Post-Concussion Symptoms in Complicated vs. Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six Months Post-Injury: Results from the CENTER-TBI Study

 , , , , ,
, , , , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Participants
2.3. Measurement-Instrument
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
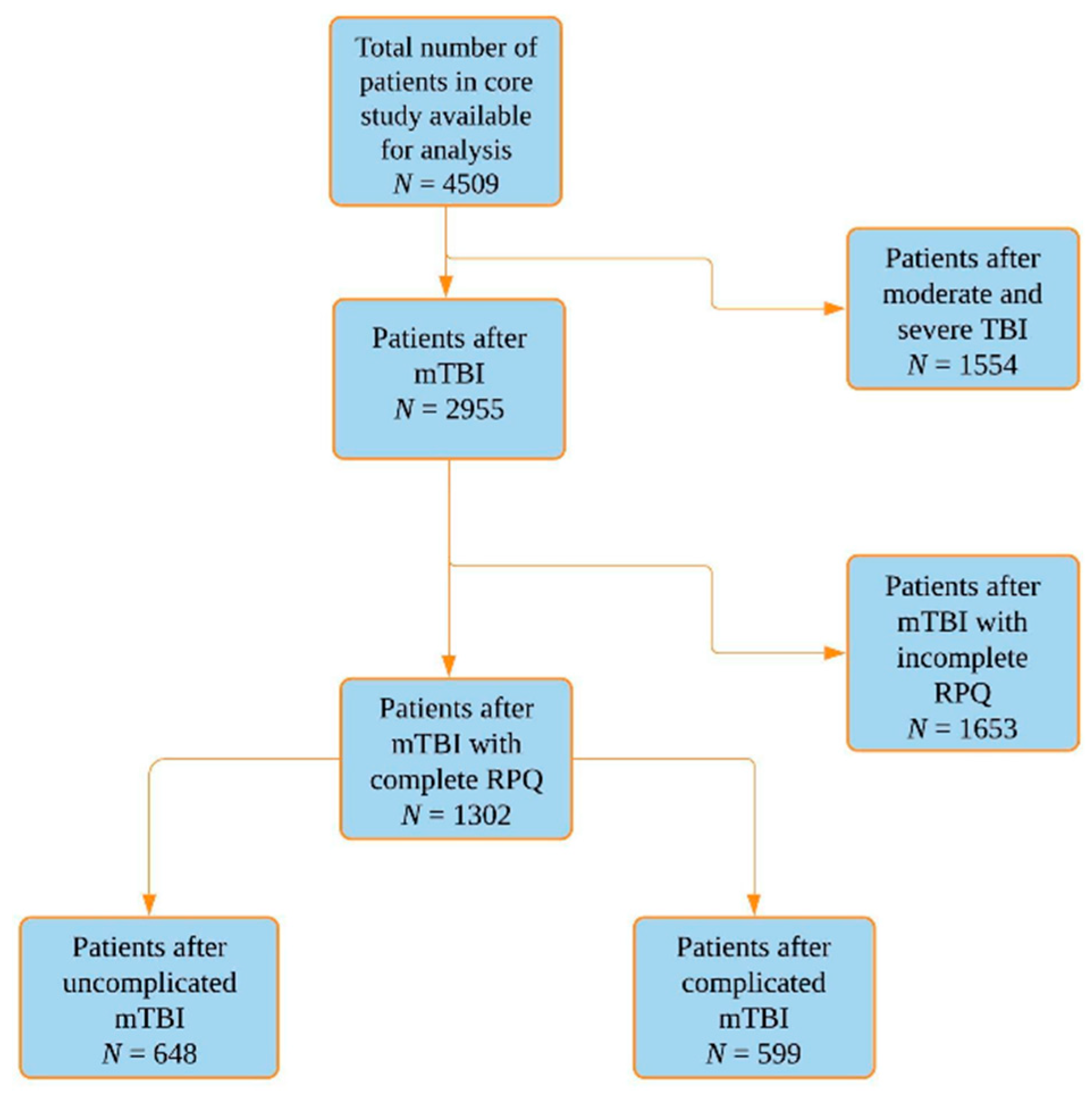
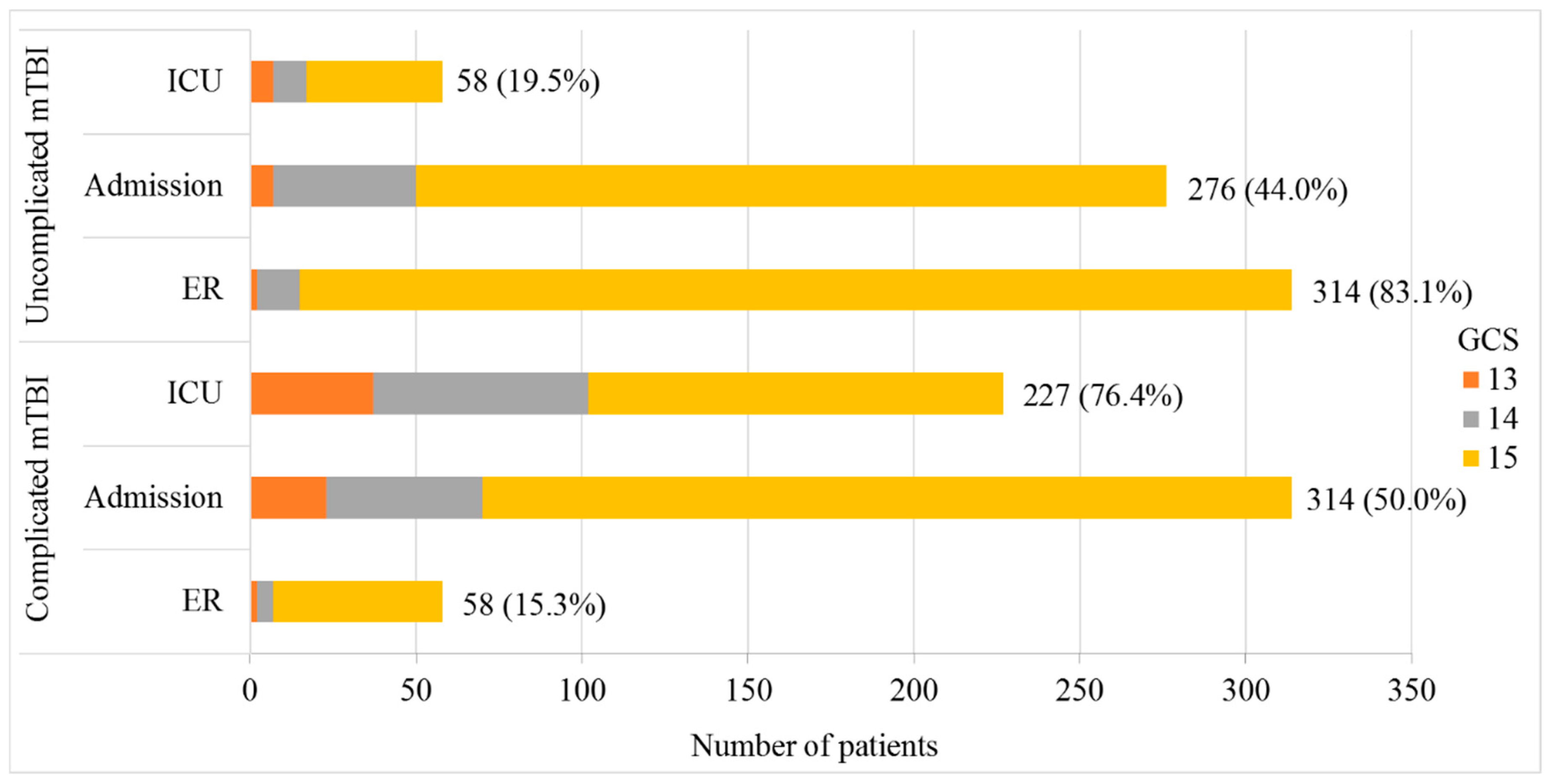
3.1. Study Population
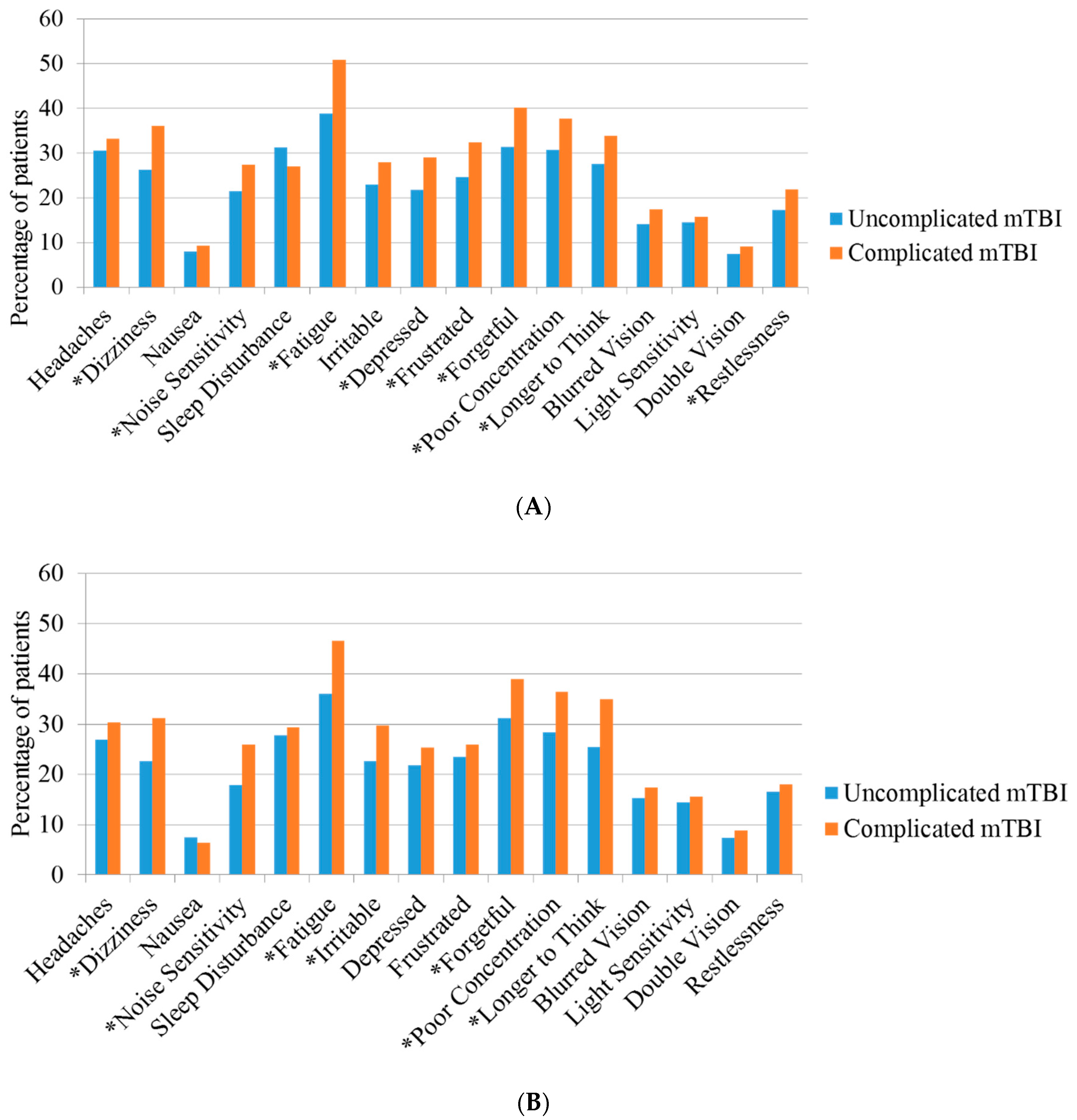
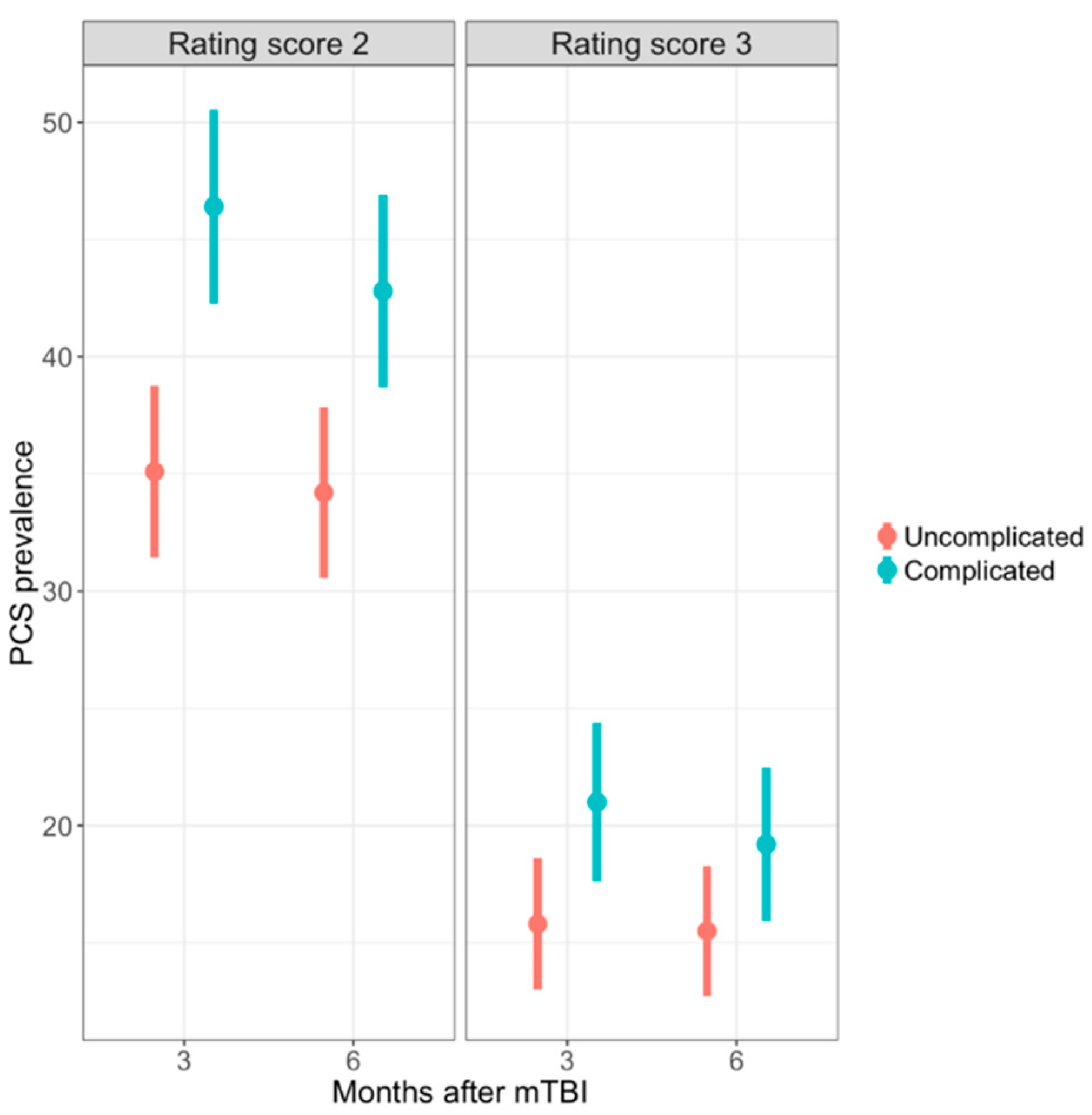
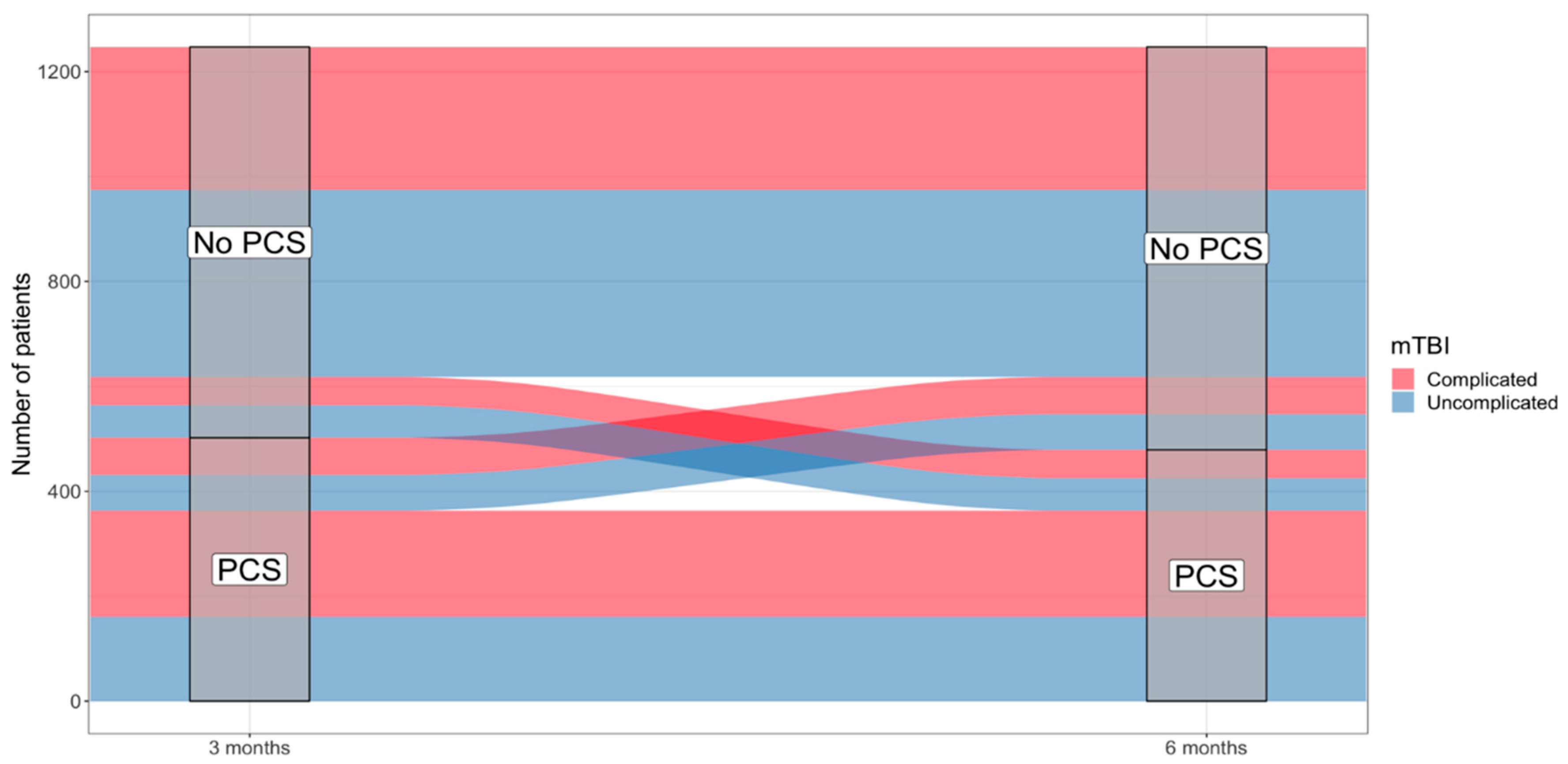
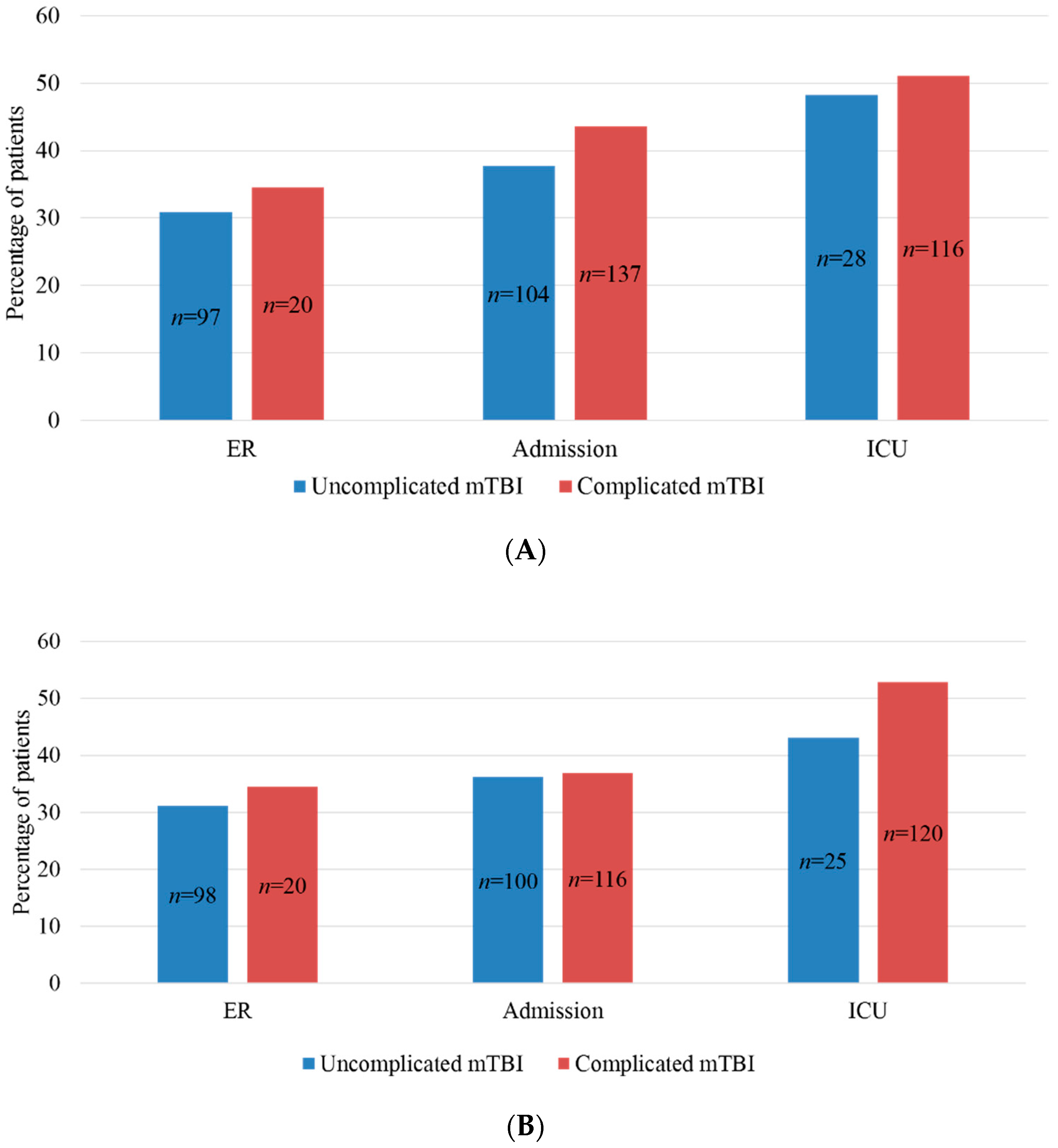
3.2. Post-Concussion Symptoms and PCS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Maas, A.I.R.; Menon, D.K.; Adelson, P.D.; Andelic, N.; Bell, M.J.; Belli, A.; Bragge, P.; Brazinova, A.; Buki, A.; Chesnut, R.M.; et al. Traumatic brain injury: Integrated approaches to improve prevention, clinical care, and research. Lancet Neurol. 2017, 16, 987–1048. [Google Scholar] [CrossRef]
- Williams, D.H.; Levin, H.S.; Eisenberg, H.M. Mild head injury classification. Neurosurgery 1990, 27, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Dikmen, S.; Machamer, J.; Temkin, N. Mild traumatic brain injury: Longitudinal study of cognition, functional status, and post-traumatic symptoms. J. Neurotrauma 2017, 34, 1524–1530. [Google Scholar] [CrossRef] [PubMed]
- Polinder, S.; Cnossen, M.C.; Real, R.G.L.; Covic, A.; Gorbunova, A.; Voormolen, D.C.; Master, C.L.; Haagsma, J.A.; Diaz-Arrastia, R.; von Steinbuechel, N. A multidimensional approach to post-concussion symptoms in mild traumatic brain injury. Front. Neurol. 2018, 9, 1113. [Google Scholar] [CrossRef]
