Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study

 ,
, 
Abstract
:1. Introduction
2. Patients and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Naci, H.; Brugts, J.J.; Fleurence, R.; Tsoi, B.; Toor, H.; Ades, A.E. Comparative benefits of statins in the primary and secondary prevention of major coronary events and all-cause mortality: A network meta-analysis of placebo-controlled and active-comparator trials. Eur. J. Prev. Cardiol. 2013, 20, 641–657. [Google Scholar] [CrossRef] [PubMed]
- Navarese, E.P.; Robinson, J.G.; Kowalewski, M.; Kolodziejczak, M.; Andreotti, F.; Bliden, K.; Tantry, U.; Kubica, J.; Raggi, P.; Gurbel, P.A. Association between baseline LDL-C level and total and cardiovascular mortality after LDL-C lowering: A systematic review and meta-analysis. JAMA 2018, 319, 1566–1579. [Google Scholar] [CrossRef] [PubMed]
- Perler, B.A. The effect of statin medications on perioperative and long-term outcomes following carotid endarterectomy or stenting. Semin. Vasc. Surg. 2007, 20, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Wang, B.; Zhan, B.; Li, Q.; Li, Y.; Zhu, Z.; Yan, Z. Statin therapy improved long-term prognosis in patients with major non-cardiac vascular surgeries: A systematic review and meta-analysis. Vascul. Pharmacol. 2018, 109, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Verzini, F.; De Rango, P.; Parlani, G.; Giordano, G.; Caso, V.; Cieri, E.; Isernia, G.; Cao, P. Effects of statins on early and late results of carotid stenting. J. Vasc. Surg. 2011, 53, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Rizwan, M.; Faateh, M.; Aridi, H.D.; Nejim, B.; Alshwaily, W.; Malas, M.B. Statins reduce mortality and failure to rescue after carotid artery stenting. J. Vasc. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Rosenfield, K.; Matsumura, J.S.; Chaturvedi, S.; Riles, T.; Ansel, G.M.; Metzger, D.C.; Wechsler, L.; Jaff, M.R.; Gray, W. Randomized trial of stent versus surgery for asymptomatic carotid stenosis. N. Engl. J. Med. 2016, 374, 1011–1120. [Google Scholar] [CrossRef] [PubMed]
