Real-World Database Examining the Association between Sjögren’s Syndrome and Chronic Rhinosinusitis


 ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. National Health Insurance Research Database
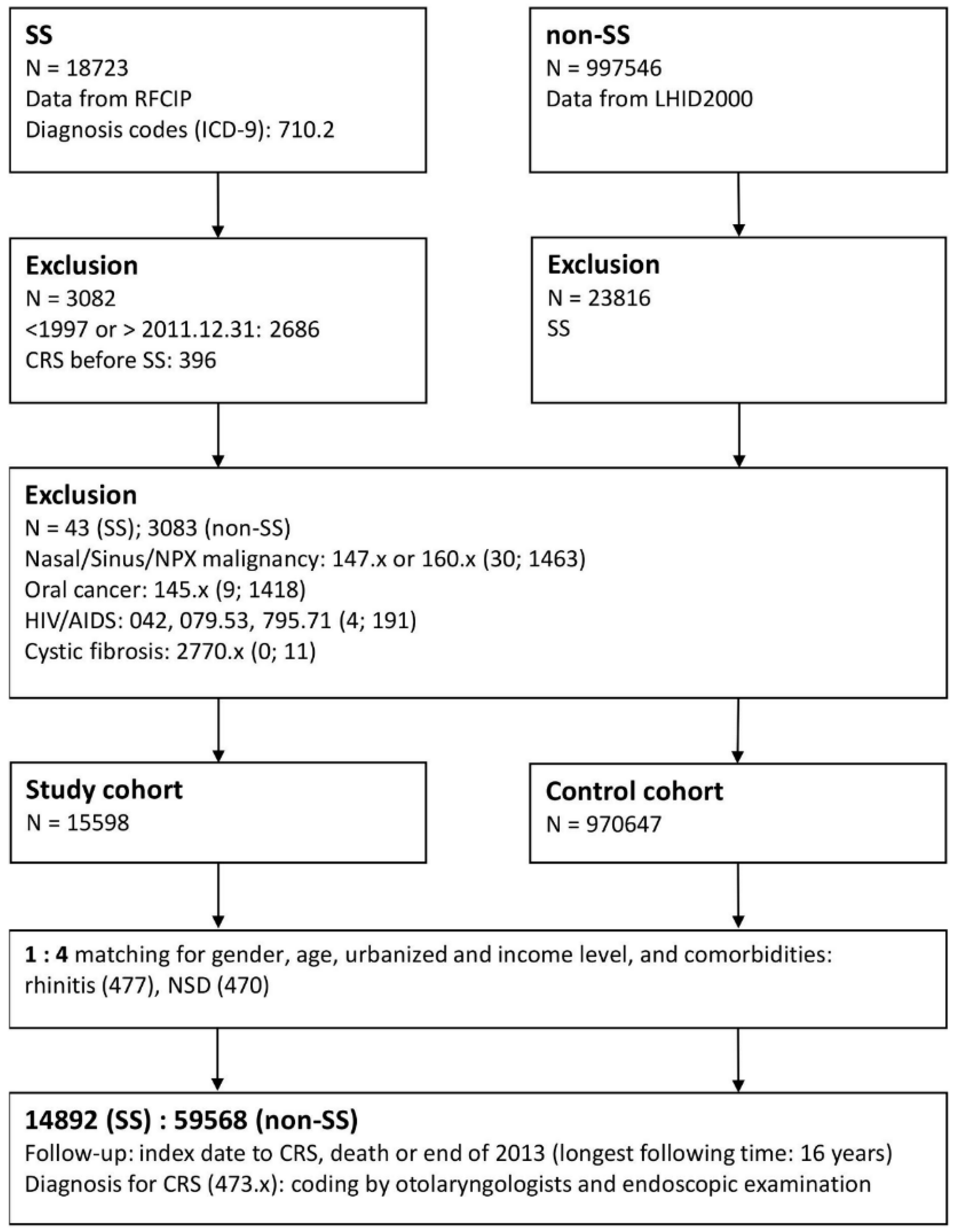
2.2. Study Group: Registry for Catastrophic Illness Patients
2.3. Comparison Group: LHID2000 Database
2.4. Matching Process
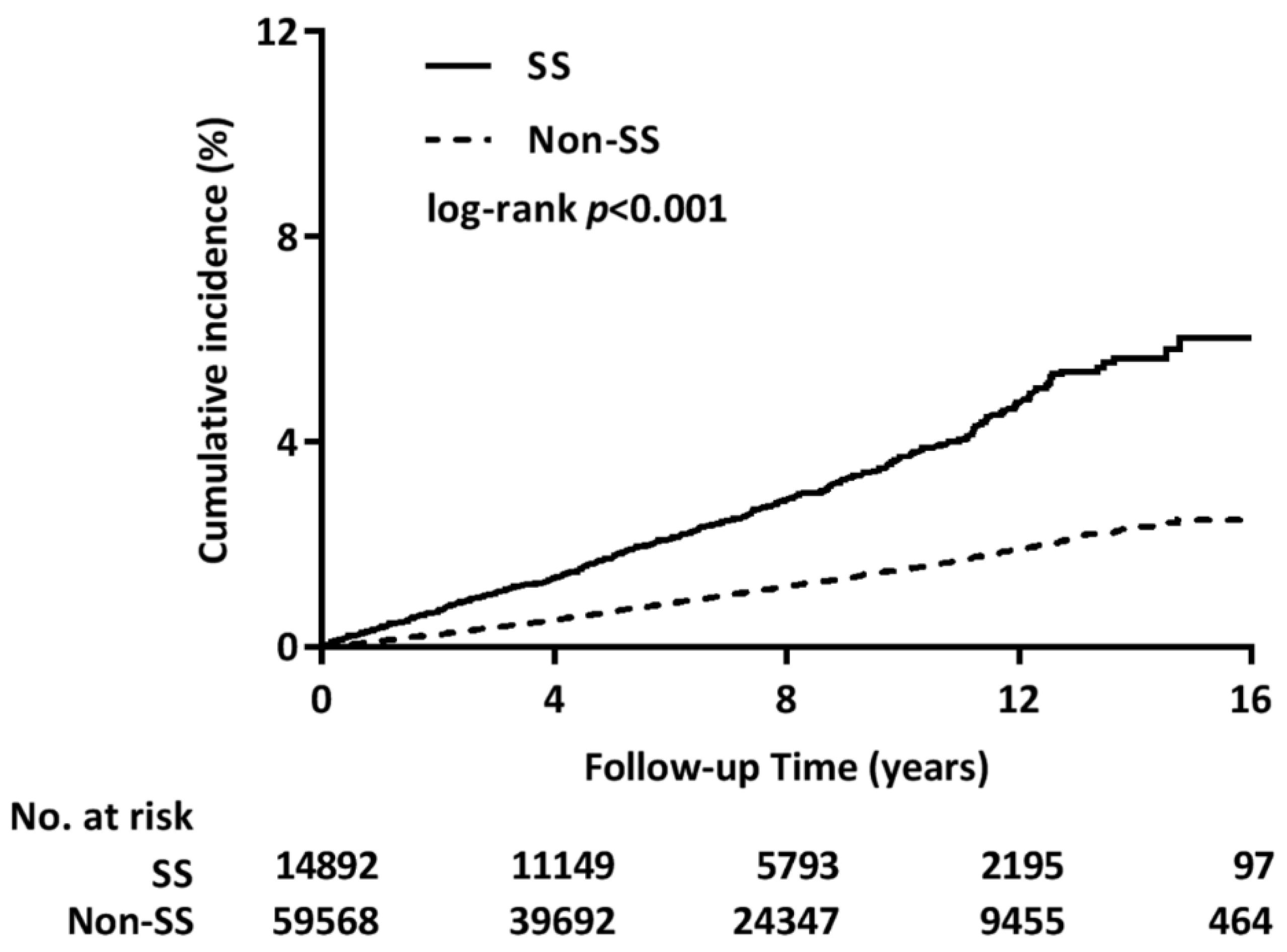
2.5. Main Outcome: Incidence of CRS
2.6. Comorbidities
2.7. Analysis of CRS therapies
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
List of abbreviations
| GERD | gastroesophageal reflux disease |
| CI | confidence interval |
| CIP | Catastrophic Illness Patients |
| COPD | chronic obstructive pulmonary disease |
| CRS | chronic rhinosinusitis |
| CRSsNP | chronic rhinosinusitis without nasal polyposis |
| CRSwNP | chronic rhinosinusitis with nasal polyposis |
| DM | diabetes mellitus |
| HT | hypertension |
| HR | hazard ratio |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| LHID2000 | Longitudinal Health Insurance Database 2000 |
| NHIRD | National Health Insurance Research Database |
| NSD | nasal septal deviation |
| RA | rheumatic arthritis |
| RFCIP | Registry for Catastrophic Illness Patients |
| SLE | systemic lupus erythematosus |
References
- Rudmik, L.; Smith, T.L. Quality of Life in Patients with Chronic Rhinosinusitis. Curr. Allergy Asthma Rep. 2011, 11, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Halawi, A.M.; Smith, S.S.; Chandra, R.K. Chronic Rhinosinusitis: Epidemiology and Cost. Allergy Asthma Proc. 2013, 34, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Lester, S.; Rischmueller, M.; Tan, L.; Wormald, P.; Zalewski, P.; Hamilton-Bruce, M.; Appleton, S.; Adams, R.; Hill, C. Sicca Symptoms and Their Association with Chronic Rhinosinusitis in a Community Sample. Open Rheumatol. J. 2012, 6, 170–174. [Google Scholar] [CrossRef]
- Reksten, T.R.; Jonsson, M.V. Sjogren’s Syndrome: An Update on Epidemiology and Current Insights on Pathophysiology. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Price, E.J.; Venables, P.J. Dry Eyes and Mouth Syndrome—A Subgroup of Patients Presenting with Sicca Symptoms. Rheumatology (Oxf.) 2002, 41, 416–422. [Google Scholar] [CrossRef]
