1. Introduction
Available data from most parts of world indicate that young people are often lacking competencies and are erroneously or partially informed about sexuality, sexual health and sexual risk behavior, and that they are the population that is at the highest risk of negative outcomes associated with sexual health, but the literature also indicates that many of these aspects could be overcome through effective sexuality education programs and interventions [
1,
2,
3]. Thus, improving or optimizing sexual health in young people should and oftentimes does constitute a priority for families and care-givers, local communities, states and global society.
There is a considerable need expressed and identified for successful sexuality education programs and interventions, both formal and informal, for young people and for parents, given the costs and consequences of a lack of competencies and of risky sexual behavior in young people [
4]. In line with this, identifying psychosocial factors relevant to the quality of the parent-child relationship and thus for the sexuality education and sexuality communication behavior between parents and their children is a promising line of research [
5,
6,
7].
The quality of a couple’s relationship and their perception of it could influence a number of aspects of the parent-child relationship [
8] and vice versa [
9,
10]. Kouros and colleagues [
11] found a positive association between daily evaluations of the emotional quality of a parent’s intimate/couple relationship and that of the parent-child relationship after controlling for relationship satisfaction and conflict and for parenting levels [
11]. This
spillover effect [
10,
11,
12], that is the transfer of a person’s (particularly negative) affect, mood and behavior from one context to another or from one interaction to another, could be bidirectional [
10,
11]. The
compensation hypothesis proposes that a compensation of negative aspects of the couple relationship might translate into a person investing parenting resources (time, attention, knowledge) and positive affect into their parent-child relationship [
13]. The two models should not necessarily be mutually exclusive [
11]. Studies investigating the influence that the quality of parent-child relationship might have on the parents’ couple relationship or the bi-directionality of these influences have found support for both hypotheses [
9,
10,
14].
Empirical evidence exists highlighting the (primary and secondary) effect that some parenting interventions might have on childrens’ behavior, on the parent-child relationship and also on the couple relationship [
9]. Also, it appears that mothers might be less vulnerable than fathers to the spillover effect from the couple relationship into the parent-child relationship [
14].
Parents’ concern over their communication with their children on sexuality topics is an aspect commonly addressed by parental programs and interventions (as a means or a goal) due to communication’s intrinsic role in parent-child relationships [
15,
16]. Studies investigating parental
connectedness [
17] with its component parent-child (sexual) communication, found communication (and connectedness) to be playing a protective role against certain sexual risk behavior in which young people might engage [
18,
19].
Communication on sexual topics between adolescents and parents predicted adolescents’ sexual communication with their partners on similar topics and for the sexually active ones it predicted the use of protection during sex (such as condoms) [
20]. Although some parents express fear of the possibility that communication about sexuality might cause adolescents and young people to start their sex lives earlier or increase the chances of them engaging in particular sexual behavior, data generally does not support this association [
15,
19,
21,
22].
The majority of parents report they wish to communicate “openly” with their children on this subject [
23], although data indicates that many of the adolescents perceive their communication on various sexuality issues with their parents to be less than satisfactory [
22]. Generally, mothers tend to communicate more (frequently and diversely) than fathers about sexuality and more with their daughters than with their sons [
24]. Also, there is a similar discrepancy with regard to parent-child sexuality communication related outcomes (e.g., sexually protective behavior) in favor of girls/daughters [
15]. Widman and colleagues [
15] suggest that besides other factors associated with the parent-child relationship, the quality of the parents’ couple relationship might interact with the parent-child communication and with its effects on children and young people’s sexual behavior [
15].
The perceived self-efficacy and outcome expectancies (both in parents and in young people) about certain sexuality and sexuality education behaviors and outcomes were identified as good predictors for the level of sexually protective behavior in which young people engage and for their intentions in that sense [
25,
26,
27]. Perceived self-efficacy is a person’s beliefs and expectations of their capacity to successfully follow a certain behavior while outcome expectancy is the person’s beliefs regarding the likelihood of a particular behavior to produce a certain outcome [
28].
