Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 ,
,  ,
,
Abstract
:1. Background
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria and Study Selection
2.3. Data Items and Collection Process
2.4. Assessment of Methodological Quality for Selected Trials
2.5. Data Synthesis and Analysis
3. Results
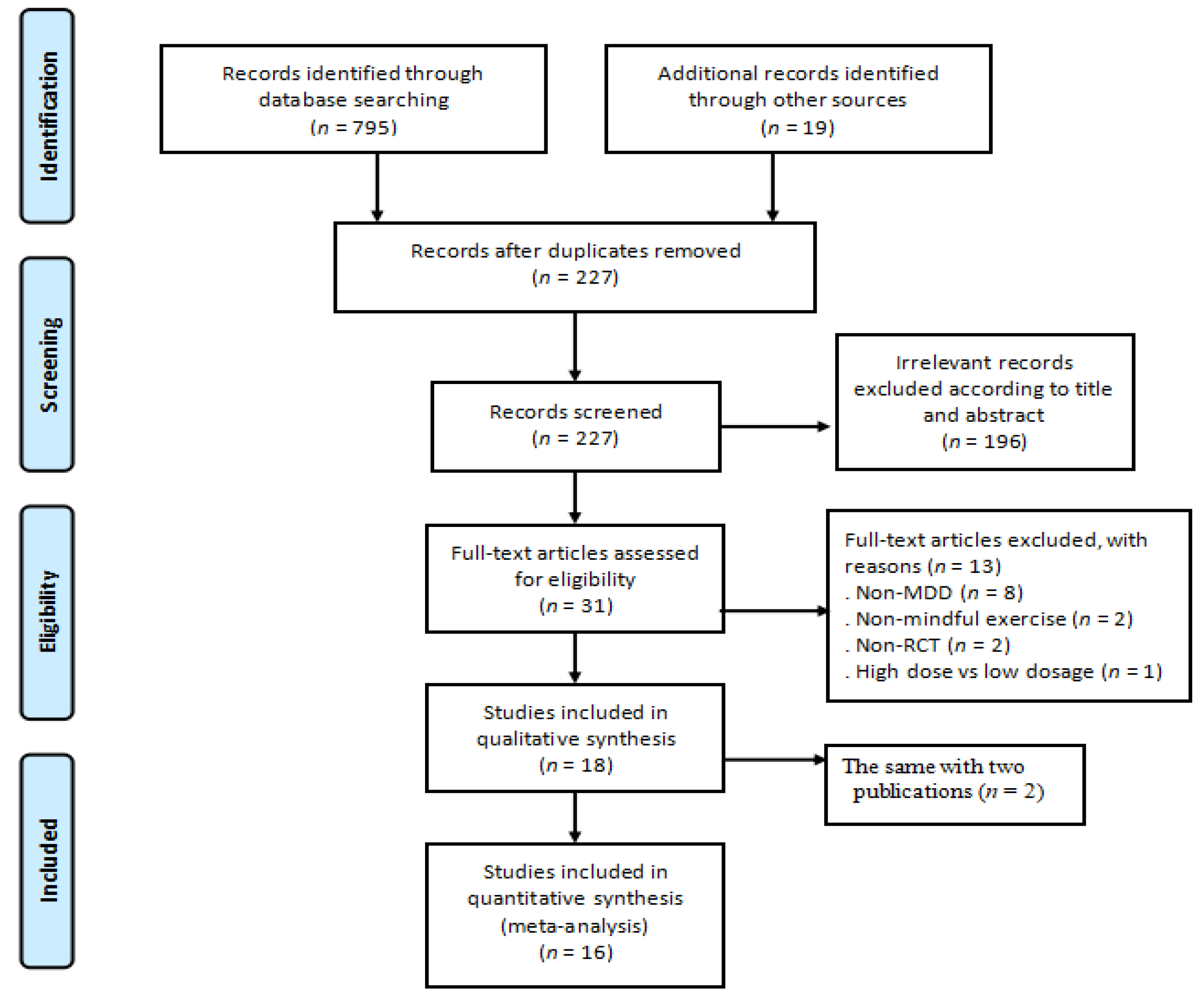
3.1. Trial Selection
3.2. Study Characteristics
3.3. Study Quality Assessment
3.4. Effects of Meditative Movements on Dichotomous and Continuous Outcomes
3.5. Moderator Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hasin, S.; Sarvet, L.; Meyers, L. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry 2018, 75, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Woo, M.; Jeon, J.; Noh, J. Importance of remission and residual somatic symptoms in health-related quality of life among outpatients with major depressive disorder: A cross-sectional study. Health Qual. Life Outcomes 2014, 12, 188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, E.; Fournier, A.; Sisitsky, T. The economic burden of adults with major depressive disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Leichsenring, F.; Steinert, C.; Hoyer, J. Psychotherapy versus pharmacotherapy of depression: What’s the evidence? Z. Psychosom. Med. Psychother. 2016, 62, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.; Katakam, K.; Schou, A. Selective serotonin reuptake inhibitors versus placebo in patients with major depressive disorder: A systematic review with meta-analysis and trial sequential analysis. BMC Psychiatry 2017, 17, 58. [Google Scholar]
- Jakobsen, C.; Hansen, L.; Storebø, J. The effects of cognitive therapy versus “no intervention” for major depressive disorder. PLoS ONE 2011, 6, e28299. [Google Scholar] [CrossRef] [PubMed]
- Jakobsen, C.; Hansen, L.; Simonsen, E. The effect of interpersonal psychotherapy and other psychodynamic therapies versus “treatment as usual” in patients with major depressive disorder. PLoS ONE 2011, 6, e19044. [Google Scholar] [CrossRef]
- Ferguson, J. SSRI antidepressant medications: Adverse effects and tolerability. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, I.; Deacon, J.; Huedo-Medina, B. Initial severity and antidepressant benefits: A meta-analysis of data submitted to the Food and Drug Administration. PLoS Med. 2008, 5, e45. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, A.; Salanti, G. Comparative efficacy and acceptability of 12 new-generation antidepressants: A multiple treatments meta-analysis. Lancet 2009, 373, 746–758. [Google Scholar] [CrossRef]
- Mathew, J.; Charney, S. Publication bias and the efficacy of antidepressants. Am. J. Psychiatry 2009, 166, 140–145. [Google Scholar] [CrossRef] [PubMed]
- Pigott, E.; Leventhal, M.; Alter, G. Efficacy and effectiveness of antidepressants: Current status of research. Psychother. Psychosom. 2010, 79, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Ravindran, V.; Balneaves, G.; Faulkner, G. Canadian network for mood and anxiety treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depression disorder: Section 5: Complementary and alternative medicine treatments. Can. J. Psychiatry 2016, 61, 576–587. [Google Scholar] [CrossRef] [PubMed]
