Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort


 and
and
Abstract
:1. Introduction
2. Methods
2.1. Data Sources
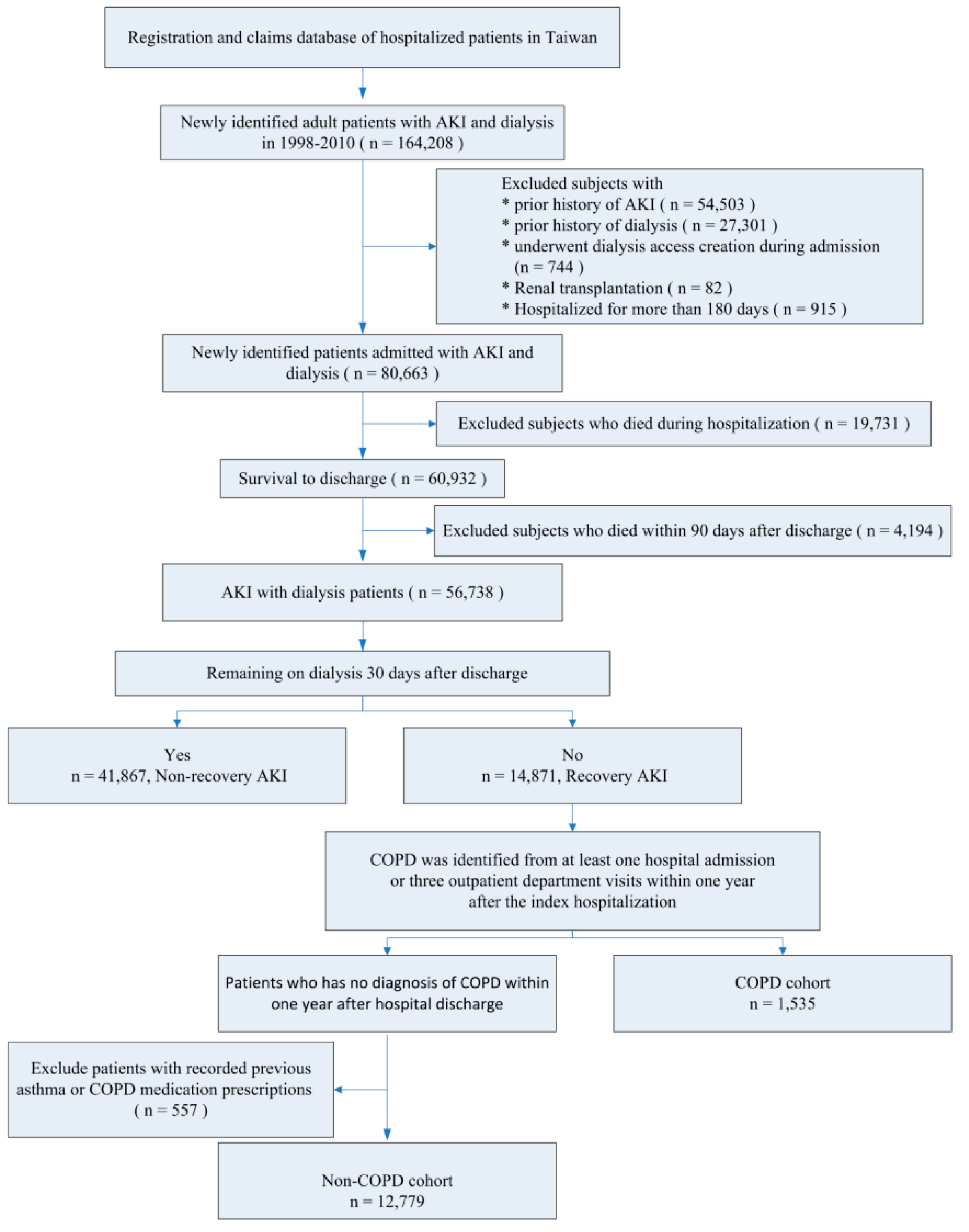
2.2. Study Group
2.3. Baseline Characteristics
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
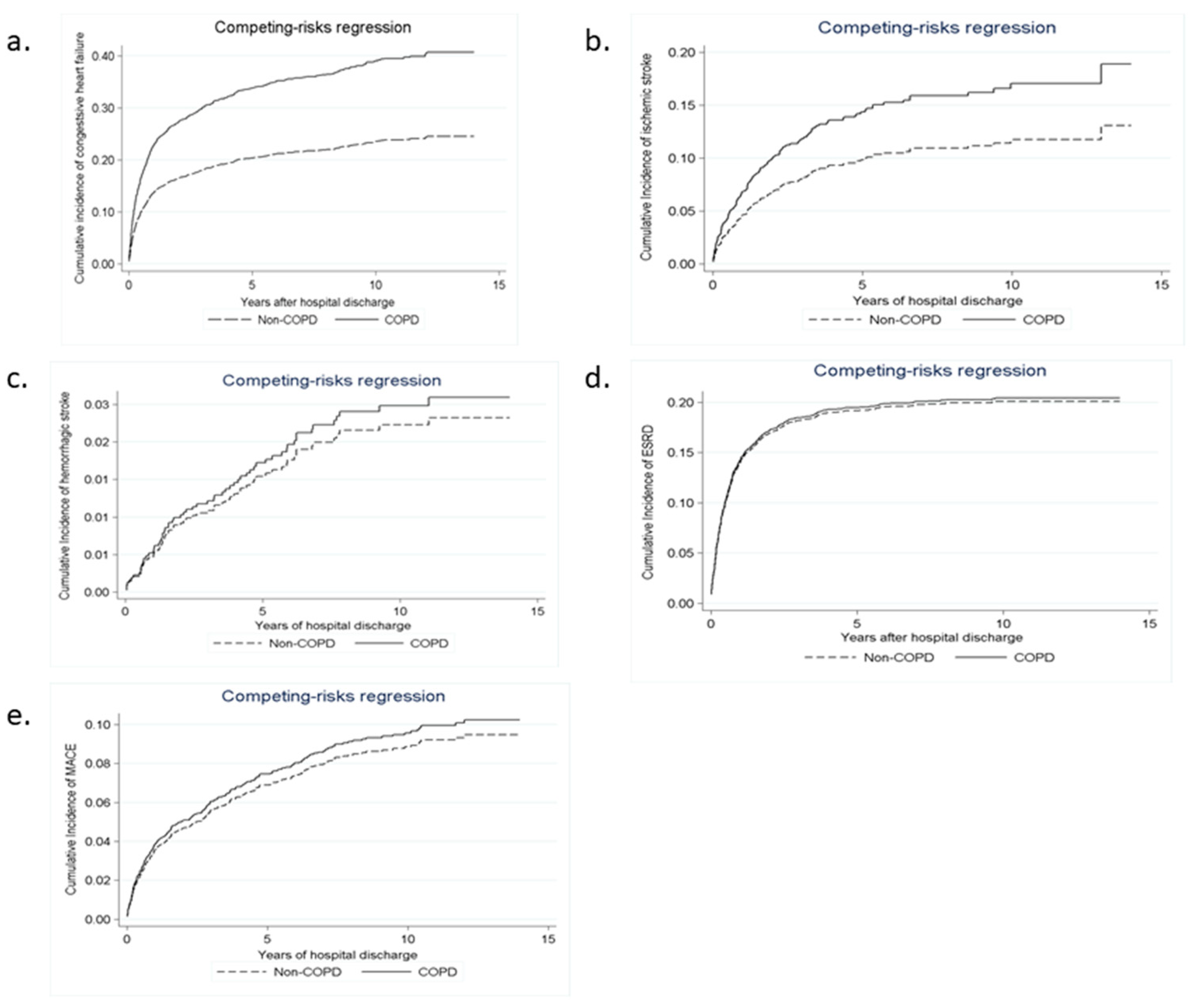
3.2. Long-Term Risks of Death, Stroke, and CHF
3.3. Long-Term Risks of MACE and ESRD
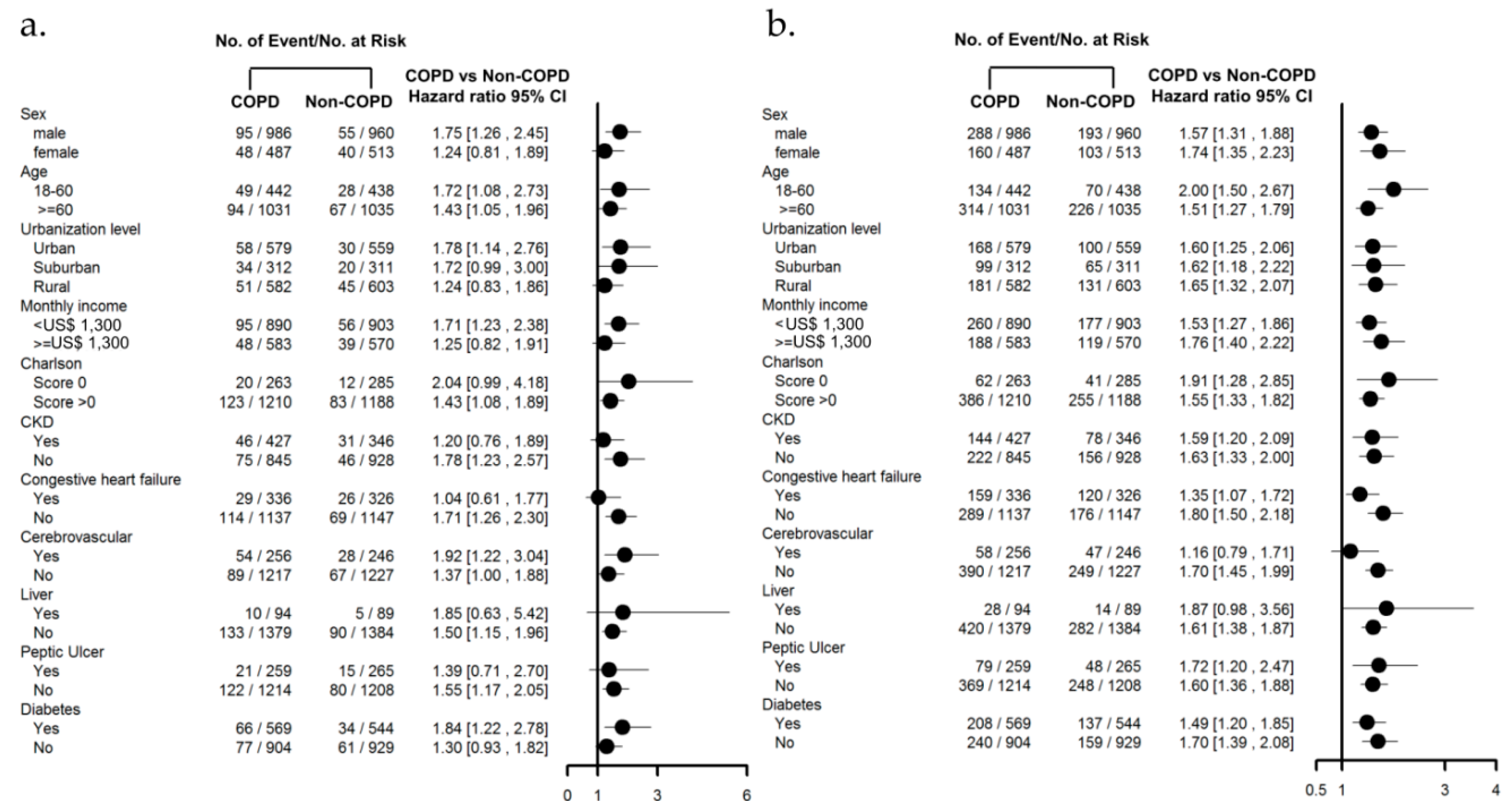
3.4. Subgroup Analysis with Comorbidities
4. Discussion
4.1. Risk of COPD after AKI-D
4.2. Stroke Risk in Patients with COPD after AKI-D
4.3. CHF Risk in Patients with COPD after AKI-D
4.4. Risk of MI and ESRD in Patients with COPD after AKI-D
4.5. Care of Patients with COPD after AKI-D
4.6. Limitation and Strength
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ali, T.; Khan, I.; Simpson, W.; Prescott, G.; Townend, J.; Smith, W.; Macleod, A. Incidence and outcomes in acute kidney injury: A comprehensive population-based study. J. Am. Soc. Nephrol. 2007, 18, 1292–1298. [Google Scholar] [CrossRef] [PubMed]
- Liangos, O.; Wald, R.; O’Bell, J.W.; Price, L.; Pereira, B.J.; Jaber, B.L. Epidemiology and outcomes of acute renal failure in hospitalized patients: A national survey. Clin. J. Am. Soc. Nephrol. 2006, 1, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Ishani, A.; Xue, J.L.; Himmelfarb, J.; Eggers, P.W.; Kimmel, P.L.; Molitoris, B.A.; Collins, A.J. Acute kidney injury increases risk of ESRD among elderly. J. Am. Soc. Nephrol. 2009, 20, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Waikar, S.S.; Winkelmayer, W.C. Chronic on acute renal failure: Long-term implications of severe acute kidney injury. JAMA 2009, 302, 1227–1229. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wu, C.H.; Huang, T.M.; Wang, C.Y.; Lai, C.F.; Shiao, C.C.; Chang, C.H.; Lin, S.L.; Chen, Y.Y.; Chen, Y.M.; et al. Long-term risk of coronary events after AKI. J. Am. Soc. Nephrol. 2014, 25, 595–605. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wu, P.C.; Wu, C.H.; Huang, T.M.; Chang, C.H.; Tsai, P.R.; Ko, W.J.; Chen, L.; Wang, C.Y.; Chu, T.S.; et al. The impact of acute kidney injury on the long-term risk of stroke. J. Am. Heart Assoc. 2014, 3, e000933. [Google Scholar] [CrossRef] [PubMed]
- Husain-Syed, F.; McCullough, P.A.; Birk, H.W.; Renker, M.; Brocca, A.; Seeger, W.; Ronco, C. Cardio-pulmonary-renal interactions: A multidisciplinary approach. J. Am. Coll. Cardiol. 2015, 65, 2433–2448. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Shiao, C.C.; Chang, C.H.; Huang, T.M.; Lai, C.F.; Lin, M.C.; Chiang, W.C.; Chu, T.S.; Wu, K.D.; Ko, W.J.; et al. Long-term outcomes after dialysis-requiring acute kidney injury. Biomed. Res. Int. 2014, 2014, 365186. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.L.; Jaber, B.L.; Faubel, S.; Chawla, L.S.; Acute Kidney Injury Advisory Group of American Society of Nephrology. AKI transition of care: A potential opportunity to detect and prevent CKD. Clin. J. Am. Soc. Nephrol. 2013, 8, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, C.; Latancia, M.T.; Otterbein, L.E.; Netti, P.A. Update on renal replacement therapy: Implantable artificial devices and bioengineered organs. Tissue Eng. Part B Rev. 2016, 22, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Anthonisen, N.R.; Connett, J.E.; Enright, P.L.; Manfreda, J.; Lung Health Study Research Group. Hospitalizations and mortality in the lung health study. Am. J. Respir. Crit. Care Med. 2002, 166, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Hansell, A.L.; Walk, J.A.; Soriano, J.B. What do chronic obstructive pulmonary disease patients die from? A multiple cause coding analysis. Eur. Respir. J. 2003, 22, 809–814. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.Y.; Liao, K.M. Chronic obstructive pulmonary disease is associated with risk of chronic kidney disease: A nationwide case-cohort study. Sci. Rep. 2016, 6, 25855. [Google Scholar] [CrossRef] [PubMed]
- Virzi, G.; Day, S.; de Cal, M.; Vescovo, G.; Ronco, C. Heart-kidney crosstalk and role of humoral signaling in critical illness. Crit. Care 2014, 18, 201. [Google Scholar] [CrossRef] [PubMed]
- Andres-Hernando, A.; Altmann, C.; Bhargava, R.; Okamura, K.; Bacalja, J.; Hunter, B.; Ahuja, N.; Soranno, D.; Faubel, S. Prolonged acute kidney injury exacerbates lung inflammation at 7 days post-acute kidney injury. Physiol. Rep. 2014, 2, e12084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Bittleman, D.; Cruz, D.; Endre, Z.; Fitzgerald, R.L.; et al. Acute kidney disease and renal recovery: Consensus report of the acute disease quality initiative (ADQI) 16 workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef] [PubMed]
- Chao, C.T.; Hou, C.C.; Wu, V.C.; Lu, H.M.; Wang, C.Y.; Chen, L.; Kao, T.W. The impact of dialysis-requiring acute kidney injury on long-term prognosis of patients requiring prolonged mechanical ventilation: Nationwide population-based study. PLoS ONE 2012, 7, e50675. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.J.; Chao, C.T.; Huang, Y.C.; Wang, C.Y.; Chang, C.H.; Huang, T.M.; Lai, C.F.; Huang, H.Y.; Shiao, C.C.; Chu, T.S.; et al. The impact of acute kidney injury with temporary dialysis on the risk of fracture. J. Bone Miner. Res. 2013, 29, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Wu, C.J.; Lin, C.J.; Wu, V.C.; National Taiwan University Study Group on Acute Renal Failure Group. Long-term risk of upper gastrointestinal hemorrhage after advanced AKI. Clin. J. Am. Soc. Nephrol. 2015, 10, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Li, C.H.; Chen, W.C.; Liao, W.C.; Tu, C.Y.; Lin, C.L.; Sung, F.C.; Chen, C.H.; Hsu, W.H. The association between chronic obstructive pulmonary disease and Parkinson’s disease: A nationwide population-based retrospective cohort study. QJM 2015, 108, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.Y.; Jian, Z.H.; Nfor, O.N.; Ku, W.Y.; Ko, P.C.; Lung, C.C.; Ho, C.C.; Pan, H.H.; Huang, C.Y.; Liang, Y.C.; et al. The effects of pulmonary diseases on histologic types of lung cancer in both sexes: A population-based study in Taiwan. BMC Cancer 2015, 15, 834. [Google Scholar] [CrossRef] [PubMed]
- Liao, K.M.; Chen, C.Y. Incidence and risk factors of atrial fibrillation in Asian COPD patients. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 2523–2530. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Hu, Y.H.; Wu, C.H.; Kao, C.C.; Wang, C.Y.; Yang, W.S.; Lee, H.H.; Chang, Y.S.; Lin, Y.H.; Wang, S.M.; et al. Administrative data on diagnosis and mineralocorticoid receptor antagonist prescription identified patients with primary aldosteronism in Taiwan. J. Clin. Epidemiol. 2014, 67, 1139–1149. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.S.; Lai, M.S.; Gau, S.S.; Wang, S.C.; Tsai, H.J. Concordance between patient self-reports and claims data on clinical diagnoses, medication use, and health system utilization in Taiwan. PLoS ONE 2014, 9, e112257. [Google Scholar] [CrossRef] [PubMed]