- Sardar, P.; Chatterjee, S.; Aronow, H.D.; Kundu, A.; Ramchand, P.; Mukherjee, D.; Nairooz, R.; Gray, W.A.; White, C.J.; Jaff, M.R.; et al. Carotid artery stenting versus endarterectomy for stroke prevention: A meta-analysis of clinical trials. J. Am. Coll. Cardiol. 2017, 69, 2266–2275. [Google Scholar] [CrossRef] [PubMed]
- Antoniou, G.A.; Georgiadis, G.S.; Georgakarakos, E.I.; Antoniou, S.A.; Bessias, N.; Smyth, J.V.; Murray, D.; Lazarides, M.K. Meta-analysis and meta-regression analysis of outcomes of carotid endarterectomy and stenting in the elderly. JAMA Surg. 2013, 148, 1140–1152. [Google Scholar] [CrossRef] [PubMed]
- Gröschel, K.; Ernemann, U.; Schulz, J.B.; Nägele, T.; Terborg, C.; Kastrup, A. Statin therapy at carotid angioplasty and stent placement: Effect on procedure-related stroke, myocardial infarction, and death. Radiology 2006, 240, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Reiff, T.; Amiri, H.; Rohde, S.; Hacke, W.; Ringleb, P.A. Statins reduce peri-procedural complications in carotid stenting. Eur. J. Vasc. Endovasc. Surg. 2014, 48, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.H.; Sohn, S.I.; Kwak, J.; Yoo, J.; Chang, H.W.; Kwon, O.K.; Jung, C.; Chung, I.; Bae, H.J.; Lee, J.S.; et al. Dose-dependent effect of statin pretreatment on preventing the periprocedural complications of carotid artery stenting. Stroke 2017, 48, 1890–1894. [Google Scholar] [CrossRef] [PubMed]
- Texakalidis, P.; Giannopoulos, S.; Jonnalagadda, A.K.; Chitale, R.V.; Jabbour, P.; Armstrong, E.J.; Schwartz, G.G.; Kokkinidis, D.G. Preoperative use of statins in carotid artery stenting: A systematic review and meta-analysis. J. Endovasc. Ther. 2018, 25, 624–631. [Google Scholar] [PubMed]
- Fleisher, L.A.; Beckman, J.A.; Brown, K.A.; Calkins, H.; Chaikof, E.L.; Fleischmann, K.E.; Freeman, W.K.; Froehlich, J.B.; Kasper, E.K.; Kersten, J.R.; et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for Noncardiac Surgery: A report of the American College of Cardiology/American Heart Association Task force on practice guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery). Circulation 2007, 116, e418–e500. [Google Scholar] [PubMed]
