An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Setting
2.2. Constructing Training Data Set
2.3. Data Description
2.4. Algorithm and Training
2.5. Statistical Analyses
3. Results
3.1. Demographic Features of Patients
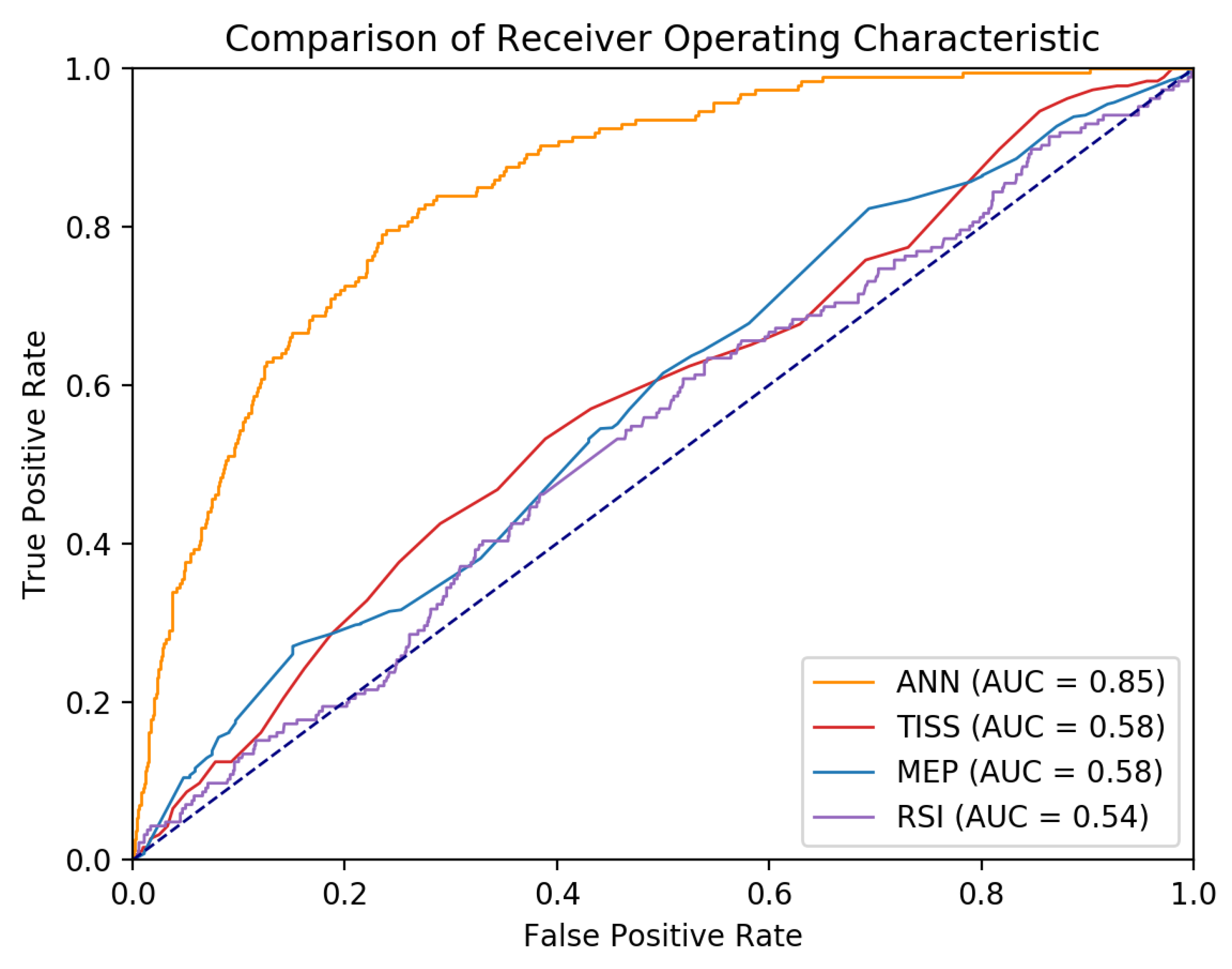
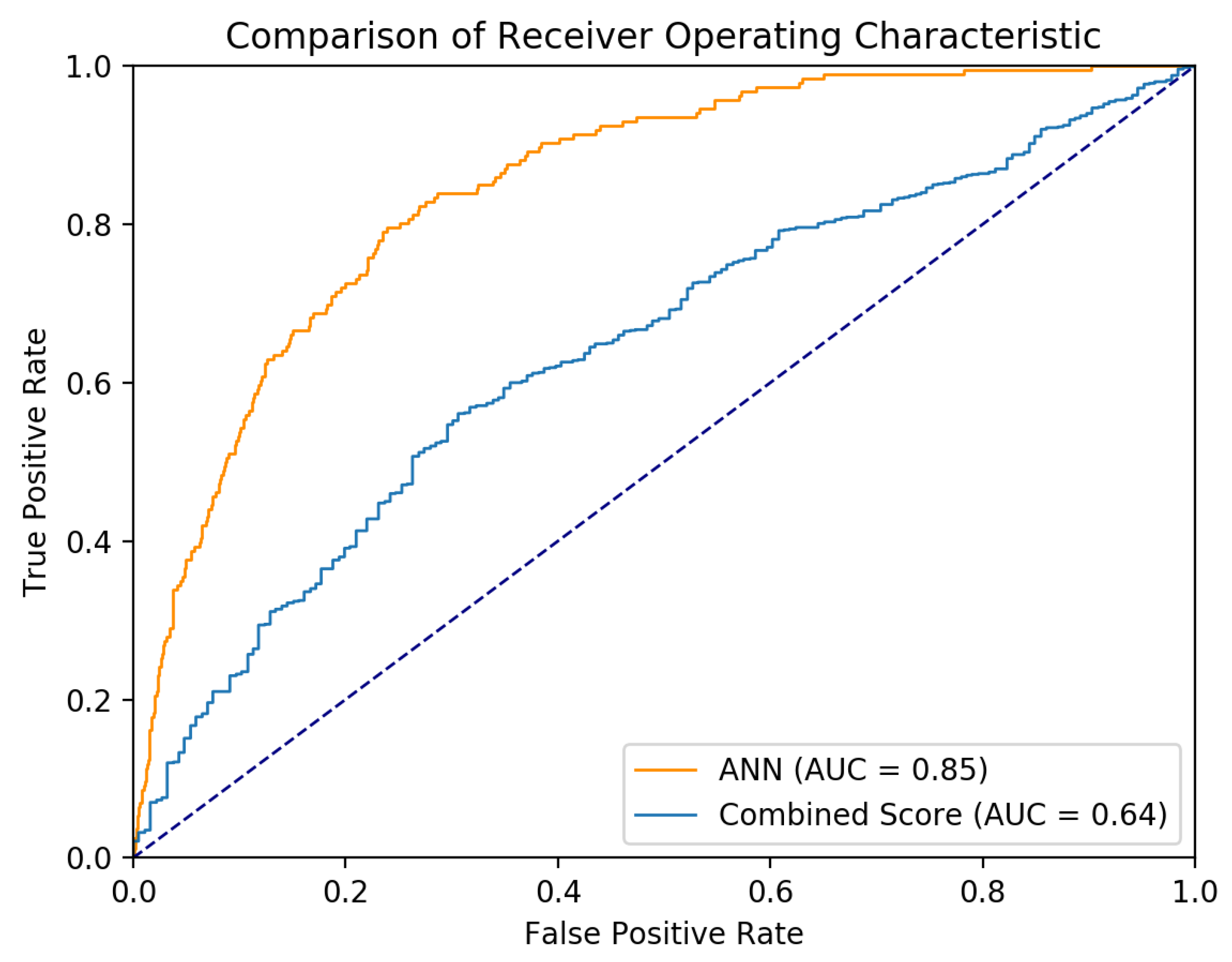
3.2. Results of Artificial Neural Networks (ANN)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lapinsky, S.E. Endotracheal intubation in the ICU. Crit. Car. 2015, 19, 258. [Google Scholar] [CrossRef] [PubMed]
- Hill, A.D.; Fowler, R.A.; Burns, K.E.; Rose, L.; Pinto, R.L.; Scales, D.C. Long-term outcomes and health care utilization after prolonged mechanical ventilation. Ann. Am. Thorac. Soc. 2017, 14, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Haas, C.F.; Loik, P.S. Ventilator discontinuation protocols. Respir. Car. 2012, 57, 1649–1662. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Giehler, K.; Walters, R.W.; Meyerink, K.; Modrykamien, A.M. The effect of a mechanical ventilation discontinuation protocol in patients with simple and difficult weaning: Impact on clinical outcomes. Respir. Car. 2014, 59, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Nemer, S.N.; Barbas, C.S. Predictive parameters for weaning from mechanical ventilation. J. Bras. Pneumol. 2011, 37, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Perren, A.; Previsdomini, M.; Llamas, M.; Cerutti, B.; Györik, S.; Merlani, G.; Jolliet, P. Patients’ prediction of extubation success. Intensive Car. Med. 2010, 36, 2045–2052. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.C.; Chen, C.M.; Chiang, S.R.; Liu, W.L.; Weng, S.F.; Sung, M.I.; Hsing, S.C.; Cheng, K.C. Establishing predictors for successfully planned endotracheal extubation. Medicine 2016, 95, 48–53. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef] [PubMed]
- Kingma, D.; Adam, J.B. A method for stochastic optimization. In Proceedings of the International Conference on Learning Representations (ICLR), San Diego, CA, USA, 30 January 2015. [Google Scholar]
- DiRusso, S.M.; Sullivan, T.; Holly, C.; Cuff, S.N.; Savino, J. An artificial neural network as a model for prediction of survival in trauma patients: Validation for a regional trauma area. J Trauma 2000, 49, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.J.; Chiu, H.W.; Lee, C.N.; Chen, T.T.; Chang, C.C.; Bien, M.Y. Improvement in the prediction of ventilator weaning outcomes by an artificial neural network in a medical ICU. Respir. Car. 2015, 60, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.; Almeida, J.S.; Stanislaus, R.; Wagner, C.L. Can machine learning methods predict extubation outcome in premature infants as well as clinicians? J. Neonatal Biol. 2013, 2, 100–118. [Google Scholar]
- Cheng, A.C.; Cheng, K.C.; Chen, C.M.; Hsing, S.C.; Sung, M.Y. The outcome and predictors of failed extubation in intensive care patients—the elderly is an important predictor. Int. J. Gerontol. 2011, 5, 206–211. [Google Scholar] [CrossRef]
- Smina, M.; Salam, A.; Khamiees, M.; Gada, P.; Amoateng-Adjepong, Y.; Manthous, C.A. Cough peak flows and extubation outcomes. Chest 2003, 12 4, 262–268. [Google Scholar] [CrossRef]
- Klambauer, G.; Unterthiner, T.; Mayr, A.; Hochreiter, S. Self-normalizing neural networks. Adv. Neural Inf. Process. Syst. 2017, 971–980. [Google Scholar]
- Béduneau, G.; Pham, T.; Schortgen, F.; Piquilloud, L.; Zogheib, E.; Jonas, M.; Grelon, F.; Runge, I.; Terzi, N.; Grange, S.; et al. Epidemiology of Weaning Outcome According to a New Definition. The WIND Study. Am. J. Respir. Crit. Car. Med. 2017, 195, 772–783. [Google Scholar] [CrossRef] [PubMed]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Vieillard-Baron, A. Weaning from mechanical ventilation. Eur. Respir. J. 2017, 29, 1033–1056. [Google Scholar] [CrossRef] [PubMed]
- Avati, A.; Jung, K.; Harman, S.; Downing, L.; Ng, A.; Shah, N.H. Improving palliative care with deep learning. In Proceedings of the IEEE International Conference on Bioinformatics and Biomedicine, Stanford, CA, USA, 17 November 2017. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Machine. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Python 3.6.5. Available online: https://www.python.org/downloads/release/python-365/ (accessed on 24 August 2018).