- American Congress of Rehabilitation Medicine. Definition of mild traumatic brain injury. J. Head Trauma Rehabil. 1993, 8, 86–87. [Google Scholar] [CrossRef]
- Gouvier, W.D.; Uddo-Crane, M.; Brown, L.M. Base rates of post-concussional symptoms. Arch. Clin. Neuropsychol. 1988, 3, 273–278. [Google Scholar] [CrossRef]
- Ryan, L.M.; Warden, D.L. Post concussion syndrome. Int. Rev. Psychiatry 2003, 15, 310–316. [Google Scholar] [CrossRef]
- World Health Organization. The Icd-10 Classification of Mental and Behavioural Disorders: Diagnostic Criteria for Research; WHO: Geneva, Switzerland, 1993. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-Iv), 4th ed.; American Psychiatric Association: Washington, DC, USA, 1994. [Google Scholar]
- Katz, D.I.; Cohen, S.I.; Alexander, M.P. Mild traumatic brain injury. Handb. Clin. Neurol. 2015, 127, 131–156. [Google Scholar] [Green Version]
- Evans, R. Persistent post-traumatic headache, postconcussion syndrome, and whiplash injuries: The evidence for a non-traumatic basis with an historical review. Headache 2010, 50, 716–724. [Google Scholar] [CrossRef]
- Evans, R.W. The postconcussion syndrome: 130 years of controversy. Semin. Neurol. 1994, 14, 32–39. [Google Scholar] [CrossRef]
- Binder, L.M. Persisting symptoms after mild head injury: A review of the postconcussive syndrome. J. Clin. Exp. Neuropsychol. 1986, 8, 323–346. [Google Scholar] [CrossRef] [PubMed]
