Epithelial Alarmins in Serum and Exhaled Breath in Patients with Idiopathic Pulmonary Fibrosis: A Prospective One-Year Follow-Up Cohort Study

 ,
, 

Abstract
:1. Introduction
2. Experimental Section
2.1. Study Population
2.2. Methods
2.3. Pulmonary Function Assessments
2.4. The Six-Minute Walk Test (6MWT)
2.5. Composite Physiologic Index (CPI)
2.6. Blood Samples Processing
2.7. Exhaled Breath Condensate (EBC)
2.8. Alarmin Levels Measurements
2.9. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Baseline Epithelial Alarmin Levels in the Serum
3.3. Baseline Epithelial Alarmin Levels in the EBC
3.4. Associations of Epithelial Alarmin Levels in the Serum and EBC of Patients with IPF
3.5. Associations between the Epithelial Alarmin Levels and Clinical Measures in Patients with IPF
3.6. Changes in the Epithelial Alarmin Levels in the Serum of Patients with IPF before and after 12 Months of Antifibrotic Therapy
3.7. Changes in the Epithelial Alarmin Levels in the EBC before and after 12 Months of Antifibrotic Therapy
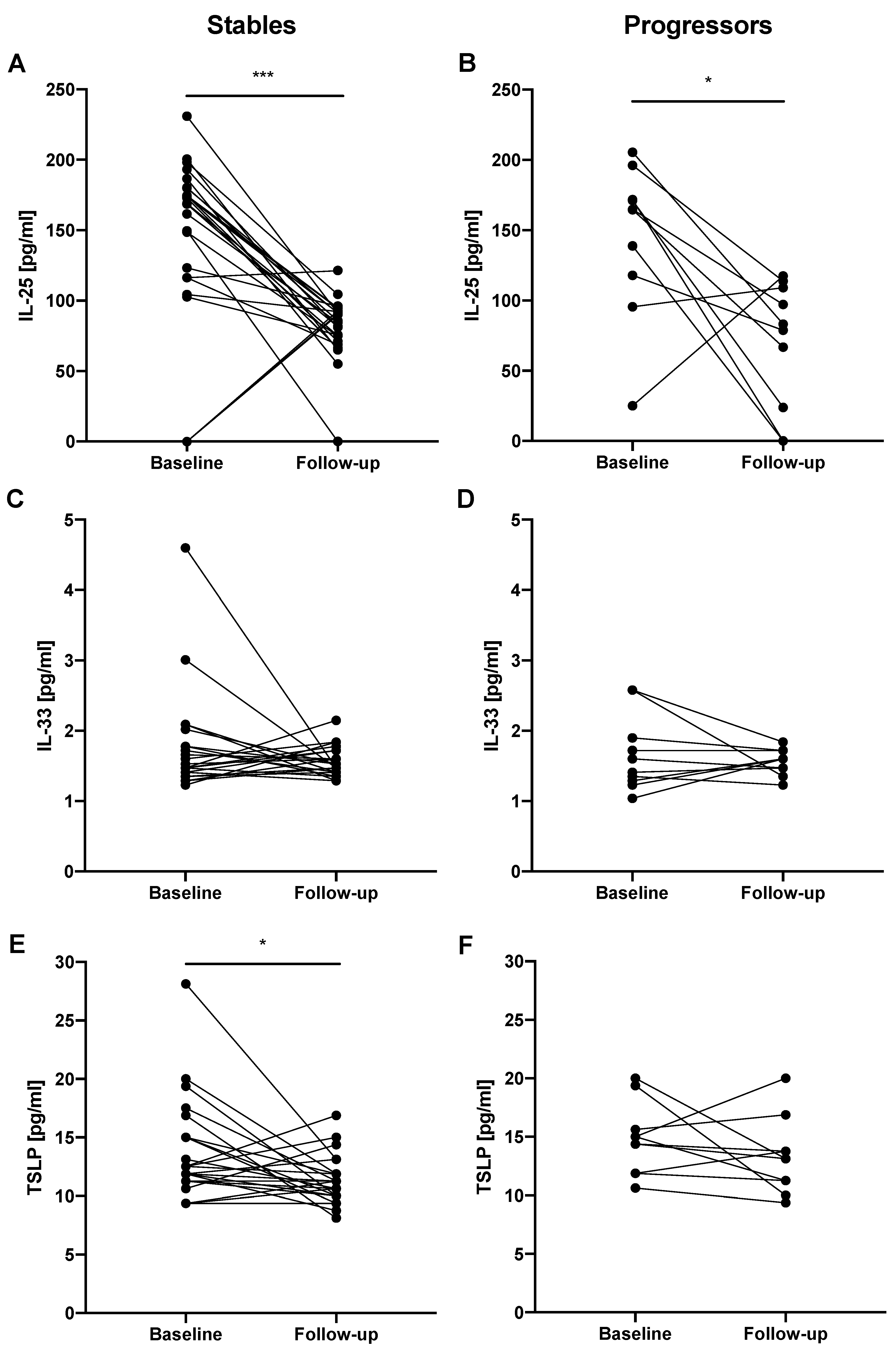
3.8. Changes in the Epithelial Alarmin Levels in the Serum of Patients with IPF before and after 12 Months of Antifibrotic Therapy According to the Functional Decline
3.9. Changes in the Epithelial Alarmin Levels in the EBC of Patients with IPF before and after 12 Months of Antifibrotic Therapy According to the Functional Decline
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Saenz, S.A.; Taylor, B.C.; Artis, D. Welcome to the neighborhood: Epithelial cell-derived cytokines license innate and adaptive immune responses at mucosal sites. Immunol. Rev. 2008, 226, 172–190. [Google Scholar] [CrossRef] [PubMed]
- Dickel, H.; Gambichler, T.; Kamphowe, J.; Altmeyer, P.; Skrygan, M. Standardized tape stripping prior to patch testing induces upregulation of Hsp90, Hsp70, IL-33, TNF-α and IL-8/CXCL8 mRNA: New insights into the involvement of “alarmins”. Contact Dermatitis. 2010, 63, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Oyoshi, M.K.; Larson, R.P.; Ziegler, S.F.; Geha, R.S. Mechanical injury polarizes skin dendritic cells to elicit a T(H)2 response by inducing cutaneous thymic stromal lymphopoietin expression. J. Allergy Clin. Immunol. 2010, 126, 976–984. [Google Scholar] [CrossRef] [PubMed]
- Licona-Limón, P.; Kim, L.K.; Palm, N.W.; Flavell, R.A. TH2, allergy and group 2 innate lymphoid cells. Nat. Immunol. 2013. [Google Scholar] [CrossRef]
- Smithgall, M.D.; Comeau, M.R.; Yoon, B.-R.P.; Kaufman, D.; Armitage, R.; Smith, D.E. IL-33 amplifies both Th1- and Th2-type responses through its activity on human basophils, allergen-reactive Th2 cells, iNKT and NK cells. Int. Immunol. 2008, 20, 1019–1030. [Google Scholar] [CrossRef]
