (n = 75) | Cross-sectional | PTSD-I | TOSCA | Trait shame did not significantly differ between reckless drivers who had caused an accidental death and control group. |
| Negrao II et al. (2005) | Female children and adults (n = 137) | Cross-sectional | PSS | EMFACS (nonverbal) and narrative coding | Coherence between facial and verbal shame expression correlated with PTSD severity in non-disclosing group of CSA survivors. |
| Ojserkis et al. (2014) | College students (n = 45) | Cross-sectional | LEC, PCL-C, IES-R, and PCI | TOSCA and visual analogue scale | State shame, but not trait shame, correlated with PTSS. |
| Øktedalen et al. (2015) | Norwegian adults in an inpatient setting (n = 65) | Longitudinal; RCT | PSS-I and PSS-SR | Study-designed self-report measure | Within-person improvements in trauma-related shame and trauma-related guilt predicted subsequent reductions in PTSD during both interventions, PE1 and modified PE. |
| Pineles et al. (2006) | College females (n = 156) | Cross-sectional | PCL | TOSCA | Shame-proneness, independent of guilt-proneness, predicted PTSD symptoms whereas guilt independent of shame did not. |
| Resick et al. (2008) | Adult female victims of interpersonal violence (n = 150) | Longitudinal; RCT | CAPS and PDS | ESS | PTSD and trait shame improved over time in all three conditions (components of CPT 1). |
| Robinaugh and McNally (2010) | Adults (n = 140) | Cross-sectional | PCL | SSGI | Event-related shame predicted PTSD symptoms. |
| Schoenleber et al. (2015) | Adult male survivors of interpersonal trauma (n = 103) | Cross-sectional | LEC and PCL-C | PANAS (single-item) | Trait shame accounted for the association between posttraumatic symptoms and aggressive behavior whereas trait guilt did not. |
| Semb et al. (2011) | Adult victims of single violent crime (n = 35) | Cross-sectional | HTQ | TOSCA and visual analogue scale | Both shame-proneness and event-related shame positively correlated with severity of posttraumatic distress. Level of event-related shame mediated the effect of shame-proneness on posttraumatic symptoms. |
| Shin et al. (2014) | Treatment-seeking Korean adult female survivors of sexual violence (n = 38) | Longitudinal; prospective | CAPS, PSS-SR, and PCI | PFQ | No correlation between shame-proneness and PTSD severity once depression severity was controlled. Similar findings for guilt-proneness. |
| Sippel and Marshall (2011) | Adult civilians (n = 47) | Cross-sectional | CAPS | Emotional Stroop task (implicit) and self-referential encoding task (implicit) | Speed of implicit shame processing and PTSD severity inversely correlated. Shame processing mediated relationship between PTSD severity and frequency of IPV perpetration. |
| Stotz et al. (2015) | Male refugee youth in Germany (age 11–20) (n = 32) | Cross-sectional | UCLA PTSD | SVQ | Both trauma-related shame and guilt positively correlated with PTSD severity. |
| Street and Arias (2001) | Adult female IPV survivors in domestic violence shelters (n = 63) | Cross-sectional | MS-Civilian | TOSCA | Shame-proneness significantly predicted of PTSD symptoms, guilt-proneness did not. |
| Uji et al. (2007) | Japanese college females (n = 172) | Cross-sectional | IES-R | ASSQ and AAI | Event-related shame directly predicted PTSD, whereas attribution style did not. |
| Vidal and Petrak (2007) | Adult female survivors of adult sexual assault (n = 25) | Cross-sectional | IES-R | ESS and study-designed measure | Shame positively correlated with traumatic stress. |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saraiya, T.; Lopez-Castro, T. Ashamed and Afraid: A Scoping Review of the Role of Shame in Post-Traumatic Stress Disorder (PTSD). J. Clin. Med. 2016, 5, 94. https://doi.org/10.3390/jcm5110094
Saraiya T, Lopez-Castro T. Ashamed and Afraid: A Scoping Review of the Role of Shame in Post-Traumatic Stress Disorder (PTSD). Journal of Clinical Medicine. 2016; 5(11):94. https://doi.org/10.3390/jcm5110094
Chicago/Turabian StyleSaraiya, Tanya, and Teresa Lopez-Castro. 2016. "Ashamed and Afraid: A Scoping Review of the Role of Shame in Post-Traumatic Stress Disorder (PTSD)" Journal of Clinical Medicine 5, no. 11: 94. https://doi.org/10.3390/jcm5110094
APA StyleSaraiya, T., & Lopez-Castro, T. (2016). Ashamed and Afraid: A Scoping Review of the Role of Shame in Post-Traumatic Stress Disorder (PTSD). Journal of Clinical Medicine, 5(11), 94. https://doi.org/10.3390/jcm5110094