- Staikov, I.N.; Nedeltchev, K.; Arnold, M.; Remonda, L.; Schroth, G.; Sturzenegger, M.; Herrmann, C.; Rivoir, A.; Mattle, H.P. Duplex sonographic criteria for measuring carotid stenoses. J. Clin. Ultrasound. 2002, 30, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Leffondré, K.; Touraine, C.; Helmer, C.; Joly, P. Interval-censored time-to-event and competing risk with death: Is the illness-death model more accurate than the Cox model? Int. J. Epidemiol. 2013, 42, 1177–1186. [Google Scholar] [CrossRef] [PubMed]
- De Wreede, L.; Fiocco, M.; Putter, H. Mstate: An R package for the analysis of competing risks and multi-state models. J. Stat. Softw. Artic. 2011, 38, 1–30. [Google Scholar] [CrossRef]
- Levin, A.; Stevens, P.E.; Bilous, R.W.; Coresh, J.; De Francisco, A.L.M.; De Jong, P.E.; Griffith, K.E.; Hemmelgarn, B.R.; Iseki, K.; Lamb, E.J.; et al. Kidney disease: Improving global outcomes (KDIGO) CKD work group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- R Development Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Austria, 2008. Available online: http://www.R-project.org (accessed on 23 April 2018).
- Chan, A.W.; Bhatt, D.L.; Chew, D.P.; Quinn, M.J.; Moliterno, D.J.; Topol, E.J.; Ellis, S.G. Early and sustained survival benefit associated with statin therapy at the time of percutaneous coronary intervention. Circulation 2002, 105, 691–696. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.; Quan, H.; Buchan, A.M.; Ghali, W.A.; Feasby, T.E. Statins are associated with better outcomes after carotid endarterectomy in symptomatic patients. Stroke 2005, 36, 2072–2076. [Google Scholar] [CrossRef] [PubMed]
- Badimon, J.J.; Ortiz, A.F.; Meyer, B.; Mailhac, A.; Fallon, J.T.; Falk, E.; Badimon, L.; Chesebro, J.H.; Fuster, V. Different response to balloon angioplasty of carotid and coronary arteries: Effects on acute platelet deposition and intimal thickening. Atherosclerosis 1998, 140, 307–314. [Google Scholar] [CrossRef]
- Brott, T.G.; Hobson, R.W.; Howard, G.; Roubin, G.S.; Clark, W.M.; Brooks, W.; Mackey, A.; Hill, M.D.; Leimgruber, P.P.; Sheffet, A.J.; et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N. Engl. J. Med. 2010, 363, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Voeks, J.H.; Howard, G.; Roubin, G.; Farb, R.; Heck, D.; Logan, W.; Longbottom, M.; Sheffet, A.; Meschia, J.F.; Brott, T.G. Mediators of the age effect in the carotid revascularization endarterectomy versus stenting trial (CREST). Stroke 2015, 46, 2868–2873. [Google Scholar] [CrossRef] [PubMed]