- Chu, Y.T.; Wu, S.C.; Lee, Y.C.; Lai, M.S.; Tam, S.C. Assessing measures of comorbidity using national health insurance databases. Taiwan J. Public Health 2010, 29, 191–200. [Google Scholar]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the national health insurance research database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Yang, Y.W.; Hung, S.C.; Kuo, K.L.; Wu, K.D.; Wu, V.C.; Hsieh, T.C.; National Taiwan University Study Group on Acute Renal Failure. Ketoanalogues supplementation decreases dialysis and mortality risk in patients with anemic advanced chronic kidney disease. PLoS ONE 2017, 12, e0176847. [Google Scholar]
- Ou, S.M.; Chen, Y.T.; Chao, P.W.; Lee, Y.J.; Liu, C.J.; Yeh, C.M.; Chen, T.J.; Chen, T.W.; Yang, W.C.; Li, S.Y. Nonsteroidal anti-inflammatory drug use is associated with cancer risk reduction in chronic dialysis patients. Kidney Int. 2013, 84, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.J.; Bai, C.H.; Yeh, W.T.; Chiu, H.C.; Pan, W.H. Influence of metabolic syndrome and general obesity on the risk of ischemic stroke. Stroke 2006, 37, 1060–1064. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Lee, W.Y.; Yang, J.; Lo, J.C.; Gurwitz, J.H. Statin therapy and risks for death and hospitalization in chronic heart failure. JAMA 2006, 296, 2105–2111. [Google Scholar] [CrossRef] [PubMed]
- Kip, K.E.; Hollabaugh, K.; Marroquin, O.C.; Williams, D.O. The problem with composite end points in cardiovascular studies: The story of major adverse cardiac events and percutaneous coronary intervention. J. Am. Coll. Cardiol. 2008, 51, 701–707. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Chang, C.H.; Wang, C.Y.; Lin, Y.H.; Kao, T.W.; Lin, P.C.; Chu, T.S.; Chang, Y.S.; Chen, L.; Wu, K.D.; et al. Risk of fracture in primary aldosteronism: A population-based cohort study. J. Bone Miner. Res. 2017, 32, 743–752. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Chueh, S.J.; Chen, L.; Chang, C.H.; Hu, Y.H.; Lin, Y.H.; Wu, K.D.; Yang, W.S.; Taiwan Primary Aldosteronism Investigation Study Group. Risk of new-onset diabetes mellitus in primary aldosteronism: A population study over 5 years. J. Hypertens. 2017, 35, 1698–1708. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet Respi. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Baty, F.; Putora, P.M.; Isenring, B.; Blum, T.; Brutsche, M. Comorbidities and burden of COPD: A population based case-control study. PLoS ONE 2013, 8, e63285. [Google Scholar] [CrossRef] [PubMed]
- Faubel, S.; Edelstein, C.L. Mechanisms and mediators of lung injury after acute kidney injury. Nat. Rev. Nephrol. 2016, 12, 48–60. [Google Scholar] [CrossRef] [PubMed]
- Lie, M.L.; White, L.E.; Santora, R.J.; Park, J.M.; Rabb, H.; Hassoun, H.T. Lung T lymphocyte trafficking and activation during ischemic acute kidney injury. J. Immunol. 2012, 189, 2843–2851. [Google Scholar] [CrossRef] [PubMed]
- Altmann, C.; Andres-Hernando, A.; McMahan, R.H.; Ahuja, N.; He, Z.; Rivard, C.J.; Edelstein, C.L.; Barthel, L.; Janssen, W.J.; Faubel, S. Macrophages mediate lung inflammation in a mouse model of ischemic acute kidney injury. Am. J. Physiol. Ren. Physiol. 2012, 302, 421–432. [Google Scholar] [CrossRef] [PubMed]
