Fat Mass Index Better Identifies Metabolic Syndrome: Insights from Patients in Early Outpatient Cardiac Rehabilitation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Anthropometric Measurements
2.3. Metabolic Syndrome
2.4. Statistical Methods
3. Results
3.1. Patient Population
3.2. Anthropometrics
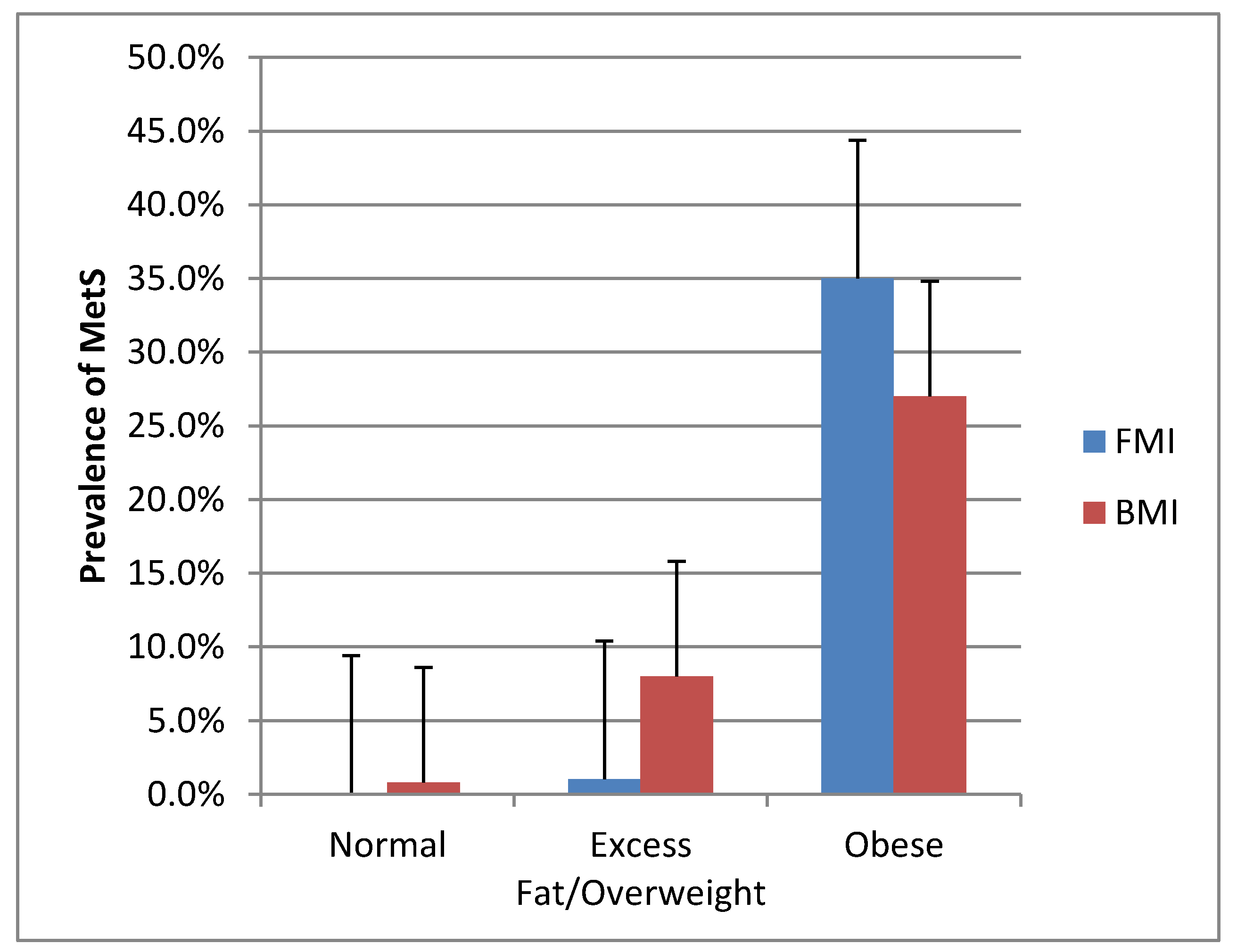
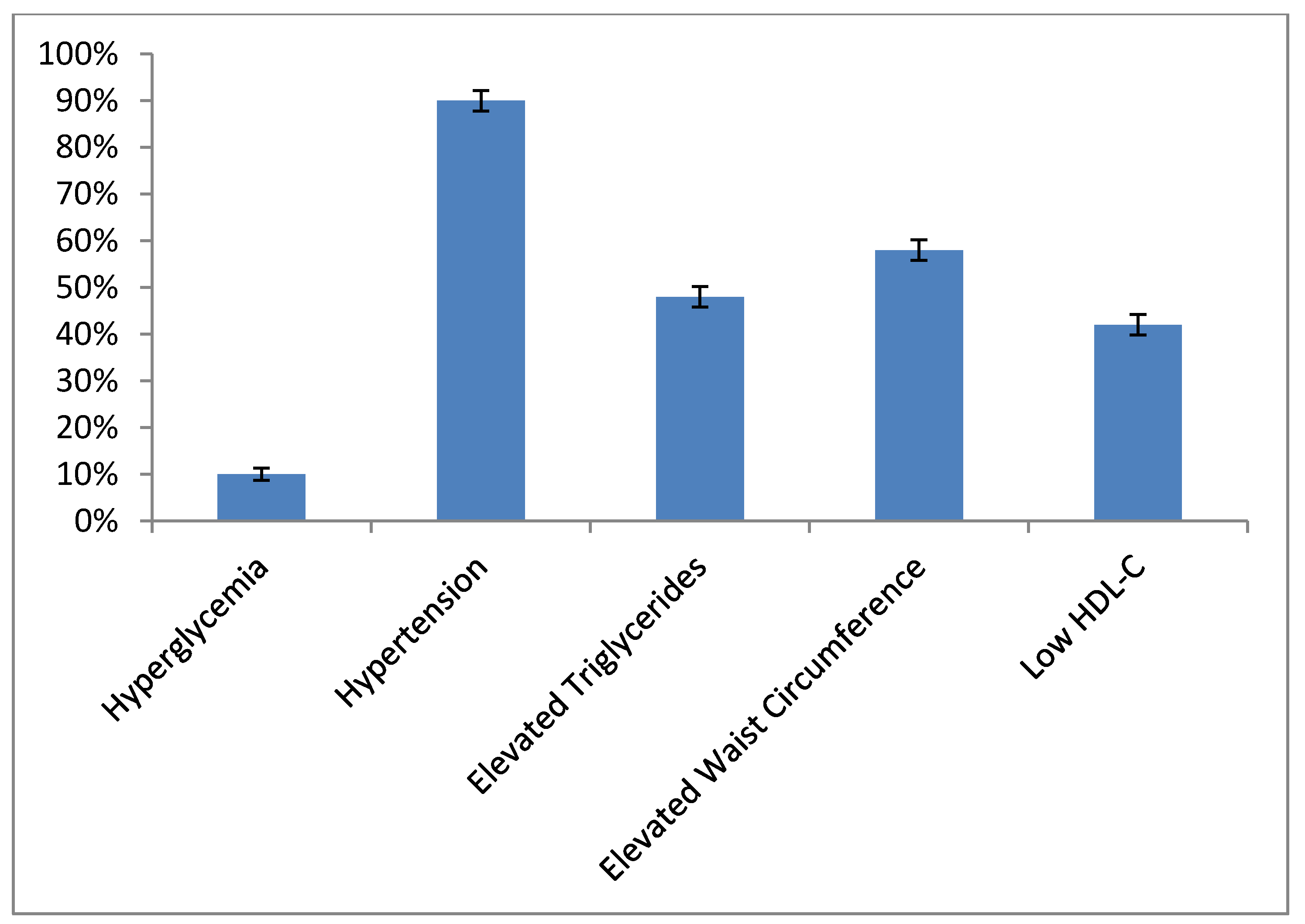
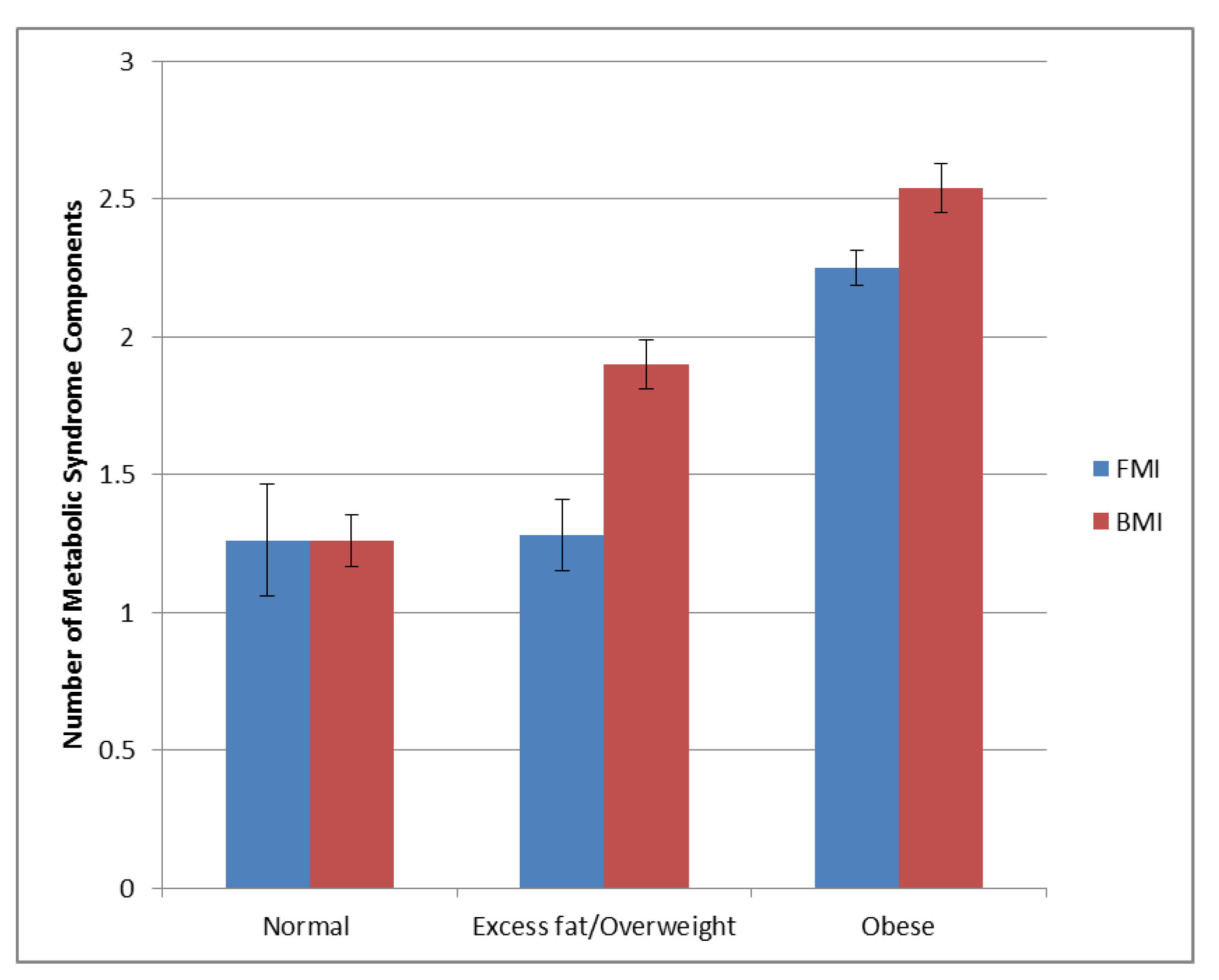
3.3. Metabolic Syndrome
4. Discussion
Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
Abbreviations
| ANOVA | analysis of variance |
| BMI | body mass index |
| CAD | coronary artery disease |
| CR | cardiac rehabilitation |
| DXA | dual-energy x-ray absorptiometry |
| FMI | fat mass index |
| HDL-C | high-density lipoprotein cholesterol |
| MetS | metabolic syndrome |
| MHO | metabolically healthy obese |
References
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.J.; Collazo-Clavell, M.L.; Korinek, J.E.; Allison, T.G.; Batsis, J.A.; Sert-Kuniyoshi, F.H.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. Lond. 2008, 32, 959–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lohman, T.G. Body Composition Methodology in Sports Medicine. Phys. Sportsmed. 1982, 10, 46–58. [Google Scholar] [CrossRef] [PubMed]
- Okorodudu, D.O.; Jumean, M.F.; Montori, V.M.; Romero-Corral, A.; Somers, V.K.; Erwin, P.J.; Lopez-Jimenez, F. Diagnostic performance of body mass index to identify obesity as defined by body adiposity: A systematic review and meta-analysis. Int. J. Obes. Lond. 2010, 34, 791–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Korenfeld, Y.; Boarin, S.; Korinek, J.; Jensen, M.D.; Parati, G.; Lopez-Jimenez, F. Normal weight obesity: A risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur. Heart J. 2010, 31, 737–746. [Google Scholar] [CrossRef]
- Mottillo, S.; Filion, K.B.; Genest, J.; Joseph, L.; Pilote, L.; Poirier, P.; Rinfret, S.; Schiffrin, E.L.; Eisenberg, M.J. The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 1113–1132. [Google Scholar] [CrossRef] [Green Version]
- Karastergiou, K.; Smith, S.R.; Greenberg, A.S.; Fried, S.K. Sex differences in human adipose tissues—The biology of pear shape. Biol. Sex. Differ. 2012, 3, 13. [Google Scholar] [CrossRef] [Green Version]
