What Difference Does it Make? Risk-Taking Behavior in Obesity after a Loss is Associated with Decreased Ventromedial Prefrontal Cortex Activity

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Methods
2.1. Participants
2.2. Impulsivity Measure (UPPS-P)
2.3. Anthropometric Measures
2.4. fMRI Risky Gains Task
2.5. In-Scanner Behavioral Analysis
2.6. Imaging Data Acquisition, Pre-processing, and Analysis
2.6.1. fMRI Image Preprocessing
2.6.2. First-Level Analyses
2.6.3. Second-Level Analyses
2.6.4. Significance Thresholding
2.7. Statistical Analyses of Non-Imaging Data
3. Results
3.1. Clinical and Behavioral Data
3.2. Imaging Data
3.2.1. Losses vs. Wins
3.2.2. Safe Choices vs. Risky Choices
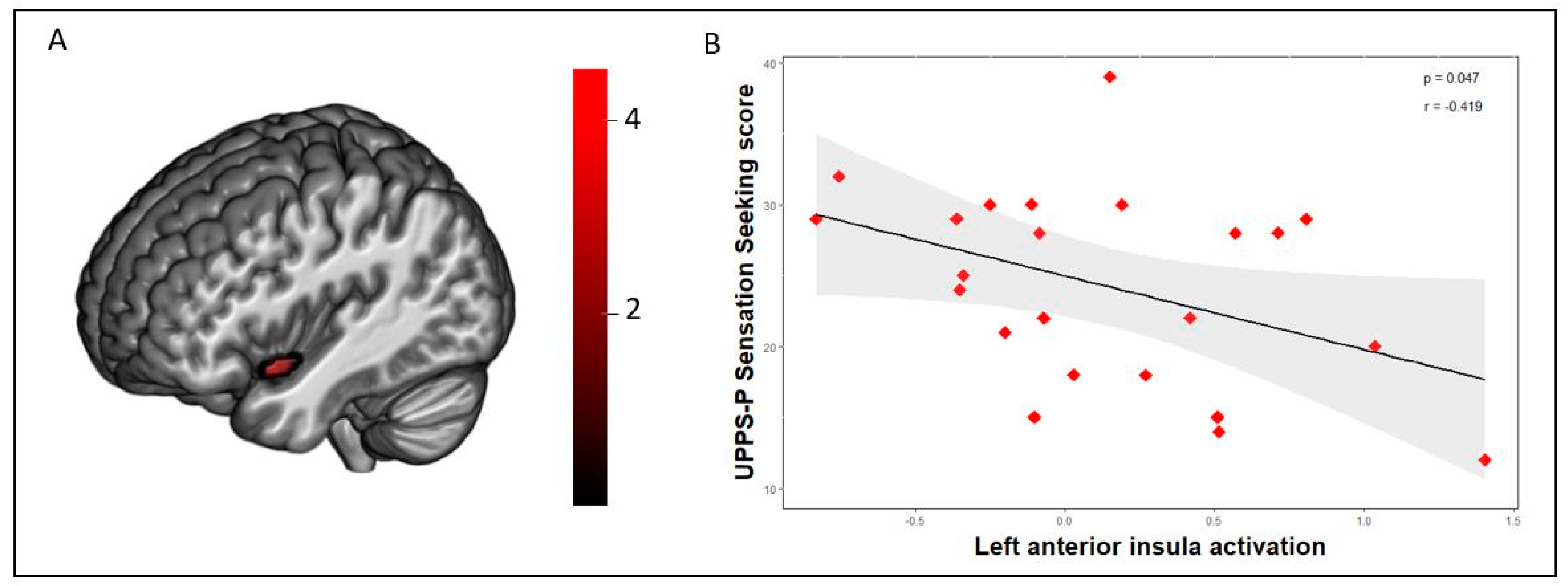
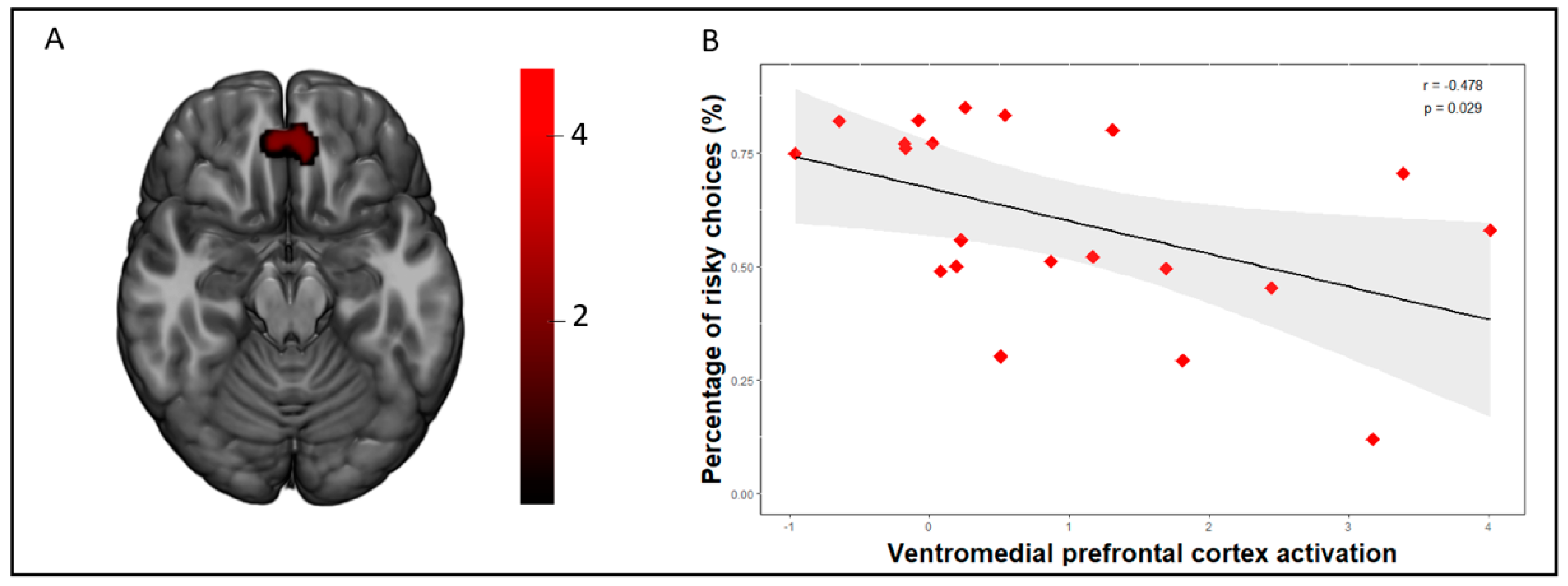
3.3. Correlations between Brain Activation Patterns and Behavioral Measures
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef]
- Mason, A.E.; Schleicher, S.; Coccia, M.; Epel, E.S.; Aschbacher, K. Chronic Stress and Impulsive Risk-Taking Predict Increases in Visceral Fat over 18 Months. Obesity 2018, 26, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Kruschwitz, J.D.; Simmons, A.N.; Flagan, T.; Paulus, M.P. Nothing to lose: Processing blindness to potential losses drives thrill and adventure seekers. Neuroimage 2012, 59, 2850–2859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotge, J.-Y.; Poitou, C.; Fossati, P.; Aron-Wisnewsky, J.; Oppert, J.-M. Decision-making in obesity without eating disorders: A systematic review and meta-analysis of Iowa gambling task performances. Obes. Rev. 2017, 18, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Mobbs, O.; Crépin, C.; Thiéry, C.; Golay, A.; Van der Linden, M. Obesity and the four facets of impulsivity. Patient Educ. Couns. 2010, 79, 372–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steward, T.; Mestre-Bach, G.; Vintró-Alcaraz, C.; Agüera, Z.; Jiménez-Murcia, S.; Granero, R.; Fernández-Aranda, F. Delay Discounting of Reward and Impulsivity in Eating Disorders: From Anorexia Nervosa to Binge Eating Disorder. Eur. Eat. Disord. Rev. 2017, 25, 601–606. [Google Scholar] [CrossRef] [PubMed]
- Navas, J.F.; Barrós-Loscertales, A.; Costumero-Ramos, V.; Verdejo-Román, J.; Vilar-López, R.; Verdejo-García, A. Excessive body fat linked to blunted somatosensory cortex response to general reward in adolescents. Int. J. Obes. 2018, 42, 88–94. [Google Scholar] [CrossRef]