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res 2011, 12, 2825–2830. [Google Scholar]
- Abadi, M.; Barham, P.; Chen, J.; Chen, Z.; Davis, A.; Dean, J.; Devin, M.; Ghemawat, S.; Irving, G.; Isard, M.; et al. TensorFlow: A System for Large-Scale Machine Learning. OSDI 2016, 16, 264–283. [Google Scholar]
- He, H.; Garcia, E.A. Learning from imbalanced data. IEEE Trans. Knowl. data eng. 2009, 21, 1263–1284. [Google Scholar]
- Powers, D.M. Evaluation: From precision, recall and f measure to roc, informedness, markedness, and correlation. J. Mach Learn. Technol. 2011, 2, 37–63. [Google Scholar]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [PubMed]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 837–845. [Google Scholar] [CrossRef]
- Meade, M.; Guyatt, G.; Cook, D.; Griffith, L.; Sinuff, T.; Kergl, C.; Mancebo, J.; Esteban, A.; Epstein, S. Predicting success in weaning from mechanical ventilation. Chest 2001, 120, 400s–424s. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.L.; Tobin, M.J. A prospective study of indexes predicting the outcome of trials of weaning from mechanical ventilation. N. Engl. J. Med. 1991, 324, 1445–1450. [Google Scholar] [CrossRef] [PubMed]
- Nemer, S.N.; Barbas, C.S.; Caldeira, J.B.; Guimarães, B.; Azeredo, L.M.; Gago, R.; Souza, P.C.P. Evaluation of maximal inspiratory pressure, tracheal airway occlusion pressure, and its ratio in the weaning outcome. J. Crit. Car. 2009, 24, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Conti, G.; Montini, L.; Pennisi, M.A.; Cavaliere, F.; Arcangeli, A.; Bocci, M.G.; Proietti, R.; Antonelli, M.A. prospective, blinded evaluation of indexes proposed to predict weaning from mechanical ventilation. Intensive Car. Med. 2004, 30, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.M.; Chan, K.S.; Fong, Y.; Hsing, S.C.; Cheng, A.C.; Sung, M.Y.; Su, M.Y.; Cheng, K.C. Age is an important predictor of failed unplanned extubation. Int. J. Gerontol. 2010, 4, 120–129. [Google Scholar] [CrossRef]
- Scheinhorn, D.J.; Hassenpflug, M.; Artinian, B.M.; LaBree, L.; Catlin, J.L. Predictors of weaning after 6 weeks of mechanical ventilation. Chest 1995, 107, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Nava, S.; Zanotti, E.; Rubini, F. Weaning and outcome from mechanical ventilation. Mon. Arch. Chest. Dis. 1994, 49, 530–532. [Google Scholar]