- Caramori, G.; Adcock, I.M.; Di Stefano, A.; Chung, K.F. Cytokine inhibition in the treatment of COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 397–412. [Google Scholar] [PubMed] [Green Version]
- Pandey, K.C.; De, S.; Mishra, P.K. Role of proteases in chronic obstructive pulmonary disease. Front. Pharmacol. 2017, 8, 512. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Aguilar, N.E.; Vargas-Camano, M.E.; Hernandez-Pliego, R.R.; Chaia-Semerena, G.M.; Perez-Chavira, M.R. Immunopathology of chronic obstructive pulmonary disease. Rev. Alerg. Mex. 2017, 64, 327–346. [Google Scholar] [PubMed]
- Polosa, R.; Malerba, M.; Cacciola, R.R.; Morjaria, J.B.; Maugeri, C.; Prosperini, G.; Gullo, R.; Spicuzza, L.; Radaeli, A.; Di Maria, G.U. Effect of acute exacerbations on circulating endothelial, clotting and fibrinolytic markers in COPD patients. Intern. Emerg. Med. 2013, 8, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Muir, K.W.; Tyrrell, P.; Sattar, N.; Warburton, E. Inflammation and ischaemic stroke. Curr. Opin. Neurol. 2007, 20, 334–342. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Young, G.H.; Huang, P.H.; Lo, S.C.; Wang, K.C.; Sun, C.Y.; Liang, C.J.; Huang, T.M.; Chen, J.H.; Chang, F.C.; et al. In acute kidney injury, indoxyl sulfate impairs human endothelial progenitor cells: Modulation by statin. Angiogenesis 2013, 16, 609–624. [Google Scholar] [CrossRef] [PubMed]
- Bonventre, J.V. Pathophysiology of AKI: Injury and normal and abnormal repair. Contrib. Nephrol. 2010, 165, 9–17. [Google Scholar] [PubMed]
- Hosohata, K. Role of oxidative stress in drug-induced kidney injury. Int. J. Mol. Sci. 2016, 17, 1826. [Google Scholar] [CrossRef] [PubMed]
- Reis, A.H. Acidemia and blood free fatty acids: Analysis of cardiovascular risk factors in a new context. Discov. Med. 2017, 23, 183–188. [Google Scholar] [PubMed]
- Gorter, K.A.; Stehouwer, M.C.; Van Putte, B.P.; Vlot, E.A.; Urbanus, R.T. Acidosis induced by carbon dioxide insufflation decreases heparin potency: A risk factor for thrombus formation. Perfusion 2017, 32, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Checherita, I.A.; David, C.; Ciocalteu, A.; Lascar, I.; Budala, L. Oral treatment of metabolic acidosis in hemodialyzed patients and the implications on the hemodynamic status. Rom. J. Morphol. Embryol. 2013, 54, 539–543. [Google Scholar] [PubMed]
- Hu, M.C.; Shiizaki, K.; Kuro-o, M.; Moe, O.W. Fibroblast growth factor 23 and Klotho: Physiology and pathophysiology of an endocrine network of mineral metabolism. Annu. Rev. Physiol. 2013, 75, 503–533. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.C.; Shi, M.; Cho, H.J.; Adams-Huet, B.; Paek, J.; Hill, K.; Shelton, J.; Amaral, A.P.; Faul, C.; Taniguchi, M.; et al. Klotho and phosphate are modulators of pathologic uremic cardiac remodeling. J. Am. Soc. Nephrol. 2015, 26, 1290–1302. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, Y.; Gao, W.; Yuan, C.; Zhang, S.; Zhou, H.; Huang, M.; Yao, X. Klotho reduction in alveolar macrophages contributes to cigarette smoke extract-induced inflammation in chronic obstructive pulmonary disease. J. Biol. Chem. 2015, 290, 27890–27900. [Google Scholar] [CrossRef] [PubMed]
