Optimal Design of Patient-Specific Total Knee Arthroplasty for Improvement in Wear Performance

Abstract
:1. Introduction
2. Material and Methods
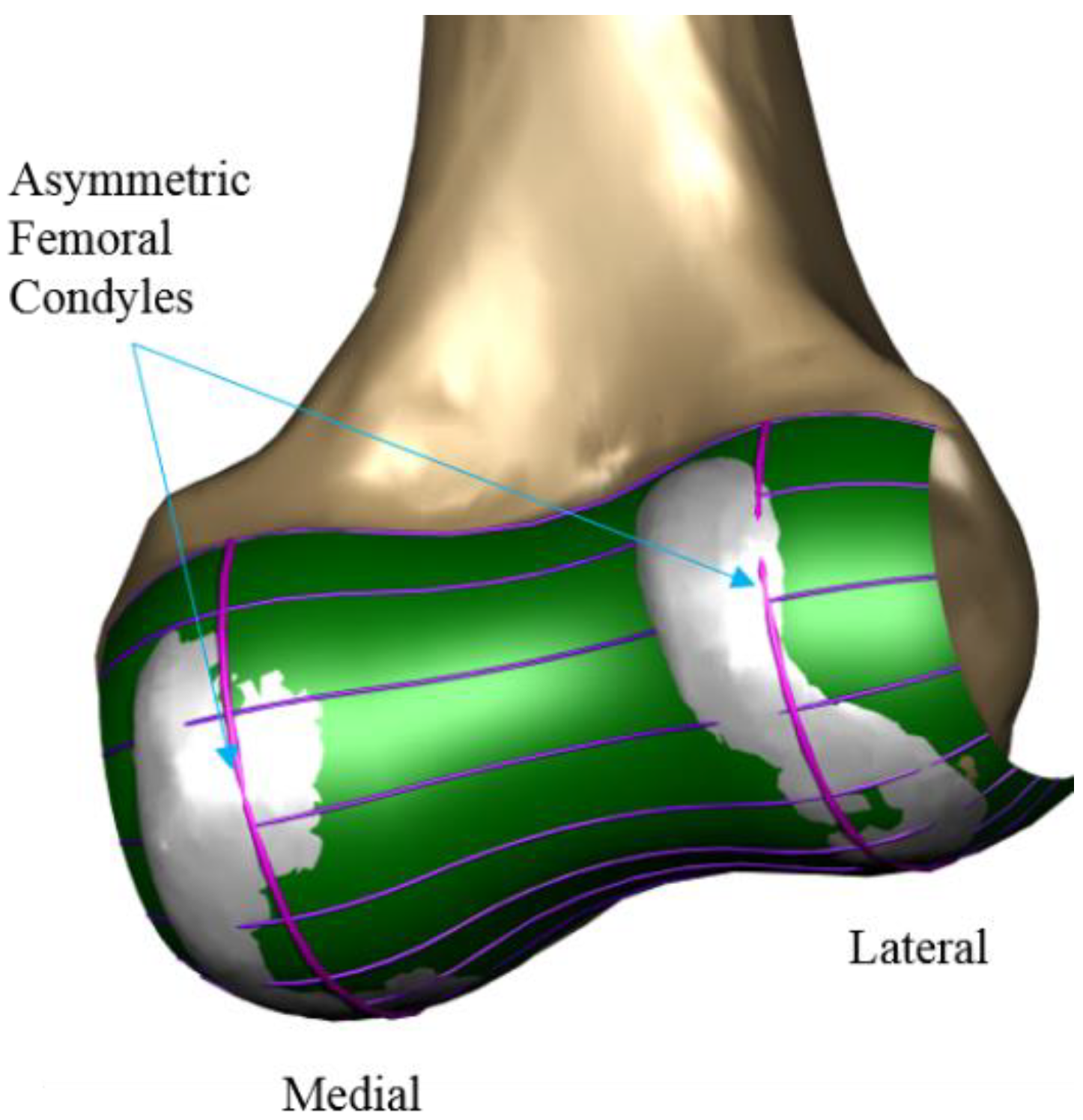
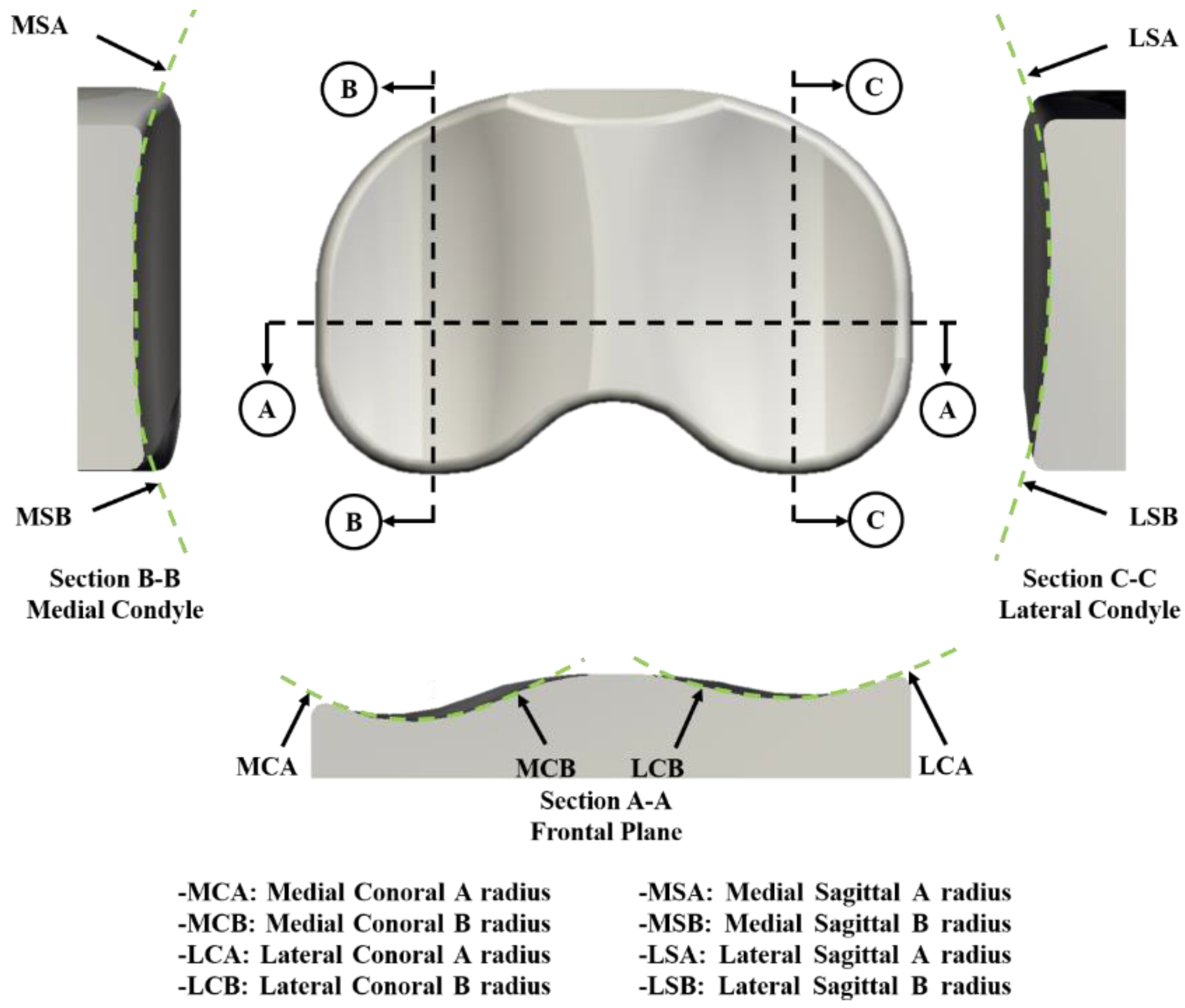
2.1. Design of Patient Specific TKA
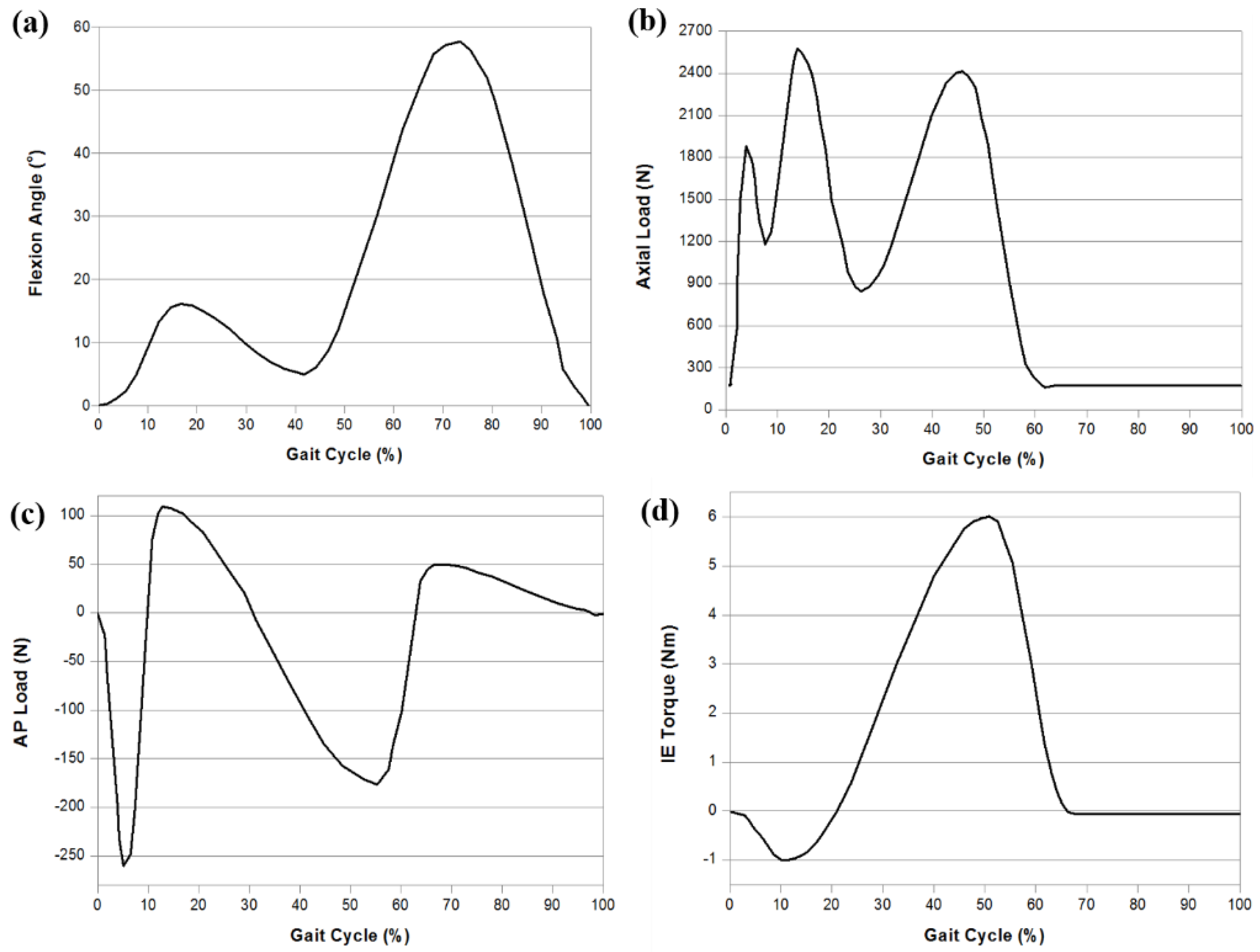
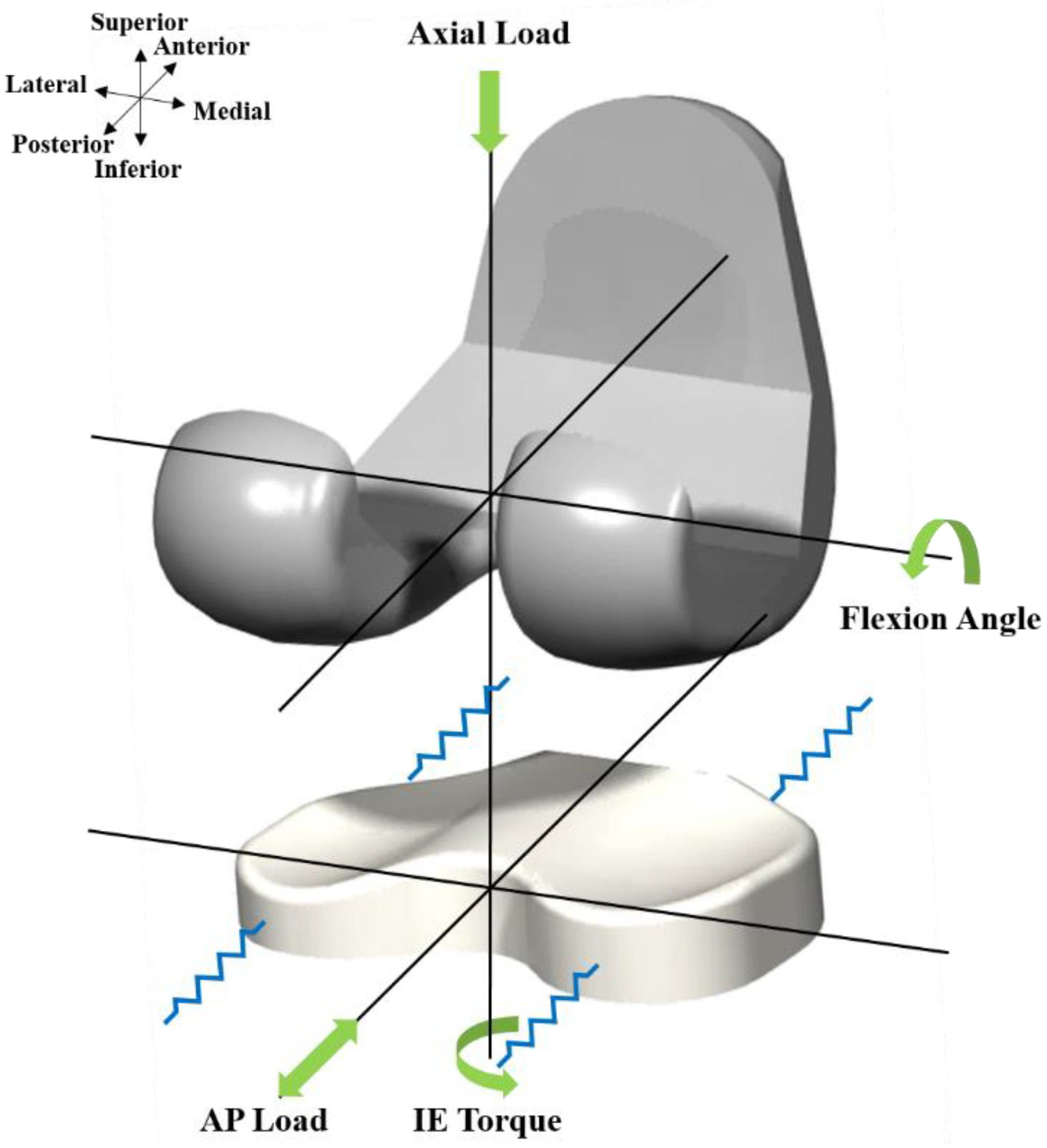
2.2. Development of the Parametric FE Model for Patient-Specific TKA
2.3. Wear Prediction of Patient-Specific TKA
2.4. Design Optimization of Patient Specific TKA
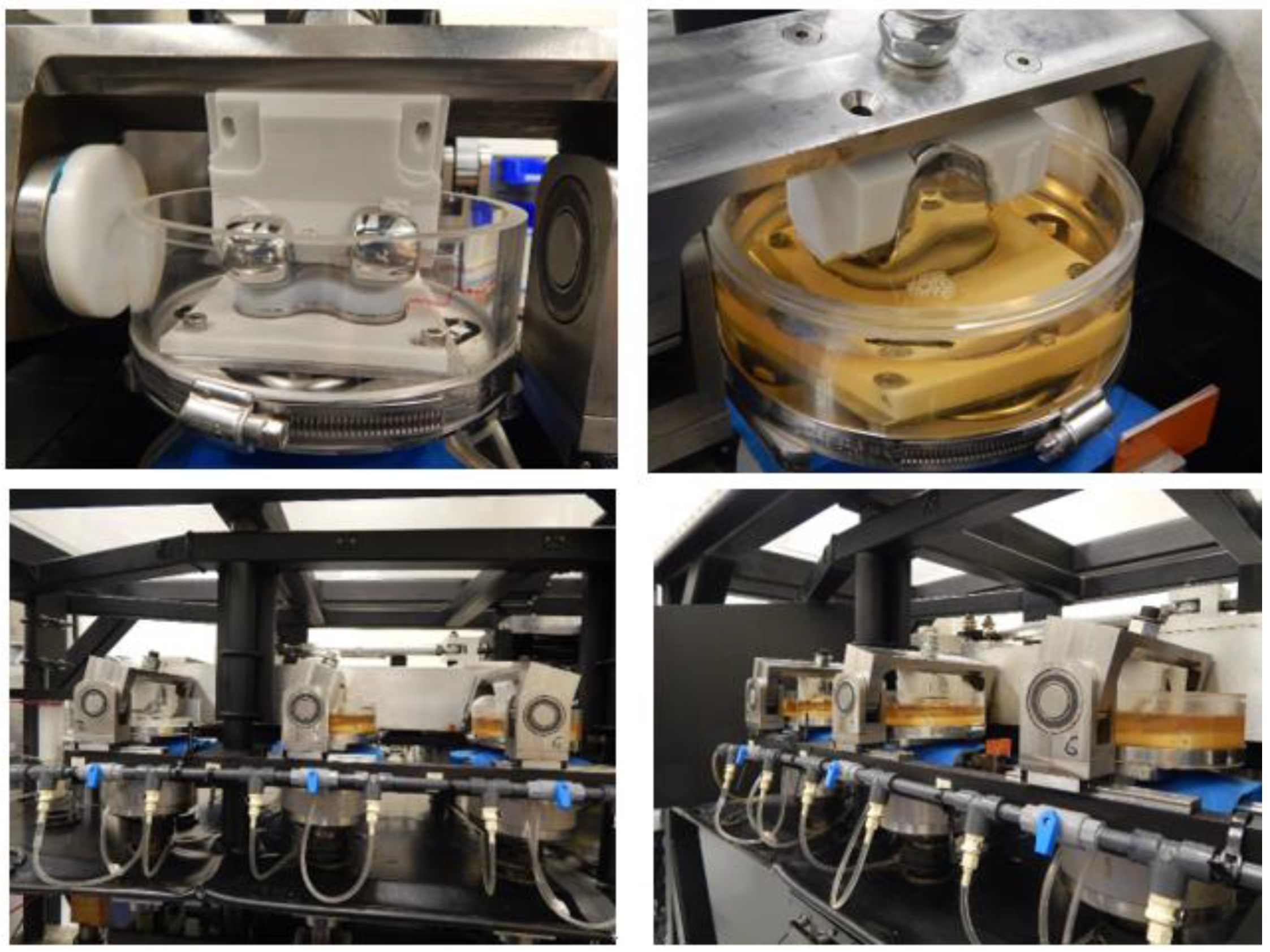
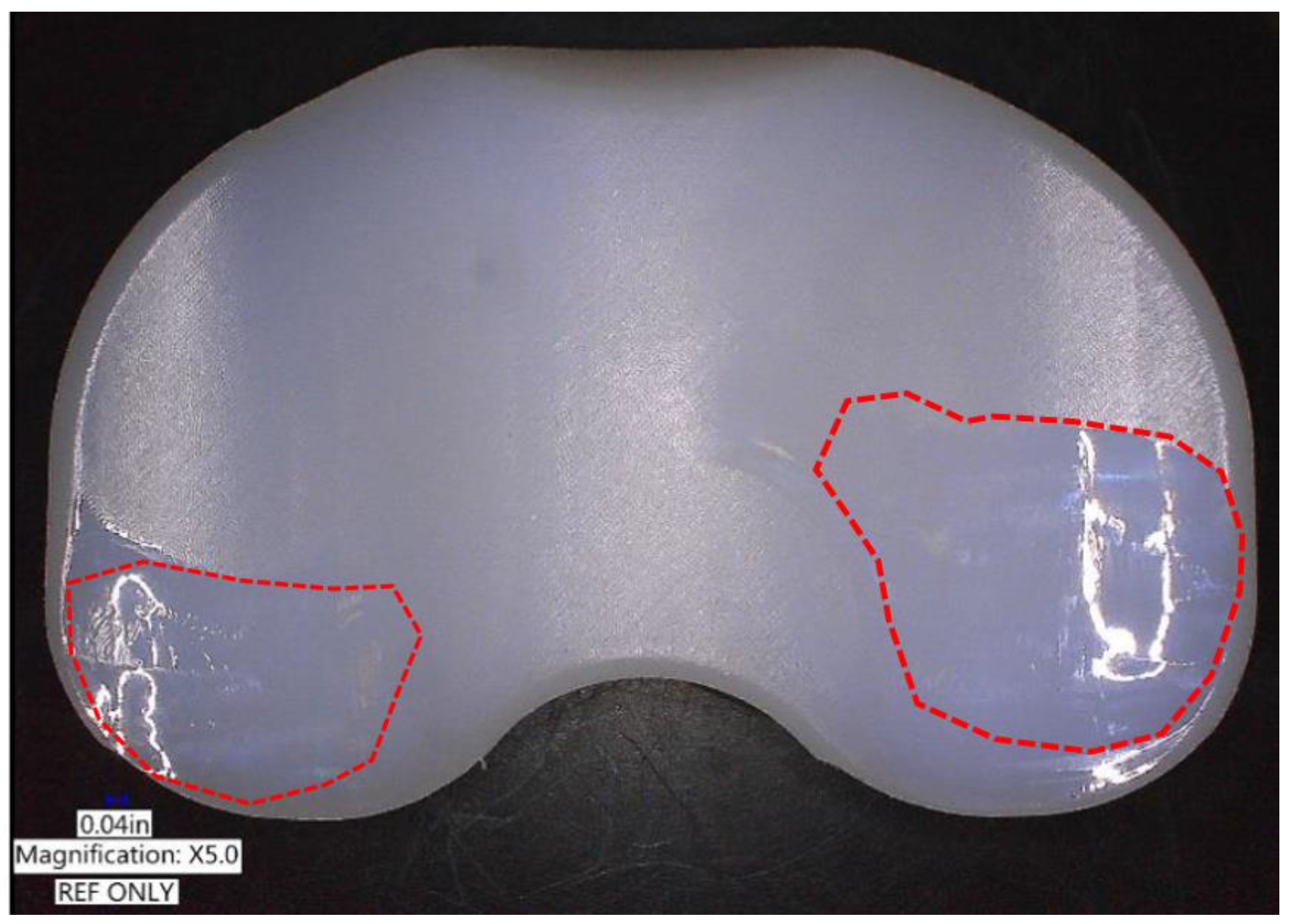
2.5. Experimental Wear Simulation
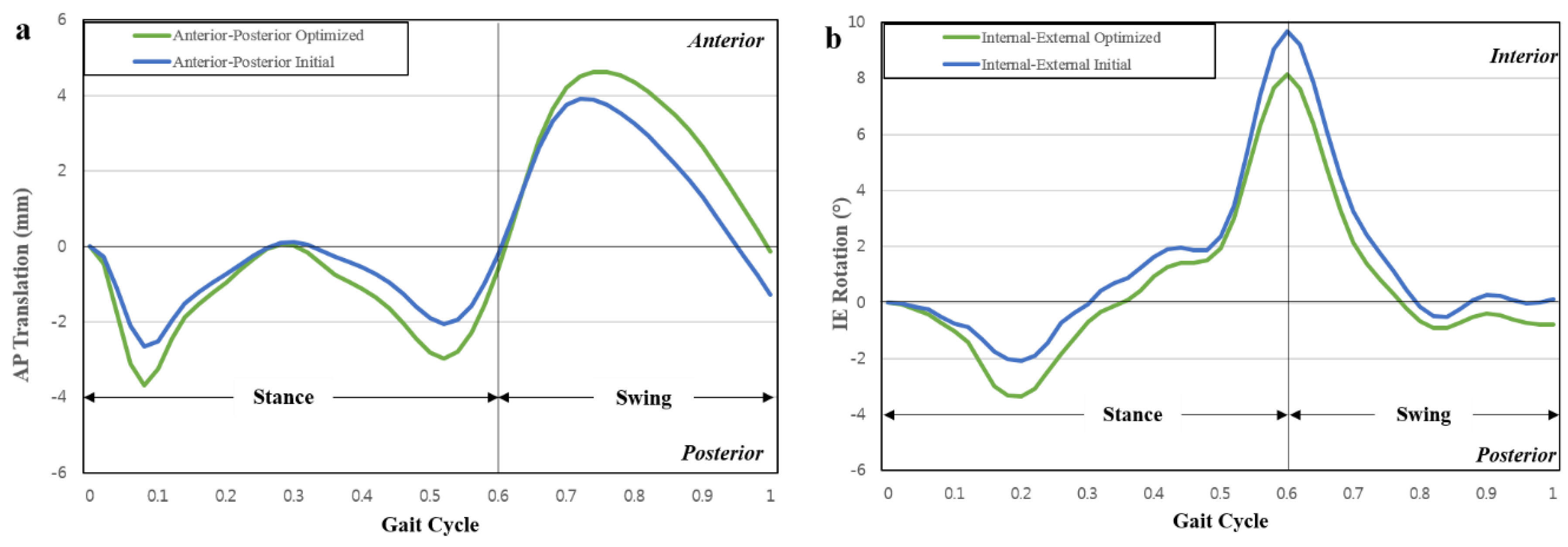
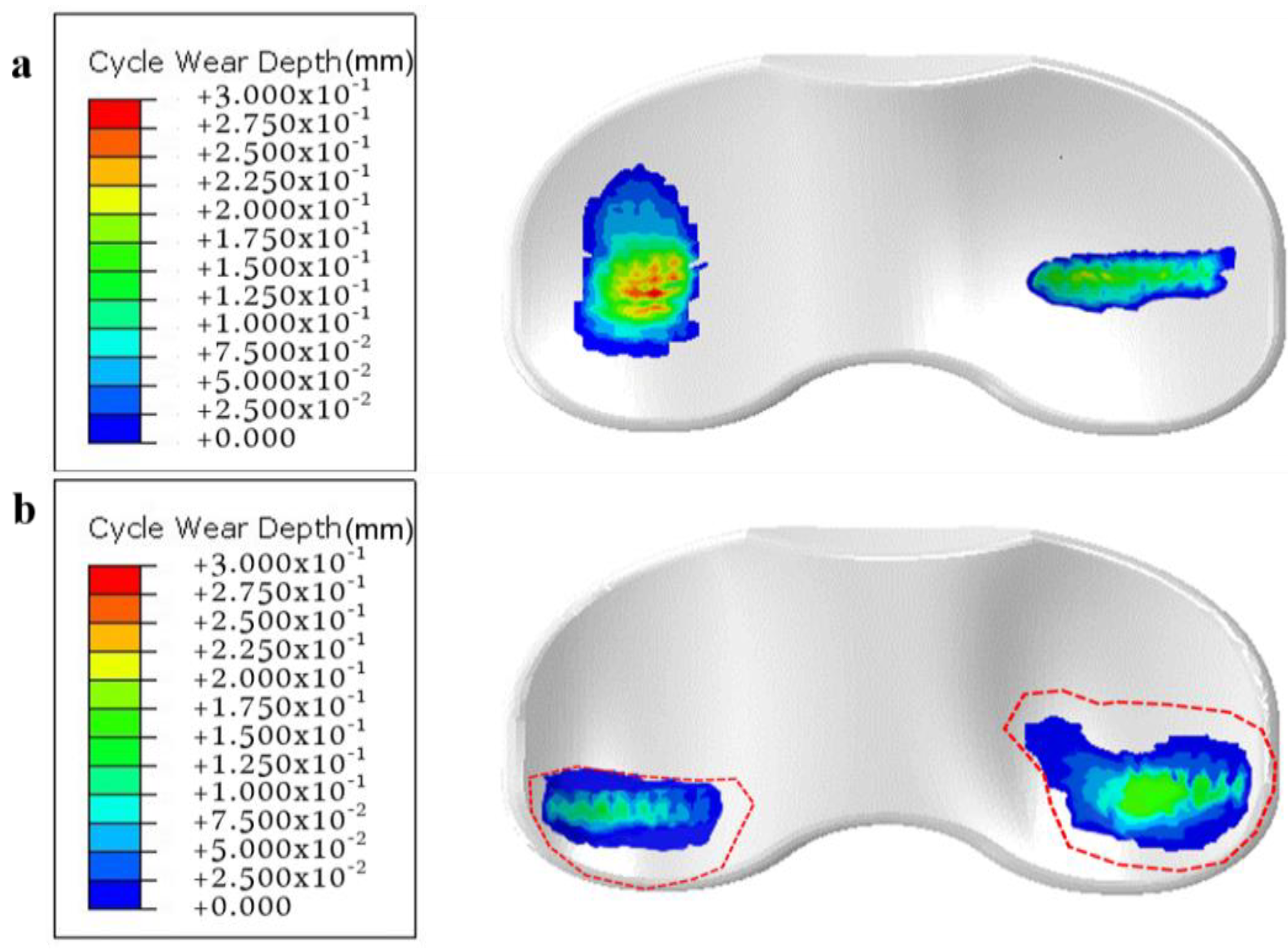
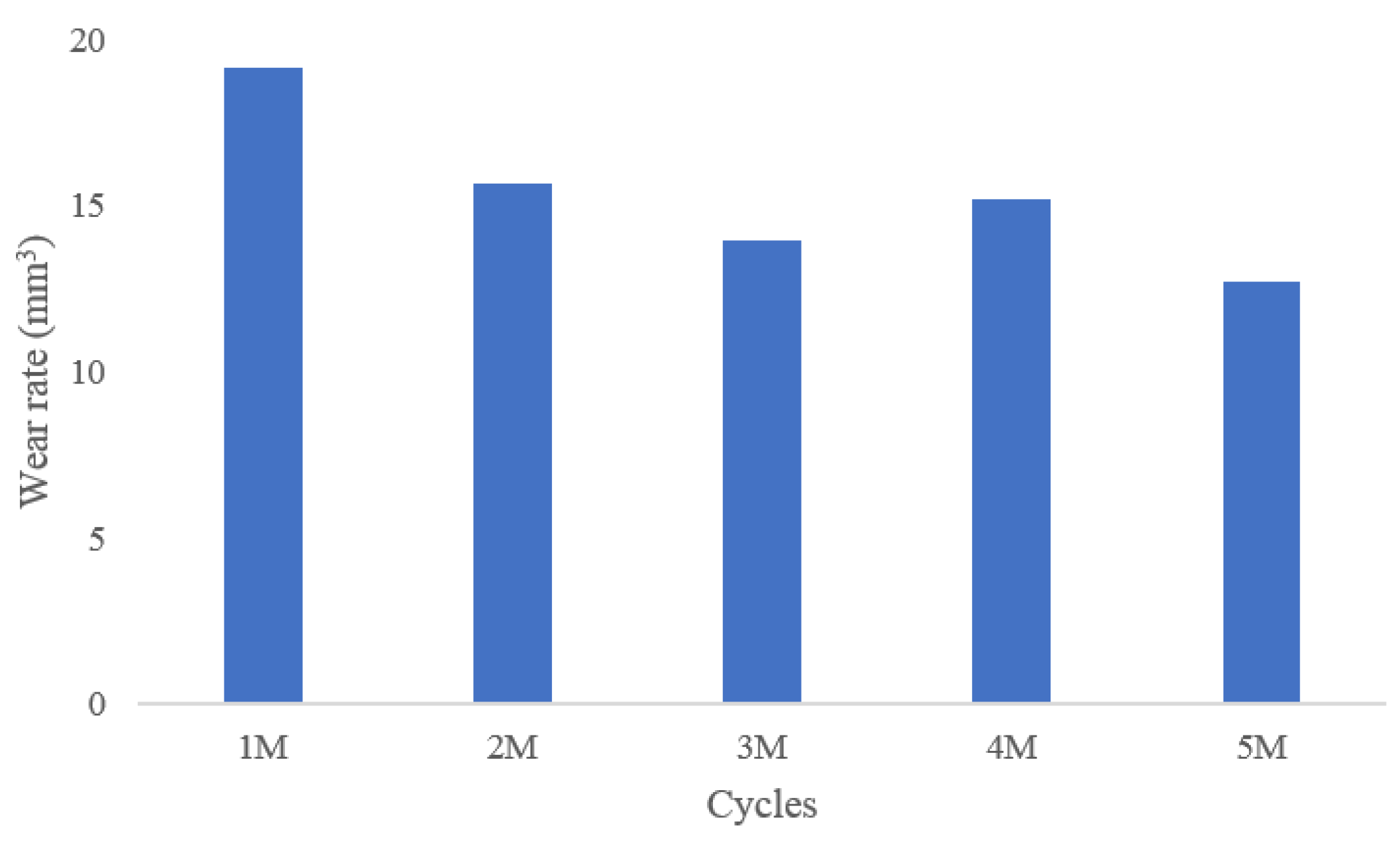
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Noble, J.W., Jr.; Moore, C.A.; Liu, N. The value of patient-matched instrumentation in total knee arthroplasty. J. Arthroplasty 2012, 27, 153–155. [Google Scholar] [CrossRef]
- Brockett, C.L.; Carbone, S.; Fisher, J.; Jennings, L.M. Influence of conformity on the wear of total knee replacement: An experimental study. Proc. Inst. Mech. Eng. H 2018, 232, 127–134. [Google Scholar] [CrossRef]
- Bae, D.K.; Song, S.J.; Park, M.J.; Eoh, J.H.; Song, J.H.; Park, C.H. Twenty-year survival analysis in total knee arthroplasty by a single surgeon. J. Arthroplast. 2012, 27, 1297–1304. [Google Scholar] [CrossRef] [PubMed]
- Von Keudell, A.; Sodha, S.; Collins, J.; Minas, T.; Fitz, W.; Gomoll, A.H. Patient satisfaction after primary total and unicompartmental knee arthroplasty: An age-dependent analysis. Knee 2014, 21, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Naudie, D.D.; Ammeen, D.J.; Engh, G.A.; Rorabeck, C.H. Wear