Predicting the Epidemiological Dynamics of Lung Cancer in Japan



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
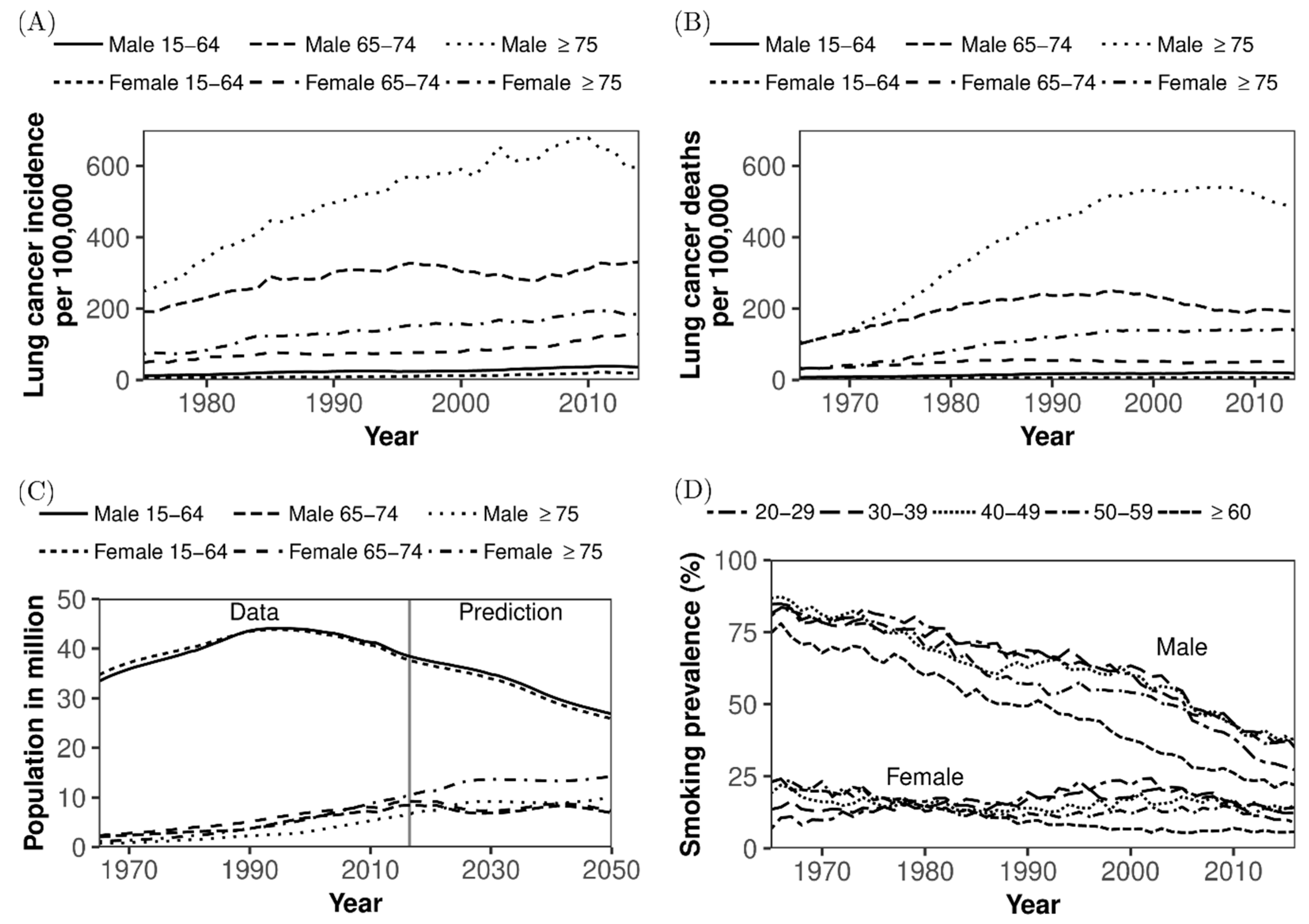
2.1. Epidemiological and Demographic Data
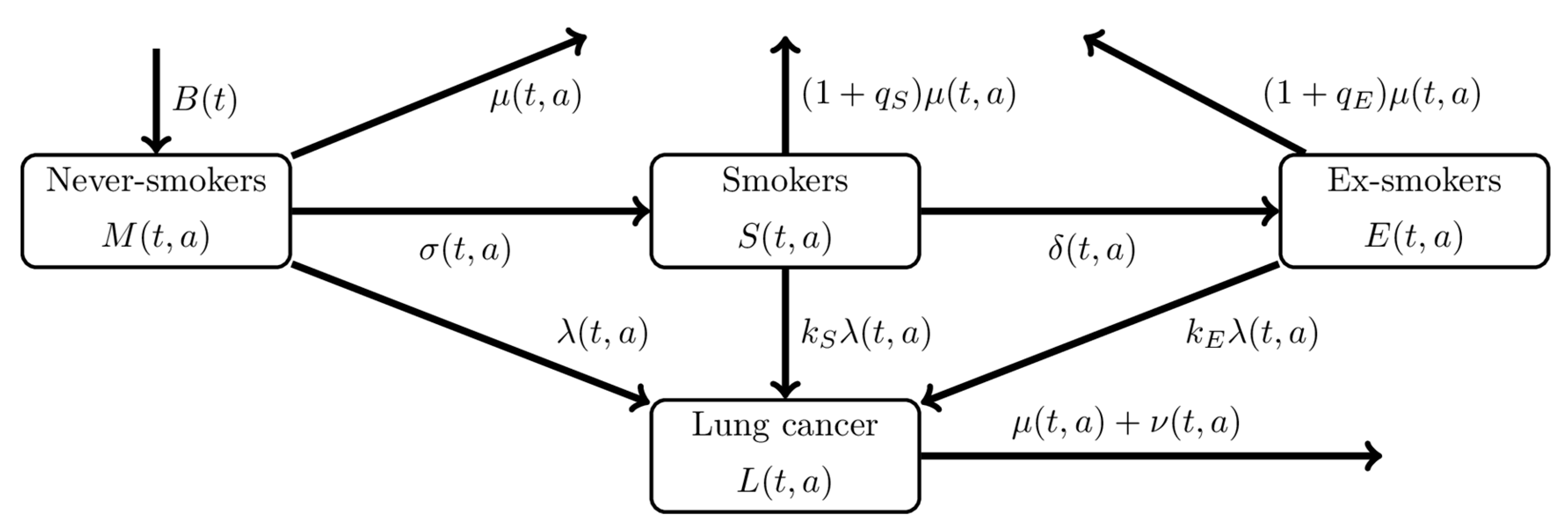
2.2. Mathematical Model
2.3. Statistical Estimation
2.4. Ethical Considerations