- Krogh, H.; Speyer, H.; Gluud, C. Exercise for patients with major depression: A systematic review with meta-analysis and trial sequential analysis. BMJ Open 2017, 7, e014820. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Chen, X. Baduanjin exercise for stroke rehabilitation: A systematic review with meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 600. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Xiao, Z. Tai Chi for health benefits in patients with multiple sclerosis: A systematic review. PLoS ONE 2017, 12, e0170212. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; SasaKi, J.; Wang, H. A systematic review and meta-analysis baduanjin qigong for health benefits: Randomized controlled trials. Evid.-Based Complement. Altern. Med. 2017, 2017, 4548706. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, H.; Li, T. Effect of Health-Qigong on spinal mobility and disease activity in people with ankylosing spondylitis. Le Trav. Hum. 2017, 80, 1585–1597. [Google Scholar]
- Zou, L.; Yeung, A.; Quan, X. Mindfulness-based Baduanjin exercise for depression and anxiety in people with physical or mental illnesses: A systematic review and meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2018, 15, 321. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Yeung, A.; Quan, X. A systematic review and meta-analysis of mindfulness-based (Baduanjin) exercise for alleviating musculoskeletal pain and improving sleep quality in people with chronic diseases. Int. J. Environ. Res. Public Health 2018, 15, 206. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Wang, C.; Yeung, A. A review study on the beneficial effects of Baduanjin. J. Altern. Complement. Med. 2018, 24, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Kachan, D.; Olano, H.; Tannenbaum, L. Prevalence of mindfulness practices in the US workforce: National health interview survey. Prev. Chronic Dis. 2017, 14, E01. [Google Scholar] [CrossRef] [PubMed]
- Cramer, H.; Anheyer, D.; Lauche, R. A systematic review of yoga for major depressive disorder. J. Affect Disord. 2017, 213, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Lavretsky, H.; Alstein, L.; Ercoli, O. Complementary use of Tai Chi Chih augments escitalopram treatment of geriatric depression: A randomized controlled trial. Am. J. Geriatr. Psychiatry 2011, 19, 839–850. [Google Scholar] [CrossRef] [PubMed]
- Chou, K.; Lee, P.; Yu, E. Effect of Tai Chi on depressive symptoms amongst Chinese older patients with depressive disorders: A randomized clinical trial. Int. J. Geriatr. Psychiatry 2004, 19, 1105–1107. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Lepoutre, V.; Wayne, P. Tai chi treatment for depression in Chinese Americans: A pilot study. Am. J. Phys. Med. Rehabil. 2012, 91, 863Y870. [Google Scholar] [CrossRef] [PubMed]
