Treatment of Liver Metastases from Midgut Neuroendocrine Tumours: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Methods
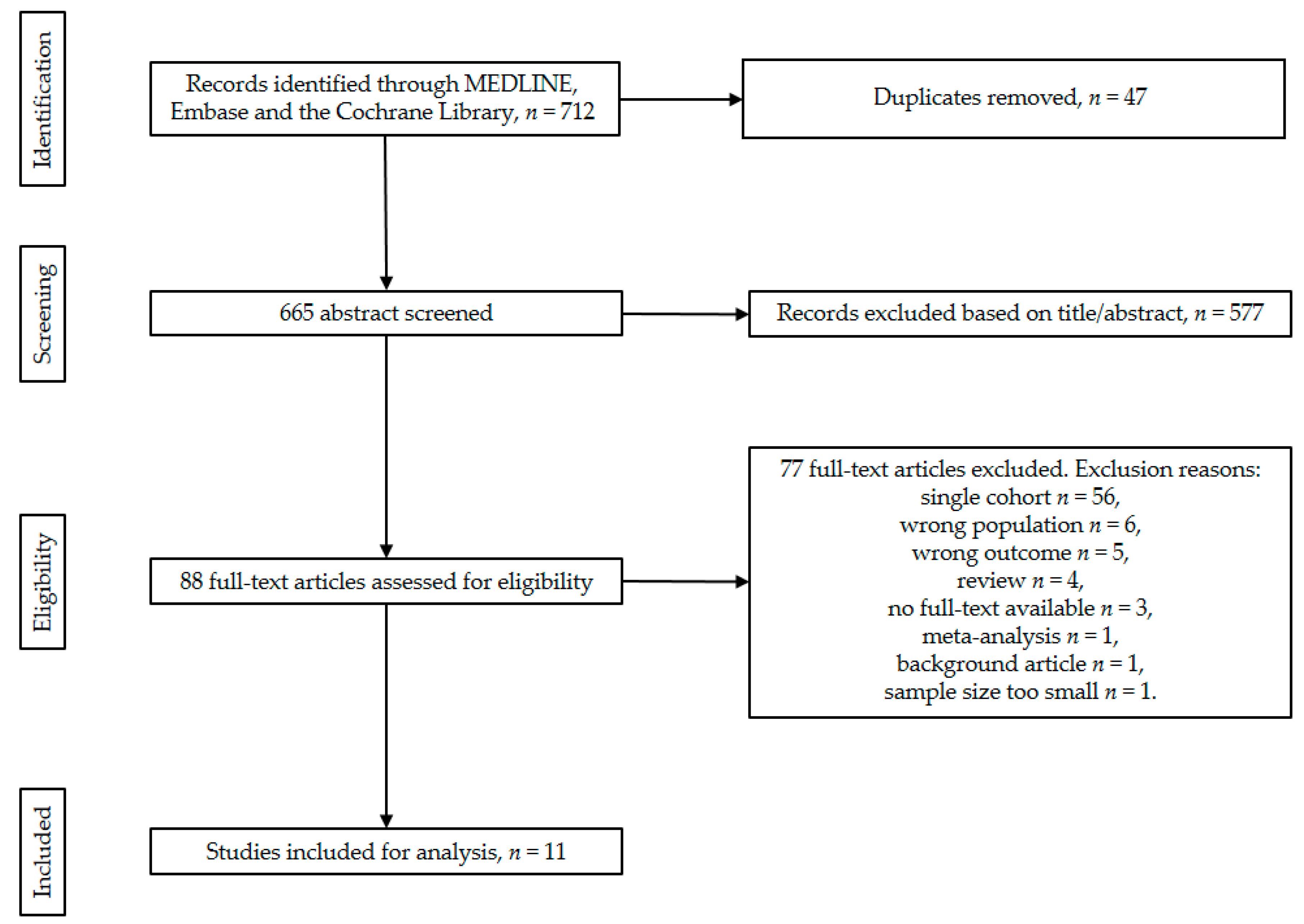
2.1. Search Strategy
2.2. In- and Exclusion Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Statistical Analysis
2.6. Risk of Bias Assessment
3. Results
3.1. Description of Studies
3.2. Resection of Primary Tumour versus No Resection at All
3.3. LM Resection versus No Resection at All
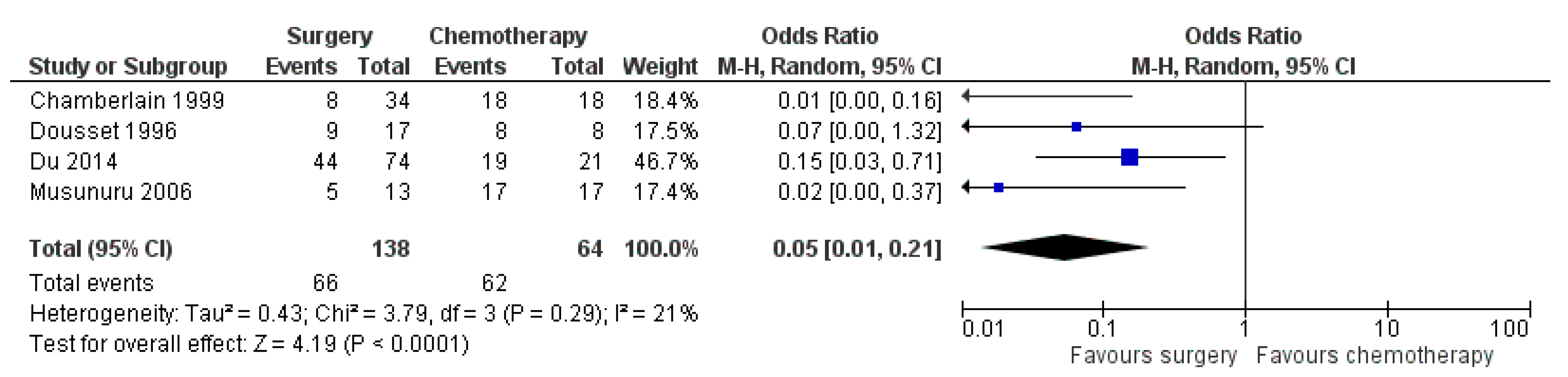
3.4. Any Surgery versus Chemotherapy
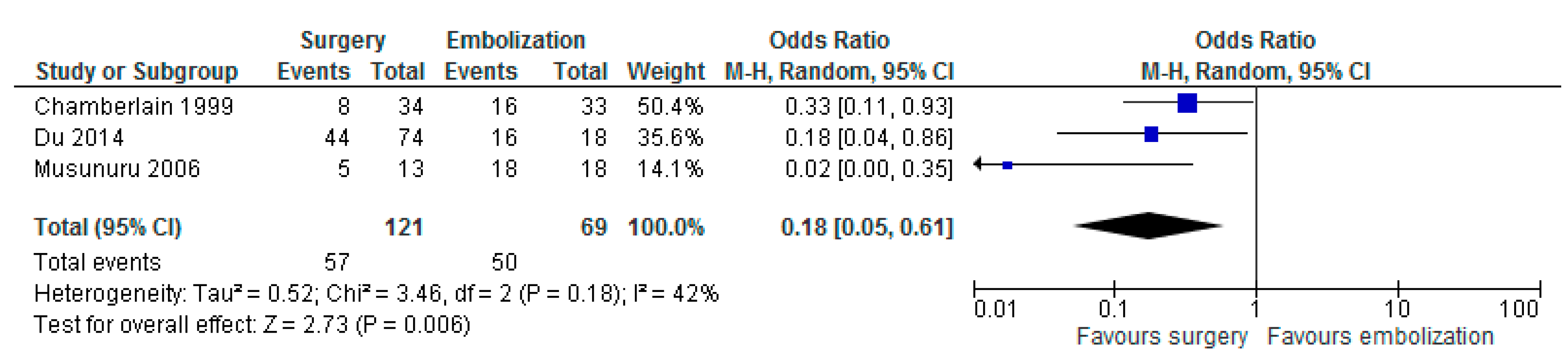
3.5. Any Surgery versus Embolization
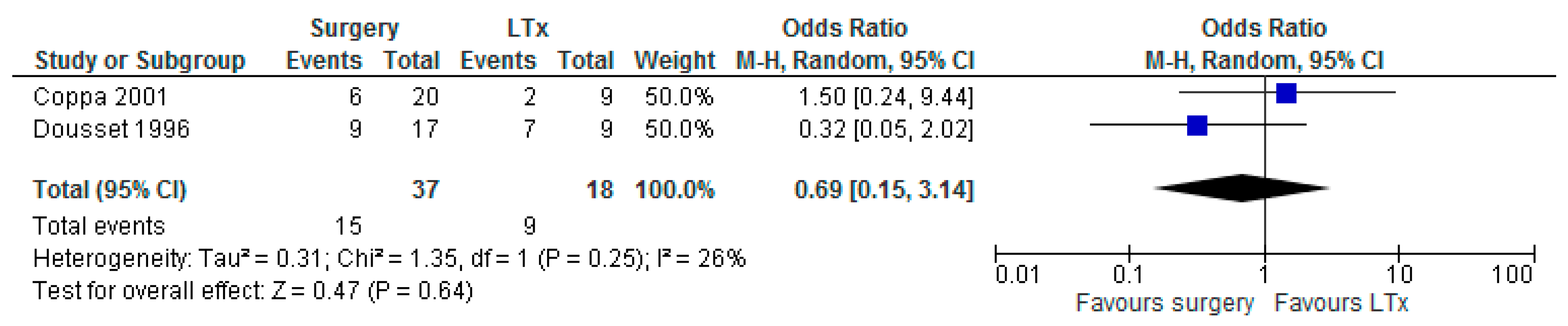
3.6. Any Surgery versus LTx
3.7. Risk of Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Integraal Kankercentrum Nederland (IKNL). Cijfers over Kanker; IKNL: Utrecht, The Netherlands, 2018. [Google Scholar]
- Pavel, M.; Baudin, E.; Couvelard, A.; Krenning, E.; Öberg, K.; Steinmüller, T.; Anlauf, M.; Wiedenmann, B.; Salazar, R. ENETS Consensus Guidelines for the Management of Patients with Liver and Other Distant Metastases from Neuroendocrine Neoplasms of Foregut, Midgut, Hindgut, and Unknown Primary. Neuroendocrinology 2012, 95, 157–176. [Google Scholar] [CrossRef]
- Frilling, A.; Sotiropoulos, G.C.; Li, J.; Kornasiewicz, O.; Plöckinger, U. Multimodal management of neuroendocrine liver metastases. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2010, 12, 361–379. [Google Scholar] [CrossRef]
- Rinke, A.; Muller, H.H.; Schade-Brittinger, C.; Klose, K.J.; Barth, P.; Wied, M.; Mayer, C.; Aminossadati, B.; Pape, U.F.; Blaker, M.; et al. Placebo-controlled, double-blind, prospective, randomized study on the effect of octreotide LAR in the control of tumor growth in patients with metastatic neuroendocrine midgut tumors: A report from the PROMID Study Group. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2009, 27, 4656–4663. [Google Scholar] [CrossRef] [PubMed]