- Majumdar, V.; Nagaraja, D.; Christopher, R. Association of the functional kL-VS variant of Klotho gene with early-onset ischemic stroke. Biochem. Biophys. Res. Commun. 2010, 403, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Yoon, J.; An, S.W.; Kuro-o, M.; Huang, C.L. Soluble Klotho protects against uremic cardiomyopathy independently of fibroblast growth factor 23 and phosphate. J. Am. Soc. Nephrol. 2015, 26, 1150–1160. [Google Scholar] [CrossRef] [PubMed]
- Druml, W. Acute renal failure is not a “cute” renal failure! Intensive. Care Med. 2004, 30, 1886–1890. [Google Scholar] [CrossRef] [PubMed]
- Griffo, R.; Spanevello, A.; Temporelli, P.L.; Faggiano, P.; Carone, M.; Magni, G.; Ambrosino, N.; Tavazzi, L.; Investigators, S. Frequent coexistence of chronic heart failure and chronic obstructive pulmonary disease in respiratory and cardiac outpatients: Evidence from suspirium, a multicentre Italian survey. Eur. J. Prev. Cardiol. 2017, 24, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Macchia, A.; Rodriguez Moncalvo, J.J.; Kleinert, M.; Comignani, P.D.; Gimeno, G.; Arakaki, D.; Laffaye, N.; Fuselli, J.J.; Massolin, H.P.; Gambarte, J.; et al. Unrecognised ventricular dysfunction in COPD. Eur. Respir. J. 2012, 39, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, M.; Agrawal, S.; Garg, L.; Garg, A.; Bhatia, N.; Kadaria, D.; Reed, G. Effect of chronic obstructive pulmonary disease on in-hospital mortality and clinical outcomes after ST-segment elevation myocardial infarction. Am. J. Cardiol. 2017, 119, 1555–1559. [Google Scholar] [CrossRef] [PubMed]
- Anand, I.S.; Chandrashekhar, Y.; Rao, S.K.; Malhotra, R.M.; Ferrari, R.; Chandana, J.; Ramesh, B.; Shetty, K.J.; Boparai, M.S. Body fluid compartments, renal blood flow, and hormones at 6000 m in normal subjects. J. Appl. Physiol. 1993, 74, 1234–1239. [Google Scholar] [CrossRef] [PubMed]
- Walley, K.R.; Lewis, T.H.; Wood, L.D. Acute respiratory acidosis decreases left ventricular contractility but increases cardiac output in dogs. Circ. Res. 1990, 67, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Mishra, J.; Ma, Q.; Prada, A.; Mitsnefes, M.; Zahedi, K.; Yang, J.; Barasch, J.; Devarajan, P. Identification of neutrophil gelatinase-associated lipocalin as a novel early urinary biomarker for ischemic renal injury. J. Am. Soc. Nephrol. 2003, 14, 2534–2543. [Google Scholar] [CrossRef] [PubMed]
- Solak, Y.; Yilmaz, M.I.; Siriopol, D.; Saglam, M.; Unal, H.U.; Yaman, H.; Gok, M.; Cetinkaya, H.; Gaipov, A.; Eyileten, T.; et al. Serum neutrophil gelatinase-associated lipocalin is associated with cardiovascular events in patients with chronic kidney disease. Int. Urol. Nephrol. 2015, 47, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Jia, M.; Yan, X.; Cao, L.; Barnes, P.J.; Adcock, I.M.; Huang, M.; Yao, X. Increased neutrophil gelatinase-associated lipocalin (NGAL) promotes airway remodelling in chronic obstructive pulmonary disease. Clin. Sci. (Lond). 2017, 131, 1147–1159. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Ishii, J.; Kitagawa, F.; Takahashi, H.; Sugiyama, K.; Tada, M.; Kanayama, K.; Takahashi, K.; Hayashi, H.; Koide, S.; et al. Plasma neutrophil gelatinase-associated lipocalin as a predictor of cardiovascular events in patients with chronic kidney disease. BioMed Res. Int. 2016, 2016, 8761475. [Google Scholar] [CrossRef] [PubMed]