- Bjørge, T.; Lukanova, A.; Jonsson, H.; Tretli, S.; Ulmer, H.; Manjer, J.; Stocks, T.; Selmer, R.; Nagel, G.; Almquist, M.; et al. Metabolic syndrome and breast cancer in the me-can (metabolic syndrome and cancer) project. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1737–1745. [Google Scholar] [CrossRef] [Green Version]
- Ford, E.S. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: A summary of the evidence. Diabetes Care 2005, 28, 1769–1778. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.H.; Liu, Z.; Ho, S.C. Metabolic syndrome and all-cause mortality: A meta-analysis of prospective cohort studies. Eur. J. Epidemiol. 2010, 25, 375–384. [Google Scholar] [CrossRef]
- Grundy, S.M.; Brewer, H.B., Jr.; Cleeman, J.I.; Smith, S.C., Jr.; Lenfant, C. Definition of metabolic syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association conference on scientific issues related to definition. Circulation 2004, 109, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Expert Panel on Detection E and Treatment of High Blood Cholesterol in A. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Savage, P.D.; Banzer, J.A.; Balady, G.J.; Ades, P.A. Prevalence of metabolic syndrome in cardiac rehabilitation/secondary prevention programs. Am. Heart J. 2005, 149, 627–631. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; Chaudhary, N.; Akinyemiju, T. Metabolic Syndrome Prevalence by Race/Ethnicity and Sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev. Chronic. Dis. 2017, 14, E24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero-Corral, A.; Montori, V.M.; Somers, V.K.; Korinek, J.; Thomas, R.J.; Allison, T.G.; Mookadam, F.; Lopez-Jimenez, F. Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: A systematic review of cohort studies. Lancet 2006, 368, 666–678. [Google Scholar] [CrossRef]
- Medina-Inojosa, J.R.; Somers, V.K.; Thomas, R.J.; Jean, N.; Jenkins, S.M.; Gomez-Ibarra, M.A.; Supervia, M.; Lopez-Jimenez, F. Association between Adiposity and Lean Mass with Long-Term Cardiovascular Events in Patients with Coronary Artery Disease: No Paradox. J. Am. Heart Assoc. 2018, 7, e007505. [Google Scholar] [CrossRef] [Green Version]