and osteolysis around total knee arthroplasty. J. Am Acad. Orthop. Surg. 2007, 15, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, P.F.; Hozack, W.J.; Rothman, R.H.; Shastri, S.; Jacoby, S.M. Insall Award paper. Why are total knee arthroplasties failing today? Clin. Orthop. Relat. Res. 2002, 7–13. [Google Scholar] [CrossRef] [PubMed]
- White, P.B.; Ranawat, A.S. Patient-Specific Total Knees Demonstrate a Higher Manipulation Rate Compared to “Off-the-Shelf Implants”. J. Arthroplasty 2016, 31, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Bauwens, K.; Matthes, G.; Wich, M.; Gebhard, F.; Hanson, B.; Ekkernkamp, A.; Stengel, D. Navigated total knee replacement. A meta-analysis. J. Bone Jt. Surg. Am. Vol. 2007, 89, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Slover, J.D.; Tosteson, A.N.; Bozic, K.J.; Rubash, H.E.; Malchau, H. Impact of hospital volume on the economic value of computer navigation for total knee replacement. J. Bone Jt. Surg. Am. Vol. 2008, 90, 1492–1500. [Google Scholar] [CrossRef]
- Kwon, O.R.; Kang, K.T.; Son, J.; Suh, D.S.; Heo, D.B.; Koh, Y.G. Patient-specific instrumentation development in TKA: 1st and 2nd generation designs in comparison with conventional instrumentation. Arch. Orthop. Trauma Surg. 2017, 137, 111–118. [Google Scholar] [CrossRef]
- Fitz, W. Unicompartmental knee arthroplasty with use of novel patient-specific resurfacing implants and personalized jigs. J. Bone Jt. Surg. Am. Vol. 2009, 91, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Steklov, N.; Slamin, J.; Srivastav, S.; D’Lima, D. Unicompartmental knee resurfacing: Enlarged tibio-femoral