- Luzina, I.G.; Kopach, P.; Lockatell, V.; Kang, P.H.; Nagarsekar, A.; Burke, A.P.; Hasday, J.D.; Todd, N.W.; Atamas, S.P. Interleukin-33 potentiates bleomycin-induced lung injury. Am. J. Respir. Cell Mol. Biol. 2013, 49, 999–1008. [Google Scholar] [CrossRef]
- Xu, J.; Zheng, J.; Song, P.; Zhou, Y.; Guan, S. IL-33/ST2 pathway in a bleomycin-induced pulmonary fibrosis model. Mol. Med. Rep. 2016, 14, 1704–1708. [Google Scholar] [CrossRef]
- Lee, J.-U.; Chang, H.S.; Lee, H.J.; Jung, C.A.; Bae, D.J.; Song, H.J.; Park, J.S.; Uh, S.-T.; Kim, Y.H.; Seo, K.-H.; et al. Upregulation of interleukin-33 and thymic stromal lymphopoietin levels in the lungs of idiopathic pulmonary fibrosis. BMC Pulm. Med. 2017. [Google Scholar] [CrossRef]
- Hams, E.; Armstrong, M.E.; Barlow, J.L.; Saunders, S.P.; Schwartz, C.; Cooke, G.; Fahy, R.J.; Crotty, T.B.; Hirani, N.; Flynn, R.J.; et al. IL-25 and type 2 innate lymphoid cells induce pulmonary fibrosis. Proc. Natl. Acad. Sci. USA 2014, 111, 367–372. [Google Scholar] [CrossRef]
- Xu, X.; Luo, S.; Li, B.; Dai, H.; Zhang, J. Feature Article: IL-25 contributes to lung fibrosis by directly acting on alveolar epithelial cells and fibroblasts. Exp. Biol. Med. Maywood NJ 2019, 244, 770–780. [Google Scholar] [CrossRef]
- Camelo, A.; Dunmore, R.; Sleeman, M.A.; Clarke, D.L. The epithelium in idiopathic pulmonary fibrosis: Breaking the barrier. Front. Pharmacol. 2014. [Google Scholar] [CrossRef]
- Lederer, D.J.; Martinez, F.J. Idiopathic Pulmonary Fibrosis. N. Engl. J. Med. 2018, 378, 1811–1823. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Guabiraba, R.; Besnard, A.-G.; Komai-Koma, M.; Jabir, M.S.; Zhang, L.; Graham, G.J.; Kurowska-Stolarska, M.; Liew, F.Y.; McSharry, C.; et al. IL-33 promotes ST2-dependent lung fibrosis by the induction of alternatively activated macrophages and innate lymphoid cells in mice. J. Allergy Clin. Immunol. 2014, 134, 1422–1432. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; De Los Santos, F.G.; Wu, Z.; Liu, T.; Phan, S.H. An ST2-dependent role of bone marrow-derived group 2 innate lymphoid cells in pulmonary fibrosis. J. Pathol. 2018, 245, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Alexander, R.; Sulikowski, M.G.; Nicholson, A.G.; Maher, T.M.; Scotton, C.J.; Chambers, R.C. Evidence for a functional thymic stromal lymphopoietin signaling axis in fibrotic lung disease. J. Immunol. Baltim. 2013, 191, 4867–4879. [Google Scholar] [CrossRef]