- Min, J.Y.; Tan, B.K. Risk Factors for Chronic Rhinosinusitis. Curr. Opin. Allergy Clin. Immunol. 2015, 15, 1–13. [Google Scholar] [CrossRef]
- Midilli, R.; Gode, S.; Oder, G.; Kabasakal, Y.; Karci, B. Nasal and Paranasal Involvement in Primary Sjogren’s Syndrome. Rhinology 2013, 51, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.S.; Lee, L.A.; Tsai, Y.T.; Yang, Y.H.; Liu, C.Y.; Lin, M.H.; Hsu, C.M.; Chen, C.K.; Li, H.Y. Sleep Apnea and Risk of Vertigo: A Nationwide Population-Based Cohort Study. Laryngoscope 2018, 128, 763–768. [Google Scholar] [CrossRef]
- Chang, G.H.; Tsai, M.S.; Liu, C.Y.; Lin, M.H.; Tsai, Y.T.; Hsu, C.M.; Yang, Y.H. End-Stage Renal Disease: A Risk Factor of Deep Neck Infection—A Nationwide Follow-up Study in Taiwan. BMC Infect. Dis. 2017, 17, 424. [Google Scholar] [CrossRef]
- Tsai, M.S.; Yang, Y.H.; Liu, C.Y.; Lin, M.H.; Chang, G.H.; Tsai, Y.T.; Li, H.Y.; Tsai, Y.H.; Hsu, C.M. Unilateral Vocal Fold Paralysis and Risk of Pneumonia: A Nationwide Population-Based Cohort Study. Otolaryngol. Head Neck Surg. 2018, 158, 896–903. [Google Scholar] [CrossRef]
- Tsai, M.S.; Lin, M.H.; Lee, C.P.; Yang, Y.H.; Chen, W.C.; Chang, G.H.; Tsai, Y.T.; Chen, P.C.; Tsai, Y.H. Chang Gung Research Database: A Multi-Institutional Database Consisting of Original Medical Records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Chang, T.S.; Yao, Y.C.; Li, Y.C. Increased Risk of Chronic Sinusitis in Adults with Gastroesophgeal Reflux Disease: A Nationwide Population-Based Cohort Study. Medicine (Baltim.) 2015, 94, e1642. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.K.; Ho, Y.L.; Chang, Y.S. Prescriptions of Traditional Chinese Medicine, Western Medicine, and Integrated Chinese-Western Medicine for Allergic Rhinitis under the National Health Insurance in Taiwan. J. Ethnopharmacol. 2015, 173, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Siao, M.J.; Chen, G.S.; Lee, W.C.; Horng, J.T.; Chang, C.W.; Li, C.H. Increased Risk of Dental Trauma in Patients with Allergic Rhinitis: A Nationwide Population-Based Cohort Study. PLoS ONE 2017, 12, e0182370. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.W.; Yu, M.C.; Lin, C.L.; Yu, T.M.; Shu, K.H.; Kao, C.H. Risk of Peripheral Arterial Occlusive Disease in Patients with Systemic Lupus Erythematosus: A Nationwide Population-Based Cohort Study. Medicine (Baltim.) 2015, 94, e2121. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.-L.; Yen, Y.-C.; Chang, W.-P.; Shiao, A.-S. Association between Middle Ear Cholesteatoma and Chronic Rhinosinusitis. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 757–763. [Google Scholar] [CrossRef] [PubMed]
- Tsai, Y.T.; Huang, E.I.; Chang, G.H.; Tsai, M.S.; Hsu, C.M.; Yang, Y.H.; Lin, M.H.; Liu, C.Y.; Li, H.Y. Risk of Acute Epiglottitis in Patients with Preexisting Diabetes Mellitus: A Population-Based Case-Control Study. PLoS ONE 2018, 13, e0199036. [Google Scholar] [CrossRef]
- Puri, V.; Khare, N.A.; Chandramouli, M.V.; Shende, N.; Bharadwaj, S. Comparative Analysis of Early Excision and Grafting Vs Delayed Grafting in Burn Patients in a Developing Country. J. Burn Care Res. 2016, 37, 278–282. [Google Scholar] [CrossRef]
- Bouros, D.; Pneumatikos, I.; Tzouvelekis, A. Pleural Involvement in Systemic Autoimmune Disorders. Respiration 2008, 75, 361–371. [Google Scholar] [CrossRef]
- Ito, I.; Nagai, S.; Kitaichi, M.; Nicholson, A.G.; Johkoh, T.; Noma, S.; Kim, D.S.; Handa, T.; Izumi, T.; Mishima, M. Pulmonary Manifestations of Primary Sjogren’s Syndrome: A Clinical, Radiologic, and Pathologic Study. Am. J. Respir. Crit. Care Med. 2005, 171, 632–638. [Google Scholar] [CrossRef]
- Parambil, J.G.; Myers, J.L.; Lindell, R.M.; Matteson, E.L.; Ryu, J.H. Interstitial Lung Disease in Primary Sjogren Syndrome. Chest 2006, 130, 1489–1495. [Google Scholar] [CrossRef] [PubMed]
- Castelino, F.V.; Varga, J. Interstitial Lung Disease in Connective Tissue Diseases: Evolving Concepts of Pathogenesis and Management. Arthritis Res. Ther. 2010, 12, 213. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, K.; Sakakura, Y.; Murai, S.; Majima, Y. Nasal Mucociliary Clearance in Sjogren’s Syndrome. Dissociation in Flow between Sol and Gel Layers. Acta Otolaryngol. 1989, 108, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Wang, J.; Meijer, J.; Ieong, S.; Xie, Y.; Yu, T.; Zhou, H.; Henry, S.; Vissink, A.; Pijpe, J.; et al. Salivary Proteomic and Genomic Biomarkers for Primary Sjogren’s Syndrome. Arthritis Rheum. 2007, 56, 3588–3600. [Google Scholar] [CrossRef] [PubMed]
