Impact of Anesthetics on Cardioprotection Induced by Pharmacological Preconditioning

 ,
,
Abstract
:1. Introduction
2. Material and Methods
2.1. Surgical Preparation
2.2. Experimental Protocol
2.3. Statistical Analysis
3. Results
3.1. Animal Characteristics
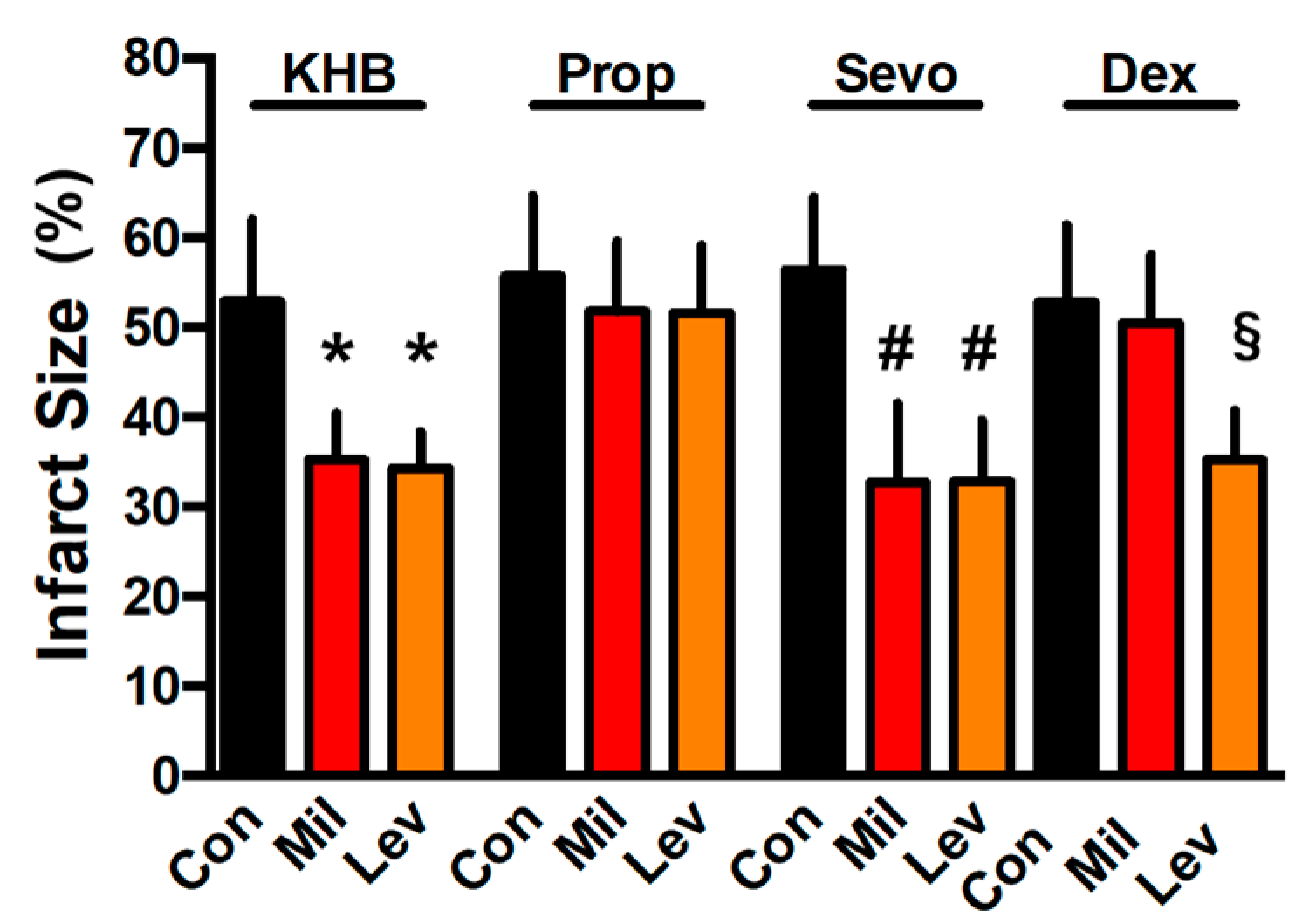
3.2. Infarct Size
3.3. Hemodynamics
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Behmenburg, F.; Trefz, L.; Dorsch, M.; Strothoff, M.; Mathes, A.; Raupach, A.; Heinen, A.; Hollmann, M.W.; Berger, M.M.; Huhn, R. Milrinone-Induced Postconditioning Requires Activation of Mitochondrial Ca2+-Sensitive Potassium (Mbkca) Channels. J. Cardiothorac. Vasc. Anesth. 2017. [Google Scholar] [CrossRef] [PubMed]
- Behmenburg, F.; van Caster, P.; Bunte, S.; Brsandenburger, T.; Heinen, A.; Hollmann, M.W.; Huhn, R. Impact of Anesthetic Regimen on Remote Ischemic Preconditioning in the Rat Heart in Vivo. Anesth. Analg. 2018, 126, 1377–1380. [Google Scholar] [CrossRef] [PubMed]
- Bunte, S.; Behmenburg, F.; Bongartz, A.; Stroethoff, M.; Raupach, A.; Heinen, A.; Minol, J.P.; Hollmann, M.W.; Huhn, R.; Sixt, S.U. Preconditioning by Levosimendan Is Mediated by Activation of Mitochondrial Ca2+-Sensitive Potassium (Mbkca) Channels. Cardiovasc. Drugs Ther. 2018. [Google Scholar] [CrossRef] [PubMed]
- Bunte, S.; Behmenburg, F.; Eckelskemper, F.; Mohr, F.; Stroethoff, M.; Raupach, A.; Heinen, A.; Hollmann, M.W.; Huhn, R. Cardioprotection by Humoral Factors Released after Remote Ischemic Preconditioning Depends on Anesthetic Regimen. Crit. Care Med. 2019. [Google Scholar] [CrossRef] [PubMed]
- Murry, C.E.; Jennings, R.B.; Reimer, K.A. Preconditioning with Ischemia: A Delay of Lethal Cell Injury in Ischemic Myocardium. Circulation 1986, 74, 1124–1136. [Google Scholar] [CrossRef] [PubMed]
- Przyklenk, K.; Bauer, B.; Ovize, M.; Kloner, R.A.; Whittaker, P. Regional Ischemic ‘Preconditioning’ Protects Remote Virgin Myocardium from Subsequent Sustained Coronary Occlusion. Circulation 1993, 87, 893–899. [Google Scholar] [CrossRef]
- Shimizu, M.; Tropak, M.; Diaz, R.J.; Suto, F.; Surendra, H.; Kuzmin, E.; Li, J.; Gross, G.; Wilson, G.J.; Callahan, J.; et al. Transient Limb Ischaemia Remotely Preconditions through a Humoral Mechanism Acting Directly on the Myocardium: Evidence Suggesting Cross-Species Protection. Clin. Sci. (Lond.) 2009, 117, 191–200. [Google Scholar] [CrossRef]