- Manetti, M.; Ibba-Manneschi, L.; Liakouli, V.; Guiducci, S.; Milia, A.F.; Benelli, G.; Marrelli, A.; Conforti, M.L.; Romano, E.; Giacomelli, R.; et al. The IL1-like cytokine IL33 and its receptor ST2 are abnormally expressed in the affected skin and visceral organs of patients with systemic sclerosis. Ann. Rheum. Dis. 2010, 69, 598–605. [Google Scholar] [CrossRef]
- Yanaba, K.; Yoshizaki, A.; Asano, Y.; Kadono, T.; Sato, S. Serum IL-33 levels are raised in patients with systemic sclerosis: Association with extent of skin sclerosis and severity of pulmonary fibrosis. Clin. Rheumatol. 2011, 30, 825–830. [Google Scholar] [CrossRef]
- Usategui, A.; Criado, G.; Izquierdo, E.; Del Rey, M.J.; Carreira, P.E.; Ortiz, P.; Leonard, W.J.; Pablos, J.L. A profibrotic role for thymic stromal lymphopoietin in systemic sclerosis. Ann. Rheum. Dis. 2013, 72, 2018–2023. [Google Scholar] [CrossRef]
- Kempf, W.; Zollinger, T.; Sachs, M.; Ullmer, E.; Cathomas, G.; Dirnhofer, S.; Mertz, K.D. Granulomas are a source of interleukin-33 expression in pulmonary and extrapulmonary sarcoidosis. Hum. Pathol. 2014, 45, 2202–2210. [Google Scholar] [CrossRef]
- Abdel-Wahab, S.M.; Tharwat, I.; Atta, D.S.; El-Sammak, A.A.; Atef, R. Serum level of interleukin-33 in rheumatoid arthritis patients and its association with bone erosion and interstitial lung disease. Egypt. Rheumatol. 2016, 38, 99–104. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.D.; Montpetit, A.; Hunt, J. Exhaled breath condensate: An overview. Immunol. Allergy Clin. N. Am. 2012, 32, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Popov, T.A. Human exhaled breath analysis. Ann. Allergy Asthma Immunol. Am. Coll. Allergy Asthma Immunol. 2011, 106, 451–456. [Google Scholar] [CrossRef] [PubMed]
- Glück, J.; Rymarczyk, B.; Kasprzak, M.; Rogala, B. Increased Levels of Interleukin-33 and Thymic Stromal Lymphopoietin in Exhaled Breath Condensate in Chronic Bronchial Asthma. Int. Arch. Allergy Immunol. 2016, 169, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Gorska, K.; Nejman-Gryz, P.; Paplinska-Goryca, M.; Korczynski, P.; Prochorec-Sobieszek, M.; Krenke, R. Comparative Study of IL-33 and IL-6 Levels in Different Respiratory Samples in Mild-to-Moderate Asthma and COPD. COPD 2018, 15, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Tworek, D.; Majewski, S.; Szewczyk, K.; Kiszałkiewicz, J.; Kurmanowska, Z.; Górski, P.; Brzeziańska-Lasota, E.; Kuna, P.; Antczak, A. The association between airway eosinophilic inflammation and IL-33 in stable non-atopic COPD. Respir. Res. 2018. [Google Scholar] [CrossRef] [PubMed]