- Fabian, T.K.; Hermann, P.; Beck, A.; Fejerdy, P.; Fabian, G. Salivary Defense Proteins: Their Network and Role in Innate and Acquired Oral Immunity. Int. J. Mol. Sci. 2012, 13, 4295–4320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hains, D.S.; Chen, X.; Saxena, V.; Barr-Beare, E.; Flemming, W.; Easterling, R.; Becknell, B.; Schwartz, G.J.; Schwaderer, A.L. Carbonic Anhydrase 2 Deficiency Leads to Increased Pyelonephritis Susceptibility. Am. J. Physiol. Ren. Physiol. 2014, 307, F869–F880. [Google Scholar] [CrossRef] [PubMed]
- Goto, E.; Matsumoto, Y.; Kamoi, M.; Endo, K.; Ishida, R.; Dogru, M.; Kaido, M.; Kojima, T.; Tsubota, K. Tear Evaporation Rates in Sjogren Syndrome and Non-Sjogren Dry Eye Patients. Am. J. Ophthalmol. 2007, 144, 81–85. [Google Scholar] [CrossRef]
- Shimazaki, J.; Goto, E.; Ono, M.; Shimmura, S.; Tsubota, K. Meibomian Gland Dysfunction in Patients with Sjogren Syndrome. Ophthalmology 1998, 105, 1485–1488. [Google Scholar] [CrossRef]
- Absolon, M.J.; Brown, C.A. Acetylcysteine in Kerato-Conjunctivitis Sicca. Br. J. Ophthalmol. 1968, 52, 310–316. [Google Scholar] [CrossRef]
- Lopez-Pintor, R.M.; Castro, M.F.; Hernandez, G. Oral Involvement in Patients with Primary Sjogren’s Syndrome. Multidisciplinary Care by Dentists and Rheumatologists. Reumatol. Clin. 2015, 11, 387–394. [Google Scholar] [CrossRef]
- Leung, K.C.; McMillan, A.S.; Cheung, B.P.; Leung, W.K. Sjogren’s Syndrome Sufferers Have Increased Oral Yeast Levels Despite Regular Dental Care. Oral Dis. 2008, 14, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Cojocaru, M.; Cojocaru, I.M.; Silosi, I.; Vrabie, C.D. Pulmonary Manifestations of Systemic Autoimmune Diseases. Maedica (Buchar) 2011, 6, 224–229. [Google Scholar] [PubMed]
- Rosenfeld, R.M.; Andes, D.; Bhattacharyya, N.; Cheung, D.; Eisenberg, S.; Ganiats, T.G.; Gelzer, A.; Hamilos, D.; Haydon, R.C., 3rd; Hudgins, P.A.; et al. Clinical Practice Guideline: Adult Sinusitis. Otolaryngol. Head Neck Surg. 2007, 137, S1–S31. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Kumar, K.A.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical Practice Guideline (Update): Adult Sinusitis. Otolaryngol. Head Neck Surg. 2015, 152, S1–S39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, A. Canadian Guidelines for Chronic Rhinosinusitis: Clinical Summary. Can. Fam. Physician 2013, 59, 1275–1281. [Google Scholar] [PubMed]