- Kelly, T.L.; Wilson, K.E.; Heymsfield, S.B. Dual energy X-Ray absorptiometry body composition reference values from NHANES. PLoS ONE 2009, 4, e7038. [Google Scholar] [CrossRef]
- GE Healthcare. Lunar enCORE Safety and Specification Manual; GE Healthcare: Chicago, IL, USA, 2009. [Google Scholar]
- Garrow, J.S.; Webster, J. Quetelet's index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar]
- National Heart, Lung, Blood Institute; National Institute of Diabetes; Digestive, Kidney Diseases (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 1998. [Google Scholar]
- Beilby, J. Definition of Metabolic Syndrome: Report of the National Heart, Lung, and Blood Institute/American Heart Association Conference on Scientific Issues Related to Definition. Clin. Biochem. Rev. 2004, 25, 195–198. [Google Scholar]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Model. Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Ma, F.; Lou, H.; Liu, Y. The utility of fat mass index vs. body mass index and percentage of body fat in the screening of metabolic syndrome. BMC Public Health 2013, 13, 629. [Google Scholar] [CrossRef] [Green Version]
- Linge, J.; Borga, M.; West, J.; Tuthill, T.; Miller, M.R.; Dumitriu, A.; Thomas, E.L.; Romu, T.; Tunón, P.; Bell, J.D.; et al. Body Composition Profiling in the UK Biobank Imaging Study. Obesity 2018, 26, 1785–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, R.; Zhou, D.; Zhu, Y. The long-term prognosis of cardiovascular disease and all-cause mortality for metabolically healthy obesity: A systematic review and meta-analysis. J. Epidemiol. Community Health 2016, 70, 1024–1031. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Choi, E.K.; Lee, S.H.; Han, K.D.; Rhee, T.M.; Park, C.S.; Lee, S.R.; Choe, W.S.; Lim, W.H.; Kang, S.H.; et al. Atrial fibrillation risk in metabolically healthy obesity: A nationwide population-based study. Int. J. Cardiol. 2017, 240, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Lavie, C.J.; De Schutter, A.; Patel, D.A.; Romero-Corral, A.; Artham, S.M.; Milani, R.V. Body composition and survival in stable coronary heart disease: Impact of lean mass index and body fat in the “obesity paradox”. J. Am. Coll. Cardiol. 2012, 60, 1374–1380. [Google Scholar] [CrossRef] [Green Version]