- Nymo, S.H.; Ueland, T.; Askevold, E.T.; Flo, T.H.; Kjekshus, J.; Hulthe, J.; Wikstrand, J.; McMurray, J.; Van Veldhuisen, D.J.; Gullestad, L.; et al. The association between neutrophil gelatinase-associated lipocalin and clinical outcome in chronic heart failure: Results from CORONA*. J. Intern. Med. 2012, 271, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, G.C.; Hurst, J.R.; Smith, C.J.; Hubbard, R.B.; Wedzicha, J.A. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest 2010, 137, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Qaseem, A.; Wilt, T.J.; Weinberger, S.E.; Hanania, N.A.; Criner, G.; van der Molen, T.; Marciniuk, D.D.; Denberg, T.; Schunemann, H.; Wedzicha, W.; et al. Diagnosis and management of stable chronic obstructive pulmonary disease: A clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann. Int. Med. 2011, 155, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Dell’Aniello, S.; Ernst, P. Concurrent use of long-acting bronchodilators in COPD and the risk of adverse cardiovascular events. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Non COPD | COPD | p-Value | Non COPD | COPD | p-Value | |
| (n = 12,779) | (n = 1535) | (n = 1473) | (n = 1473) | |||
| Age (year, SD) | 63.63 ± 16.39 | 74.02 ± 11.31 | <0.001 | 73.95 ± 11.28 | 73.91 ± 11.25 | 0.888 |
| Male gender | 6715 (52.55%) | 1044 (68.01%) | <0.001 | 960 (65.17%) | 986 (66.94%) | 0.331 |
| Monthly income, US dollars | ||||||
| <600 | 7865 (61.55%) | 923 (60.13%) | 0.004 | 903 (61.30%) | 890 (60.42%) | 0.304 |
| 600–1300 | 4484 (35.09%) | 581 (37.85%) | 530 (35.98%) | 554 (37.61%) | ||
| ≥1300 | 430 (3.36%) | 31 (2.02%) | 40 (2.72%) | 29 (1.97%) | ||
| Hospital location | ||||||
| Urban | 5276 (41.29%) | 604 (39.35%) | 0.005 | 559 (37.95%) | 579 (39.31%) | 0.696 |
| Suburban | 2947 (23.06%) | 320 (20.85%) | 311 (21.11%) | 312 (21.18%) | ||
| Rural | 4556 (35.65%) | 611 (39.80%) | 603 (40.94%) | 582 (39.51%) | ||
| Baseline comorbidities | ||||||
| Charlson comorbidity index | 2.17 ± 2.03 | 2.61 ± 2.06 | <0.001 | 2.59 ± 2.09 | 2.61 ± 2.08 | 0.736 |
| Myocardial infarction | 542 (4.24%) | 75 (4.89%) | 0.232 | 68 (4.62%) | 75 (5.09%) | 0.607 |
| Congestive heart failure | 1956 (15.31%) | 349 (22.74%) | <0.001 | 326 (22.13%) | 336 (22.81%) | 0.691 |
| Peripheral vascular disease | 244 (1.91%) | 25 (1.63%) | 0.487 | 29 (1.97%) | 25 (1.70%) | 0.681 |
| Cerebrovascular disease | 1382 (10.81%) | 276 (17.98%) | <0.001 | 246 (16.70%) | 256 (17.38%) | 0.659 |
| Dementia | 315 (2.46%) | 98 (6.38%) | <0.001 | 91 (6.18%) | 91 (6.18%) | 0.999 |
| Reumatologic disease | 243 (1.90%) | 18 (1.17%) | 0.043 | 16 (1.09%) | 18 (1.22%) | 0.863 |
| Peptic ulcer disease | 1791 (14.02%) | 273 (17.79%) | <0.001 | 265 (17.99%) | 259 (17.58%) | 0.81 |
| Hemiplegia or paraplegia | 117 (0.92%) | 26 (1.69%) | 0.006 | 16 (1.09%) | 26 (1.77%) | 0.161 |
| Diabetes | 4956 (38.78%) | 582 (37.92%) | 0.524 | 544 (36.93%) | 569 (38.63%) | 0.362 |
| Moderate or severe liver disease | 1036 (8.11%) | 98 (6.38%) | 0.019 | 89 (6.04%) | 94 (6.38%) | 0.76 |
| Chronic kidney disease | 4034 (31.57%) | 445 (28.99%) | 0.041 | 447 (30.35%) | 437 (29.67%) | 0.718 |
| Hypertension | 6630 (51.88%) | 950 (61.89%) | <0.001 | 889 (60.35%) | 911 (61.85%) | 0.427 |
| Dyslipidemia | 1765 (13.81%) | 167 (10.88%) | 0.001 | 185 (12.56%) | 164 (11.13%) | 0.254 |
| Medication for hypertension before index hospitalization | ||||||
| Alpha-blocker | 1326 (10.38%) | 206 (13.42%) | <0.001 | 201 (13.65%) | 201 (13.65%) | 0.999 |