- Caplin, M.E.; Pavel, M.; Ćwikła, J.B.; Phan, A.T.; Raderer, M.; Sedláčková, E.; Cadiot, G.; Wolin, E.M.; Capdevila, J.; Wall, L.; et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2014, 371, 224–233. [Google Scholar] [CrossRef] [PubMed]
- Ruszniewski, P.; Ish-Shalom, S.; Wymenga, M.; O’Toole, D.; Arnold, R.; Tomassetti, P.; Bax, N.; Caplin, M.; Eriksson, B.; Glaser, B.; et al. Rapid and sustained relief from the symptoms of carcinoid syndrome: Results from an open 6-month study of the 28-day prolonged-release formulation of lanreotide. Neuroendocrinology 2004, 80, 244–251. [Google Scholar] [CrossRef]
- Strosberg, J.; El-Haddad, G.; Wolin, E.; Hendifar, A.; Yao, J.; Chasen, B.; Mittra, E.; Kunz, P.L.; Kulke, M.H.; Jacene, H.; et al. Phase 3 Trial of (177)Lu-Dotatate for Midgut Neuroendocrine Tumors. N. Engl. J. Med. 2017, 376, 125–135. [Google Scholar] [CrossRef]
- Raymond, E.; Dahan, L.; Raoul, J.-L.; Bang, Y.-J.; Borbath, I.; Lombard-Bohas, C.; Valle, J.; Metrakos, P.; Smith, D.; Vinik, A.; et al. Sunitinib Malate for the Treatment of Pancreatic Neuroendocrine Tumors. N. Engl. J. Med. 2011, 364, 501–513. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M.; et al. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): A randomised, placebo-controlled, phase 3 study. Lancet 2016, 387, 968–977. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; de Vries, E.G.; et al. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Sward, C.; Johanson, V.; Nieveen van Dijkum, E.; Jansson, S.; Nilsson, O.; Wangberg, B.; Ahlman, H.; Kolby, L. Prolonged survival after hepatic artery embolization in patients with midgut carcinoid syndrome. Br. J. Surg. 2009, 96, 517–521. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]