- Langhoff, R. Carotid stenosis-basing treatment on individual patients’ needs. Optimal medical therapy alone or accompanied by stenting or endarterectomy. Vasa 2018, 47, 7–16. [Google Scholar] [CrossRef] [PubMed]
- De Carlo, M.; Cortese, B.; Pennesi, M.; Misuraca, L.; Conte, L.; Pitì, A.; Petronio, A.S.; Balbarini, A. Design of the rosuvastatin pretreatment to reduce embolization during carotid artery stenting trial. J. Cardiovasc. Med. 2014, 15, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Catena, C.; Colussi, G.; Brosolo, G.; Sechi, L.A. A prothrombotic state is associated with early arterial damage in hypertensive patients. J. Atheroscler. Thromb. 2012, 19, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Catena, C.; Novello, M.; Lapenna, R.; Baroselli, S.; Colussi, G.; Nadalini, E.; Favret, G.; Cavarape, A.; Soardo, G.; Sechi, L.A. New risk factors for atherosclerosis in hypertension: Focus on the prothrombotic state and lipoprotein(a). J. Hypertens. 2005, 23, 1617–1631. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Catena, C.; Ray, K.K.; Vallejo-Vaz, A.J.; Reiner, Ž.; Sechi, L.A.; Colussi, G. Impact of statin therapy on plasma levels of plasminogen activator inhibitor-1: A systematic review and meta-analysis of randomised controlled trials. Thromb. Haemost. 2016, 116, 162–171. [Google Scholar] [CrossRef] [PubMed]
- Tadros, R.O.; Vouyouka, A.G.; Chung, C.; Malik, R.K.; Krishnan, P.; Ellozy, S.H.; Marin, M.L.; Faries, P.L. The effect of statin use on embolic potential during carotid angioplasty and stenting. Ann. Vasc. Surg. 2013, 27, 96–103. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 171) | Censored (n = 96) | Died (n = 75) | −MACE (n = 112) | +MACE (n = 59) | −Statins (n = 58) | +Statins (n = 113) |
|---|---|---|---|---|---|---|---|
| Enrolment age (years) | 72 ± 8 | 70 ± 8 | 74 ± 9 *** | 72 ± 9 | 72 ± 8 | 75 ± 8 | 70 ± 8 *** |
| Male sex (n (%)) | 125 (73) | 70 (73) | 55 (73) | 86 (77) | 39 (66) | 43 (77) | 82 (71) |
| Smoke history (n (%)) | 115 (67) | 62 (64) | 53 (71) | 76 (68) | 39 (66) | 44 (76) | 71 (63) |