- Coutinho, T.; Goel, K.; De Sá, D.C.; Carter, R.E.; Hodge, D.O.; Kragelund, C.; Kanaya, A.M.; Zeller, M.; Park, J.S.; Kober, L.; et al. Combining body mass index with measures of central obesity in the assessment of mortality in subjects with coronary disease: Role of “normal weight central obesity”. J. Am. Coll. Cardiol. 2013, 61, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Heitmann, B.L.; Erikson, H.; Ellsinger, B.M.; Mikkelsen, K.L.; Larsson, B. Mortality associated with body fat, fat-free mass and body mass index among 60-year-old swedish men-a 22-year follow-up. The study of men born in 1913. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 33–37. [Google Scholar] [CrossRef] [Green Version]
- Lin, H.; Zhang, L.; Zheng, R.; Zheng, Y. The prevalence, metabolic risk and effects of lifestyle intervention for metabolically healthy obesity: A systematic review and meta-analysis: A PRISMA-compliant article. Med. Baltim. 2017, 96, e8838. [Google Scholar] [CrossRef]
- Caleyachetty, R.; Thomas, G.N.; Toulis, K.A.; Mohammed, N.; Gokhale, K.M.; Balachandran, K.; Nirantharakumar, K. Metabolically Healthy Obese and Incident Cardiovascular Disease Events Among 3.5 Million Men and Women. J. Am. Coll. Cardiol. 2017, 70, 1429–1437. [Google Scholar] [CrossRef]
- Eckel, N.; Meidtner, K.; Kalle-Uhlmann, T.; Stefan, N.; Schulze, M.B. Metabolically healthy obesity and cardiovascular events: A systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2016, 23, 956–966. [Google Scholar] [CrossRef]
- Milani, R.V.; Lavie, C.J. Prevalence and profile of metabolic syndrome in patients following acute coronary events and effects of therapeutic lifestyle change with cardiac rehabilitation. Am. J. Cardiol. 2003, 92, 50–54. [Google Scholar] [CrossRef]
- Solymoss, B.C.; Bourassa, M.G.; Lespérance, J.; Levesque, S.; Marcil, M.; Varga, S.; Campeau, L. Incidence and clinical characteristics of the metabolic syndrome in patients with coronary artery disease. Coron. Artery Dis. 2003, 14, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity Among Adults and Youth: United States, 2015–2016. NCHS Data Brief 2017, 288, 1–8. [Google Scholar]