2.5. Data Sharing Policy
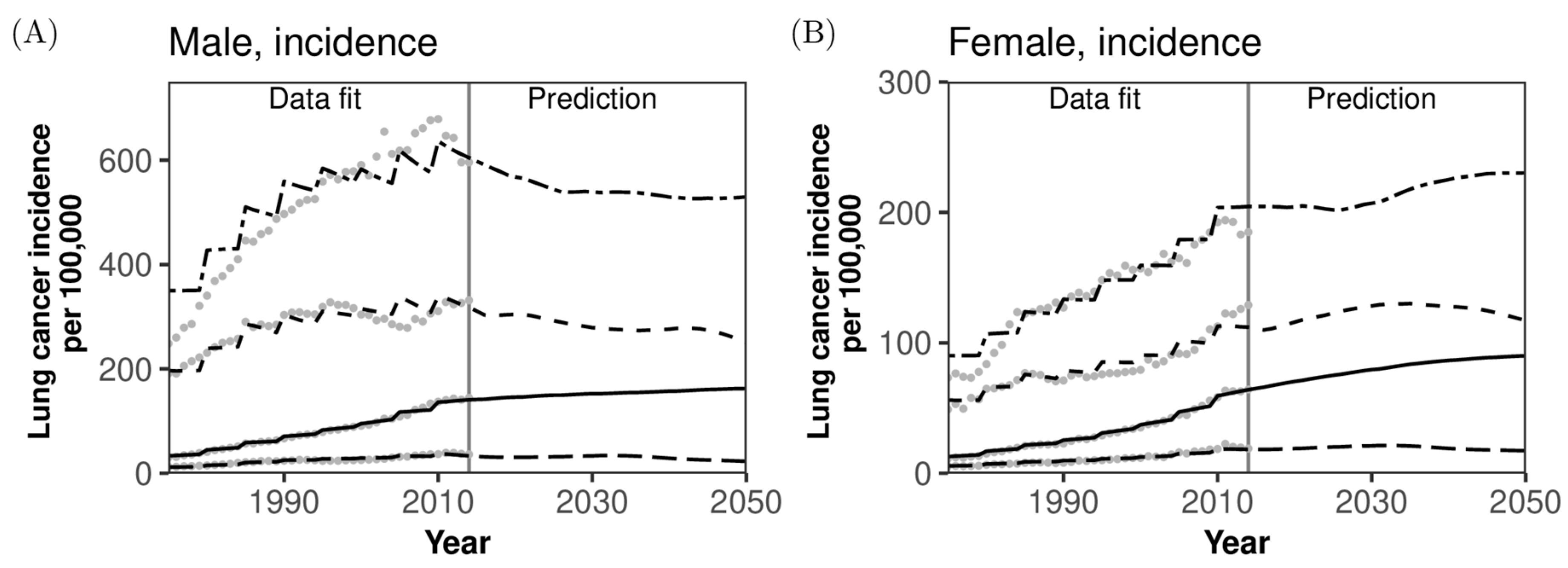
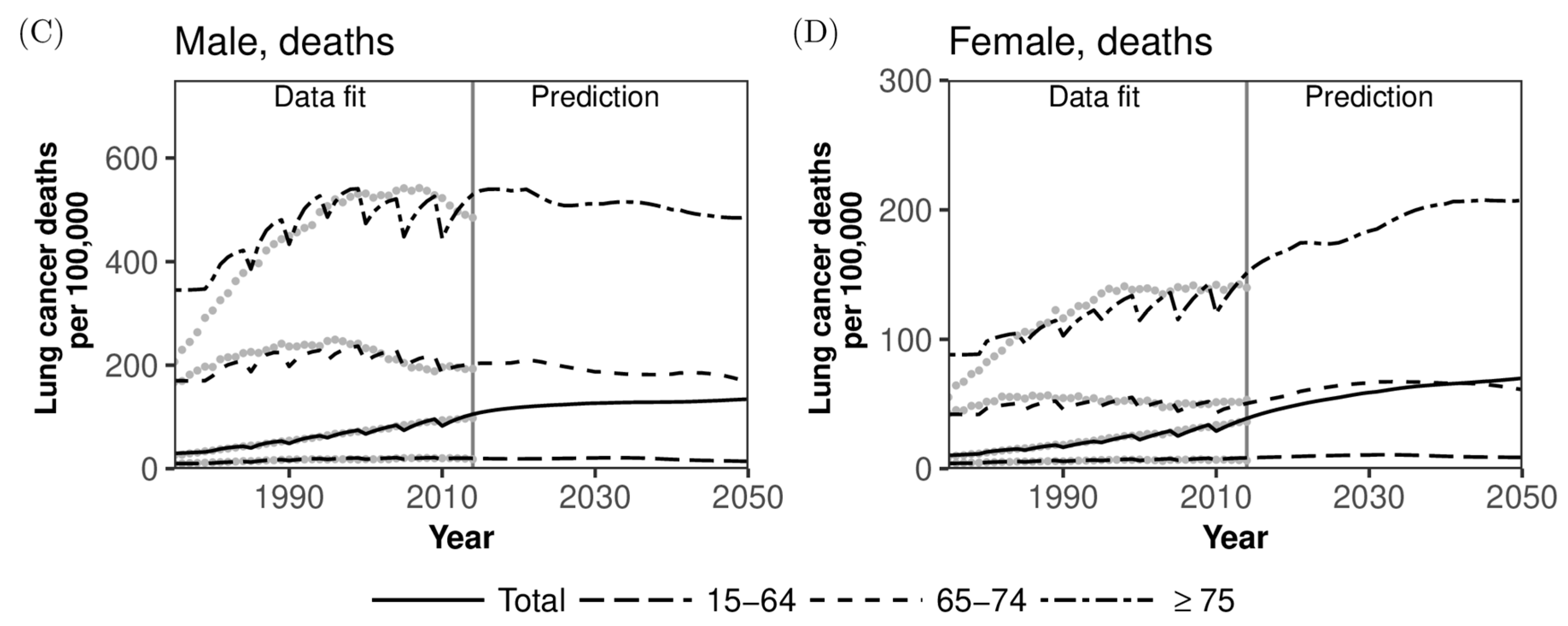
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
List of Abbreviations
Availability of Data and Materials
Appendix A. Derivation of Likelihood Function
Appendix B. Population Size Adjustment
- The population data [5] contain 1-year age groups up to age 85 years from 1975 to 1979, up to age 90 years from 1980 to 2004, and up to age 100 years from 2005 onward. A census was held every 5 years, and the census data contain 1-year age groups up to age 100 years from 1975 onward. We interpolated the population data by census data as follows.