| Beta-blocker | 4696 (36.75%) | 509 (33.16%) | 0.006 | 507 (34.42%) | 494 (33.54%) | 0.641 |
| CCB | 6807 (53.27%) | 946 (61.63%) | <0.001 | 881 (59.81%) | 903 (61.30%) | 0.429 |
| Diuretic | 6657 (52.09%) | 926 (60.33%) | <0.001 | 859 (58.32%) | 887 (60.22%) | 0.311 |
| ACEI or ARB | 5577 (43.64%) | 767 (49.97%) | <0.001 | 719 (48.81%) | 744 (50.51%) | 0.376 |
| Other medication | ||||||
| Aspirin | 1107 (8.66%) | 163 (10.62%) | 0.013 | 171 (11.61%) | 156 (10.59%) | 0.412 |
| Clopidogrel | 640 (5.01%) | 107 (6.97%) | 0.002 | 97 (6.59%) | 105 (7.13%) | 0.61 |
| Ticlopidine | 471 (3.69%) | 76 (4.95%) | 0.017 | 70 (4.75%) | 74 (5.02%) | 0.798 |
| Dipyridamole | 2851 (22.31%) | 357 (23.26%) | 0.4 | 358 (24.30%) | 348 (23.63%) | 0.698 |
| Nitrate | 93 (0.73%) | 22 (1.43%) | 0.006 | 19 (1.29%) | 19 (1.29%) | 0.999 |
| Statin | 2009 (15.72%) | 191 (12.44%) | 0.001 | 209 (14.19%) | 184 (12.49%) | 0.193 |
| NSAID | 6375 (49.89%) | 859 (55.96%) | <0.001 | 822 (55.80%) | 819 (55.60%) | 0.941 |
| PPI | 1214 (9.50%) | 201 (13.09%) | <0.001 | 165 (11.20%) | 191 (12.97%) | 0.158 |
| Index hospital comorbidity | ||||||
| Cardiovascular | 1148 (8.98%) | 150 (9.77%) | 0.301 | 153 (10.39%) | 142 (9.64%) | 0.539 |
| Respiratory | 2819 (22.06%) | 635 (41.37%) | <0.001 | 602 (40.87%) | 582 (39.51%) | 0.475 |
| Hepatic | 267 (2.09%) | 15 (0.98%) | 0.002 | 22 (1.49%) | 14 (0.95%) | 0.24 |
| Neurologic | 250 (1.96%) | 37 (2.41%) | 0.247 | 35 (2.38%) | 35 (2.38%) | 0.999 |
| Hematologic | 201 (1.57%) | 16 (1.04%) | 0.121 | 17 (1.15%) | 15 (1.02%) | 0.859 |
| Metabolic | 365 (2.86%) | 35 (2.28%) | 0.219 | 41 (2.78%) | 35 (2.38%) | 0.561 |
| ICU admission | 8492 (66.45%) | 1189 (77.46%) | <0.001 | 1141 (77.46%) | 1130 (76.71%) | 0.661 |
| Operation | 1314 (10.28%) | 151 (9.84%) | 0.624 | 136 (9.23%) | 139 (9.44%) | 0.899 |
| Renal function status at AKD periods (1 year after index hospitalization) | ||||||
| CKD | 4958 (38.80%) | 642 (41.82%) | 0.023 | 532 (36.12%) | 622 (42.23%) | 0.001 |
| Advanced CKD | 2410 (18.86%) | 206 (13.42%) | <0.001 | 199 (13.51%) | 201 (13.65%) | 0.957 |
| Events | Before Matching | After Matching | ||||
|---|---|---|---|---|---|---|
| Non-COPD (n = 12,779) | COPD (n = 1535) | p-Value | Non-COPD (n = 1473) | COPD (n = 1473) | p-Value | |
| All-cause death | 6931 (54.24%) | 1096 (71.40%) | <0.001 | 971 (65.92%) | 1050 (71.28%) | 0.002 |
| Stroke | 1044 (8.17%) | 172 (11.21%) | <0.001 | 121 (8.21%) | 170 (11.54%) | 0.003 |
| Ischemic stroke | 774 (6.06%) | 144 (9.38%) | <0.001 | 95 (6.45%) | 143 (9.71%) | 0.001 |
| Hemorrhagic stroke | 327 (2.56%) | 36 (2.35%) | 0.668 | 30 (2.04%) | 35 (2.38%) | 0.616 |
| CHF | 2541 (19.88%) | 458 (29.84%) | <0.001 | 296 (20.10%) | 448 (30.41%) | <0.001 |
| MACE * | 802 (6.28%) | 96 (6.25%) | 0.999 | 87 (5.91%) | 95 (6.45%) | 0.592 |
| ESRD | 3362 (26.31%) | 311 (20.26%) | <0.001 | 299 (20.30%) | 302 (20.50%) | 0.927 |
| COPD | Non-COPD | Crude | Adjusted † | Compete Risk †† | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Event | Person-Year | Incidence Rate (per 1000 Person-Years) | Event | Person-Year | Incidence Rate (per 1000 Person-Years) | HR (95%CI) | p Value | HR (95%CI) | p Value | sHR (95%CI) | p Value | |
| Before Propensity Score Matching | ||||||||||||
| All-cause death | 1096 | 4848.71 | 226.0 | 6931 | 57,368.8 | 120.8 | 1.55 [1.45,1.65] | <0.001 | 0.96 [0.90,1.04] | 0.323 | NA | NA |