- Zhang, J.; Zhang, J.; Yu, P.; Chen, M.; Peng, Q.; Wang, Z.; Dong, N. Remote Ischaemic Preconditioning and Sevoflurane Postconditioning Synergistically Protect Rats from Myocardial Injury Induced by Ischemia and Reperfusion Partly Via Inhibition Tlr4/Myd88/Nf-Kappab Signaling Pathway. Cell. Physiol. Biochem. 2017, 41, 22–32. [Google Scholar] [CrossRef]
- Thielmann, M.; Kottenberg, E.; Kleinbongard, P.; Wendt, D.; Gedik, N.; Pasa, S.; Price, V.; Tsagakis, K.; Neuhauser, M.; Peters, J.; et al. Cardioprotective and Prognostic Effects of Remote Ischaemic Preconditioning in Patients Undergoing Coronary Artery Bypass Surgery: A Single-Centre Randomised, Double-Blind, Controlled Trial. Lancet 2013, 382, 597–604. [Google Scholar] [CrossRef]
- Botker, H.E.; Kharbanda, R.; Schmidt, M.R.; Bottcher, M.; Kaltoft, A.K.; Terkelsen, C.J.; Munk, K.; Andersen, N.H.; Hansen, T.M.; Trautner, S.; et al. Remote Ischaemic Conditioning before Hospital Admission, as a Complement to Angioplasty, and Effect on Myocardial Salvage in Patients with Acute Myocardial Infarction: A Randomised Trial. Lancet 2010, 375, 727–734. [Google Scholar] [CrossRef]
- Meybohm, P.; Bein, B.; Brosteanu, O.; Cremer, J.; Gruenewald, M.; Stoppe, C.; Coburn, M.; Schaelte, G.; Boning, A.; Niemann, B.; et al. A Multicenter Trial of Remote Ischemic Preconditioning for Heart Surgery. N. Engl. J. Med. 2015, 373, 1397–1407. [Google Scholar] [CrossRef] [PubMed]
- Hausenloy, D.J.; Candilio, L.; Evans, R.; Ariti, C.; Jenkins, D.P.; Kolvekar, S.; Knight, R.; Kunst, G.; Laing, C.; Nicholas, J.; et al. Remote Ischemic Preconditioning and Outcomes of Cardiac Surgery. N. Engl. J. Med. 2015, 373, 1408–1417. [Google Scholar] [CrossRef] [PubMed]
- Behmenburg, F.; Boekholt, Y.; van Caster, P.; Dorsch, M.; Heinen, A.; Hollmann, M.W.; Huhn, R. Extended Second Window of Protection of Sevoflurane-Induced Preconditioning. J. Cardiovasc. Pharmacol. 2017, 70, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, M.; Behmenburg, F.; Raible, M.; Blase, D.; Grievink, H.; Hollmann, M.W.; Heinen, A.; Huhn, R. Morphine-Induced Preconditioning: Involvement of Protein Kinase a and Mitochondrial Permeability Transition Pore. PLoS ONE 2016, 11, e0151025. [Google Scholar] [CrossRef] [PubMed]