- Paulus, M.P.; Rogalsky, C.; Simmons, A.; Feinstein, J.S.; Stein, M.B. Increased activation in the right insula during risk-taking decision making is related to harm avoidance and neuroticism. Neuroimage 2003, 19, 1439–1448. [Google Scholar] [CrossRef]
- Gowin, J.L.; May, A.C.; Wittmann, M.; Tapert, S.F.; Paulus, M.P. Doubling down: Increased risk-taking behavior following a loss by individuals with cocaine use disorder is associated with striatal and anterior cingulate dysfunction. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2017, 2, 94–103. [Google Scholar] [CrossRef]
- Mata, F.; Verdejo-Roman, J.; Soriano-Mas, C.; Verdejo-Garcia, A. Insula tuning towards external eating versus interoceptive input in adolescents with overweight and obesity. Appetite 2015, 93, 24–30. [Google Scholar] [CrossRef]
- Craig, A.D.B. How do you feel--now? The anterior insula and human awareness. Nat. Rev. Neurosci. 2009, 10, 59–70. [Google Scholar] [CrossRef]
- Mata, F.; Verdejo-Roman, J.; Soriano-Mas, C.; Yücel, M.; Verdejo-Garcia, A. Changes in choice evoked brain activations after a weight loss intervention in adolescents. Appetite 2016, 103, 113–117. [Google Scholar] [CrossRef]
- Herbert, B.M.; Blechert, J.; Hautzinger, M.; Matthias, E.; Herbert, C. Intuitive eating is associated with interoceptive sensitivity. Effects on body mass index. Appetite 2013, 70, 22–30. [Google Scholar] [CrossRef]
- Herbert, B.M.; Pollatos, O. Attenuated interoceptive sensitivity in overweight and obese individuals. Eat. Behav. 2014, 15, 445–448. [Google Scholar] [CrossRef]
- Steward, T.; Menchón, J.M.; Jiménez-Murcia, S.; Soriano-Mas, C.; Fernández-Aranda, F. Neural network alterations across eating disorders: A narrative review of fMRI studies. Curr. Neuropharmacol. 2018, 16, 1150–1163. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.-J.; Tomasi, D.; Baler, R.D. Obesity and addiction: Neurobiological overlaps. Obes. Rev. 2013, 14, 2–18. [Google Scholar] [CrossRef]
- Cross, C.P.; Cyrenne, D.-L.M.; Brown, G.R. Sex differences in sensation-seeking: A meta-analysis. Sci. Rep. 2013, 3, 2486. [Google Scholar] [CrossRef]
- Dietrich, A.; Federbusch, M.; Grellmann, C.; Villringer, A.; Horstmann, A. Body weight status, eating behavior, sensitivity to reward/punishment, and gender: Relationships and interdependencies. Front. Psychol. 2014, 5, 1073. [Google Scholar] [CrossRef]