- Yeung, S.; Feng, R.; Kim, H. A pilot randomized controlled study of Tai Chi with passive and active controls in the treatment of depressed Chinese Americans. J. Clin. Psychiatry 2017, 78, e522–e528. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Wong, Q.; Sze, S. A Chinese Chan-based mind-body intervention for patients with depression. J. Affect Disord. 2012, 142, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Elkins, R.; Moseley, M.; Sherrington, C. Growth in the Physiotherapy Evidence Database (PEDro) and use of the PEDro scale. Br. J. Sports Med. 2013, 47, 188–189. [Google Scholar] [CrossRef] [PubMed]
- Bühlmayer, L.; Birrer, D.; Röthlin, P. Effects of mindfulness practice on performance-relevant parameters and performance outcomes in sports: A meta-analysis review. Sports Med. 2017, 47, 2309–2321. [Google Scholar] [CrossRef] [PubMed]
- Higgins, T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: http://www.cochrane-handbook.org/Selezione%20a%20cura%20di%20Liliana%20LeoneSeminario%2030/03/2010 (accessed on 15 May 2018).
- Williams, W. A structured interview guide for the Hamilton Depression Rating Scale. Arch. Gen. Psychiatry 1998, 45, 742–747. [Google Scholar] [CrossRef]
- Field, T.; Diego, M.; Delgado, J. Tai Chi/yoga reduces prenatal depression, anxiety and sleep disturbance. Complement. Ther. Clin. Pract. 2013, 19, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Field, T.; Diego, M.; Medina, L. Yoga and massage therapy reduce prenatal depression and prematurity. J. Body Mov. Ther. 2012, 16, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuver, K.; Lewis, B. Mindfulness-based yoga intervention for women with depression. Complement. Ther. Med. 2016, 26, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Barrett, M.; Cucchiara, A. A breathing-based meditation intervention for patients with major depressive disorder following inadequate response to antidepressants: A randomized controlled pilot study. J. Clin. Psychiatry 2017, 78, e59–e63. [Google Scholar] [CrossRef] [PubMed]
- Kinser, P.; Bourguignon, C.; Whaley, D. Feasibility, acceptability, and effects of gentle Hatha yoga for women with major depression: From a randomized controlled mixed methods study. Arch. Psychatry Nurs. 2013, 27, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Uebelacker, L.; Battle, C.; Sutton, K. A pilot randomized controlled trial comparing prenatal yoga to perinatal health education for antenatal depression. Arch. Women’s Ment. Health 2016, 19, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Uebelacker, L.; Tremont, G.; Gillette, L. Adjunctive yoga vs. health education for persistent major depression: A randomized controlled trial. Psychol. Med. 2017, 47, 2130–2142. [Google Scholar] [CrossRef] [PubMed]
- Prathikanti, S.; Rivera, R.; Cochran, A. Treating major depression with yoga: A prospective, randomized, controlled trial. PLoS ONE 2017, 12, e0173869. [Google Scholar] [CrossRef] [PubMed]