- Frassdorf, J.; Huhn, R.; Niersmann, C.; Weber, N.C.; Schlack, W.; Preckel, B.; Hollmann, M.W. Morphine Induces Preconditioning Via Activation of Mitochondrial K(Ca) Channels. Can. J. Anaesth 2010, 57, 767–773. [Google Scholar] [CrossRef] [PubMed]
- Lepran, I.; Pollesello, P.; Vajda, S.; Varro, A.; Papp, J.G. Preconditioning Effects of Levosimendan in a Rabbit Cardiac Ischemia-Reperfusion Model. J. Cardiovasc. Pharmacol. 2006, 48, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Huhn, R.; Heinen, A.; Weber, N.C.; Schlack, W.; Preckel, B.; Hollmann, M.W. Ischaemic and Morphine-Induced Post-Conditioning: Impact of Mk(Ca) Channels. Br. J. Anaesth. 2010, 105, 589–595. [Google Scholar] [CrossRef]
- Behmenburg, F.; Dorsch, M.; Huhn, R.; Mally, D.; Heinen, A.; Hollmann, M.W.; Berger, M.M. Impact of Mitochondrial Ca2+-Sensitive Potassium (Mbkca) Channels in Sildenafil-Induced Cardioprotection in Rats. PLoS ONE 2015, 10, e0144737. [Google Scholar] [CrossRef]
- Riess, M.L.; Kevin, L.G.; Camara, A.K.; Heisner, J.S.; Stowe, D.F. Dual Exposure to Sevoflurane Improves Anesthetic Preconditioning in Intact Hearts. Anesthesiology 2004, 100, 569–574. [Google Scholar] [CrossRef]
- Coverdale, N.S.; Hamilton, A.; Petsikas, D.; McClure, R.S.; Malik, P.; Milne, B.; Saha, T.; Zelt, D.; Brown, P.; Payne, D.M. Remote Ischemic Preconditioning in High-Risk Cardiovascular Surgery Patients: A Randomized-Controlled Trial. Semin. Thorac. Cardiovasc. Surg. 2017. [Google Scholar] [CrossRef]
- Ayres, J.K.; Maani, C.V. Milrinone. In Statpearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2018. [Google Scholar]
- Harjola, V.P.; Giannakoulas, G.; von Lewinski, D.; Matskeplishvili, S.; Mebazaa, A.; Papp, Z.; Schwinger, R.H.G.; Pollesello, P.; Parissis, J.T. Use of Levosimendan in Acute Heart Failure. Eur. Heart J. Suppl. 2018, 20, I2–I10. [Google Scholar] [CrossRef]
- Kottenberg, E.; Thielmann, M.; Bergmann, L.; Heine, T.; Jakob, H.; Heusch, G.; Peters, J. Protection by Remote Ischemic Preconditioning During Coronary Artery Bypass Graft Surgery with Isoflurane but Not Propofol—A Clinical Trial. Acta Anaesthesiol. Scand. 2012, 56, 30–38. [Google Scholar] [CrossRef]