contact area and reduced contact stress using novel patient-derived geometries. Open Biomed. Eng. J. 2010, 4, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Martin, G.; Swearingen, A.; Culler, S. Hospital outcomes and cost for patients undergoing a customized individually made TKA vs off-the-shelf TKA. JISRF Reconstr. Rev. 2014, 4, 103. [Google Scholar]
- Dalury, D.F.; Pomeroy, D.L.; Gorab, R.S.; Adams, M.J. Why are total knee arthroplasties being revised? J. Arthroplast. 2013, 28, 120–121. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, W.B.; Slamin, J.E.; Doody, S.W. Bone Preservation in a Novel Patient Specific Total Knee Replacement. Reconstr. Rev. 2016, 6. [Google Scholar] [CrossRef]
- Bartel, D.L.; Bicknell, V.L.; Wright, T.M. The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components for total joint replacement. J. Bone Jt. Surg. Am. Vol. 1986, 68, 1041–1051. [Google Scholar] [CrossRef]
- Koh, Y.G.; Son, J.; Kwon, O.R.; Kwon, S.K.; Kang, K.T. Tibiofemoral conformity variation offers changed kinematics and wear performance of customized posterior-stabilized total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1213–1223. [Google Scholar] [CrossRef]
- Koh, Y.G.; Park, K.M.; Lee, J.A.; Nam, J.H.; Lee, H.Y.; Kang, K.T. Total knee arthroplasty application of polyetheretherketone and carbon-fiber-reinforced polyetheretherketone: A review. Mater. Sci. Eng. C 2019, 100, 70–81. [Google Scholar] [CrossRef]
- Dargahi, J.; Najarian, S.; Amiri, S. Optimization of the geometry of total knee implant in the sagittal plane using FEA. Biomed. Mater. Eng. 2003, 13, 439–449. [Google Scholar]