- Delgado-Rico, E.; Soriano-Mas, C.; Verdejo-Román, J.; Río-Valle, J.S.; Verdejo-García, A. Decreased insular and increased midbrain activations during decision-making under risk in adolescents with excess weight. Obesity 2013, 21, 1662–1668. [Google Scholar] [CrossRef]
- Pujara, M.S.; Philippi, C.L.; Motzkin, J.C.; Baskaya, M.K.; Koenigs, M. Ventromedial Prefrontal Cortex Damage Is Associated with Decreased Ventral Striatum Volume and Response to Reward. J. Neurosci. 2016, 36, 5047–5054. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. 20), 22–33. [Google Scholar]
- Whiteside, S.P.; Lynam, D.R.; Miller, J.D.; Reynolds, S.K. Validation of the UPPS impulsive behaviour scale: A four-factor model of impulsivity. Eur. J. Personal. 2005, 19, 559–574. [Google Scholar] [CrossRef]
- Verdejo-García, A.; Lozano, O.; Moya, M.; Alcázar, M.A.; Pérez-García, M. Psychometric properties of a Spanish version of the UPPS-P impulsive behavior scale: Reliability, validity and association with trait and cognitive impulsivity. J. Personal. Assess. 2010, 92, 70–77. [Google Scholar] [CrossRef]
- Browning, L.M.; Mugridge, O.; Dixon, A.K.; Aitken, S.W.; Prentice, A.M.; Jebb, S.A. Measuring abdominal adipose tissue: Comparison of simpler methods with MRI. Obes. Facts 2011, 4, 9–15. [Google Scholar] [CrossRef]
- Blair, M.A.; Stewart, J.L.; May, A.C.; Reske, M.; Tapert, S.F.; Paulus, M.P. Blunted Frontostriatal Blood Oxygen Level-Dependent Signals Predict Stimulant and Marijuana Use. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 947–958. [Google Scholar] [CrossRef]
- Patel, A.X.; Bullmore, E.T. A wavelet-based estimator of the degrees of freedom in denoised fMRI time series for probabilistic testing of functional connectivity and brain graphs. Neuroimage 2016, 142, 14–26. [Google Scholar] [CrossRef]
- Whitfield-Gabrieli, S.; Nieto-Castanon, A. Conn: A Functional Connectivity Toolbox for Correlated and Anticorrelated Brain Networks. Brain Connect. 2012, 2, 125–141. [Google Scholar] [CrossRef]
- Song, X.-W.; Dong, Z.-Y.; Long, X.-Y.; Li, S.-F.; Zuo, X.-N.; Zhu, C.-Z.; He, Y.; Yan, C.-G.; Zang, Y.-F. REST: A Toolkit for Resting-State Functional Magnetic Resonance Imaging Data Processing. PLoS ONE 2011, 6, e25031. [Google Scholar] [CrossRef]
- Kelley, K.; Preacher, K.J. On effect size. Psychol. Methods 2012, 17, 137–152. [Google Scholar] [CrossRef]