- Bachert, C.; Pawankar, R.; Zhang, L.; Bunnag, C.; Fokkens, W.J.; Hamilos, D.L.; Jirapongsananuruk, O.; Kern, R.; Meltzer, E.O.; Mullol, J.; et al. Icon: Chronic Rhinosinusitis. World Allergy Organ. J. 2014, 7, 25. [Google Scholar] [CrossRef] [PubMed]
- Nair, S.; Dutta, A.; Rajagopalan, R.; Nambiar, S. Endoscopic Sinus Surgery in Chronic Rhinosinusitis and Nasal Polyposis: A Comparative Study. Indian J. Otolaryngol. Head Neck Surg. 2011, 63, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Zhang, G.H.; Liu, X.; Ye, J.; Zeng, Z.P. Clinical Prognostic Factors of Chronic Rhinosinusitis after Endoscopic Sinus Surgery. ORL J. Otorhinolaryngol. Relat. Spec. 2008, 70, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H.S.; Nunez, D.A. Functional Endoscopic Sinus Surgery for Chronic Rhinosinusitis. Cochrane Database Syst. Rev. 2006, CD004458. [Google Scholar] [CrossRef] [PubMed]
- Gosepath, J.; Pogodsky, T.; Mann, W.J. Characteristics of Recurrent Chronic Rhinosinusitis after Previous Surgical Therapy. Acta Otolaryngol. 2008, 128, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Chaaban, M.R.; Walsh, E.M.; Woodworth, B.A. Epidemiology and Differential Diagnosis of Nasal Polyps. Am. J. Rhinol. Allergy 2013, 27, 473–478. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.H. Mechanisms of Glucocorticoid Action in Chronic Rhinosinusitis. Allergy Asthma Immunol. Res. 2015, 7, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Van Crombruggen, K.; Zhang, N.; Gevaert, P.; Tomassen, P.; Bachert, C. Pathogenesis of Chronic Rhinosinusitis: Inflammation. J. Allergy Clin. Immunol. 2011, 128, 728–732. [Google Scholar] [CrossRef] [PubMed]