The sexuality (education) and sexual health of young people with intellectual or developmental disabilities has not been the subject of many research efforts thus far [
29]. Significantly fewer aspects of the association between couple relationship factors and parent-child relationship factors in parents and their children with developmental problems or difficulties have been investigated. In comparison to others, these parents experience higher levels of stress and lower levels of couple relationship satisfaction [
30,
31].
Although the literature on the subject is not extensive, it is known that young LGBT people and their parents face various additional and specific challenges regarding sexuality education, sexual health and general well-being [
32]. Research efforts in the health promotion and prevention of risk behavior in sexual and gender minorities revealed that positive parenting practices, acceptance and support from families, and communication between parents and LGBT youth were found to have protective roles for young people’s health and well-being [
32].
There is very little research in the area of sexual risk behavior and sexuality education with participants, young or otherwise, from Romania. Romania does not have sexuality education in the national curriculum; currently, it lacks a national strategy and has had inconsistent or partially successful public policies regarding sexual and reproductive health. Data provided by reports from various international health promotion organizations have, in recent years, placed Romania in undesired leading positions among European countries with respect to various sexual and reproductive health outcomes [
33].
This study aims to explore the ways in which, for parents in Romania, the perception of their couple-relationship quality and of several factors associated with it (such as sexual communication anxiety and sexual perfectionism) is related to the perception of factors describing parenting dimensions relevant for the sexuality education of children and young people. The perception of the quality of the couple relationship was previously, in studies [
34] of adult participants from Romania, associated with their perception of the quality of their sexual relationship, with their anxiety to talk about sexual issues with their partners, and with aspects of their sexual perfectionism. Sexual communication anxiety is the anxiety or fear associated with a real or anticipated communication with one’s sexual partner about sexuality [
35]. Perfectionism is defined as a person’s constant striving to avoid mistakes (
flawlessness), their establishing extremely high standards of performance, accompanied by a tendency to make excessively critical self-evaluations and to be preoccupied with others’ negative evaluations of them [
36]. Sexual perfectionism refers to the perfectionistic beliefs, standards and expectations people have for sexual performance and relationships, i.e., perfectionism related to the sexual aspects of a relationship [
37,
38].
Thus, the following hypotheses were tested: (1) Sexual communication anxiety and sexual perfectionism are significant predictors (individually and together) for parents’ self-efficacy, outcome expectancy and communication-and-parenting behavior regarding sexuality education; (2) Parents’ self-efficacy and outcome expectancy about parent-child communication on sexual topics are predictors (separately and together) of the level of parenting behavior in this respect; and (3) Parents’ sexual perfectionism and sexual communication anxiety together with their self-efficacy and outcome expectancy regarding parent-child communication about sexuality predict the level of parental sexuality-communication-and-education behavior.
3. Results
The results (Spearman rho coefficients) of the correlation analyses on subscale scores of study measures can be seen in
Table 1.
Table 1 shows significant Spearman rho correlation coefficients (
p < 0.01, 2-tailed) of adequate values, describing the relation between global scores on OECS and PCSQ (
rest = 0.628,
p < 0.01), on OECS and SCAI (
rs = −0.564,
p < 0.01) and on PCSQ and SCAI (
rs = −0.516,
p < 0.01). MSPQ global scores had no statistically significant relation with global scores on other measures in the study, although the Spearman rho correlation coefficient’s value for the MSPQ and SCAI global scores almost reached statistical significance (
p = 0.06, 2 -tailed). Of particular interest are PCSQ subscales 1 and 2, which assess two different variables of the study: the OECS scores significantly positively correlate with the PCSQ1-SE scores (
rest = 0.657,
p < 0.01) and with the PCSQ2-B scores (
rs = 0.478,
p < 0.01); the SCAI global scores significantly negatively correlate with the PCSQ1-SE scores (
rs = −0.526,
p < 0.01) and with the PCSQ2-B scores (
rs = −0.391,
p < 0.01) (see
Table 1).