- Simmons, W.K.; DeVille, D.C. Interoceptive contributions to healthy eating and obesity. Curr. Opin. Psychol. 2017, 17, 106–112. [Google Scholar] [CrossRef]
- Zheng, Y.; Li, Q.; Tian, M.; Nan, W.; Yang, G.; Liang, J.; Liu, X. Deficits in voluntary pursuit and inhibition of risk taking in sensation seeking. Hum. Brain Mapp. 2017, 38, 6019–6028. [Google Scholar] [CrossRef] [Green Version]
- Steward, T.; Picó-Pérez, M.; Mata, F.; Martínez-Zalacaín, I.; Cano, M.; Contreras-Rodríguez, O.; Fernández-Aranda, F.; Yucel, M.; Soriano-Mas, C.; Verdejo-García, A. Emotion Regulation and Excess Weight: Impaired Affective Processing Characterized by Dysfunctional Insula Activation and Connectivity. PLoS ONE 2016, 11, e0152150. [Google Scholar] [CrossRef]
- O’Reilly, G.A.; Cook, L.; Spruijt-Metz, D.; Black, D.S. Mindfulness-based interventions for obesity-related eating behaviours: A literature review. Obes. Rev. 2014, 15, 453–461. [Google Scholar] [CrossRef]
- Gowin, J.L.; Stewart, J.L.; May, A.C.; Ball, T.M.; Wittmann, M.; Tapert, S.F.; Paulus, M.P. Altered cingulate and insular cortex activation during risk-taking in methamphetamine dependence: Losses lose impact. Addiction 2014, 109, 237–247. [Google Scholar] [CrossRef]
- Steward, T.; Picó-Pérez, M.; Mestre-Bach, G.; Martínez-Zalacaín, I.; Suñol, M.; Jiménez-Murcia, S.; Fernández-Formoso, J.A.; Vilarrasa, N.; García-Ruiz-de-Gordejuela, A.; de las Heras, M.; et al. A multimodal MRI study of the neural mechanisms of emotion regulation impairment in women with obesity. Transl. Psychiatry 2019, 9, 194. [Google Scholar] [CrossRef]
- Steward, T.; Mestre-Bach, G.; Vintró-Alcaraz, C.; Lozano-Madrid, M.; Agüera, Z.; Fernández-Formoso, J.A.; Granero, R.; Jiménez-Murcia, S.; Vilarrasa, N.; García-Ruiz-de-Gordejuela, A.; et al. Food addiction and impaired executive functions in women with obesity. Eur. Eat. Disord. Rev. 2018, 26, 574–584. [Google Scholar] [CrossRef]
- Haber, S.N.; Behrens, T.E.J. The neural network underlying incentive-based learning: Implications for interpreting circuit disruptions in psychiatric disorders. Neuron 2014, 83, 1019–1039. [Google Scholar] [CrossRef]
- Suarez-Jimenez, B.; Bisby, J.A.; Horner, A.J.; King, J.A.; Pine, D.S.; Burgess, N. Linked networks for learning and expressing location-specific threat. Proc. Natl. Acad. Sci. USA 2018, 115, E1032–E1040. [Google Scholar] [CrossRef]