- Leddy, J.J.; Sandhu, H.; Sodhi, V.; Baker, J.G.; Willer, B. Rehabilitation of concussion and post-concussion syndrome. Sports Health 2012, 4, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Spinos, P.; Sakellaropoulos, G.; Georgiopoulos, M.; Stavridi, K.; Apostolopoulou, K.; Ellul, J.; Constantoyannis, C. Postconcussion syndrome after mild traumatic brain injury in western greece. J. Trauma 2010, 69, 789–794. [Google Scholar] [CrossRef] [PubMed]
- King, N.S.; Kirwilliam, S. The nature of permanent post-concussion symptoms after mild traumatic brain injury. Brain Impair. 2013, 14, 235–242. [Google Scholar] [CrossRef]
- Ruff, R.M. Mild traumatic brain injury and neural recovery: Rethinking the debate. NeuroRehabilitation 2011, 28, 167–180. [Google Scholar]
- Hiploylee, C.; Dufort, P.A.; Davis, H.S.; Wennberg, R.A.; Tartaglia, M.C.; Mikulis, D.; Hazrati, L.N.; Tator, C.H. Longitudinal study of postconcussion syndrome: Not everyone recovers. J. Neurotrauma 2017, 34, 1511–1523. [Google Scholar] [CrossRef]
- Smits, M.; Hunink, M.G.M.; van Rijssel, D.A.; Dekker, H.M.; Vos, P.E.; Kool, D.R.; Nederkoorn, P.J.; Hofman, P.A.M.; Twijnstra, A.; Tanghe, H.L.J.; et al. Outcome after complicated minor head injury. Am. J. Neuroradiol. 2008, 29, 506–513. [Google Scholar] [CrossRef]
- McMahon, P.; Hricik, A.; Yue, J.K.; Puccio, A.M.; Inoue, T.; Lingsma, H.F.; Beers, S.R.; Gordon, W.A.; Valadka, A.B.; Manley, G.T.; et al. Symptomatology and functional outcome in mild traumatic brain injury: Results from the prospective track-tbi study. J. Neurotrauma 2014, 31, 26–33. [Google Scholar] [CrossRef]
- Iverson, G.L.; Lange, R.T.; Waljas, M.; Liimatainen, S.; Dastidar, P.; Hartikainen, K.M.; Soimakallio, S.; Ohman, J. Outcome from complicated versus uncomplicated mild traumatic brain injury. Rehabil. Res. Pract. 2012, 2012, 415740. [Google Scholar] [CrossRef]