- Gurusamy, K.S.; Ramamoorthy, R.; Sharma, D.; Davidson, B.R. Liver resection versus other treatments for neuroendocrine tumours in patients with resectable liver metastases. Cochrane Database Syst. Rev. 2009, Cd007060. [Google Scholar] [CrossRef] [PubMed]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, M.N.; Maggiori, L.; Gaujoux, S.; Couvelard, A.; Guedj, N.; Ruszniewski, P.; Panis, Y. Surgery for small-bowel neuroendocrine tumors: Is there any benefit of the laparoscopic approach? Surg. Endosc. 2014, 28, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed]
- Bertani, E.; Fazio, N.; Radice, D.; Zardini, C.; Spinoglio, G.; Chiappa, A.; Ribero, D.; Biffi, R.; Partelli, S.; Falconi, M. Assessing the role of primary tumour resection in patients with synchronous unresectable liver metastases from pancreatic neuroendocrine tumour of the body and tail. A propensity score survival evaluation. Eur. J. Surg. Oncol. 2017, 43, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Boyar Cetinkaya, R.; Vatn, M.; Aabakken, L.; Bergestuen, D.S.; Thiis-Evensen, E. Survival and prognostic factors in well-differentiated pancreatic neuroendocrine tumors. Scand. J. Gastroenterol. 2014, 49, 734–741. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, R.S.; Canes, D.; Brown, K.T.; Saltz, L.; Jarnagin, W.; Fong, Y.; Blumgart, L.H. Hepatic neuroendocrine metastases: Does intervention alter outcomes? J. Am. Coll. Surg. 2000, 190, 432–445. [Google Scholar] [CrossRef]
- Chen, H.; Hardacre, J.M.; Uzar, A.; Cameron, J.L.; Choti, M.A. Isolated liver metastases from neuroendocrine tumors: Does resection prolong survival? J. Am. Coll. Surg. 1998, 187, 88–92; discussion 92–93. [Google Scholar] [CrossRef]