- Janakiramaiah, N.; Gangadhar, B.; Murthy, N. Antidepressant efficacy of SudarshanKriya Yoga (SKY) in melancholia: A randomized comparison with electroconvulsive therapy (ECT) and imipramine. J. Affect Disord. 2000, 57, 255–259. [Google Scholar] [CrossRef]
- Sharma, V.; Mondal, S.; Goswami, U. Effect of Sahaj Yoga on depressive disorders. Indian J. Physiol. Pharmacol. 2015, 49, 462–468. [Google Scholar]
- Sarubin, N.; Nothdurfter, C.; Schule, C. The influence of Hatha yoga as an add-on treatment in major depression on hypothalamic-pituitary-adrenal-axia activity: A randomized controlled trial. J. Psychiatry Res. 2014, 53, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.; Chan, J.; Cheung, J. Qigong and Tai Chi for mood regulation. J. Lifelong Learn Psychiatry 2018, 16, 40–47. [Google Scholar] [CrossRef]
- Ma, X.; Yue, Z.; Gong, Z. The effect of diaphragmatic breathing on attention, negative affect and stress in healthy adults. Front. Psychol. 2017, 8, 874. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.; Gerbarg, L. Muench. Breathing practices for treatment of psychiatric and stress- related medical conditions. Psychiatry Clin. North Am. 2013, 36, 121–140. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.; Tam, B.; Lai, C. Revealing the neural mechanisms underlying the beneficial effects of Tai Chi: A neuroimaging perspective. Am. J. Chin. Med. 2018, 46, 231–259. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Han, Y.; Sze, S. A randomized controlled neurophysiological study of a Chinese Chan-based mind-body intervention in patients with major depressive disorder. Evid.-Based Complement. Altern. Med. 2013, 2013, 812096. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Berger, C.; Manheimer, E. Meditative therapies for reducing anxiety: A systematic review and meta-analysis of randomized controlled trials. Depress. Anxiety 2012, 29, 545–562. [Google Scholar] [CrossRef] [PubMed]
- Nüesch, E.; Reichenbach, S.; Trelle, S. The importance of allocation concealment and patient blinding in osteoarthritis trials: A meta-epidemiologic study. Arthritis Care Res. 2009, 61, 1633–1641. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Country | Participant Characteristics | Intervention Protocol | Outcome Measured and Safety | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnostic Criteria, Assessor | N (AT) | MDD | Female | Predominant Ethnicity | Age (Year) | Weekly Dosage (Type of ☯ and ○, Qualified Instructor [Yes/No]) | TTT (Min) | Ind or Grp | Duration (Weeks),FU | Drug and/or PSY | 1 = Primary and 2 = Secondary Outcome (Measuring Instrument); Adverse Event | |
| Lavretsky et al. (2011) [24] USA | DSM-IV, a psychiatrist | 73 (6.8%) | 100% | 61.6% | 74% Caucasian | 70.57 | ☯ (36): 1 × 120 min/ week (Tai Chi, yes) ○ (37): 1 × 120 min/ week (HE, yes) | 1200 | Grp | 10, No | Yes | 1. Depression severity (HAM-D24); No |
| Chou et al. (2004) [25] China | DSM-IV, a psychiatrist | 14 (0%) | 90% | 50% | 100% Chinese | 72.6 | ☯ (7): 3 × 45 min/week (Tai Chi, yes) ○ (7): waitlist | 1620 | Grp | 12, No | Yes | 1. Depression severity (CES-D); No |