- Let and be years in which the census was held and be the population size at year and age for , and . Note that is the population size aged over 100 years. Let be the population size at year and age for in which the census was not held. We assume that so that are given for and is the population size aged over .
- The population size for and is . Distributing into 1-year age groups using and , the population size for and was calculated by
- We obtained the interpolated population size for all ages up to 100 years. Let be mortality at year and age from to . is assumed to be the mortality of the population aged over 100 years. Mortality values are given by 5-year age groups, that is, and for . We corrected the population size so that the difference between and is equal to mortality. is defined as
- The difference between mortality and is calculated by
- If , that is, the decline in population is less than mortality, we increase the population size at year . Let represent a corrected 1-year age group. Distributing according to the proportions of population sizes, we have
- for . If , that is, the decline in population is larger than mortality, we decrease the population size at year . Distributing according to the proportions of , we have
- for . For and ,


References
- Cancer Information Service, National Cancer Center, Japan. Cancer Registry and Statistics. Available online: https://ganjoho.jp/en/professional/statistics/table_download.html (accessed on 27 December 2018).
- Center for Cancer Control and Information Services, National Cancer Center. Monitoring of Cancer Incidence in Japan—Survival 2006–2008 Report. 2016. Available online: https://ganjoho.jp/data/en/professional/statistics/files/cancer_survival(1993-2008)E.xls (accessed on 27 December 2018).
- Matsuda, T.; Ajiki, W.; Marugame, T.; Ioka, A.; Tsukuma, H.; Sobue, T.; Matsuda, T.; Shibata, A.; Mikami, H.; Okamoto, N.; et al. Population-based survival of cancer patients diagnosed between 1993 and 1999 in Japan: A chronological and international comparative study. Jpn. J. Clin. Oncol. 2011, 41, 40–51. [Google Scholar] [CrossRef] [PubMed]
- Japan Tobacco, Inc. Nationwide Smoking Prevalence Survey. Available online: https://www.jti.co.jp/investors/library/press_releases/2018/pdf/20181213_01_appendix_01.pdf (accessed on 27 December 2018). (In Japanese).
- Health, Labour and Welfare Statistics Association. Demographic Statistical Time Series Data 1899–2012. 2014. Available online: https://www.mhlw.go.jp/toukei/list/81-1.html (accessed on 27 December 2018). (In Japanese)
- National Institute of Population and Social Security Research. Population Projection for Japan: 2016–2065; National Institute of Population and Social Security Research: Tokyo, Japan, 2017.
- Loddenkemper, R.; Kreuter, M. (Eds.) The Tobacco Epidemic, 2nd ed.; Progress in Respiratory Research; Revised and Extended Edition; S. Karger AG: Basel, Switzerland, 2015; Volume 42. [Google Scholar]
- McMahon, P.M.; Kong, C.Y.; Johnson, B.E.; Weinstein, M.C.; Weeks, J.C.; Tramontano, A.C.; Cipriano, L.E.; Bouzan, C.; Gazelle, G.S. Chapter 9: The MGH-HMS lung cancer policy model: Tobacco control versus screening. Risk Anal. 2012, 32, S117–S124. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Blackman, K.; Zaloshnja, E. Chapter 10: A macro-model of smoking and lung cancer: Examining aggregate trends in lung cancer rates using the CPS-I and CPS-II and two-stage clonal expansion models. Risk Anal. 2012, 32, S125–S141. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Health, Labour and Welfare Statistics Association. Demographic Statistical Time Series Data 2013–14. 2015. Available online: https://www.mhlw.go.jp/toukei/list/81-1.html (accessed on 27 December 2018). (In Japanese)