- Citterio, D.; Pusceddu, S.; Facciorusso, A.; Coppa, J.; Milione, M.; Buzzoni, R.; Bongini, M.; deBraud, F.; Mazzaferro, V. Primary tumour resection may improve survival in functional well-differentiated neuroendocrine tumours metastatic to the liver. Eur. J. Surg. Oncol. 2017, 43, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Coppa, J.; Pulvirenti, A.; Schiavo, M.; Romito, R.; Collini, P.; Di Bartolomeo, M.; Fabbri, A.; Regalia, E.; Mazzaferro, V. Resection versus transplantation for liver metastases from neuroendocrine tumors. Transplant. Proc. 2001, 33, 1537–1539. [Google Scholar] [CrossRef]
- Dousset, B.; Saint-Marc, O.; Pitre, J.; Soubrane, O.; Houssin, D.; Chapuis, Y. Metastatic endocrine tumors: Medical treatment, surgical resection, or liver transplantation. World J. Surg. 1996, 20, 908–914, discussion 914–915. [Google Scholar] [CrossRef] [PubMed]
- Du, S.; Wang, Z.; Sang, X.; Lu, X.; Zheng, Y.; Xu, H.; Xu, Y.; Chi, T.; Zhao, H.; Wang, W.; et al. Surgical resection improves the outcome of the patients with neuroendocrine tumor liver metastases: Large data from Asia. Medicine (Baltimore) 2015, 94, e388. [Google Scholar] [CrossRef] [PubMed]
- Musunuru, S.; Chen, H.; Rajpal, S.; Stephani, N.; McDermott, J.C.; Holen, K.; Rikkers, L.F.; Weber, S.M. Metastatic neuroendocrine hepatic tumors: Resection improves survival. Arch. Surg. 2006, 141, 1000–1004, discussion 1005. [Google Scholar] [CrossRef]
- Partelli, S.; Inama, M.; Rinke, A.; Begum, N.; Valente, R.; Fendrich, V.; Tamburrino, D.; Keck, T.; Caplin, M.E.; Bartsch, D.; et al. Long-Term Outcomes of Surgical Management of Pancreatic Neuroendocrine Tumors with Synchronous Liver Metastases. Neuroendocrinology 2015, 102, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Watzka, F.M.; Fottner, C.; Miederer, M.; Schad, A.; Weber, M.M.; Otto, G.; Lang, H.; Musholt, T.J. Surgical therapy of neuroendocrine neoplasm with hepatic metastasis: patient selection and prognosis. Langenbeck’s Arch. Surg. 2015, 400, 349–358. [Google Scholar] [CrossRef]