- McCauley, S.R.; Boake, C.; Levin, H.S.; Contant, C.F.; Song, J.X. Postconcussional disorder following mild to moderate traumatic brain injury: Anxiety, depression, and social support as risk factors and comorbidities. J. Clin. Exp. Neuropsychol. 2001, 23, 792–808. [Google Scholar] [CrossRef]
- Maas, A.I.; Menon, D.K.; Steyerberg, E.W.; Citerio, G.; Lecky, F.; Manley, G.T.; Hill, S.; Legrand, V.; Sorgner, A.; Participants, C.-T.; et al. Collaborative european neurotrauma effectiveness research in traumatic brain injury (center-tbi): A prospective longitudinal observational study. Neurosurgery 2015, 76, 67–80. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.; Wiegers, E.; Sewalt, C.; Maas, A.I. Case-mix, care pathways, and outcomes in patients with traumatic brain injury in center-tbi: A european prospective, multicentre, longitudinal, cohort study. Lancet Neurol. 2019, in press. [Google Scholar] [CrossRef]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.; Wade, D.T. The rivermead post concussion symptoms questionnaire: A measure of symptoms commonly experienced after head injury and its reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Voormolen, D.C.; Cnossen, M.C.; Polinder, S.; von Steinbuechel, N.; Vos, P.E.; Haagsma, J.A. Divergent classification methods of post-concussion syndrome after mild traumatic brain injury: Prevalence rates, risk factors, and functional outcome. J. Neurotrauma 2018, 35, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Plass, A.M.C.; Van