- Willing, R.; Kim, I.Y. Three dimensional shape optimization of total knee replacements for reduced wear. Struct. Multidiscip. Optim. 2009, 38, 405–414. [Google Scholar] [CrossRef]
- Kang, K.T.; Koh, Y.G.; Nam, J.H.; Jung, M.; Kim, S.J.; Kim, S.H. Biomechanical evaluation of the influence of posterolateral corner structures on cruciate ligaments forces during simulated gait and squatting. PLoS ONE 2019, 14, e0214496. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.G.; Lee, J.A.; Lee, H.Y.; Chun, H.J.; Kim, H.J.; Kang, K.T. Anatomy-mimetic design preserves natural kinematics of knee joint in patient-specific mobile-bearing unicompartmental knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2019. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.G.; Lee, J.A.; Chung, P.K.; Kang, K.T. Computational analysis of customized cruciate retaining total knee arthroplasty restoration of native knee joint biomechanics. Artif. Organs 2019, 43, 504–514. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.T.; Son, J.; Suh, D.S.; Kwon, S.K.; Kwon, O.R.; Koh, Y.G. Patient-specific medial unicompartmental knee arthroplasty has a greater protective effect on articular cartilage in the lateral compartment: A Finite Element Analysis. Bone Joint Res. 2018, 7, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.G.; Park, K.M.; Lee, H.Y.; Kang, K.T. Influence of tibiofemoral congruency design on the wear of patient-specific unicompartmental knee arthroplasty using finite element analysis. Bone Joint Res. 2019, 8, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Kang, K.T.; Son, J.; Kwon, O.R.; Choi, Y.J.; Jo, S.B.; Choi, Y.W.; Koh, Y.G. Graft Extrusion Related to the Position of Allograft in Lateral Meniscal Allograft Transplantation: Biomechanical Comparison Between Parapatellar and Transpatellar Approaches Using Finite Element Analysis. Arthroscopy 2015, 31, 2380–2391. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.T.; Son, J.; Kim, H.J.; Baek, C.; Kwon, O.R.; Koh, Y.G. Wear predictions for UHMWPE material with various surface properties used on the femoral component in total knee arthroplasty: A computational simulation study. J. Mater. Sci. Mater. Med. 2017, 28, 105. [Google Scholar] [CrossRef]
- Godest, A.C.; Beaugonin, M.; Haug, E.; Taylor, M.; Gregson, P.J. Simulation of a knee joint replacement during a gait cycle using explicit finite element analysis. J. Biomech. 2002, 35, 267–275. [Google Scholar] [CrossRef]
- Walker, P.S.; Lowry, M.T.; Kumar, A. The effect of geometric variations in posterior-stabilized knee designs on motion characteristics measured in a knee loading machine. Clin. Orthop Relat. Res. 2014, 472, 238–247. [Google Scholar] [CrossRef]
- Ardestani, M.M.; Moazen, M.; Jin, Z. Contribution of geometric design parameters to knee implant performance: Conflicting impact of conformity on kinematics and contact mechanics. Knee 2015, 22, 217–224. [Google Scholar] [CrossRef]
- Archard, J.; Hirst, W. The wear of metals under unlubricated conditions. Proc. R. Soc. Lond. A 1956, 236, 397–410. [Google Scholar]
- McGloughlin, T.M.; Murphy, D.M.; Kavanagh, A.G. A machine for the preliminary investigation of design features influencing the wear behaviour of knee prostheses. Proc. Inst. Mech. Eng. H 2004, 218, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Deb, K.; Pratap, A.; Agarwal, S.; Meyarivan, T. A fast and elitist multiobjective genetic algorithm: NSGA-II. IEEE Trans. Evol. Comput. 2002, 6, 182–197. [Google Scholar] [CrossRef]