- Berger, M.M.; Huhn, R.; Oei, G.T.; Heinen, A.; Winzer, A.; Bauer, I.; Preckel, B.; Weber, N.C.; Schlack, W.; Hollmann, M.W. Hypoxia Induces Late Preconditioning in the Rat Heart in Vivo. Anesthesiology 2010, 113, 1351–1360. [Google Scholar] [CrossRef]
- Bein, B.; Renner, J.; Caliebe, D.; Hanss, R.; Bauer, M.; Fraund, S.; Scholz, J. The Effects of Interrupted or Continuous Administration of Sevoflurane on Preconditioning before Cardio-Pulmonary Bypass in Coronary Artery Surgery: Comparison with Continuous Propofol. Anaesthesia 2008, 63, 1046–1055. [Google Scholar] [CrossRef]
- Behmenburg, F.; Heinen, A.; Bruch, L.V.; Hollmann, M.W.; Huhn, R. Cardioprotection by Remote Ischemic Preconditioning Is Blocked in the Aged Rat Heart in Vivo. J. Cardiothorac. Vasc. Anesth. 2017, 31, 1223–1226. [Google Scholar] [CrossRef]
- Heinen, A.; Behmenburg, F.; Aytulun, A.; Dierkes, M.; Zerbin, L.; Kaisers, W.; Schaefer, M.; Meyer-Treschan, T.; Feit, S.; Bauer, I.; et al. The Release of Cardioprotective Humoral Factors after Remote Ischemic Preconditioning in Humans Is Age- and Sex-Dependent. J. Transl. Med. 2018, 16, 112. [Google Scholar] [CrossRef]
- Heinen, A.; Winning, A.; Schlack, W.; Hollmann, M.W.; Preckel, B.; Frassdorf, J.; Weber, N.C. The Regulation of Mitochondrial Respiration by Opening of Mkca Channels Is Age-Dependent. Eur. J. Pharmacol. 2008, 578, 108–113. [Google Scholar] [CrossRef]
- Huhn, R.; Weber, N.C.; Preckel, B.; Schlack, W.; Bauer, I.; Hollmann, M.W.; Heinen, A. Age-Related Loss of Cardiac Preconditioning: Impact of Protein Kinase A. Exp. Gerontol. 2012, 47, 116–121. [Google Scholar] [CrossRef]
- Ferdinandy, P.; Hausenloy, D.J.; Heusch, G.; Baxter, G.F.; Schulz, R. Interaction of Risk Factors, Comorbidities, and Comedications with Ischemia/Reperfusion Injury and Cardioprotection by Preconditioning, Postconditioning, and Remote Conditioning. Pharmacol. Rev. 2014, 66, 1142–1174. [Google Scholar] [CrossRef]
- Canadian Institutes of Health Research; Alberta Innovates - Health Solutions; The Metabolomics Innovation Centre (TMIC). Drugbank Database. Available online: https://www.drugbank.ca/drugs/DB00235 (accessed on 20 December 2018).