- Majewski, S.; Tworek, D.; Szewczyk, K.; Kurmanowska, Z.; Antczak, A.; Górski, P.; Piotrowski, W.J. Epithelial alarmin levels in exhaled breath condensate in patients with idiopathic pulmonary fibrosis—A pilot study. Clin. Respir. J. 2019. [Google Scholar] [CrossRef]
- Raghu, G.; Collard, H.R.; Egan, J.J.; Martinez, F.J.; Behr, J.; Brown, K.K.; Colby, T.V.; Cordier, J.-F.; Flaherty, K.R.; Lasky, J.A.; et al. An official ATS/ERS/JRS/ALAT statement: Idiopathic pulmonary fibrosis: Evidence-based guidelines for diagnosis and management. Am. J. Respir. Crit. Care Med. 2011, 183, 788–824. [Google Scholar] [CrossRef]
- Miller, M.R. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Graham, B.L.; Brusasco, V.; Burgos, F.; Cooper, B.G.; Jensen, R.; Kendrick, A.; MacIntyre, N.R.; Thompson, B.R.; Wanger, J. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung. Eur. Respir. J. 2017, 49. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef]
- Stanojevic, S.; Graham, B.L.; Cooper, B.G.; Thompson, B.R.; Carter, K.W.; Francis, R.W.; Hall, G.L. Official ERS technical standards: Global Lung Function Initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur. Respir. J. 2017. [Google Scholar] [CrossRef] [PubMed]
- Przybyłowski, T.; Tomalak, W.; Siergiejko, Z.; Jastrzębski, D.; Maskey-Warzęchowska, M.; Piorunek, T.; Wojda, E.; Boros, P. Polish Respiratory Society guidelines for the methodology and interpretation of the 6 minute walk test (6MWT). Pneumonol. Alergol. Pol. 2015, 83, 283–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, A.U.; Desai, S.R.; Rubens, M.B.; Goh, N.S.L.; Cramer, D.; Nicholson, A.G.; Colby, T.V.; du Bois, R.M.; Hansell, D.M. Idiopathic pulmonary fibrosis: A composite physiologic index derived from disease extent observed by computed tomography. Am. J. Respir. Crit. Care Med. 2003, 167, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Horváth, I.; Hunt, J.; Barnes, P.J.; Alving, K.; Antczak, A.; Baraldi, E.; Becher, G.; van Beurden, W.J.C.; Corradi, M.; Dekhuijzen, R.; et al. Exhaled breath condensate: Methodological recommendations and unresolved questions. Eur. Respir. J. 2005, 26, 523–548. [Google Scholar] [CrossRef] [PubMed]
- Hallstrand, T.S.; Hackett, T.L.; Altemeier, W.A.; Matute-Bello, G.; Hansbro, P.M.; Knight, D.A. Airway epithelial regulation of pulmonary immune homeostasis and inflammation. Clin. Immunol. Orlando Fla 2014, 151, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fort, M.M.; Cheung, J.; Yen, D.; Li, J.; Zurawski, S.M.; Lo, S.; Menon, S.; Clifford, T.; Hunte, B.; Lesley, R.; et al. IL-25 induces IL-4, IL-5, and IL-13 and Th2-associated pathologies in vivo. Immunity 2001, 15, 985–995. [Google Scholar] [CrossRef]