| Yeung et al. (2012) [26] USA | DSM-IV, a psychiatrist | 39 (5.1%) | 100% | 77% | 100% Chinese American | 55 | ☯ (26):2 × 60 min/week (Tai Chi, yes); ○ (13): waitlist | 1440 | Grp | 12, No | Yes | 1. Remission rate (HAM-D17 scores ≤ 7), Response rate (≥ 50% improvement on the HAM-D17 score) and depression severity (HAM-D17); No |
| Yeung et al. (2017) [27] USA | DSM-IV, a psychiatrist | 67 (25.3%) | 100% | 72% | 100% Chinese American | 54 | ☯ (23):2 × 60 min/week (Tai Chi, yes); ○ (22):2 × 60 min × 2/week (HE, yes); ◎ (22): waitlist | 1440 | Grp | 12, 12 | None | 1. Remission rate (HAM-D17 ≤ 7), Response rate (≥ 50% improvement on the HAMA17 score), and depression severity (HAM-D17 and BDI); No |
| Chan et al. (2012) [28] China | DSM-IV, a psychiatrist | 75 (33.3%) | 100% | 80% | 100% Chinese | 46.48 | ☯ (25):1 × 90 min/week (Qigong, yes); ○ (25):1 × 90 min/week (CBT, yes); ◎ (25): waitlist | 900 | Grp | 10, No | Yes | 1. Depression severity (HAM-D17 and BDI); No |
| Field et al. (2013) [34] USA | DSM-IV, a RA supervised by a psychiatrist | 92 (18.5%) | 100% | 100% | 57% Hispanic, 40% Black | 26.6 | ☯ (46):1 × 20 min/ week (Tai Chi +Yoga, yes); ○ (46): waitlist | 240 | Grp | 12, No | None | 1. Depression severity (CES-D), 2. Anxiety (State-Trait Anxiety Inventory); No |
| Field et al. (2012) [35] USA | SCID, a RA supervised by a psychiatrist | 84 (11%) | 100% | 100% | 38% Hispanic, 40% Black, 12% Caucasian | 28.57 | ☯ (28):1 × 20 min/week (Yoga, yes); ○ (28):1 × 20 min/week (massage, yes); ◎ (28): standard care | 240 | Grp | 12, No | None | 1. Depression severity (CES-D), 2. Anxiety (State-Trait Anxiety Inventory); No |
| Janakiramaiah et al. (2000) [42] India | DSM-IV, a psychiatrist | 45 (0%) | 100% | 44.4% | 100% Indian | 38.7 | ☯ (15) :4–6 × 45 min/week (Yoga, yes); ○ (15): 3 times/week Electroconvulsive therapy; ◎ (15):150 mg/day (imipramine) | 900 | Grp | 4, No | No in ☯ | 1. Remission rate (HAM-D17 score ≤ 7), Depression severity (HAM-D17 and BDI); No |
| Sarubin et al. (2014) [44] Germany | DSM-IV, a psychiatrist | 53 (0%) | 100% | 39.5% | 100% Caucasian | 40.25 | ☯ (22):1 × 60 min/week (Yoga, yes); ○ (31):300 mg/day (QXR) or 10 mg/day (ESC) | 300 | Grp | 5, No | No in ☯ | 1. Response rate (≥ 50% improvement on the HAMA21 score) and depression severity (HAM-D21); No |
| Schuver et al. (2016) [36] USA | SCID, RAs supervised by a psychiatrist | 40 (15%) | 100% | 100% | 80% Caucasian | 42.68 | ☯ (20): 2 × 60–75 min/week (Yoga, no) + 15 min (weekly telephone counselor); ○ (20): 2 × 65 min/week (self-walking) + 15 min (weekly telephone counselor) | 1740 | Ind | 12, 4 | Yes | 1. Depression severity (BDI); No |
| Sharma et al. (2005) [43] India | DSM-IV, two psychiatrists | 30 (0%) | 100% | 36.7% | 100% Indian | 31.77 | ☯ (15):3 × 30 min/week (Yoga, yes); ○ (15): sitting quietly | 720 | Grp | 8, No | Yes | 1. Remission rates (HAM-D17 score ≤ 7). depression severity (HAM-D17), 2. Anxiety (HAM-A17); No |