Regarding sexual perfectionism and its dimensions’ correlations with other variables of the study, the only statistically significant ones were between scores on: MSPQ2-PS and PCSQ1-SE (
rest = −0.330,
p < 0.01); MSPQ3-DP and PCSQ1-SE (
rs = −0.215,
p < 0.05); MSPQ5-PSD and OECS (
rs = −0.245,
p < 0.05), MSPQ5-PSD and PCSQ1-SE (
rs = −0.392,
p < 0.01); MSPQ5-PSD and SCAI (
rs = 0.301,
p < 0.01); and MSPQ global scores and PCSQ1-SE (
rs = −0.300,
p < 0.01) (see
Table 1).
Simple linear regression analyses were carried out to test the predictor quality of some study variables as posited by hypotheses 1 and 2. Simple linear regression equations (df = 1 and residual df = 104) indicated that the following significant predictors were found: (1) the MSPQ5-PSD scores predicted the PCSQ1-SE scores (F = 12.557, p < 0.01; R2 = 0.108) and SCAI global scores (F = 11.384, p < 0.01 R2 = 0.099); (2) the SCAI global scores predicted the PCSQ1-SE scores (F = 39.982, p < 0.01, R2 = 0.278), PCSQ2-B scores (F = 22.244, p < 0.01, R2 = 0.176) and POES scores (F = 47.265, p < 0.01, R2 = 0.312); (3) the POES scores predicted the PCSQ1-SE scores (F = 81.050, p < 0.01, R2 = 0.438) and PCSQ2-B scores (F = 32.401, p < 0.01, R2 = 0.238) and (4) the PCSQ1-SE scores predicted the PCSQ2-B scores (F = 74.308, p < 0.01, R2 = 0.417) and POES global scores (F = 81.050, p < 0.01, R2 = 0.438).
Simple linear regression analyses were followed (when the case) by a multiple linear regression. For all regression models proposed, the data satisfactorily verified all the assumptions of a multiple regression analysis [
39,
42,
43].
The regression equation found for the “predictors SCA and MSP-PSD and criterion SESC” model was significant: F(2,103) = 22.821, p < 0.000, with R2 = 0.307. The SESC predicted level was 220.912–0.658 (SCA) −1.280 (MSP-PSD), where 220.912 was the constant’s regression coefficient’s value. Only SCA predicted SESC significantly at a p < 0.01 level, but at p < 0.05 both predictors were significant.
The regression equation found for the “predictors OECS and SESC and criterion SECB” model was significant: F (2,103) = 37.782, p < 0.000, with R2 = 0.423. The SECB predicted level was −0.500 + 0.210 (SESC) + 0.151 (OECS), where −0.500 was the constant’s regression coefficient’s value. Only SESC was a significant predictor for SECB. The regression equation found for the “predictors OECS and SCA and criterion SESC” model was significant: F (2,103) = 46.381, p < 0.000, with R2 = 0.474. The SESC predicted level was 1.247–0.320 (SCA) + 2.062 (OECS), where 1.247 was the constant’s regression coefficient’s value. Both SCA and OECS were significant predictors for SESC.
The regression equation found for the “predictors SCA and SESC and criterion SECB” model was significant: F (2,103) = 38.144, p < 0.000, cu R2 = 0.426. The SECB predicted level was 15.114–0.056 (SCA) + 0.215 (SESC), where 15.114 was the constant’s regression coefficient’s value. Only SESC was a significant predictor for SECB.