- Sobue, T.; Yamamoto, S.; Hara, M.; Sasazuki, S.; Sasaki, S.; Tsugane, S.; JPHC study Group. Cigarette smoking and subsequent risk of lung cancer by histologic type in middle-aged Japanese men and women: The JPHC study. Int. J. Cancer 2002, 99, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statistics Bureau, Ministry of Internal Affairs and Communications. Population Estimates. Available online: https://www.stat.go.jp/data/jinsui/index.html (accessed on 27 December 2018). (In Japanese)
- Ozasa, K. Smoking and mortality in the Japan Collaborative Cohort Study for Evaluation of Cancer (JACC). Asian Pac. J. Cancer Prev. 2007, 8, 89–96. [Google Scholar] [PubMed]
- Ando, M.; Wakai, K.; Seki, N.; Tamakoshi, A.; Suzuki, K.; Ito, Y.; Nishino, Y.; Kondo, T.; Watanabe, Y.; Ozasa, K.; et al. Attributable and absolute risk of lung cancer death by smoking status: Findings from the Japan collaborative cohort study. Int. J. Cancer 2003, 105, 249–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marugame, T.; Sobue, T.; Satoh, H.; Komatsu, S.; Nishino, Y.; Nakatsuka, H.; Nakayama, T.; Suzuki, T.; Takezaki, T.; Tajima, K.; et al. Lung cancer death rates by smoking status: Comparison of the three-prefecture cohort study in Japan to the Cancer Prevention Study II in the USA. Cancer Sci. 2005, 96, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Seki, T.; Nishino, Y.; Tanji, F.; Maemondo, M.; Takahashi, S.; Sato, I.; Kawai, M.; Minami, Y. Cigarette smoking and lung cancer risk according to histologic type in Japanese men and women. Cancer Sci. 2013, 104, 1515–1522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakai, K.; Inoue, M.; Mizoue, T.; Tanaka, K.; Tsuji, I.; Nagata, C.; Tsugane, S. Tobacco smoking and lung cancer risk: An evaluation based on a systematic review of epidemiological evidence among the Japanese population. Jpn. J. Clin. Oncol. 2006, 36, 309–324. [Google Scholar] [CrossRef]
- Nakamura, K.; Ukawa, S.; Okada, E.; Hirata, M.; Nagai, A.; Yamagata, Z.; Ninomiya, T.; Muto, K.; Kiyohara, Y.; Matsuda, K.; et al. Characteristics and prognosis of Japanese male and female lung cancer patients: The BioBank Japan Project. J. Epidemiol. 2017, 27, S49–S57. [Google Scholar] [CrossRef] [PubMed]
- Funatogawa, I.; Funatogawa, T.; Yano, E. Trends in smoking and lung cancer mortality in Japan, by birth cohort, 1949–2010. Bull. World Health Organ. 2013, 91, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Charvat, H.; Sasazuki, S.; Shimazu, T.; Budhathoki, S.; Inoue, M.; Iwasaki, M.; Sawada, N.; Yamaji, T.; Tsugane, S.; JPHC Study Group. Development of a risk prediction model for lung cancer: The Japan public health center-based prospective study. Cancer Sci. 2018, 109, 854–862. [Google Scholar] [CrossRef] [PubMed]
- Clements, M.S.; Armstrong, B.K.; Moolgavkar, S.H. Lung cancer rate predictions using generalized additive models. Biostatistics 2005, 6, 576–589. [Google Scholar] [CrossRef] [PubMed]
- Lubin, J.H.; Caporaso, N.; Wichmann, H.E.; Schaffrath-Rosario, A.; Alavanja, M.C.R. Cigarette smoking and lung cancer: Modeling effect modification of total exposure and intensity. Epidemiology 2007, 18, 639–648. [Google Scholar] [CrossRef] [PubMed]
- Darby, S.C.; Pike, M.C. Lung cancer and passive smoking: Predicted effects from a mathematical model for cigarette smoking and lung cancer. Br. J. Cancer 1988, 58, 825–831. [Google Scholar] [CrossRef] [PubMed]
- Chadeau-Hyam, M.; Tubert-Bitter, P.; Guihenneuc-Jouyaux, C.; Campanella, G.; Richardson, S.; Vermeulen, R.; De Iorio, M.; Galea, S.; Vineis, P. Dynamics of the risk of smoking-induced lung cancer: A compartmental hidden Markov model for longitudinal analysis. Epidemiology 2014, 25, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Holford, T.R.; Levy, D.T.; Feuer, E.J.; Cao, P.; Tam, J.; Clarke, L.; Clarke, J.; Kong, C.Y.; Meza, R. Smoking and lung cancer mortality in the United States from 2015 to 2065: A comparative modeling approach. Ann. Intern. Med. 2018, 169, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Han, S.S.; Erdogan, S.A.; Toumazis, I.; Leung, A.; Plevritis, S.K. Evaluating the impact of varied compliance to lung cancer screening recommendations using a microsimulation model. Cancer Causes Control 2017, 28, 947–958. [Google Scholar] [CrossRef] [PubMed]