- Wang, J.; Sarnola, K.; Ruotsalainen, S.; Moilanen, L.; Lepistö, P.; Laakso, M.; Kuusisto, J. The metabolic syndrome predicts incident congestive heart failure: A 20-year follow-up study of elderly Finns. Atherosclerosis 2010, 210, 237–242. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Normal | Overweight | Obese | All | p-Value | |
|---|---|---|---|---|---|
| n (%) | 93 (19%) | 174 (36%) | 216 (45%) | 483 (100%) | |
| Age, years | 63 ± 16 | 66 ± 13 | 63 ± 13 | 64 ± 14 | 0.0416 * |
| Height, cm | 169 ± 9 | 171 ± 9 | 172 ± 9 | 171 ± 9 | 0.1457 |
| Weight, kg | 64 ± 9 | 80 ± 11 | 103 ± 16 | 87 ± 20 | <0.0001 * |
| Body mass index | 22 ± 2 | 27 ± 2 | 35 ± 4 | 30 ± 6 | <0.0001 * |
| Female | 34 (37%) | 44 (25%) | 64 (30%) | 142 (29%) | 0.1597 |
| Waist, cm | 86 ± 8 | 98 ± 8 | 116 ± 11 | 104 ± 15 | <0.0001 * |
| Hip, cm | 95 ± 5 | 103 ± 5 | 116 ± 10 | 107 ± 12 | <0.0001 * |
| Resting Blood pressure | |||||
| Systolic, mmHg | 120 ± 22 | 118 ± 18 | 120 ± 16 | 120 ± 19 | 0.2164 |
| Diastolic, mmHg | 67 ± 12 | 68 ± 12 | 69 ± 12 | 68 ± 12 | 0.0462 * |
| DXA Variables | |||||
| Total body mass, kg | 65 ± 9 | 80 ± 10 | 103 ± 16 | 87 ± 20 | <0.0001 * |
| Total fat mass, kg | 20 ± 14 | 26 ± 6 | 42 ± 10 | 32 ± 13 | <0.0001 * |
| Total lean mass, kg | 45 ± 7 | 50 ± 8 | 57 ± 10 | 53 ± 10 | <0.0001 * |
| Body fat, % | 27 ± 7 | 34 ± 6 | 42 ± 7 | 36 ± 8 | <0.0001 * |
| Trunk | |||||
| Total mass, kg | 32 ± 5 | 41 ± 6 | 54 ± 9 | 45 ± 12 | <0.0001 * |
| Fat mass, kg | 9 ± 3 | 15 ± 3 | 26 ± 7 | 19 ± 8 | <0.0001 * |
| Lean mass, kg | 22 ± 3 | 24 ± 4 | 27 ± 5 | 25 ± 5 | <0.0001 * |
| Fat % | 29 ± 9 | 39 ± 6 | 49 ± 6 | 41 ± 10 | <0.0001 * |
| Android | |||||
| Total mass, kg | 5 ± 1 | 6 ± 1 | 9 ± 2 | 7 ± 2 | <0.0001 * |
| Fat mass, kg | 1.4 ± 0.7 | 2.7 ± 0.7 | 4.7 ± 1.3 | 3.3 ± 1.7 | <0.0001 * |
| Lean mass, kg | 3.3 ± 0.6 | 3.7 ± 0.7 | 4.3 ± 0.9 | 3.9 ± 0.9 | <0.0001 * |
| Fat % | 29 ± 11 | 41 ± 7 | 52 ± 7 | 44 ± 11 | <0.0001 * |
| Gynoid | |||||
| Total mass, kg | 9 ± 1 | 11 ± 2 | 15 ± 3 | 13 ± 3 | <0.0001 * |
| Fat mass, kg | 3 ± 0.9 | 4 ± 1 | 7 ± 7 | 5 ± 5 | <0.0001 * |
| Lean mass, kg | 6 ± 1 | 7 ± 1 | 8 ± 1 | 8± 2 | <0.0001 * |