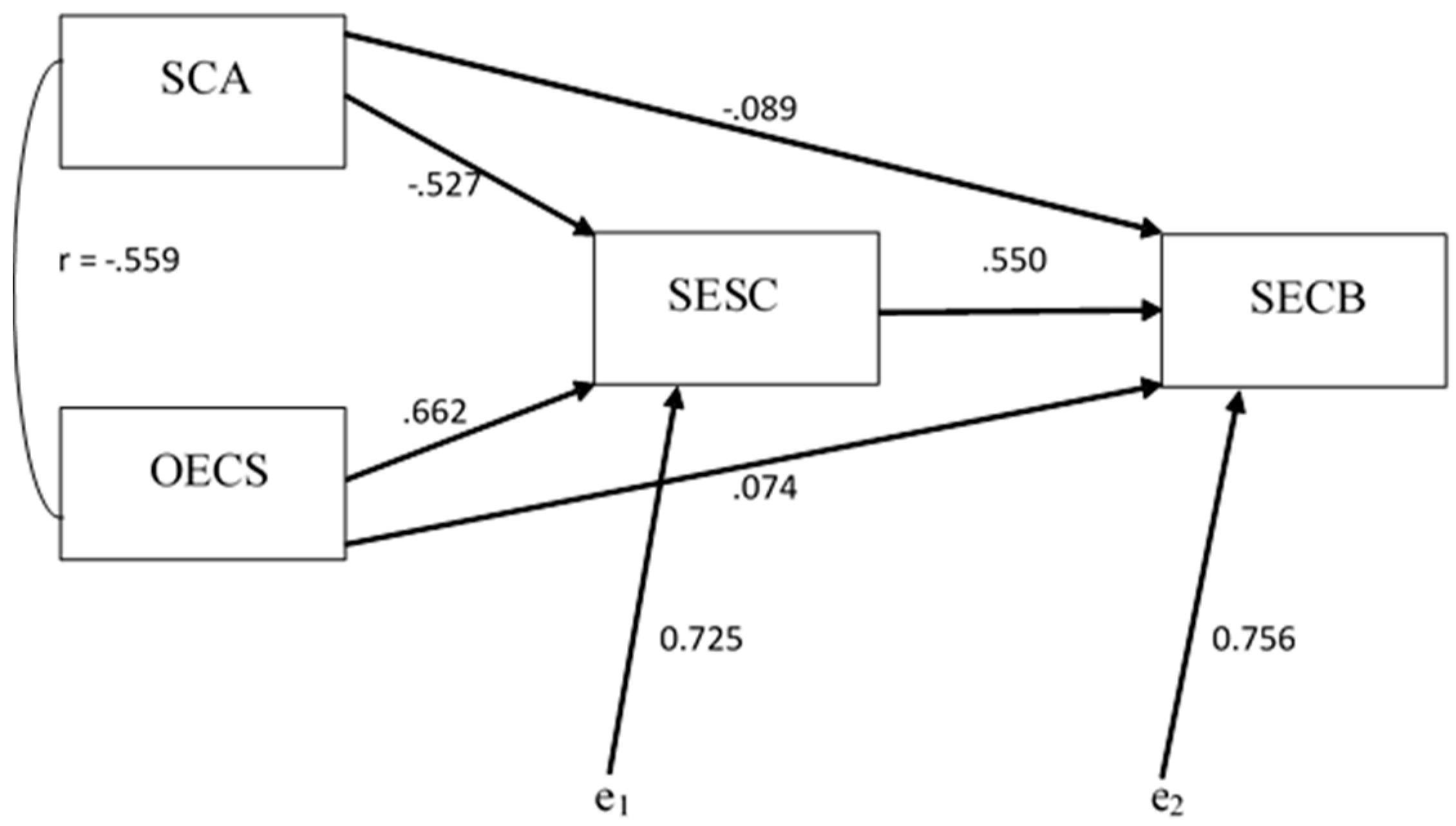
A two-step hierarchical regression analysis was carried out to test the third hypothesis of this study. One of the distal predictors (i.e., MSP) for the SECB criterion was excluded from the analysis due to the fact that previous analyses revealed that it was not a good predictor for the dependent variable of the model. As such, the first predictor block included only SCA as an independent variable while the second regression predictor block contained SESC and OECS (see
Figure 1). Tests of the model data revealed that it met the assumptions of a multiple regression analysis.
The linear hierarchical (2-step) regression analysis returned significant (
p < 0.001) regression equations for both models (steps):
model 1 (only predictor block 1) and
model 2 (predictor blocks 1 and 2) (see
Table 2).