- Gauvreau, C.L.; Fitzgerald, N.R.; Memon, S.; Flanagan, W.M.; Nadeau, C.; Asakawa, K.; Garner, R.; Miller, A.B.; Evans, W.K.; Popadiuk, C.M.; et al. The OncoSim model: Development and use for better decision-making in Canadian cancer control. Curr. Oncol. 2017, 24, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Goffin, J.R.; Flanagan, W.M.; Miller, A.B.; Fitzgerald, N.R.; Memon, S.; Wolfson, M.C.; Evans, W.K. Biennial lung cancer screening in Canada with smoking cessation—outcomes and cost-effectiveness. Lung Cancer 2016, 101, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Ten Haaf, K.; Tammemägi, M.C.; Bondy, S.J.; van der Aalst, C.M.; Gu, S.; McGregor, S.E.; Nicholas, G.; de Koning, H.J.; Paszat, L.F. Performance and cost-effectiveness of computed tomography lung cancer screening scenarios in a population-based setting: A microsimulation modeling analysis in Ontario, Canada. PLoS Med. 2017, 14, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Meza, R.; ten Haaf, K.; Kong, C.Y.; Erdogan, A.; Black, W.C.; Tammemagi, M.C.; Choi, S.E.; Jeon, J.; Han, S.S.; Munshi, V.; et al. Comparative analysis of 5 lung cancer natural history and screening models that reproduce outcomes of the NLST and PLCO trials. Cancer 2014, 120, 1713–1724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuer, E.J.; Levy, D.T.; McCarthy, W.J. Chapter 1: The impact of the reduction in tobacco smoking on U.S. lung cancer mortality, 1975–2000: An introduction to the problem. Risk Anal. 2012, 32, S6–S13. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.M.; Burns, D.M.; Dodd, K.W.; Feuer, E.J. Chapter 2: Birth-cohort-specific estimates of smoking behaviors for the U.S. population. Risk Anal. 2012, 32, S14–S24. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, M.A.; Feuer, E.J.; Yu, B.; Sun, J.; Henley, S.J.; Shanks, T.G.; Anderson, C.M.; McMahon, P.M.; Thun, M.J.; Burns, D.M. Chapter 3: Cohort life tables by smoking status, removing lung cancer as a cause of death. Risk Anal. 2012, 32, S25–S38. [Google Scholar] [CrossRef] [PubMed]
- Holford, T.R.; Clark, L. Chapter 4: Development of the counterfactual smoking histories used to assess the effects of tobacco control. Risk Anal. 2012, 32, S39–S50. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.; Meza, R.; Krapcho, M.; Clarke, L.D.; Byrne, J.; Levy, D.T. Chapter 5: Actual and counterfactual smoking prevalence rates in the U.S. Population via microsimulation. Risk Anal. 2012, 32, S51–S68. [Google Scholar] [CrossRef] [PubMed]
- Schultz, F.W.; Boer, R.; de Koning, H.J. Chapter 7: Description of MISCAN-Lung, the Erasmus MC lung cancer microsimulation model for evaluating cancer control interventions. Risk Anal. 2012, 32, S85–S98. [Google Scholar] [CrossRef] [PubMed]
- Hazelton, W.D.; Jeon, J.; Meza, R.; Moolgavkar, S.H. Chapter 8: The FHCRC lung cancer model. Risk Anal. 2012, 32, S99–S116. [Google Scholar] [CrossRef] [PubMed]
- Foy, M.; Deng, L.; Spitz, M.; Gorlova, O.; Kimmel, M. Chapter 11: Rice-MD Anderson lung cancer model. Risk Anal. 2012, 32, S142–S150. [Google Scholar] [CrossRef] [PubMed]
- Holford, T.R.; Ebisu, K.; McKay, L.; Oh, C.; Zheng, T. Chapter 12: Yale lung cancer model. Risk Anal. 2012, 32, S151–S165. [Google Scholar] [CrossRef] [PubMed]
- Holford, T.R.; Levy, D.T. Chapter 14: Comparing the adequacy of carcinogenesis models in estimating U.S. population rates for lung cancer mortality. Risk Anal. 2012, 32, S179–S189. [Google Scholar] [CrossRef] [PubMed]