| Fat % | 30 ± 8 | 35 ± 7 | 42 ± 8 | 37 ± 9 | <0.0001 * |
| Other Characteristics | |||||
| Metabolic syndrome | 4 (4%) | 39 (22%) | 129 (60%) | 172 (36%) | <0.0001 * |
| Current smoker | 5 (5%) | 13 (7%) | 11 (5%) | 29 (6%) | 0.4653 |
| Hyperglycemia | 6 (6%) | 11 (6%) | 32 (15%) | 49 (10%) | 0.0093 * |
| Dyslipidemia | 20 (21%) | 87 (50%) | 126 (58%) | 233 (48%) | <0.0001 * |
| Hypertension | 87 (93%) | 159 (91%) | 190 (88%) | 436 (90%) | 0.2521 |
| Low HDL | 17 (18%) | 75 (43%) | 113 (52%) | 205 (42%) | <0.0001 * |
| Hypertriglyceridemia | 20 (21%) | 87 (50%) | 126 (58%) | 233 (48%) | <0.0001 * |
| Elevated waist | 5 (5%) | 75 (43%) | 200 (93%) | 280 (58%) | <0.0001 * |
| Medications | |||||
| ASA | 77 (83%) | 154 (88%) | 188 (87%) | 419 (87%) | 0.4331 |
| Plavix | 36 (39%) | 80 (46%) | 112 (52%) | 228 (47%) | 0.0955 |
| Beta blocker | 70 (75%) | 145 (83%) | 191 (88%) | 406 (84%) | 0.0170 * |
| ACE/ARB | 36 (39%) | 78 (45%) | 121 (56%) | 235 (49%) | 0.0089 * |
| Statin | 66 (71%) | 147 (85%) | 185 (86%) | 398 (82%) | 0.0086 * |
| CR Reasons | |||||
| Angina/CAD | 3 (3%) | 10 (6%) | 13 (6%) | 26 (5%) | 0.0569 |
| CABG | 11 (12%) | 24 (14%) | 34 (16%) | 69 (14%) | 0.3565 |
| CHF | 4 (4%) | 9 (5%) | 11 (5%) | 24 (5%) | 0.3565 |
| NSTEMI | 13 (14%) | 29 (17%) | 30 (14%) | 72 (15%) | 0.3565 |
| Other | 6 (6%) | 8 (5%) | 9 (4%) | 23 (5%) | 0.3565 |
| PAD | 0 (0%) | 0 (0%) | 1 (0.5%) | 1 (0.2%) | 0.3565 |
| PCI | 16 (17%) | 36 (21%) | 62 (29%) | 114 (24%) | 0.3565 |
| STEMI | 15 (16%) | 26 (15%) | 25 (12%) | 66 (14%) | 0.3565 |
| Ventricular assist device | 8 (9%) | 9 (5%) | 4 (2%) | 21 (4%) | 0.3565 |
| Valve disease | 17 (18%) | 23 (13%) | 27 (12%) | 67 (14%) | 0.3565 |
| Normal | Excess Fat | Obese | All | p-Value | |
|---|---|---|---|---|---|
| n (%) | 15 (3%) | 74 (15%) | 394 (81%) | 483 (100%) | |
| Age, years | 53 ± 19 | 60 ± 14 | 62 ± 12 | 61 ± 13 | 0.1014 |
| Height, cm | 170 ± 8 | 172 ± 10 | 171 ± 9 | 171 ± 9 | 0.6024 |
| Weight, kg | 60 ± 11 | 73 ± 14 | 91 ± 20 | 87 ± 20 | <0.0001 * |
| Body mass index | 21 ± 3 | 25 ± 4 | 31 ± 5 | 30 ± 6 | <0.0001 * |
| Female | 6 (40%) | 23 (31%) | 113 (29%) | 142 (29%) | 0.6173 |