- Thille, A.W.; Boissier, F.; Ben-Ghezala, H.; Razazi, K.; Mekontso-Dessap, A.; Brun-Buisson, C.; Brochard, L. Easily identified at-risk patients for extubation failure may benefit from noninvasive ventilation: A prospective before-after study. Crit. Car. 2016, 20, 48. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Successful Extubation | Failed Extubation | p |
|---|---|---|---|
| n = 3417 (94.9%) | n = 185 (5.1%) | ||
| Age (years) | 63.9 ± 16.5 | 68.1 ± 14.6 | <0.001 |
| Male | 1729 (50.6%) | 106 (57.3%) | 0.426 |
| BMI (kg/m2) | 23.7 ± 4.5 | 23.2 ± 4.5 | 0.144 |
| APACHE II | 16.2 ± 7.4 | 18.9 ± 7.0 | <0.001 |
| TISS Scale | 27.1 ± 7.8 | 29.3 ± 7.5 | <0.001 |
| Glasgow coma scale | 12.1 ± 3.5 | 11.1 ± 3.8 | 0.001 |
| Comorbidities | |||
| Cardiovascular accident | 635 (18.6%) | 45 (24.3%) | 0.052 |
| Chronic lung disease | 264 (7.7%) | 21 (11.4%) | 0.075 |
| Chronic hemodialysis | 314 (9.2%) | 105 (56.8%) | <0.001 |
| Chronic liver disease | 76 (2.2%) | 3 (1.6%) | 0.586 |
| Diabetes | 999 (29.2%) | 71 (38.4%) | 0.008 |
| Old stroke | 866 (25.3%) | 56 (30.3%) | 0.135 |
| Active cancer | 755 (22.1%) | 28 (15.1%) | 0.025 |
| Pre-extubation data | |||
| FiO2 | 27.4 ± 3.5 | 28.0 ± 3.7 | 0.029 |
| Pressure support level | 9.2 ± 1.5 | 9.2 ± 1.6 | 0.840 |
| PEEP | 5.1 ± 0.5 | 5.2 ± 0.6 | 0.028 |
| Minute ventilation | 7.8 ± 2.6 | 7.5 ± 2.4 | 0.075 |
| Pulse rate | 86.6 ± 16.2 | 87.9 ± 17.3 | 0.236 |
| Mean arterial pressure | 96.5 ± 16.2 | 94.7 ± 18.1 | 0.184 |
| Respiratory rate | 16.7 ± 5.1 | 18.0 ± 5.3 | 0.001 |
| pH | 7.441 ± 0.054 | 7.446 ± 0.051 | 0.279 |
| PaCO2 | 37.6 ± 6.2 | 38.5 ± 6.0 | 0.057 |
| PaO2 | 105.9 ± 41.6 | 94.9 ± 27.4 | <0.001 |
| PaO2/FiO2 | 361.0 ± 101.0 | 329.3 ± 94.1 | <0.001 |
| Hemoglobin | 11.3 ± 1.9 | 10.7 ± 1.8 | <0.001 |
| Hematocrit (%) | 34.2 ± 6.7 | 32.4 ± 6.7 | 0.001 |
| Blood urea nitrogen | 25.1 ± 21.3 | 32.9 ± 31.8 | 0.002 |
| Creatinine | 1.7 ± 2.1 | 1.9 ± 2.1 | 0.200 |
| Sodium | 139.1 ± 4.6 | 138.8 ± 5.1 | 0.370 |
| Potassium | 3.8 ± 0.5 | 3.9 ± 0.5 | 0.398 |
| Calcium | 7.9 ± 0.9 | 8.0 ± 0.9 | 0.598 |
| Phosphate | 3.4 ± 1.5 | 3.3 ± 1.7 | 0.812 |
| Albumin | 2.8 ± 0.6 | 2.7 ± 0.6 | 0.074 |
| Weaning parameters | |||
| RSI | 52.8 ± 29.9 | 62.8 ± 33.2 | <0.001 |
| MIP | 37.9 ± 14.1 | 34.9 ± 13.0 | 0.008 |
| MEP | 61.0 ± 29.4 | 52.6 ± 26.7 | <0.001 |
| Ventilator use duration (h) | 106.0 ± 126.9 | 140.8 ± 145.8 | 0.002 |
| Variable | OR | 95% CI | P * | OR | 95% CI | P ** |
|---|---|---|---|---|---|---|
| Age (years) | 1.107 | 1.007–1.027 | 0.001 | |||
| APACHE II | 1.046 | 1.027–1.066 | <0.001 | |||
| TISS Scale | 1.036 | 1.017–1.055 | <0.001 | 1.814 # | 1.283–2.563 | 0.001 |