- Schmitz, J.; Owyang, A.; Oldham, E.; Song, Y.; Murphy, E.; McClanahan, T.K.; Zurawski, G.; Moshrefi, M.; Qin, J.; Li, X.; et al. IL-33, an interleukin-1-like cytokine that signals via the IL-1 receptor-related protein ST2 and induces T helper type 2-associated cytokines. Immunity 2005, 23, 479–490. [Google Scholar] [CrossRef]
- Cheng, D.; Xue, Z.; Yi, L.; Shi, H.; Zhang, K.; Huo, X.; Bonser, L.R.; Zhao, J.; Xu, Y.; Erle, D.J.; et al. Epithelial interleukin-25 is a key mediator in Th2-high, corticosteroid-responsive asthma. Am. J. Respir. Crit. Care Med. 2014, 190, 639–648. [Google Scholar] [CrossRef]
- Wynn, T.A. Fibrotic disease and the T(H)1/T(H)2 paradigm. Nat. Rev. Immunol. 2004, 4, 583–594. [Google Scholar] [CrossRef]
- Gieseck, R.L.; Wilson, M.S.; Wynn, T.A. Type 2 immunity in tissue repair and fibrosis. Nat. Rev. Immunol. 2018, 18, 62–76. [Google Scholar] [CrossRef]
- Lloyd, C.M.; Snelgrove, R.J. Type 2 immunity: Expanding our view. Sci. Immunol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Luzina, I.G.; Pickering, E.M.; Kopach, P.; Kang, P.H.; Lockatell, V.; Todd, N.W.; Papadimitriou, J.C.; McKenzie, A.N.J.; Atamas, S.P. Full-length IL-33 promotes inflammation but not Th2 response in vivo in an ST2-independent fashion. J. Immunol. Baltim. 2012, 189, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Mjösberg, J.M.; Trifari, S.; Crellin, N.K.; Peters, C.P.; van Drunen, C.M.; Piet, B.; Fokkens, W.J.; Cupedo, T.; Spits, H. Human IL-25- and IL-33-responsive type 2 innate lymphoid cells are defined by expression of CRTH2 and CD161. Nat. Immunol. 2011, 12, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Vannella, K.M.; Ramalingam, T.R.; Borthwick, L.A.; Barron, L.; Hart, K.M.; Thompson, R.W.; Kindrachuk, K.N.; Cheever, A.W.; White, S.; Budelsky, A.L.; et al. Combinatorial targeting of TSLP, IL-25, and IL-33 in type 2 cytokine-driven inflammation and fibrosis. Sci. Transl. Med. 2016. [Google Scholar] [CrossRef] [PubMed]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef]
- King, T.E.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef]
- Raghu, G.; Rochwerg, B.; Zhang, Y.; Garcia, C.A.C.; Azuma, A.; Behr, J.; Brozek, J.L.; Collard, H.R.; Cunningham, W.; Homma, S.; et al. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline: Treatment of Idiopathic Pulmonary Fibrosis. An Update of the 2011 Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2015, 192, e3–e19. [Google Scholar] [CrossRef]
- Chaudhary, N.I.; Roth, G.J.; Hilberg, F.; Müller-Quernheim, J.; Prasse, A.; Zissel, G.; Schnapp, A.; Park, J.E. Inhibition of PDGF, VEGF and FGF signalling attenuates fibrosis. Eur. Respir. J. 2007, 29, 976–985. [Google Scholar] [CrossRef] [Green Version]