Praag, D.; Covic, A.; Gorbunova, A.; Real, R.; von Steinbuechel, N.; Flemish CENTER TBI Investigators. The psychometric validation of the dutch version of the rivermead post-concussion symptoms questionnaire (RPQ) after traumatic brain injury (TBI). Biorxiv 2018. [Google Scholar] [CrossRef] [PubMed]
- Van Buuren, S.; Groothuis-Oudshoorn, K. Mice: Multivariate imputation by chained equations in r. J. Stat. Softw. 2011, 1, 1–68. [Google Scholar] [CrossRef]
- Van Buuren, S. Flexible Imputation of Missing Data; Chapman & Hall/CRC: London, UK, 2012. [Google Scholar]
- Rubin, D.B. Multiple imputation for nonresponse in surveys. Biom. J. 1989, 31, 131–132. [Google Scholar]
- Voormolen, D.C.; Cnossen, M.C.; Polinder, S.; Gravesteijn, B.Y.; Von Steinbuechel, N.; Real, R.G.L.; Haagsma, J.A. Prevalence of post-concussion-like symptoms in the general population in Italy, The Netherlands and the United Kingdom. Brain Inj. 2019, 33, 1–9. [Google Scholar] [CrossRef]
- Iverson, G.L. Network analysis and precision rehabilitation for the post-concussion syndrome. Front. Neurol. 2019, 10, 489. [Google Scholar] [CrossRef]
- Iverson, G.L.; Lange, R.T. Examination of “postconcussion-like” symptoms in a healthy sample. Appl. Neuropsychol. 2003, 10, 137–144. [Google Scholar] [CrossRef]
- Lees-Haley, P.R.; Brown, R.S. Neuropsychological complaint base rates of 170 personal injury claimants. Arch. Clin. Neuropsychol. 1993, 8, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Kay, T.; Newman, B.; Cavallo, M.; Ezrachi, O.; Resnick, M. Toward a neuropsychological model of functional disability after mild traumatic brain injury. Neuropsychology 1992, 6, 371–384. [Google Scholar] [CrossRef]