For
model 1, the regression equation was F (1,104) = 22.244,
p < 0.000, with
R2 = 0.176. The level of the predicted SECB was 59.470–0.215 (SCA), where 59.470 was the constant’s regression coefficient value. For
model 2, the regression equation was F (2,102) = 25.465,
p < 0.000, with
R2 = 0.428. The level of the predicted SECB was 7.573 - 0.045 (SCA) + 0.104 (OECS) + 0.201 (SESC), where 7.573 was the constant’s regression coefficient value (see
Table 3). Both models contributed significantly (F value is significant,
p < 0.000) to the capacity of predicting the criterion in comparison to models with estimated population parameters [
44].
Both models explained a significant variance at the criterion level (see
Table 2)
. Model 1 indicated that SCA significantly (
p < 0.000) predicted the criterion SECB, i.e., 17.6% of its variance.
Model 2 indicated that together the three predictors (SCA, OECS and SESC) significantly (
p < 0.000) predicted the criterion SECB, i.e., 42.8% of its variance. Thus, adding the two predictors (in block 2) to the hierarchical regression brought a significant (
p < 0.000) improvement to the prediction model (R
2 change = 0.252) of SECB. Adding OECS and SESC as predictors increased the percentage of criterion-variance prediction by 25.2% [
44].
The values of the adjusted coefficient of determination (
R2 adjust.) for both models of the hierarchical regression analysis were very similar to those of the coefficient of determination
R2 (see
Table 2), which indicates that if they were to be derived from the population and not from the study sample the two models of the hierarchical regression would explain approximately similar levels of the criterion variance. It could be thus said that the two models have a high generalizability level (Field, 2013).
Table 3 indicated that when SCA was the only independent variable in the model, it was a significant predictor for SECB (
t = −4.716,
p < 0.000), but once the other two predictors (OECS and SESC) were introduced in the regression analysis, SCA did not remain significant as a predictor of SECB (
t = −0.950,
p = 0.344). Also, OECS proved not to be a significant predictor for SECB when considered together with the other two predictors (
t = 0.698,
p = 0.487). In this model (i.e., 2) the only predictor that remained significant for the criterion variance was SESC (
t = 5.328,
p < 0.000). Thus, although the three predictors had, separately, a significant direct influence on the criterion (as shown by the results of simple regression analyses), when their interaction was taken into consideration (controlling for levels of any two of them), the only one retaining a significant direct influence on SECB in this model was SESC. SCA and OECS lost their influence in this model as direct predictors of SECB and only showed an indirect influence [
44].
Based on these results a mediation model was proposed with SESC mediating the relation/path between the predictors SCA and OECS with SECB.
Figure 2 describes this model. The validity of this model needs further testing in future studies.
The information offered by the parents in Romania participating in the study based on their answers to the socio-demographic data questionnaire revealed that a percentage of 94.3% (N = 100) did not consider their children to have ever been in a sexual risk situation. Only 31.13% (N = 33) of them were able to describe what in their opinion could constitute such a situation (e.g., exposure to online pornography, unprotected sex or being approached for sex by strangers, adults or older children/young people). 23.6% (n = 25) of the 106 participants reported that they had never used any type of resources to help them with the communication about sexuality and sexuality education they provided to their children; the majority of the participants, 64.2% (n = 68), mentioned books as a source of information, while 56.6% (n = 60) of them mentioned online resources and 40.6% (n = 43) of them mentioned talking to friends. Only 17.9% (n = 19) had talked to professionals while 11.3% (n = 12) had attended a specific course/training. During the 6 months prior to the study, 35 (33%) participants did not use any type of resource, 27 (25.5%) participants used them rarely, another 27 participants used them moderately frequently, while only 14 (13.2%) used them quite frequently and 3 (2.8%) used them very frequently. 17.9% (n = 19) of participants had not communicated to their children about sexuality in the 6 months prior to the study, 27.4% (n = 29) had only communicated rarely, 32.1% (n = 34) had communicated moderately frequently, 21.7% (n = 23) quite often, and 0.9% (n = 1) reported communicating very often.