- Oku, H.; Shimizu, T.; Kawabata, T.; Nagira, M.; Hikita, I.; Ueyama, A.; Matsushima, S.; Torii, M.; Arimura, A. Antifibrotic action of pirfenidone and prednisolone: Different effects on pulmonary cytokines and growth factors in bleomycin-induced murine pulmonary fibrosis. Eur. J. Pharmacol. 2008, 590, 400–408. [Google Scholar] [CrossRef]
- Didiasova, M.; Singh, R.; Wilhelm, J.; Kwapiszewska, G.; Wujak, L.; Zakrzewicz, D.; Schaefer, L.; Markart, P.; Seeger, W.; Lauth, M.; et al. Pirfenidone exerts antifibrotic effects through inhibition of GLI transcription factors. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2017, 31, 1916–1928. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Yu, W.; Guo, F. Pirfenidone suppresses bleomycin-induced pulmonary fibrosis and periostin expression in rats. Exp. Ther. Med. 2018, 16, 1800–1806. [Google Scholar] [CrossRef] [PubMed]
- Kwapiszewska, G.; Gungl, A.; Wilhelm, J.; Marsh, L.M.; Thekkekara Puthenparampil, H.; Sinn, K.; Didiasova, M.; Klepetko, W.; Kosanovic, D.; Schermuly, R.T.; et al. Transcriptome profiling reveals the complexity of pirfenidone effects in idiopathic pulmonary fibrosis. Eur. Respir. J. 2018. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jones, K.D.; Achtar-Zadeh, N.; Green, G.; Kukreja, J.; Xu, B.; Wolters, P.J. Histopathological and molecular analysis of idiopathic pulmonary fibrosis lungs from patients treated with pirfenidone or nintedanib. Histopathology 2019, 74, 341–349. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Controls | IPF | |
|---|---|---|
| Number of subjects | 30 | 52 |
| Sex (male/female) | 17/13 | 39/13 |
| Age (years), mean (SD) | 61.36 (7.26) | 68.21 (8.76) *** |
| Smoking exposure (pack-years) median (IQR) | 8 (0–25) | 26.5 (7.75–39) ** |
| Smoking status | ||
| never smokers, n (%) | 12 (40.00) | 12 (23.07) |
| ex-smokers, n (%) | 8 (26.67) | 37 (71.15) |
| current smokers, n (%) | 10 (33.33) | 3 (5.77) |
| GAP score, median (IQR) | N/A | 4.0 (3.0–4.5) |
| GAP index: | N/A | |
| Stage I, n (%) | 24 (46.15) | |
| Stage II, n (%) | 27 (51.92) | |
| Stage III, n (%) | 1 (1.92) | |
| CPI score, mean (SD) | N/A | 71.42 (8.41) |
| Time since diagnosis (years), median (IQR) | N/A | 1.17 (0.08–2.79) |
| FEV1 (l), mean (SD) | 3.07 (0.81) | 2.21 (0.56) **** |
| FEV1 (% of predicted), mean (SD) | 100.88 (14.59) | 77.16 (17.08) **** |
| FVC (l), mean (SD) | 4.09 (1.10) | 2.74 (0.78) **** |
| FVC (% of predicted), mean (SD) | 103.97 (14.74) | 72.96 (16.87) **** |
| FEV1/FVC%, mean (SD) | 75.26 (4.83) | 81.67 (7.61) **** |