| Waist, cm | 80 ± 9 | 90 ± 10 | 107 ± 14 | 104 ± 15 | <0.0001 * |
| Hip, cm | 92 ± 7 | 99 ± 7 | 110 ± 11 | 107 ± 12 | <0.0001 * |
| Resting Blood pressure | |||||
| Systolic, mmHg | 117 ± 15 | 117 ± 17 | 123 ± 20 | 122 ± 20 | 0.1397 |
| Diastolic, mmHg | 72 ± 11 | 70 ± 9 | 71 ± 14 | 71 ± 14 | 0.8213 |
| DXA Variables | |||||
| Total body mass, kg | 60 ± 11 | 73 ± 14 | 91 ± 19 | 87 ± 20 | <0.0001 * |
| Total fat mass, kg | 21 ± 29 | 21 ± 10 | 35 ± 12 | 32 ± 13 | <0.0001 * |
| Total lean mass, kg | 48 ± 9 | 51 ± 10 | 53 ± 10 | 53 ± 10 | 0.0474 * |
| Body fat, % | 17 ± 4 | 28 ± 6 | 39 ± 7 | 37 ± 9 | <0.0001 * |
| Trunk | |||||
| Total mass, kg | 29 ± 5 | 37 ± 8 | 48 ± 11 | 45 ± 12 | <0.0001 * |
| Fat mass, kg | 4 ± 2 | 11 ± 5 | 21 ± 7 | 19 ± 8 | <0.0001 * |
| Lean mass, kg | 23 ± 4 | 25 ± 4 | 25 ± 5 | 25 ± 5 | 0.3245 |
| Fat % | 15 ± 4 | 30 ± 8 | 45 ± 7 | 41 ± 10 | <0.0001 * |
| Android | |||||
| Total mass, kg | 4 ± 1 | 6 ± 1 | 8 ± 2 | 7 ± 2 | <0.0001 * |
| Fat mass, kg | 0.5 ± 0.3 | 2 ± 0.8 | 4 ± 1 | 3 ± 2 | <0.0001 * |
| Lean mass, kg | 4 ± 0.8 | 4 ± 0.8 | 4 ± 0.9 | 4 ± 0.9 | 0.1473 |
| Fat % | 13 ± 4 | 30 ± 9 | 47 ± 8 | 44 ± 11 | <0.0001 * |
| Gynoid | |||||
| Total mass, kg | 9 ± 2 | 11 ± 2 | 13 ± 3 | 13 ± 3 | <0.0001 * |
| Fat mass, kg | 2 ± 0.4 | 3 ± 1 | 5 ± 5 | 4 ± 4 | <0.0001 * |
| Lean mass, kg | 6 ± 1 | 7 ± 1 | 8 ± 2 | 8 ± 1 | 0.0019 * |
| Fat % | 21 ± 6 | 31 ± 8 | 39 ± 8 | 37 ± 9 | <0.0001 * |
| Other Characteristics | |||||
| Metabolic syndrome | 0 (0%) | 5 (7%) | 167 (42%) | 172 (46%) | <0.0001 * |
| Current smoker | 0 (0%) | 3 (4%) | 26 (7%) | 29 (6%) | 0.5039 |
| Hyperglycemia | 0 (0%) | 3 (4%) | 46 (12%) | 49 (10%) | 0.0184 * |
| Dyslipidemia | 4 (27%) | 18 (24%) | 211 (54%) | 233 (48%) | <0.0001 * |
| Hypertension | 13 (87%) | 62 (84%) | 361 (92%) | 436 (90%) | 0.1304 |
| Low HDL | 3 (20%) | 18 (24%) | 184 (47%) | 205 (42%) | 0.0002 * |
| Hypertriglyceridemia | 4 (27%) | 18 (24%) | 211 (54%) | 233 (48%) | <0.0001 * |
| Elevated waist | 2 (13%) | 12 (16%) | 266 (68%) | 280 (58%) | <0.0001 * |
| Medications | |||||
| ASA | 11 (73%) | 63 (85%) | 345 (88%) | 419 (87%) | 0.3179 |
| Plavix | 6 (40%) | 30 (41%) | 192 (49%) | 228 (47%) | 0.3656 |