- Zhang, J.; Zhu, H.; Yang, C.; Li, Y.; Wei, H. Multi-objective shape optimization of helico-axial multiphase pump impeller based on NSGA-II and ANN. Energy Convers. Manag. 2011, 52, 538–546. [Google Scholar] [CrossRef]
- Patil, S.; Bunn, A.; Bugbee, W.D.; Colwell, C.W., Jr.; D’Lima, D.D. Patient-specific implants with custom cutting blocks better approximate natural knee kinematics than standard TKA without custom cutting blocks. Knee 2015, 22, 624–629. [Google Scholar] [CrossRef]
- Abdelgaied, A.; Brockett, C.L.; Liu, F.; Jennings, L.M.; Jin, Z.; Fisher, J. The effect of insert conformity and material on total knee replacement wear. Proc. Inst. Mech. Eng. H 2014, 228, 98–106. [Google Scholar] [CrossRef] [Green Version]
- Luger, E.; Sathasivam, S.; Walker, P.S. Inherent differences in the laxity and stability between the intact knee and total knee replacements. Knee 1997, 4, 7–14. [Google Scholar] [CrossRef]
- Sathasivam, S.; Walker, P.S. The conflicting requirements of laxity and conformity in total knee replacement. J. Biomech. 1999, 32, 239–247. [Google Scholar] [CrossRef]
- Fitzpatrick, C.K.; Clary, C.W.; Laz, P.J.; Rullkoetter, P.J. Relative contributions of design, alignment, and loading variability in knee replacement mechanics. J. Orthop. Res. 2012, 30, 2015–2024. [Google Scholar] [CrossRef]
- Wimmer, M.A.; Laurent, M.P.; Haman, J.D.; Jacobs, J.J.; Galante, J.O. Surface damage versus tibial polyethylene insert conformity: A retrieval study. Clin. Orthop. Relat. Res. 2012, 470, 1814–1825. [Google Scholar] [CrossRef] [Green Version]