| TLCO (mmol/min/kPa), median (IQR) | N/A | 3.7 (2.97–4.59) |
| TLCO (% of predicted), mean (SD) | N/A | 49.29 (13.61) |
| 6MWT (meters), mean (SD) | N/A | 378.37 (113.31) |
| Baseline | 12-Months Follow-Up | |||
|---|---|---|---|---|
| Number of subjects | 35 | 35 | ||
| Sex (male/female) | 24/11 | 24/11 | ||
| Age (years), mean (SD) | 68.78 (7.81) | 69.78 (7.81) | ||
| Smoking exposure (pack-years) median (IQR) | 28.00 (0–40.00) | 28.00 (0–40.00) | ||
| Smoking status | ||||
| never smokers, n (%) | 8 (22.86) | 8 (22.86) | ||
| ex-smokers, n (%) | 25 (71.43) | 25 (71.43) | ||
| current smokers, n (%) | 2 (5.71) | 2 (5.71) | ||
| GAP score, median (IQR) | 3.00 (3.00–4.00) | 4.00 (3.00–5.00) *** | ||
| GAP index: | ||||
| Stage I, n (%) | 21 (60.00) | 10 (28.57) | ||
| Stage II, n (%) | 14 (40.00) | 23 (65.71) | ||
| Stage III, n (%) | 0 (0.00) | 2 (5.71) | ||
| CPI score, mean (SD) | 69.69 (7.90) | 74.97 (8.67) **** | ||
| Time since diagnosis (years), median (IQR) | 1.25 (0.17–3.50) | 2.25 (1.17–4.50) **** | ||
| FEV1 (l), mean (SD) | 2.20 (0.58) | 2.11 (0.56) * | ||
| FEV1 (% of predicted), mean (SD) | 78.84 (18.36) | 77.04 (19.50) | ||
| FVC (l), mean (SD) | 2.75 (0.82) | 2.64 (0.78) * | ||
| FVC (% of predicted), mean (SD) | 74.85 (17.93) | 72.98 (18.62) | ||
| FEV1/FVC%, mean (SD) | 81.25 (7.42) | 81.13 (8.03) | ||
| TLCO (mmol/min/kPa), mean (SD) | 4.04 (1.11) | 3.36 (1.18) **** | ||
| TLCO (% of predicted), mean (SD) | 52.58 (12.99) | 43.86 (15.28) **** | ||
| 6MWT (meters), mean (SD) | 389.00 (106.86) | 368.00 (125.22) | ||
| Nintedanib | Pirfenidone | Nintedanib | Pirfenidone | |
| Number of subjects | 10 | 25 | 10 | 25 |
| Sex (male/female) | 7/3 | 17/8 | 7/3 | 17/8 |
| Age (years), mean (SD) | 68.42 (8.64) | 68.92 (7.63) | 69.42 (8.64) | 69.92 (7.63) |
| Smoking exposure (pack-years), median (IQR) | 37.70 (0.00–46.00) | 25.00 (5.50–30.00) | 37.70 (0.00–46.00) | 25.00 (5.50–30.00) |
| Smoking status | ||||
| never smokers, n (%) | 3 (30.00%) | 5 (20.00) | 3 (30.00) | 5 (20.00) |
| ex-smokers, n (%) | 6 (60.00%) | 19 (76.00) | 6 (60.00) | 19 (76.00) |
| current smokers, n (%) | 1 (10.00%) | 1 (4.00) | 1 (10.00) | 1 (4.00) |
| GAP score, median (IQR) | 3.00 (2.00–3.00) | 3.00 (3.00–4.00) | 4.00 (3.00–5.00) *** | 4.00 (3.00–5.00) ** |
| GAP index: | ||||
| Stage I, n (%) | 8 (80.00) | 13 (52.00%) | 3 (30.00) | 7 (28.00) |
| Stage II, n (%) | 2 (20.00) | 12 (48.00%) | 7 (70.00) | 16 (64.00) |
| Stage III, n (%) | 0 (0.00) | 0 (0.00) | 0 (0.00) | 2 (8.00) |
| CPI score, mean (SD) | 71.20 (6.94) | 69.08 (8.31) | 78.20 (6.94) *** | 73.68 (9.07) *** |