- Xiao, Y.; Lei, S.; Huang, Y.; Zhao, Bo.; Wang, H.; Cao, H.; Xia, Z. Dexmedetomidine Protects against Renal Ischemia and Reperfusion Injury by Inhibiting the P38-Mapk/Txnip Signaling Activation in Streptozotocin Induced Diabetic Rats. Acta Cir. Bras. 2017, 32, 429–439. [Google Scholar] [CrossRef]
- Sanada, S.; Kitakaze, M.; Papst, P.J.; Asanuma, H.; Node, K.; Takashima, S.; Asakura, M.; Ogita, H.; Liao, Y.; Sakata, Y.; et al. Cardioprotective Effect Afforded by Transient Exposure to Phosphodiesterase Iii Inhibitors: The Role of Protein Kinase a and P38 Mitogen-Activated Protein Kinase. Circulation 2001, 104, 705–710. [Google Scholar] [CrossRef]
- Kaheinen, P.; Pollesello, P.; Levijoki, J.; Haikala, H. Effects of Levosimendan and Milrinone on Oxygen Consumption in Isolated Guinea-Pig Heart. J. Cardiovasc. Pharmacol. 2004, 43, 555–561. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n | Body Weight (g) | Heart Weight Dry (g) | Heart Weight Wet (g) | Time of Max. Ischemic Contracture (min) | Level of Max. Ischemic Contracture (min) | ||
|---|---|---|---|---|---|---|---|
| KHB | Con | 8 | 301 ± 10 | 0.14 ± 0.02 | 1.47 ± 0.12 | 15:46 ± 1:42 | 54 ± 7 |
| Mil | 7 | 299 ± 23 | 0.15 ± 0.01 | 1.46 ± 0.11 | 16:27 ± 1:18 | 54 ± 11 | |
| Lev | 7 | 291 ± 21 | 0.14 ± 0.01 | 1.32 ± 0.14 | 15:39 ± 0:39 | 56 ± 12 | |
| Prop | Con | 8 | 286 ± 17 | 0.13 ± 0.02 | 1.44 ± 0.11 | 16:17 ± 1:05 | 59 ± 12 |
| Mil | 8 | 303 ± 23 | 0.16 ± 0.02 | 1.46 ± 0.08 | 16:00 ± 1:10 | 55 ± 4 | |
| Lev | 8 | 299 ± 26 | 0.15 ± 0.01 | 1.47 ± 0.11 | 16:26 ± 1:59 | 61 ± 11 | |
| Sevo | Con | 7 | 300 ± 08 | 0.12 ± 0.01 | 1.34 ± 0.06 | 14:26 ± 0:23 | 82 ± 13 |
| Mil | 7 | 298 ± 19 | 0.13 ± 0.01 | 1.30 ± 0.06 | 15:05 ± 1:53 | 70 ± 13 | |
| Lev | 7 | 297 ± 11 | 0.13 ± 0.01 | 1.29 ± 0.07 | 14:40 ± 1:07 | 81 ± 11 | |
| Dex | Con | 8 | 293 ± 18 | 0.14 ± 0.03 | 1.42 ± 0.09 | 15:21 ± 2:10 | 67 ± 17 |
| Mil | 8 | 290 ± 19 | 0.14 ± 0.02 | 1.41 ± 0.07 | 16:16 ± 1:54 | 55 ± 9 | |
| Lev | 7 | 296 ± 11 | 0.15 ± 0.02 | 1.42 ± 0.09 | 16:14 ± 1:23 | 55 ± 10 |
| Group | Baseline | PC | Reperfusion | ||
|---|---|---|---|---|---|
| 30 | 60 | ||||
| Heart Rate (bpm) | |||||
| KHB | Con | 333 ± 40 | 314 ± 42 | 279 ± 92 | 275 ± 62 |
| Mil | 327 ± 48 | 347 ± 44 | 242 ± 61 | 275 ± 43 | |
| Lev | 318 ± 39 | 312 ± 33 | 274 ± 34 | 258 ± 36 | |
| Prop | Con | 308 ± 32 | 294 ± 32 | 183 ± 69 * | 180 ± 67 * |
| Mil | 313 ± 30 | 293 ± 27 | 237 ± 46 | 212 ± 54 | |
| Lev | 316 ± 50 | 300 ± 51 | 208 ± 77 | 212 ± 74 | |
| Sevo | Con | 296 ± 23 | 271 ± 28 | 246 ± 20 | 215 ± 45 |
| Mil | 345 ± 38 | 367 ± 32 | 221 ± 60 | 266 ± 63 | |
| Lev | 304 ± 37 | 300 ± 27 | 271 ± 37 | 253 ± 32 | |