- Willing, R.; Kim, I.Y. Quantifying the competing relationship between durability and kinematics of total knee replacements using multiobjective design optimization and validated computational models. J. Biomech. 2012, 45, 141–147. [Google Scholar] [CrossRef] [PubMed]
- DesJardins, J.D.; Walker, P.S.; Haider, H.; Perry, J. The use of a force-controlled dynamic knee simulator to quantify the mechanical performance of total knee replacement designs during functional activity. J. Biomech. 2000, 33, 1231–1242. [Google Scholar] [CrossRef]
- Zhao, D.; Sakoda, H.; Sawyer, W.G.; Banks, S.A.; Fregly, B.J. Predicting knee replacement damage in a simulator machine using a computational model with a consistent wear factor. J. Biomech. Eng. 2008, 130, 011004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fregly, B.J.; Marquez-Barrientos, C.; Banks, S.A.; DesJardins, J.D. Increased conformity offers diminishing returns for reducing total knee replacement wear. J. Biomech. Eng. 2010, 132, 021007. [Google Scholar] [CrossRef] [Green Version]
- Sathasivam, S.; Walker, P.S. Optimization of the bearing surface geometry of total knees. J. Biomech. 1994, 27, 255–264. [Google Scholar] [CrossRef]
- Bei, Y.; Fregly, B.J.; Sawyer, W.G.; Banks, S.A.; Kim, N.H. The relationship between contact pressure, insert thickness, and mild wear in total knee replacements. Comput. Model. Eng. Sci. 2004, 6, 145–152. [Google Scholar]
- Essner, A.; Klein, R.; Bushelow, M.; Wang, A.; Kvitnitsky, M.; Mahoney, O. The effect of sagittal conformity on knee wear. Wear 2003, 255, 1085–1092. [Google Scholar] [CrossRef]