| Beta blocker | 14 (93%) | 52 (70%) | 340 (86%) | 406 (84%) | 0.0032 * |
| ACE/ARB | 4 (27%) | 25 (34%) | 206 (52%) | 235 (49%) | 0.0037 * |
| Statin | 9 (60%) | 54 (73%) | 335 (85%) | 398 (82%) | 0.0063 * |
| CR Reasons | |||||
| Angina/CAD | 1 (7%) | 4 (5%) | 21 (5%) | 26 (5%) | 0.232 |
| CABG | 2 (13%) | 7 (9%) | 60 (15%) | 69 (14%) | 0.5291 |
| CHF | 2 (13%) | 3 (4%) | 19 (5%) | 24 (5%) | 0.9731 |
| NSTEMI | 1 (7%) | 16 (22%) | 55 (14%) | 72 (15%) | 0.9731 |
| Other | 1 (7%) | 4 (5%) | 18 (5%) | 23 (5%) | 0.9731 |
| PAD | 0 (0%) | 0 (0%) | 1 (0.25%) | 1 (0.21%) | 0.9731 |
| PCI | 3 (20%) | 10 (14%) | 101 (26%) | 114 (24%) | 0.9731 |
| STEMI | 1 (7%) | 14 (19%) | 51 (13%) | 66 (14%) | 0.9731 |
| Ventricular sssist device | 2 (13%) | 5 (7%) | 14 (4%) | 21 (4%) | 0.9731 |
| Valve disease | 2 (13%) | 11 (15%) | 54 (14%) | 67 (14%) | 0.9731 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonikowske, A.R.; Barillas Lara, M.I.; Koepp, K.E.; Medina Inojosa, J.R.; Squires, R.W.; Lopez-Jimenez, F.; Olson, T.P. Fat Mass Index Better Identifies Metabolic Syndrome: Insights from Patients in Early Outpatient Cardiac Rehabilitation. J. Clin. Med. 2019, 8, 2147. https://doi.org/10.3390/jcm8122147
Bonikowske AR, Barillas Lara MI, Koepp KE, Medina Inojosa JR, Squires RW, Lopez-Jimenez F, Olson TP. Fat Mass Index Better Identifies Metabolic Syndrome: Insights from Patients in Early Outpatient Cardiac Rehabilitation. Journal of Clinical Medicine. 2019; 8(12):2147. https://doi.org/10.3390/jcm8122147
Chicago/Turabian StyleBonikowske, Amanda R., Maria Irene Barillas Lara, Katlyn E. Koepp, Jose R. Medina Inojosa, Ray W. Squires, Francisco Lopez-Jimenez, and Thomas P. Olson. 2019. "Fat Mass Index Better Identifies Metabolic Syndrome: Insights from Patients in Early Outpatient Cardiac Rehabilitation" Journal of Clinical Medicine 8, no. 12: 2147. https://doi.org/10.3390/jcm8122147
APA StyleBonikowske, A. R., Barillas Lara, M. I., Koepp, K. E., Medina Inojosa, J. R., Squires, R. W., Lopez-Jimenez, F., & Olson, T. P. (2019). Fat Mass Index Better Identifies Metabolic Syndrome: Insights from Patients in Early Outpatient Cardiac Rehabilitation. Journal of Clinical Medicine, 8(12), 2147. https://doi.org/10.3390/jcm8122147