| BMI (Kg/m2) | 26.4 ± 3.8 | 26.3 ± 3.6 | 26.5 ± 4.1 | 26.2 ± 3.7 | 26.7 ± 4.0 | 25.8 ± 4.0 | 26.7 ± 3.7 |
| SBP (mmHg) | 159 ± 25 | 159 ± 23 | 159 ± 28 | 158 ± 24 | 161 ± 27 | 160 ± 28 | 158 ± 24 |
| DBP (mmHg) | 84 ± 13 | 82 ± 10 | 86 ± 17 | 84 ± 14 | 84 ± 12 | 85 ± 18 | 83 ± 11 |
| eGFR (mL/min/1.73 m2) | 67 ± 23 | 70 ± 21 | 64 ± 25 | 67 ± 23 | 67 ± 23 | 62 ± 22 | 70 ± 23 * |
| Hypertension (n (%)) | 146 (85) | 77 (80) | 69 (92) | 96 (86) | 50 (85) | 46 (79) | 100 (88) |
| Diabetes (n (%)) | 79 (46) | 33 (34) | 46 (61) *** | 53 (47) | 26 (44) | 25 (43) | 54 (48) |
| Dyslipidemia (n (%)) | 121 (71) | 73 (76) | 48 (64) | 80 (71) | 41 (69) | 13 (22) | 108 (96) *** |
| Atrial fibrillation (n (%)) | 16 (9) | 4 (4) | 12 (16) * | 11 (10) | 5 (8) | 6 (10) | 10 (9) |
| IHD (n (%)) | 61 (36) | 34 (35) | 27 (36) | 37 (33) | 24 (41) | 12 (21) | 49 (43) *** |
| Peripheral artery disease (n (%)) | 57 (33) | 29 (30) | 28 (37) | 38 (34) | 19 (32) | 17 (29) | 40 (35) |
| Carotid restenosis (n (%)) | 12 (7) | 6 (6) | 6 (8) | 6 (5) | 6 (10) | 4 (7) | 8 (7) |
| Preexistent MACE (n (%)) | 116 (68) | 65 (68) | 51 (68) | 75 (67) | 41 (69) | 34 (59) | 82 (73) |
| Statins users (n (%)) | 113 (66) | 76 (79) | 37 (49) *** | 79 (70) | 34 (58) | 0 (0) | 115 (100) |
| Antiplatelet users (n (%)) | 156 (91) | 89 (93) | 67 (89) | 103 (92) | 53 (90) | 54 (93) | 102 (90) |
| Follow-up (months) | 87 ± 45 | 101 ± 44 | 69 ± 39 *** | 86 ± 45 | 87 ± 45 | 74 ± 45 | 93 ± 43 ** |
| New MACE (n (%)) | 59 (34) | 35 (36) | 24 (32) | 0 (0) | 59 (100) | 25 (43) | 34 (30) |
| Time to new MACE (months) | 68 ± 50 | 78 ± 54 | 55 ± 42 ** | 86 ± 45 | 35 ± 42 *** | 51 ± 47 | 77 ± 50 ** |
| MACE within 1 month (n (%)) | 14 (8.2) | 5 (5) | 9 (12) | - | 14 (100) | 8 (14) | 6 (5) |
| Deaths (n (%)) | 75 (44) | 0 (0) | 75 (100) | 51 (45) | 24 (41) | 38 (65) | 37 (33) *** |
| Time to death (months) | 69 ± 39 | - | 69 ± 39 | 86 ± 45 | 89 ± 45 | 74 ± 45 | 93 ± 43 ** |
| Variable | HR 95% CI | p |
|---|---|---|
| Enrolment age (years) | 1.08 (1.04–1.13) | <0.001 |
| Male sex (no/yes) | 1.34 (0.70–2.55) | NS |
| Smoke history (no/yes) | 0.77 (0.41–1.46) | NS |
| BMI (Kg/m2) | 0.99 (0.91–1.09) | NS |
| eGFR (mL/min/1.73 m2) | 1.00 (0.99–1.02) | NS |