- Blaha, J.D. The rationale for a total knee implant that confers anteroposterior stability throughout range of motion. J. Arthroplasty 2004, 19, 22–26. [Google Scholar] [CrossRef]
- Netter, J.; Hermida, J.; Flores-Hernandez, C.; Steklov, N.; Kester, M.; D’Lima, D.D. Prediction of wear in crosslinked polyethylene unicompartmental knee arthroplasty. Lubricants 2015, 3, 381–393. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Design Variables (mm) | ||||||||
|---|---|---|---|---|---|---|---|---|
| MCA | MCB | MSA | MSB | LCA | LCB | LSA | LSB | |
| Initial | 17.00 | 30.00 | 38.00 | 24.00 | 17.00 | 32.00 | 50.00 | 23.00 |
| Optimal | 18.03 | 33.87 | 39.15 | 25.11 | 18.31 | 34.32 | 52.02 | 24.31 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koh, Y.-G.; Jung, K.-H.; Hong, H.-T.; Kim, K.-M.; Kang, K.-T. Optimal Design of Patient-Specific Total Knee Arthroplasty for Improvement in Wear Performance. J. Clin. Med. 2019, 8, 2023. https://doi.org/10.3390/jcm8112023
Koh Y-G, Jung K-H, Hong H-T, Kim K-M, Kang K-T. Optimal Design of Patient-Specific Total Knee Arthroplasty for Improvement in Wear Performance. Journal of Clinical Medicine. 2019; 8(11):2023. https://doi.org/10.3390/jcm8112023
Chicago/Turabian StyleKoh, Yong-Gon, Kyung-Hwan Jung, Hyoung-Taek Hong, Kang-Min Kim, and Kyoung-Tak Kang. 2019. "Optimal Design of Patient-Specific Total Knee Arthroplasty for Improvement in Wear Performance" Journal of Clinical Medicine 8, no. 11: 2023. https://doi.org/10.3390/jcm8112023
APA StyleKoh, Y. -G., Jung, K. -H., Hong, H. -T., Kim, K. -M., & Kang, K. -T. (2019). Optimal Design of Patient-Specific Total Knee Arthroplasty for Improvement in Wear Performance. Journal of Clinical Medicine, 8(11), 2023. https://doi.org/10.3390/jcm8112023