| Glasgow coma scale | 0.930 | 0.894–0.967 | <0.001 | |||
| Comorbidities | ||||||
| Chronic hemodialysis | 12.970 | 9.483–17.740 | <0.001 | 12.264 | 8.556–17.580 | <0.001 |
| Diabetes | 1.507 | 1.110–2.045 | 0.008 | |||
| Active cancer | 0.629 | 0.417–0.948 | 0.027 | |||
| Ventilator use duration (h) | 1.002 | 1.001–1.003 | <0.001 | |||
| Weaning parameter | ||||||
| RSI | 1.008 | 1.004–1.012 | <0.001 | 2.003 % | 1.378–2.910 | <0.001 |
| MIP | 0.983 | 0.970–0.995 | 0.008 | |||
| MEP | 0.989 | 0.983–0.995 | <0.001 | 0.610 @ | 0.413–0.899 | 0.013 |
| Pre-extubation data | ||||||
| Pulse rate | 1.014 | 1.005–1.023 | 0.003 | 1.705 * | 1.173–2.480 | 0.005 |
| PaO2/FiO2 | 0.997 | 0.995–0.998 | <0.001 | 0.529 & | 0.373–0.750 | <0.001 |
| Hemoglobin | 0.832 | 0.765–0.904 | <0.001 | |||
| Hematocrit (%) | 0.961 | 0.939–0.984 | 0.001 | |||
| BUN | 1.012 | 1.007–1.017 | <0.001 | |||
| Test Set (n = 37) | All Patients (n = 307) | |
|---|---|---|
| F1 | 0.871 | 0.867 |
| Precision | 0.957 | 0.939 |
| Recall | 0.808 | 0.822 |
| Variable | Weighting |
|---|---|
| Age (years) | −0.474 |
| APACHE II | −0.75 |
| TISS Scale | −0.286 |
| Glasgow coma scale | 0.566 |
| Comorbidities | |
| Chronic hemodialysis | −0.289 |
| Diabetes | −0.022 |
| Active cancer | 0.027 |
| Ventilator use duration (h) | −0.611 |
| Weaning parameter | |
| RSI | −0.005 |
| MIP | 0.238 |
| MEP | 0.353 |
| Pre-extubation data | |
| Pulse rate | 0.066 |
| PaO2/FiO2 | 0.097 |
| Hemoglobin | 0.692 |
| Hematocrit (%) | 0.643 |
| BUN | −0.033 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, M.-H.; Hsieh, M.-J.; Chen, C.-M.; Hsieh, C.-C.; Chao, C.-M.; Lai, C.-C. An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units. J. Clin. Med. 2018, 7, 240. https://doi.org/10.3390/jcm7090240
Hsieh M-H, Hsieh M-J, Chen C-M, Hsieh C-C, Chao C-M, Lai C-C. An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units. Journal of Clinical Medicine. 2018; 7(9):240. https://doi.org/10.3390/jcm7090240
Chicago/Turabian StyleHsieh, Meng-Hsuen, Meng-Ju Hsieh, Chin-Ming Chen, Chia-Chang Hsieh, Chien-Ming Chao, and Chih-Cheng Lai. 2018. "An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units" Journal of Clinical Medicine 7, no. 9: 240. https://doi.org/10.3390/jcm7090240
APA StyleHsieh, M. -H., Hsieh, M. -J., Chen, C. -M., Hsieh, C. -C., Chao, C. -M., & Lai, C. -C. (2018). An Artificial Neural Network Model for Predicting Successful Extubation in Intensive Care Units. Journal of Clinical Medicine, 7(9), 240. https://doi.org/10.3390/jcm7090240