| Time since diagnosis (years), median (IQR) | 1.19 (0.17–3.00) | 1.58 (0.33–3.50) | 2.19 (1.17–4.00) ** | 2.58 (1.33–4.50) **** |
| FEV1 (l), mean (SD) | 2.47 (0.44) | 2.10 (0.60) | 2.35 (0.57) | 2.02 (0.54) |
| FEV1 (% of predicted), mean (SD) | 87.00 (15.58) | 75.57 (18.64) | 84.01 (21.01) | 74.26 (18.58) |
| FVC (l), mean (SD) | 3.09 (0.70) | 2.62 (0.84) | 2.92 (0.82) | 2.53 (0.75) |
| FVC (% of predicted), mean (SD) | 83.09 (17.02) | 71.55 (17.53) | 79.33 (21.11) | 70.43 (17.33) |
| FEV1/FVC%, mean (SD) | 80.95 (8.36) | 81.37 (7.20) | 81.43 (9.99) | 81.01 (7.34) |
| TLCO (mmol/min/kPa), mean (SD) | 4.20 (1.19) | 3.98 (1.09) | 3.24 (1.14) *** | 3.40 (1.21) **** |
| TLCO (% of predicted), mean (SD) | 52.68 (10.59) | 52.54 (14.04) | 40.43 (12.58) *** | 45.23 (16.26) *** |
| 6MWT (meters), mean (SD) | 388.20 (72.61) | 389.32 (119.16) | 368.89 (56.74) | 367.68 (143.13) |
| Entire IPF Follow-Up Cohort | Stables | Progressors | |
|---|---|---|---|
| Number of subjects | 35 | 25 | 10 |
| FVC decline per year (l), median (IQR) | 0.09 (−0.04–0.21) | 0.01 (−0.11–0.12) | 0.31 (0.20–0.54) **** |
| FVC decline per year (% of predicted), median (IQR) | 2.01 (−2.10–6.11) | −0.69 (−3.35–2.18) | 6.98 (6.28–13.12) **** |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Majewski, S.; Szewczyk, K.; Białas, A.J.; Miłkowska-Dymanowska, J.; Górski, P.; Piotrowski, W.J. Epithelial Alarmins in Serum and Exhaled Breath in Patients with Idiopathic Pulmonary Fibrosis: A Prospective One-Year Follow-Up Cohort Study. J. Clin. Med. 2019, 8, 1590. https://doi.org/10.3390/jcm8101590
Majewski S, Szewczyk K, Białas AJ, Miłkowska-Dymanowska J, Górski P, Piotrowski WJ. Epithelial Alarmins in Serum and Exhaled Breath in Patients with Idiopathic Pulmonary Fibrosis: A Prospective One-Year Follow-Up Cohort Study. Journal of Clinical Medicine. 2019; 8(10):1590. https://doi.org/10.3390/jcm8101590
Chicago/Turabian StyleMajewski, Sebastian, Karolina Szewczyk, Adam J. Białas, Joanna Miłkowska-Dymanowska, Paweł Górski, and Wojciech J. Piotrowski. 2019. "Epithelial Alarmins in Serum and Exhaled Breath in Patients with Idiopathic Pulmonary Fibrosis: A Prospective One-Year Follow-Up Cohort Study" Journal of Clinical Medicine 8, no. 10: 1590. https://doi.org/10.3390/jcm8101590
APA StyleMajewski, S., Szewczyk, K., Białas, A. J., Miłkowska-Dymanowska, J., Górski, P., & Piotrowski, W. J. (2019). Epithelial Alarmins in Serum and Exhaled Breath in Patients with Idiopathic Pulmonary Fibrosis: A Prospective One-Year Follow-Up Cohort Study. Journal of Clinical Medicine, 8(10), 1590. https://doi.org/10.3390/jcm8101590