| Sharma et al. (2017) [37] USA | DSM-IV, a psychiatrist | 25 (12%) | 100% | 72% | 92% Caucasian | 37.19 | ☯ (13): 6 × 210 min for week 1 + 1 × 90 min for week 2–8 (Yoga, yes) + 20–25 min daily home practice; ○ (12): waitlist | 1890 | Mixed | 8, No | Yes | 1. Remission rate (HAM-D17 score ≤ 7), response rate (≥ 50% improvement on the HAMA17 score and Depression severity (HAM-D17 and BDI), 2. Anxiety (Beck Anxiety Inventory); No |
| Kinser et al. (2013) [38] USA | MINI, a board-certified clinician | 27 (33%) | 81.5% | 100% | 63% Caucasian | 43.26 | ☯ (15): 1 × 75 min/week + home practice (Yoga, yes); ○ (12): 1 × 75 min/week (HE, yes) | 600 | Mixed | 8, 52 | Yes | 1. Depression severity (Patient Health Questionnaire-9), 2. Anxiety (State Trait Anxiety Inventory); No |
| Uebelacker et al. (2016) [39] USA | DSM-IV, psychiatrists | 20 (10%) | 75% | 100% | 75% Caucasian | 28.4 | ☯ (12):1 × 75min × 1/week + home practice (Yoga, yes); ○ (8): 1 × 75 min/week (WW, yes) | 675 | Mixed | 9, No | None | 1. Depression severity (QIDS); No |
| Ubelacker et al. (2017) [40] USA | SDM-IV, two psychologists | 122 (14.8%) | 64.7% | 84.4% | 84% Caucasian | 46.5 | ☯ (63): 2 × 80 min/week (Yoga, yes); ○ (59): 1–2 × 60min/week (HE, yes) | 1600 | Grp | 10, 34 | Yes | 1. Remission rate (QIDS scores ≤ 5), response rate ≥ 50% improvement on the QIDS), and depression severity (the QIDS); No |
| Prathikanti et al. (2017) [41] USA | MINI, a psychiatrist | 38 (34.2%) | 100% | 68% | 58% Caucasian | 43.4 | ☯ (20):2 × 90min/week (Yoga, yes); ○ (18):2 × 90 min/week (Education on Yoga history& philosophy, yes) | 1440 | Grp | 8, No | None | 1. Depression severity (BDI); No |
| Reference | Item 1 | Item 2 | Item 3 | Item 4 | Item 5 | Item 6 | Item 7 | Item 8 | Item 9 | Sum Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Lavretsky et al. (2011) [24] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/9 |
| Chou et al. (2004) [25] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8/9 |
| Yeung et al. (2012) [26] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/9 |
| Yeung et al. (2017) [27] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 6/9 |
| Chan et al. (2012) [28] | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 7/9 |
| Field et al. (2013) [34] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8/9 |
| Field et al. (2012) [35] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9/9 |
| Janakiramaiah et al. (2000) [42] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8/9 |
| Sarubin et al. (2014) [44] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7/9 |
| Schuver et al. (2016) [36] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 1 | 6/9 |
| Sharma et al. (2005) [43] | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 7/9 |
| Sharma et al. (2017) [37] | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 8/9 |
| Kinser et al. (2013) [38] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 6/9 |