- Wong, I.W.; Rees, G.; Greiff, L.; Myers, J.C.; Jamieson, G.G.; Wormald, P.-J. Gastroesophageal Reflux Disease and Chronic Sinusitis: In Search of an Esophageal–Nasal Reflex. Am. J. Rhinol. Allergy 2010, 24, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Schan, C.A.; Harding, S.M.; Haile, J.M.; Bradley, L.A.; Richter, J.E. Gastroesophageal Reflux-Induced Bronchoconstriction: An Intraesophageal Acid Infusion Study Using State-of-the-Art Technology. Chest 1994, 106, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.-N.; Tanifuji, Y.; Kobayashi, H.; Yamauchi, K.; Kato, C.; Suzuki, K.; Inoue, H. Effects of Esophageal Acid Perfusion on Airway Hyperresponsiveness in Patients with Bronchial Asthma. Chest 2000, 118, 1553–1556. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | SS | Non-SS | p-value * | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Total | 14,892 | 59,568 | |||
| Gender | 1 | ||||
| Male | 1551 | 10.4 | 6204 | 10.4 | |
| Female | 13341 | 89.6 | 53,364 | 89.6 | |
| Age (years) | 1 | ||||
| <65 | 11742 | 78.9 | 46,968 | 78.9 | |
| ≥65 | 3150 | 21.2 | 12,600 | 21.2 | |
| Urbanized level | 1 | ||||
| 1 (City) | 4692 | 31.5 | 18,768 | 31.5 | |
| 2 | 6571 | 44.1 | 26,284 | 44.1 | |
| 3 | 2140 | 14.4 | 8560 | 14.4 | |
| 4 (Village) | 1489 | 10.0 | 5956 | 10.0 | |
| Income (NTD, per month) | 1 | ||||
| 0 | 3375 | 22.7 | 13,500 | 22.7 | |
| 1–15,840 | 2096 | 14.1 | 8384 | 14.1 | |
| 15,841–25,000 | 6390 | 42.9 | 25,560 | 42.9 | |
| ≥25,001 | 3031 | 20.4 | 12,124 | 20.4 | |
| Comorbidities | |||||
| Rhinitis | 5639 | 37.9 | 22,561 | 37.9 | 1 |
| NSD | 136 | 0.9 | 544 | 0.9 | 1 |
| GERD | 4378 | 29.4 | 8193 | 13.6 | <0.001 |
| COPD | 2877 | 19.3 | 7605 | 12.8 | <0.001 |
| Asthma | 2230 | 15.0 | 7086 | 11.9 | <0.001 |
| DM | 2411 | 16.2 | 11,787 | 19.8 | <0.001 |
| HT | 5837 | 39.2 | 23,690 | 39.8 | 0.200 |
| SLE | 3156 | 21.2 | 183 | 0.3 | <0.001 |
| RA | 4299 | 28.9 | 1618 | 2.7 | <0.001 |
| CRS | |||||
| Total | 408 | 2.7 | 667 | 1.1 | <0.001 |
| Variables | HR | 95% CI | p-value |
|---|---|---|---|
| Main model * | 2.51 | (2.22–2.84) | <0.001 |
| Additional covariates † | |||
| Main model+GERD | 2.52 | (2.22–2.86) | <0.001 |
| Main model+COPD | 2.51 | (2.22–2.84) | <0.001 |
| Main model+Asthma | 2.51 | (2.22–2.84) | <0.001 |
| Main model+DM | 2.48 | (2.20–2.81) | <0.001 |
| Main model+HT | 2.50 | (2.21–2.83) | <0.001 |
| Main model+SLE | 2.57 | (2.25–2.94) | <0.001 |
| Main model+RA | 2.69 | (2.36–3.08) | <0.001 |
| Subgroup effects | |||