Participants’ self-rated level of religiosity was not a good predictor for any of the variables of the study. The number of sexual partners that participants estimated they had had by that time (
M = 4.86,
SD = 5.109) proved to be a moderate predictor for their level of self-efficacy regarding communication with children on sexuality topics and for their level of sexuality education parenting behavior. The majority of participants responded to the three optional open-ended questions in PCSQ [
40] regarding communication about sexuality and sexuality education programs, i.e., all of the participants responded to the question “Please describe how you communicate with your child about sexuality?”, more than 99% of them responded to “What would make it easier for you to talk to your child about sexuality?” and 95% responded to “What additional information or topics would you like to see included in a parenting program to help parents develop skills to support children’s developing sexuality?”.
The responses to the first of these questions were very diverse, although participants predominantly answered that they communicated “openly” and in a “relaxed” way, and that they had “positive” and “natural” conversations on the topic with their children, many using, as expected, the verbal approach to communication. Only seven participants stated they didn’t communicate with their children about sexuality, citing mainly the child’s “inappropriate” age as a reason for it. Some parents (around 25%) used the only-answer-when-asked approach, while others (also approximately 25%) mentioned they initiated conversations. Many of them stressed the anatomic and physiological aspects of development in their conversations with their children and expressed beliefs about the “age-appropriateness” of the conversations’ content. One parent said “With honesty, trust and responsibility and without thinking my children are too young to know the truth. I tell them what they need to know at their age based on their cognitive development phase. I answer their questions about sexuality. We do not hide our bodies, we use the appropriate names for genitalia” while another said, “I haven’t talked to my children about this subject. I don’t feel prepared for such conversations. I don’t have the necessary courage to talk to them.”
To the second question, 13 participants responded with “I don’t know”, while 18 parents (17%) said schools (and also sometimes pre-schools) should provide sexuality education classes for children. Participants mostly mentioned the following means of facilitating communication with children about sexuality: being properly informed and trained; having access to various types of resources and support; changed societal and individual (their own) attitudes regarding sexuality; their children’s age and perceived interest for the topic. Almost a fifth of the participants considered that the communication with their children about sexuality was good and it couldn’t be improved. One parent said that “Sexuality education in schools using accurate scientific resources and leaving aside any unnecessary self-consciousness would help”, while another participant responded that ”It would be helpful to involve parents in having all the necessary knowledge to approach all the aspects of sexuality in a competent and relaxed way”.
To the third open-ended question, approximately one third of the participants responded by saying they wouldn’t add anything to a sexuality education parenting program besides the topics already mentioned in the previous item of PCSQ. Almost a quarter of the respondents considered that the parent-child relationship and communication about sexuality should be part of a parental sexuality education program, and a similar number of parents thought that such a program should include information on how to access accurate information sources for both parents and children and also information about children’s and adolescents’ development and about age-appropriate communication. Approximately 10% of the parents considered that information about negative consequences of sexual activity, sexually transmitted infections, protection, pregnancy and contraception, sexual orientation and gender identity, morality, religion and their relation to sexuality, should be added. A few parents mentioned that a sexuality education parenting program should also be about romantic relationships, consent, abuse, media influence and pornography. One participant said that “If we want a healthier generation, adopting older generations’ models will only bring negative consequences; as such, sexuality education should be provided by professionals and with minimum involvement from dilettantes in the subject, be they well-intended parents” and another noted, “How to communicate so that we don’t push them away from us and that they come and ask for advice when they need it, even in this sensitive domain. Children rarely talk to their parents about this subject”.
4. Discussion
The results of the investigation on parents from Romania support the fact that participants’ level of sexual communication (with their partner) anxiety predicted their level of parental outcome expectancy and self-efficacy regarding communication with children about sexuality, as well as the level of communication-with-children-about-sexuality behavior they engaged in.
With regard to the sexual perfectionism dimensions, partners’ self-directed (towards respondent) sexual perfectionism was found to be a significant predictor for respondents’ level of sexual communication anxiety and for their level of parental self-efficacy about discussing sexuality. Moreover, this dimension of sexual perfectionism proved to be significantly correlated with the majority of the study’s variables and their dimensions, with the exception of parental communication-about-sexuality-and-sexuality-education behavior. As a result of that, sexual perfectionism was replaced by this dimension (partners’ self-directed sexual perfectionism) throughout the following analyses of the study. Sexual communication anxiety and partners’ self-directed sexual perfectionism together significantly predicted the level of parental self-efficacy of communication with children about sexuality, sexual communication anxiety being a mediator in their relation. Other multiple prediction models were not tested due to the fact that partners’ self-directed sexual perfectionism was not a significant predictor for the other variables. Since no prior results on this subject (hypothesis 1) were found in literature, a comparison could not be made, but theoretical models and other connected results encouraged such a hypothesis being formulated and the attempt made in this direction by this study indicated promising results.