- Ruff, R.M.; Camenzuli, L.; Mueller, J. Miserable minority: Emotional risk factors that influence the outcome of a mild traumatic brain injury. Brain Inj. 1996, 10, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Iverson, G.L. Complicated vs uncomplicated mild traumatic brain injury: Acute neuropsychological outcome. Brain Inj. 2006, 20, 1335–1344. [Google Scholar] [CrossRef] [PubMed]
- Kondiles, B.R.; Starr, C.R.; Larson, E.B.; Zollman, F. Method of assessment and symptom reporting in veterans with mild traumatic brain injury. Health Psychol. Behav. Med. 2015, 3, 1–11. [Google Scholar] [CrossRef]
- van der Naalt, J.; Hew, J.M.; van Zomeren, A.H.; Sluiter, W.J.; Minderhoud, J.M. Computed tomography and magnetic resonance imaging in mild to moderate head injury: Early and late imaging related to outcome. Ann. Neurol. 1999, 46, 70–78. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total mTBI | Uncomplicated mTBI | Complicated mTBI | |
|---|---|---|---|
| ER N (%) | 826 (97.4%) | 699 (84.6%) | 97 (11.7%) |
| Admission N (%) | 1409 (92.5%) | 686 (48.7%) | 627 (44.5%) |
| ICU N (%) | 720 (33.7%) | 144 (20.0%) | 527 (73.2%) |
| Total | 2955 (65.5%) | 1529 (51.7%) | 1251 (42.3%) |
| Total mTBI with Completed RPQ | Uncomplicated | Complicated | p-Value | |
|---|---|---|---|---|
| N | 1302 | 648 | 599 | |
| Gender (male) | 827 (63.5%) | 398 (61.4%) | 396 (66.1%) | 0.085 |
| Age 1 (years) | 53 (35–66) | 51 (31.25–64) | 58 (39–68) | <0.01 |
| Education 1 (years) | 14 (11–17) | 14 (12–17) | 13 (11–17) | 0.054 |