- García-García, I.; Michaud, A.; Dadar, M.; Zeighami, Y.; Neseliler, S.; Collins, D.L.; Evans, A.C.; Dagher, A. Neuroanatomical differences in obesity: Meta-analytic findings and their validation in an independent dataset. Int. J. Obes. 2019, 43, 943–951. [Google Scholar] [CrossRef]
- Arnoriaga Rodríguez, M.; Blasco, G.; Coll, C.; Biarnés, C.; Contreras-Rodríguez, O.; Garre-Olmo, J.; Puig, J.; Gich, J.; Ricart, W.; Ramió-Torrentà, L.; et al. Glycated Hemoglobin, but not Insulin Sensitivity, is Associated with Memory in Subjects with Obesity. Obesity 2019, 27, 932–942. [Google Scholar] [CrossRef]
- Leslie, M.; Turton, R.; Burgess, E.; Nazar, B.P.; Treasure, J. Testing the addictive appetite model of binge eating: The importance of craving, coping, and reward enhancement. Eur. Eat. Disord. Rev. 2018, 26, 541–550. [Google Scholar] [CrossRef] [Green Version]
- Preuss, H.; Pinnow, M.; Schnicker, K.; Legenbauer, T. Improving Inhibitory Control Abilities (ImpulsE)—A Promising Approach to Treat Impulsive Eating? Eur. Eat. Disord. Rev. 2017, 25, 533–543. [Google Scholar] [CrossRef]
- Reggente, N.; Moody, T.D.; Morfini, F.; Sheen, C.; Rissman, J.; O’Neill, J.; Feusner, J.D. Multivariate resting-state functional connectivity predicts response to cognitive behavioral therapy in obsessive–compulsive disorder. Proc. Natl. Acad. Sci. USA 2018, 115, 2222–2227. [Google Scholar] [CrossRef]
- Gowin, J.L.; Ball, T.M.; Wittmann, M.; Tapert, S.F.; Paulus, M.P. Individualized relapse prediction: Personality measures and striatal and insular activity during reward-processing robustly predict relapse. Drug Alcohol Depend. 2015, 152, 93–101. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Healthy Weight | Obese | |||||
|---|---|---|---|---|---|---|
| n = 23 | n = 23 | |||||
| Mean | SD | Mean | SD | p | |d| | |
| Age | 30.57 | 10.96 | 36.57 | 9.75 | 0.056 | 0.58 |
| Education (years) | 15.80 | 1.67 | 14.79 | 2.29 | 0.17 | 0.50 |
| BMI | 20.93 | 1.90 | 43.35 | 6.98 | <0.001 a | 4.39 b |
| Body fat mass (%) | 24.50 | 5.26 | 47.11 | 5.12 | <0.001 a | 4.35 b |
| UPPS-P subscales | ||||||
| Negative urgency | 25.22 | 6.52 | 28.17 | 6.39 | 0.13 | 0.46 |
| Lack of premeditation | 21.78 | 4.96 | 23.30 | 5.14 | 0.31 | 0.30 |
| Lack of perseverance | 19.30 | 5.30 | 22.17 | 5.16 | 0.07 | 0.54 |
| Sensation seeking | 28.35 | 8.44 | 24.26 | 6.84 | 0.08 | 0.53 |
| Positive urgency | 22.52 | 6.63 | 20.78 | 5.13 | 0.33 | 0.29 |
| Risky gains task | ||||||
| Risky choices following loss (%) | 59.87 | 21.05 | 46.93 | 29.55 | 0.09 | 0.50 |