| Dex | Con | 308 ± 27 | 286 ± 15 | 248 ± 53 | 247 ± 28 |
| Mil | 318 ± 43 | 309 ± 39 | 257 ± 46 | 264 ± 26 | |
| Lev | 331 ± 54 | 328 ± 36 | 304 ± 36 | 265 ± 54 | |
| Phasic LVP (mmHg) | |||||
| KHB | Con | 117 ± 16 | 122 ± 10 | 17 ± 8 * | 22 ± 7 * |
| Mil | 130 ± 16 | 115 ± 13 | 15 ± 5 * | 19 ± 6 * | |
| Lev | 109 ± 17 | 116 ± 17 | 25 ± 15 * | 25 ± 11 * | |
| Prop | Con | 132 ± 20 | 126 ± 20 | 17 ± 8 * | 28 ± 14 * |
| Mil | 118 ± 18 | 119 ± 19 | 20 ± 4 * | 31 ± 11 * | |
| Lev | 130 ± 12 | 131 ± 13 | 20 ± 9 * | 27 ± 6 * | |
| Sevo | Con | 144 ± 17 | 145 ± 23 | 25 ± 14 * | 32 ± 10 * |
| Mil | 129 ± 19 | 143 ± 24 | 26 ± 13 * | 39 ± 18 * | |
| Lev | 136 ± 24 | 139 ± 11 | 27 ± 12 * | 35 ± 10 * | |
| Dex | Con | 124 ± 16 | 113 ± 20 | 21 ± 10 * | 29 ± 12 * |
| Mil | 123 ± 15 | 125 ± 17 | 27 ± 13 * | 30 ± 8 * | |
| Lev | 126 ± 11 | 127 ± 10 | 24 ± 14 * | 24 ± 10 * | |
| CF (mL·min−1) | |||||
| KHB | Con | 17 ± 3 | 15 ± 4 | 10 ± 1 * | 8 ± 1 * |
| Mil | 18 ± 2 | 16 ± 2 | 9 ± 2 * | 8 ± 2 * | |
| Lev | 15 ± 2 | 17 ± 2 | 7 ± 2 * | 5 ± 2 * | |
| Prop | Con | 17 ± 1 | 16 ± 1 | 9 ± 1 * | 7 ± 1 * |
| Mil | 16 ± 2 | 18 ± 3 | 10 ± 1 * | 8 ± 2 * | |
| Lev | 16 ± 1 | 19 ± 2 | 10 ± 2 * | 8 ± 2 * | |
| Sevo | Con | 15 ± 3 | 14 ± 3 * | 9 ± 2 * | 7 ± 2 * |
| Mil | 17 ± 3 | 18 ± 3 * | 11 ± 4 * | 9 ± 3 * | |
| Lev | 14 ± 3 | 17 ± 2 | 8 ± 3 * | 7 ± 3 * | |
| Dex | Con | 16 ± 3 | 14 ± 4 | 8 ± 1 * | 6 ± 1 * |
| Mil | 16 ± 2 | 14 ± 2 | 7 ± 3 * | 7 ± 1 * | |
| Lev | 19 ± 2 | 18 ± 3 | 9 ± 2 * | 7 ± 2 * | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bunte, S.; Lill, T.; Falk, M.; Stroethoff, M.; Raupach, A.; Mathes, A.; Heinen, A.; Hollmann, M.W.; Huhn, R. Impact of Anesthetics on Cardioprotection Induced by Pharmacological Preconditioning. J. Clin. Med. 2019, 8, 396. https://doi.org/10.3390/jcm8030396
Bunte S, Lill T, Falk M, Stroethoff M, Raupach A, Mathes A, Heinen A, Hollmann MW, Huhn R. Impact of Anesthetics on Cardioprotection Induced by Pharmacological Preconditioning. Journal of Clinical Medicine. 2019; 8(3):396. https://doi.org/10.3390/jcm8030396
Chicago/Turabian StyleBunte, Sebastian, Tobias Lill, Maximilian Falk, Martin Stroethoff, Annika Raupach, Alexander Mathes, André Heinen, Markus W. Hollmann, and Ragnar Huhn. 2019. "Impact of Anesthetics on Cardioprotection Induced by Pharmacological Preconditioning" Journal of Clinical Medicine 8, no. 3: 396. https://doi.org/10.3390/jcm8030396
APA StyleBunte, S., Lill, T., Falk, M., Stroethoff, M., Raupach, A., Mathes, A., Heinen, A., Hollmann, M. W., & Huhn, R. (2019). Impact of Anesthetics on Cardioprotection Induced by Pharmacological Preconditioning. Journal of Clinical Medicine, 8(3), 396. https://doi.org/10.3390/jcm8030396