| Stroke | 172 | 4368.39 | 39.4 | 1044 | 53,890 | 19.4 | 1.70 [1.45,2.00] | <0.001 | 1.27 [1.06,1.53] | 0.009 | 1.30 [1.07,1.56] | 0.007 |
| Ischemic stroke | 144 | 4413.14 | 32.6 | 774 | 54,369.5 | 14.2 | 1.88 [1.57,2.24] | <0.001 | 1.33 [1.09,1.63] | 0.006 | 1.37 [1.11,1.69] | 0.004 |
| Hemorrhagic stroke | 36 | 4783.3 | 7.5 | 327 | 56,658.6 | 5.8 | 1.18 [0.84,1.67] | 0.349 | 1.08 [0.74,1.57] | 0.691 | 1.05 [0.72,1.54] | 0.8 |
| CHF | 458 | 3769.6 | 121.5 | 2541 | 50,533.8 | 50.3 | 1.89 [1.71,2.09] | <0.001 | 1.37 [1.22,1.53] | <0.001 | 1.39 [1.24,1.56] | <0.001 |
| MACE | 127 | 4595.71 | 27.6 | 1127 | 54,737.5 | 20.6 | 1.20 [1.00,1.44] | 0.055 | 0.89 [0.73,1.09] | 0.270 | 0.89 [0.72,1.08] | 0.240 |
| ESRD | 311 | 4073.25 | 76.4 | 3362 | 45,620.2 | 73.7 | 0.81 [0.72,0.91] | <0.001 | 0.90 [0.80,1.02] | 0.102 | 0.91 [0.80,1.03] | 0.120 |
| After Propensity Score Matching | ||||||||||||
| All-cause death | 1050 | 4633.13 | 226.6 | 971 | 5159.11 | 188.2 | 1.08 [0.99,1.17] | 0.104 | 1.04 [0.96,1.14] | 0.331 | NA | NA |
| Stroke | 170 | 4156.28 | 40.9 | 121 | 4788.18 | 25.3 | 1.45 [1.14,1.83] | 0.002 | 1.42 [1.12,1.79] | 0.004 | 1.43 [1.13,1.81] | 0.003 |
| Ischemic stroke | 143 | 4201.03 | 34.0 | 95 | 4831.49 | 19.7 | 1.52 [1.17,1.97] | 0.002 | 1.48 [1.14,1.92] | 0.003 | 1.52 [1.17,1.97] | 0.002 |
| Hemorrhagic stroke | 35 | 4567.72 | 7.7 | 30 | 5107.35 | 5.9 | 1.26 [0.77,2.05] | 0.362 | 1.26 [0.77,2.05] | 0.361 | 1.19 [0.73,1.96] | 0.480 |
| CHF | 448 | 3583.99 | 125.0 | 296 | 4547.46 | 65.1 | 1.62 [1.40,1.88] | <0.001 | 1.59 [1.37,1.84] | <0.001 | 1.61 [1.39,1.86] | <0.001 |
| MACE * | 126 | 4391.31 | 28.7 | 116 | 4871.23 | 23.8 | 1.13 [0.87,1.45] | 0.357 | 1.12 [0.87,1.44] | 0.396 | 1.09 [0.84,1.40] | 0.520 |
| ESRD | 302 | 3870.54 | 78.0 | 299 | 4367.31 | 68.5 | 0.97 [0.83,1.14] | 0.695 | 0.96 [0.81,1.12] | 0.579 | 0.95 [0.81,1.12] | 0.550 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-H.; Chang, H.-M.; Wang, C.-Y.; Chen, L.; Chen, L.-W.; Lai, C.-H.; Kuo, S.-W.; Wang, H.-C.; Wu, V.-C.; The National Taiwan University Study Group on Acute Renal Failure. Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort. J. Clin. Med. 2018, 7, 237. https://doi.org/10.3390/jcm7090237
Wu C-H, Chang H-M, Wang C-Y, Chen L, Chen L-W, Lai C-H, Kuo S-W, Wang H-C, Wu V-C, The National Taiwan University Study Group on Acute Renal Failure. Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort. Journal of Clinical Medicine. 2018; 7(9):237. https://doi.org/10.3390/jcm7090237
Chicago/Turabian StyleWu, Che-Hsiung, Huang-Ming Chang, Cheng-Yi Wang, Likwang Chen, Liang-Wen Chen, Chien-Heng Lai, Shuenn-Wen Kuo, Hao-Chien Wang, Vin-Cent Wu, and The National Taiwan University Study Group on Acute Renal Failure. 2018. "Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort" Journal of Clinical Medicine 7, no. 9: 237. https://doi.org/10.3390/jcm7090237
APA StyleWu, C. -H., Chang, H. -M., Wang, C. -Y., Chen, L., Chen, L. -W., Lai, C. -H., Kuo, S. -W., Wang, H. -C., Wu, V. -C., & The National Taiwan University Study Group on Acute Renal Failure. (2018). Long-Term Outcomes in Patients with Incident Chronic Obstructive Pulmonary Disease after Acute Kidney Injury: A Competing-Risk Analysis of a Nationwide Cohort. Journal of Clinical Medicine, 7(9), 237. https://doi.org/10.3390/jcm7090237