| Injury Mechanism | 0.394 | |||
| Road traffic accident | 504 (38.7%) | 255 (39.4%) | 227 (37.9%) | |
| Incidental fall | 616 (47.3%) | 300 (46.3%) | 289 (48.2%) | |
| Other non-intentional | 72 (5.5%) | 41 (6.3%) | 29 (4.8%) | |
| Violence/assault | 43 (3.3%) | 22 (3.4%) | 19 (3.2%) | |
| Act of mass violence | 1 (0.1%) | 1 (0.2%) | ||
| Suicide attempt | 7 (0.5%) | 2 (0.3%) | 5 (0.8%) | |
| Other | 42 (3.2%) | 23 (3.5%) | 18 (3.0%) | |
| Unknown | 17 (1.3%) | 5 (0.8%) | 11 (1.8%) | |
| Psychiatric Medical History | 146 (11.2%) | 68 (10.5%) | 73 (12.2%) | 0.329 |
| Anxiety | 36 (24.7%) | 13 (19.1%) | 22 (30.1%) | 0.130 |
| Depression | 89 (61.0%) | 46 (67.6%) | 41 (56.2%) | 0.161 |
| Sleep disorders | 19 (13.0%) | 8 (11.8%) | 10 (13.7%) | 0.731 |
| Schizophrenia | 3 (2.1%) | 1 (1.5%) | 2 (2.7%) | 0.602 |
| Substance abuse disorder | 17 (11.6%) | 5 (7.4%) | 9 (12.3%) | 0.324 |
| Other | 19 (13.0%) | 9 (13.2%) | 9 (12.3%) | 0.872 |
| GCS baseline 1 | 15 (15–15) | 15 (15–15) | 15 (14–15) | <0.01 |
| Computed Tomography | ||||
| Any intracranial injury on first CT | 599 (46.0%) | 648 (0.0%) | 599 (100.0%) | <0.01 |
| RPQ total score 1 | ||||
| 3 months | 6 (0–17) | 4 (0–14) | 7 (2–20) | <0.01 |
| 6 months | 5 (0–15) | 4 (0–14) | 7 (2–17) | <0.01 |
| 3 Months | 6 Months | |||
|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |
| Unadjusted | 1.54 | 1.22–1.94 | 1.39 | 1.10–1.76 |