| GERD | |||
| Yes | 2.21 | (1.73–2.83) | <0.001 |
| No | 2.64 | (2.28–3.05) | <0.001 |
| COPD | |||
| Yes | 2.16 | (1.66–2.82) | <0.001 |
| No | 2.60 | (2.26–2.99) | <0.001 |
| Asthma | |||
| Yes | 2.18 | (1.63–2.90) | <0.001 |
| No | 2.58 | (2.25–2.96) | <0.001 |
| DM | |||
| Yes | 2.71 | (1.99–3.68) | <0.001 |
| No | 2.47 | (2.15–2.82) | <0.001 |
| HT | |||
| Yes | 2.74 | (2.25–3.33) | <0.001 |
| No | 2.35 | (2.01–2.76) | <0.001 |
| SLE | |||
| Yes | 4.71 | (0.65–33.9) | 0.124 |
| No | 2.56 | (2.24–2.92) | <0.001 |
| RA | |||
| Yes | 2.25 | (1.38–3.68) | 0.001 |
| No | 2.71 | (2.36–3.11) | <0.001 |
| SS-CRS | Non-SS-CRS | ||
|---|---|---|---|
| Characteristic | n = 407 | n = 667 | p-value * |
| INCS (mean ± SD) | |||
| vial, per year | 1.42 ± 1.71 | 1.50 ± 3.39 | 0.712 |
| mg, per year | 11.43 ± 18.36 | 13.02 ± 34.87 | 0.491 |
| Surgery | |||
| Yes or No | 82 (20.2%) | 179 (26.84%) | 0.013 |
| times (mean ± SD) | 1.07 ± 0.19 | 1.14 ± 0.31 | 0.064 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, G.-H.; Chen, Y.-C.; Lin, K.-M.; Yang, Y.-H.; Liu, C.-Y.; Lin, M.-H.; Wu, C.-Y.; Hsu, C.-M.; Tsai, M.-S. Real-World Database Examining the Association between Sjögren’s Syndrome and Chronic Rhinosinusitis. J. Clin. Med. 2019, 8, 155. https://doi.org/10.3390/jcm8020155
Chang G-H, Chen Y-C, Lin K-M, Yang Y-H, Liu C-Y, Lin M-H, Wu C-Y, Hsu C-M, Tsai M-S. Real-World Database Examining the Association between Sjögren’s Syndrome and Chronic Rhinosinusitis. Journal of Clinical Medicine. 2019; 8(2):155. https://doi.org/10.3390/jcm8020155
Chicago/Turabian StyleChang, Geng-He, Yu-Cheng Chen, Ko-Ming Lin, Yao-Hsu Yang, Chia-Yen Liu, Meng-Hung Lin, Ching-Yuan Wu, Cheng-Ming Hsu, and Ming-Shao Tsai. 2019. "Real-World Database Examining the Association between Sjögren’s Syndrome and Chronic Rhinosinusitis" Journal of Clinical Medicine 8, no. 2: 155. https://doi.org/10.3390/jcm8020155
APA StyleChang, G. -H., Chen, Y. -C., Lin, K. -M., Yang, Y. -H., Liu, C. -Y., Lin, M. -H., Wu, C. -Y., Hsu, C. -M., & Tsai, M. -S. (2019). Real-World Database Examining the Association between Sjögren’s Syndrome and Chronic Rhinosinusitis. Journal of Clinical Medicine, 8(2), 155. https://doi.org/10.3390/jcm8020155