| Risky choices overall (%) | 67.34 | 16.81 | 60.26 | 21.09 | 0.22 | 0.37 |
| MNI | ||||
|---|---|---|---|---|
| Coordinates | ||||
| Contrast | Peak Region | (x,y,z) | Ke a | t |
| Losses vs. wins | Right angular gyrus | 46, −54, 30 | 188 | 5.78 |
| HC > OB | Right occipital lobe | 10, −82, 36 | 301 | 4.53 |
| Left anterior insula | −44, 8, −14 | 52 | 4.15 | |
| Left extrastriate visual cortex | −6, −80, 18 | 101 | 3.88 | |
| Safe choices vs risky choices following a loss | Ventromedial prefrontal cortex | 2, 44, −24 | 175 | 4.75 |
| HC > OB |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steward, T.; Juaneda-Seguí, A.; Mestre-Bach, G.; Martínez-Zalacaín, I.; Vilarrasa, N.; Jiménez-Murcia, S.; Fernández-Formoso, J.A.; Veciana de las Heras, M.; Custal, N.; Virgili, N.; et al. What Difference Does it Make? Risk-Taking Behavior in Obesity after a Loss is Associated with Decreased Ventromedial Prefrontal Cortex Activity. J. Clin. Med. 2019, 8, 1551. https://doi.org/10.3390/jcm8101551
Steward T, Juaneda-Seguí A, Mestre-Bach G, Martínez-Zalacaín I, Vilarrasa N, Jiménez-Murcia S, Fernández-Formoso JA, Veciana de las Heras M, Custal N, Virgili N, et al. What Difference Does it Make? Risk-Taking Behavior in Obesity after a Loss is Associated with Decreased Ventromedial Prefrontal Cortex Activity. Journal of Clinical Medicine. 2019; 8(10):1551. https://doi.org/10.3390/jcm8101551
Chicago/Turabian StyleSteward, Trevor, Asier Juaneda-Seguí, Gemma Mestre-Bach, Ignacio Martínez-Zalacaín, Nuria Vilarrasa, Susana Jiménez-Murcia, Jose A Fernández-Formoso, Misericordia Veciana de las Heras, Nuria Custal, Nuria Virgili, and et al. 2019. "What Difference Does it Make? Risk-Taking Behavior in Obesity after a Loss is Associated with Decreased Ventromedial Prefrontal Cortex Activity" Journal of Clinical Medicine 8, no. 10: 1551. https://doi.org/10.3390/jcm8101551
APA StyleSteward, T., Juaneda-Seguí, A., Mestre-Bach, G., Martínez-Zalacaín, I., Vilarrasa, N., Jiménez-Murcia, S., Fernández-Formoso, J. A., Veciana de las Heras, M., Custal, N., Virgili, N., Lopez-Urdiales, R., García-Ruiz-de-Gordejuela, A., Menchón, J. M., Soriano-Mas, C., & Fernandez-Aranda, F. (2019). What Difference Does it Make? Risk-Taking Behavior in Obesity after a Loss is Associated with Decreased Ventromedial Prefrontal Cortex Activity. Journal of Clinical Medicine, 8(10), 1551. https://doi.org/10.3390/jcm8101551