| Adjusted | 1.25 | 0.95–1.66 | 1.07 | 0.80–1.42 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Voormolen, D.C.; Haagsma, J.A.; Polinder, S.; Maas, A.I.R.; Steyerberg, E.W.; Vuleković, P.; Sewalt, C.A.; Gravesteijn, B.Y.; Covic, A.; Andelic, N.; et al. Post-Concussion Symptoms in Complicated vs. Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six Months Post-Injury: Results from the CENTER-TBI Study. J. Clin. Med. 2019, 8, 1921. https://doi.org/10.3390/jcm8111921
Voormolen DC, Haagsma JA, Polinder S, Maas AIR, Steyerberg EW, Vuleković P, Sewalt CA, Gravesteijn BY, Covic A, Andelic N, et al. Post-Concussion Symptoms in Complicated vs. Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six Months Post-Injury: Results from the CENTER-TBI Study. Journal of Clinical Medicine. 2019; 8(11):1921. https://doi.org/10.3390/jcm8111921
Chicago/Turabian StyleVoormolen, Daphne C., Juanita A. Haagsma, Suzanne Polinder, Andrew I.R. Maas, Ewout W. Steyerberg, Petar Vuleković, Charlie A. Sewalt, Benjamin Y. Gravesteijn, Amra Covic, Nada Andelic, and et al. 2019. "Post-Concussion Symptoms in Complicated vs. Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six Months Post-Injury: Results from the CENTER-TBI Study" Journal of Clinical Medicine 8, no. 11: 1921. https://doi.org/10.3390/jcm8111921
APA StyleVoormolen, D. C., Haagsma, J. A., Polinder, S., Maas, A. I. R., Steyerberg, E. W., Vuleković, P., Sewalt, C. A., Gravesteijn, B. Y., Covic, A., Andelic, N., Plass, A. M., von Steinbuechel, N., & on behalf of the CENTER-TBI Participants and Investigators. (2019). Post-Concussion Symptoms in Complicated vs. Uncomplicated Mild Traumatic Brain Injury Patients at Three and Six Months Post-Injury: Results from the CENTER-TBI Study. Journal of Clinical Medicine, 8(11), 1921. https://doi.org/10.3390/jcm8111921