| Hypertension (no/yes) | 2.00 (0.83–4.81) | NS |
| Diabetes (no/yes) | 2.45 (1.49–4.04) | <0.001 |
| Preexistent MACE (no/yes) | 0.96 (0.54–1.71) | NS |
| Statins users (no/yes) | 0.56 (0.33–0.94) | 0.028 |
| Antiplatelet users (no/yes) | 1.20 (0.57–2.55) | NS |
| Time to new MACE (months) | 0.987 (0.981–0.992) | <0.001 |
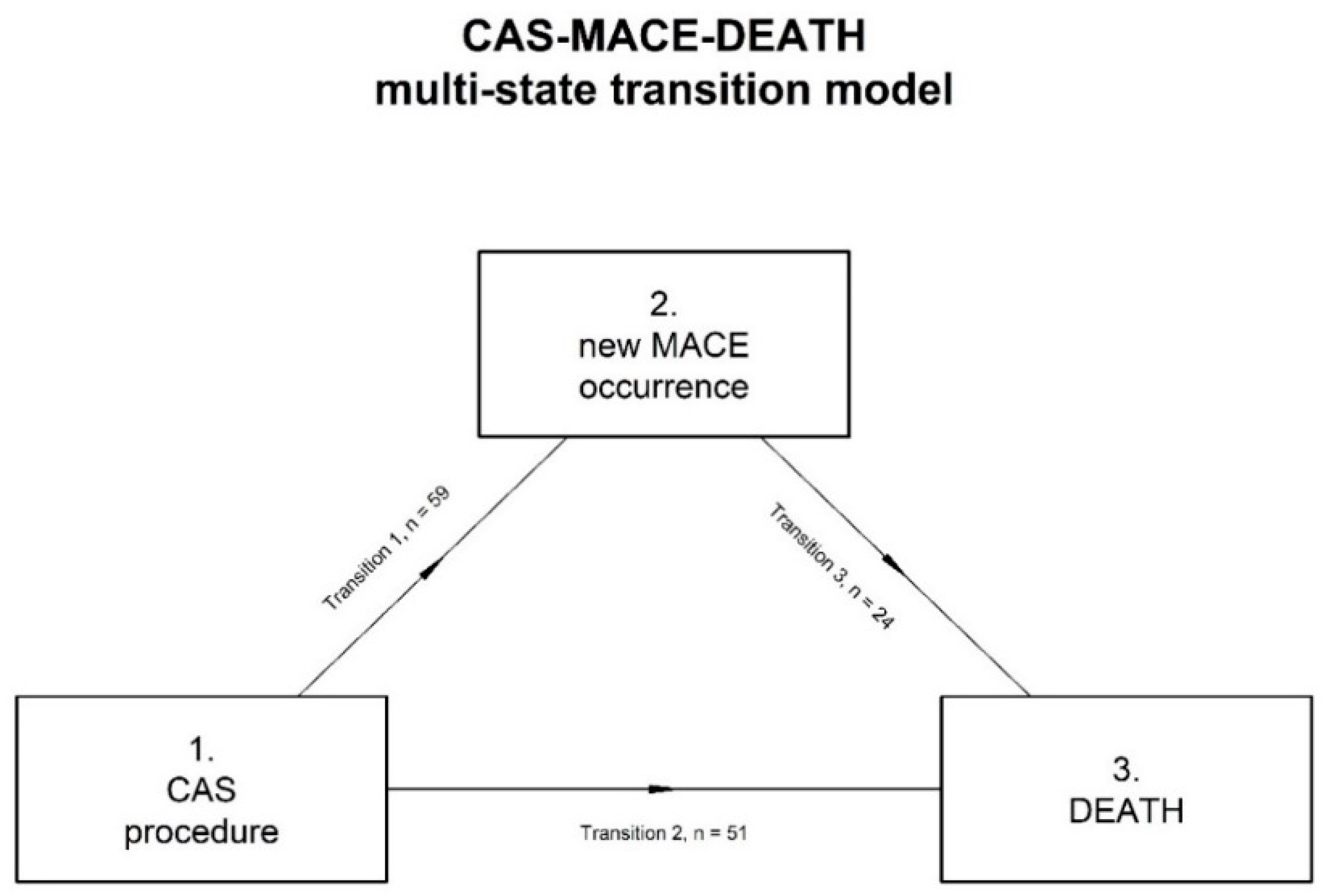
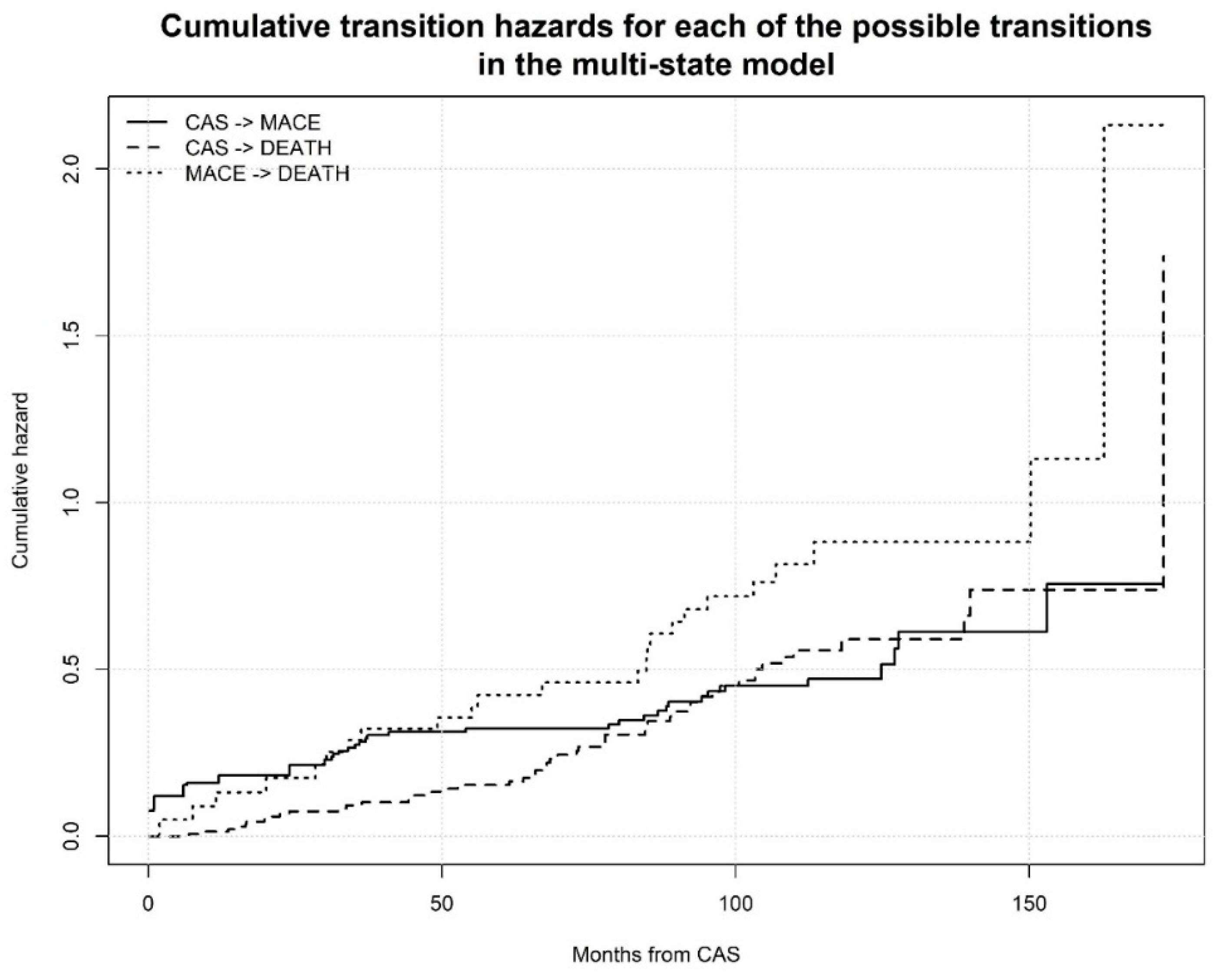
| Variable | Transition 1 CAS to MACE (n = 59) | Transition 2 CAS to DEATH (n = 51) | Transition 3 MACE to DEATH (n = 24) | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | ||
| Enrolment age (years) | <65 | Ref. | Ref. | Ref. | |||
| 65–75 | 1.43 (0.64–3.20) | NS | 2.23 (0.68–7.27) | NS | 0.04 (0.004–0.345) | 0.004 | |
| >75 | 1.42 (0.55–3.68) | NS | 4.47 (1.23–16.10) | 0.023 | 0.12 (0.02–0.84) | 0.033 | |
| Sex | Female | Ref. | Ref. | Ref. | |||
| Male | 0.52 (0.24–1.12) | NS | 1.83 (0.70–4.77) | NS | 1.78 (0.47–6.89) | NS | |
| Smoke history | No | Ref. | Ref. | Ref. | |||
| Yes | 1.12 (0.55–2.28) | NS | 0.62 (0.28–1.36) | NS | 0.40 (0.10–1.70) | NS | |
| BMI class (Kg/m2) | <25 | Ref | Ref. | Ref. | |||
| 25–30 | 1.50 (0.81–2.81) | NS | 1.68 (0.83–3.43) | NS | 1.86 (0.55–6.32) | NS | |
| >30 | 1.08 (0.39–2.97) | NS | 2.86 (0.97–8.37) | NS | 3.50 (0.27–46.0) | NS | |
| Stage of renal failure | Stage I | Ref. | Ref. | Ref. | |||
| Stage II | 0.84 (0.37–1.90) | NS | 0.54 (0.19–1.55) | NS | 11.0 (0.74–162) | NS | |
| Stage III + IV | 0.77 (0.28–2.09) | NS | 2.13 (0.66–6.90) | NS | 46.5 (2.09–1034) | 0.015 | |
| Hypertension | No | Ref. | Ref. | Ref. | |||
| Yes | 0.94 (0.43–2.06) | NS | 1.60 (0.55–4.64) | NS | 6.35 (0.43–93.9) | NS | |
| Diabetes | No | Ref. | Ref. | Ref. | |||
| Yes | 1.13 (0.66–1.94) | NS | 2.29 (1.23–4.27) | 0.009 | 5.00 (1.26–20.0) | 0.022 | |
| Preexistent MACE | No | Ref. | Ref. | Ref. | |||
| Yes | 1.64 (0.88–3.03) | NS | 1.93 (0.96–3.89) | NS | 0.31 (0.07–1.47) | NS | |
| Statin users | No | Ref. | Ref. | Ref. | |||
| Yes | 0.48 (0.27–0.85) | 0.012 | 0.43 (0.22–0.84) | 0.014 | 0.12 (0.03–0.47) | 0.002 | |
| Antiplatelet users | No | Ref. | Ref. | Ref. | |||
| Yes | 0.84 (0.35–1.98) | NS | 1.37 (0.50–3.70) | NS | 1.84 (0.42–8.14) | NS | |