| Uebelacker et al. (2016) [39] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 8/9 |
| Ubelacker et al. (2017) [40] | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 8/9 |
| Prathikanti et al. (2017) [41] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 8/9 |
| Categorical Moderator | Outcome | Level | No. of Studies/Comparisons | Hedges’ g | 95% Confidence Interval | I2, % | Test for between-Group Homogeneity | ||
|---|---|---|---|---|---|---|---|---|---|
| Q-Value | df(Q) | p-Value | |||||||
| Attrition Rate ≥15% | Depression | Yes | 8 | −0.59 | −0.96 to −0.32 | 5.42% | 0.33 | 1 | 0.57 |
| No | 11 | −0.52 | −0.77 to −0.26 | 48.39% | |||||
| 100% of MDD | Depression | Yes | 16 | −0.62 | −0.83 to −0.42 | 35.21% | 2.37 | 1 | 0.12 |
| No | 3 | −0.23 | −0.68 to 0.22 | 0% | |||||
| Predominant Ethnicity | Depression | Caucasian/Hispanic | 11 | −0.54 | −0.78 to −0.29 | 41.18% | 0.00 | 1 | 0.97 |
| Chinese/Indians | 8 | −0.62 | −0.97 to −0.28 | 33.3% | |||||
| Control Type | Depression | Active | 13 | −0.45 ☯ | −0.67 to −0.23 | 11.8% | 2.76 | 1 | 0.15 ☯ |
| Passive | 6 | −0.79 ☯ | −1.13 to −0.46 | 51.05% | |||||
| Mindfulness Type | Depression | Taichi/Qigong | 6 ※ | −0.64 | −1.04 to −0.23 | 44.07% | 0.02 | 1 | 0.87 |
| Yoga | 12 ※ | −0.7 | −1.35 to −0.04 | 72.83% | |||||
| Intervention Duration | Depression | <12 weeks | 12 | −0.61 | −0.87 to −0.35 | 56.14% | 0.3 | 1 | 0.59 |
| ≥12 weeks | 7 | −0.5 | −0.82 to −0.17 | 0% | |||||
| Training mode | Depression | Group | 15 | −0.55 ® | −0.77 to −0.33 | 32.3% | 0.71 | 1 | 0.4 |
| Mixed | 3 | −0.84 ® | −1.47 to −0.21 | 63.21% | |||||
| Drug and/or psychotherapy | Depression | Yes | 9 | −0.52 | −0.80 to −0.23 | 49.94% | 0.21 | 1 | 0.65 |
| No | 10 | −0.61 | −0.89 to −0.33 | 19.19% | |||||
| Continuous Moderator | Level | No. of Studies/Comparisons | β | 95% Confidence Interval | Q-Value | df | p | ||
| Mean age | Depression | 19 | 0.00292 | −0.00923 to 0.01506 | 0.22 | 1 | 0.63 | ||
| Total minutes in practice | Depression | 19 | −0.00003 | −0.0003 to −0.22368 | 0.05 | 1 | 0.82 | ||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zou, L.; Yeung, A.; Li, C.; Wei, G.-X.; Chen, K.W.; Kinser, P.A.; Chan, J.S.M.; Ren, Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2018, 7, 195. https://doi.org/10.3390/jcm7080195
Zou L, Yeung A, Li C, Wei G-X, Chen KW, Kinser PA, Chan JSM, Ren Z. Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2018; 7(8):195. https://doi.org/10.3390/jcm7080195
Chicago/Turabian StyleZou, Liye, Albert Yeung, Chunxiao Li, Gao-Xia Wei, Kevin W. Chen, Patricia Anne Kinser, Jessie S. M. Chan, and Zhanbing Ren. 2018. "Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 7, no. 8: 195. https://doi.org/10.3390/jcm7080195
APA StyleZou, L., Yeung, A., Li, C., Wei, G. -X., Chen, K. W., Kinser, P. A., Chan, J. S. M., & Ren, Z. (2018). Effects of Meditative Movements on Major Depressive Disorder: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine, 7(8), 195. https://doi.org/10.3390/jcm7080195