Regarding the second hypothesis of the study, the data analysis revealed that parental self-efficacy and outcome expectancy about communicating with children on topics of sexuality were significant predictors (both separately and together) for the parental level of communication about sexuality and sexual education with the children. Parents’ communication self-efficacy appeared to mediate the relation of the other two variables.
Both self-efficacy and outcome expectancy were good predictors for each other. When taking into account their interaction, only self-efficacy about communicating with children on sexuality topics remained significant in predicting the level of communication behavior between parents and children about sexuality. These results confirmed, on the one hand, the predictions of Bandura’s theory of self-efficacy regarding the role that self-efficacy and outcome expectancy played in predicting the performance and intention to perform certain behaviors. On the other hand, they partially contradicted Bandura’s view [
28] of these processes, offering alongside other results [
45] valuable insights about the possibility of a bi-causal relation existing between parental self-efficacy and outcome expectancy with regard to their communication with children on sexuality topics.
The third hypothesis of the study tested a two-step multiple prediction model for the level of parental communication-with-children-about-sexuality behavior. Sexual communication anxiety was a predictor in the first block of predictors and parental outcome expectancy and self-efficacy regarding communication with children about sexuality were in the second prediction block. The results of the model testing pointed out that only parental self-efficacy about communication with children on sexuality topics remained a significant predictor for their levels of parenting behavior in that respect. The other two predictors had only an indirect effect over the parental communication with children about sexuality. A path model describing these relations was built. These findings are among the very few results proposing a model that describes the relations between these variables (i.e., characterizing parents’ perceptions of their couple relationship and of their parental relationship and parenting aspects) with an explanatory value for the variance in the levels of parents’ communication-with-children-about-sexuality behavior and with implications both at a theoretical and a practical level.
From a practical point of view, these results have a potential applicability in the configuration of new or in the adjustment of already-existing family counselling interventions, as well as in educational approaches such as sexuality education programs addressed to young people and/or to their parents. Based on the explored model of prediction and mediation from this study, these interventions could target the perception of a couple’s sexual relationship or of the parent-child relationship with the projected outcome of changing the sexuality-communication behavior between parents and children while also bringing other secondary benefits in the parent-child relationship and also in the couple relationship. Specifically, these benefits refer to lowering the levels of anxiety about communication on sexual topics with one’s partner or the levels of one’s sexual perfectionism, which in turn could contribute to the quality of one’s intimate relationships. Understandably, these results, especially the ones obtained by testing exploratory hypotheses, need further investigation in future studies with the purpose of better comprehending this research area and the associations between individual characteristics, family dynamics and processes which influence the sexual health outcomes in young people.
There are some possible limitations to the conclusions drawn from the results of this study. Among them might be the characteristics of the study sample (e.g., mostly women, mostly married or in a long-term relationship, mostly holding a university degree), while others relate to the study procedure and the assessment instruments (e.g., access restricted to online participation, some of instruments translated but not validated), and others relate to the data sample. Our opinion is that these possible limitations affecting the generalizability of our conclusions could be seen as an opportunity and a basis for future studies, where their influence on the results could be additionally investigated and understood.
In conclusion, the study successfully explored and investigated how factors characterizing parents-from-Romania’s perceptions of their (sexual) couple relationships and of their parent-child relationships were both relevant for their communication with their children on sexual topics. The more anxious participating parents were about communicating about sexual issues with their partner and the less confident they were about their capacity to communicate with their children about sexuality or about the effects of such a communication, the less likely they were to talk with their children about sexuality.




{kind=link}
{kind=link}