| New MACE occurrence | 2.79 (0.01–556.4) NS | ||||||
| Time to new MACE (months) | 1.01 (0.98–1.03) NS | ||||||
| Age Class (Years) | <65 | 65–75 | >75 | p |
| n (%) | 32 (19) | 73 (43) | 66 (38) | <0.001 |
| Age | 59 ± 2 | 70 ± 3 | 80 ± 4 | |
| BMI Class (Kg/m2) | <25 | 25–30 | >30 | p |
| n (%) | 71 (42) | 76 (44) | 24 (14) | <0.001 |
| BMI | 23.3 ± 1.5 | 27.2 ± 1.4 | 32.9 ± 4.1 | |
| Renal Failure Stage | I | II | III + IV | p |
| n (%) | 27 (16) | 80 (47) | 74 (37) | <0.001 |
| eGFR (mL/min/1.73 m2) | 124 ± 22 | 78 ± 11 | 47 ± 10 |
| Event | All Patients (n = 171) | −Statins (n = 58) | +Statins (n = 113) | p |
|---|---|---|---|---|
| Transitory ischemic attack (n (%)) | 26 (15) | 9 (15) | 17 (15) | NS |
| Fatal and non-fatal stroke (n (%)) | 23 (13) | 13 (22) | 10 (9) | 0.018 |
| Fatal and non-fatal ischemic heart disease (n (%)) | 35 (20) | 10 (17) | 25 (22) | NS |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colussi, G.; Zuttion, F.; Bais, B.; Dolso, P.; Valente, M.; Gigli, G.L.; Gasparini, D.; Sponza, M.; Catena, C.; Sechi, L.A.; et al. Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study. J. Clin. Med. 2018, 7, 286. https://doi.org/10.3390/jcm7090286
Colussi G, Zuttion F, Bais B, Dolso P, Valente M, Gigli GL, Gasparini D, Sponza M, Catena C, Sechi LA, et al. Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study. Journal of Clinical Medicine. 2018; 7(9):286. https://doi.org/10.3390/jcm7090286
Chicago/Turabian StyleColussi, GianLuca, Francesca Zuttion, Bruno Bais, Pierluigi Dolso, Mariarosaria Valente, Gian Luigi Gigli, Daniele Gasparini, Massimo Sponza, Cristiana Catena, Leonardo A. Sechi, and et al. 2018. "Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study" Journal of Clinical Medicine 7, no. 9: 286. https://doi.org/10.3390/jcm7090286
APA StyleColussi, G., Zuttion, F., Bais, B., Dolso, P., Valente, M., Gigli, G. L., Gasparini, D., Sponza, M., Catena, C., Sechi, L. A., & Cavarape, A. (2018). Pre-Procedural Statin Use Is Associated with Improved Long-Term Survival and Reduced Major Cardiovascular Events in Patients Undergoing Carotid Artery Stenting: A Retrospective Study. Journal of Clinical Medicine, 7(9), 286. https://doi.org/10.3390/jcm7090286