- Boer, R.; Moolgavkar, S.H.; Levy, D.T. Chapter 15: Impact of tobacco control on lung cancer mortality in the United States over the period 1975–2000—Summary and limitations. Risk Anal. 2012, 32, S190–S201. [Google Scholar] [CrossRef] [PubMed]
- Brouwer, A.F.; Eisenberg, M.C.; Meza, R. Case studies of gastric, lung, and oral cancer connect etiologic agent prevalence to cancer incidence. Cancer Res 2018, 78, 3386–3396. [Google Scholar] [PubMed]
- Criss, S.D.; Sheehan, D.F.; Palazzo, L.; Kong, C.Y. Population impact of lung cancer screening in the United States: Projections from a microsimulation model. PLoS Med. 2018, 15, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Levy, D.T.; Yuan, Z.; Li, Y. The US SimSmoke tobacco control policy model of smokeless tobacco and cigarette use. BMC Public Health 2018, 18, 696. [Google Scholar] [CrossRef] [PubMed]
- Nautiyal, N.; Holford, T.R. A spatiotemporal back-calculation approach to estimate cancer incidence measures. Stat. Med. 2018, 37, 4472–4489. [Google Scholar] [CrossRef] [PubMed]
- Kayano, T.; Lee, K.D.; Nishiura, H. Estimating the force of infection with Helicobacter pylori in Japan. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 1451490. [Google Scholar] [CrossRef] [PubMed]
- Nishiura, H. Estimating the incidence and diagnosed proportion of HIV infections in Japan: A statistical modeling study. PeerJ 2019, 7, e6275. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.J.; Jeon, C.; Jee, S.H. The effect of smoking on lung cancer: Ethnic differences and the smoking paradox. Epidemiol Health 2016, 38, e2016060. [Google Scholar] [CrossRef] [PubMed]
- Hori, M.; Tanaka, H.; Wakai, K.; Sasazuki, S.; Katanoda, K. Secondhand smoke exposure and risk of lung cancer in Japan: A systematic review and meta-analysis of epidemiologic studies. Jpn. J. Clin. Oncol. 2016, 46, 942–951. [Google Scholar] [CrossRef]
- Kishida, N.; Nishiura, H. Demographic supply-demand imbalance in industrial structure in the super-aged nation Japan. Theor. Biol. Med. Model. 2018, 15, 19. [Google Scholar] [CrossRef]
- Jung, S.M.; Lee, H.; Nishiura, H. The impact of pneumococcal vaccination on pneumonia mortality among the elderly in Japan: A difference-in-difference study. PeerJ 2018, 6, e6085. [Google Scholar] [CrossRef]
- Saito, M.M.; Nishiura, H.; Higuchi, T. Reconstructing the transmission dynamics of rubella in Japan, 2012–2013. PLoS ONE 2018, 13, e0205889. [Google Scholar] [CrossRef] [PubMed]
- Hamaguchi, Y.; Yamaguchi, T.; Nishiura, H. Estimating the annual risk of tuberculosis infection in Japan from interferon-gamma release assay data. J. Theor. Biol. 2019, 460, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Akhmetzhanov, A.R.; Lee, H.; Jung, S.M.; Kinoshita, R.; Shimizu, K.; Yoshii, K.; Nishiura, H. Real time forecasting of measles using generation-dependent mathematical model in Japan, 2018. PLoS Curr. Outbreaks 2018, 10. [Google Scholar] [CrossRef] [PubMed]








© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamaguchi, T.; Nishiura, H. Predicting the Epidemiological Dynamics of Lung Cancer in Japan. J. Clin. Med. 2019, 8, 326. https://doi.org/10.3390/jcm8030326
Yamaguchi T, Nishiura H. Predicting the Epidemiological Dynamics of Lung Cancer in Japan. Journal of Clinical Medicine. 2019; 8(3):326. https://doi.org/10.3390/jcm8030326
Chicago/Turabian StyleYamaguchi, Takayuki, and Hiroshi Nishiura. 2019. "Predicting the Epidemiological Dynamics of Lung Cancer in Japan" Journal of Clinical Medicine 8, no. 3: 326. https://doi.org/10.3390/jcm8030326
APA StyleYamaguchi, T., & Nishiura, H. (2019). Predicting the Epidemiological Dynamics of Lung Cancer in Japan. Journal of Clinical Medicine, 8(3), 326. https://doi.org/10.3390/jcm8030326