- Yu, X.; Gu, J.; Wu, H.; Fu, D.; Li, J.; Jin, C. Resection of Liver Metastases: A Treatment Provides a Long-Term Survival Benefit for Patients with Advanced Pancreatic Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. J. Oncol. 2018, 2018, 6273947. [Google Scholar] [CrossRef]
- Partelli, S.; Cirocchi, R.; Rancoita, P.M.V.; Muffatti, F.; Andreasi, V.; Crippa, S.; Tamburrino, D.; Falconi, M. A Systematic review and meta-analysis on the role of palliative primary resection for pancreatic neuroendocrine neoplasm with liver metastases. HPB (Oxford) 2018, 20, 197–203. [Google Scholar] [CrossRef]
- Zhou, B.; Zhan, C.; Ding, Y.; Yan, S.; Zheng, S. Role of palliative resection of the primary pancreatic neuroendocrine tumor in patients with unresectable metastatic liver disease: A systematic review and meta-analysis. OncoTargets Ther. 2018, 11, 975–982. [Google Scholar] [CrossRef]
- Moris, D.; Tsilimigras, D.I.; Ntanasis-Stathopoulos, I.; Beal, E.W.; Felekouras, E.; Vernadakis, S.; Fung, J.J.; Pawlik, T.M. Liver transplantation in patients with liver metastases from neuroendocrine tumors: A systematic review. Surgery 2017, 162, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Design | No. Patients (n) | Inclusion Criteria Per Study | Exclusion Criteria Per Study | Intervention Groups | Control Group |
|---|---|---|---|---|---|---|---|
| Watzka et al. [27] | DE | Retrospective | 204 | Patients with LM of NEN. | N/A | Radical LM resection (n = 38) | No resection at all (n = 110) |
| Partelli et al. [26] | IT | Retrospective | 166 | Patients with synchronous LM from sporadic pNET. | Patients with extra-abdominal disease as well as those with peritoneal carcinomatosis and those with an inherited syndrome. | Radical LM resection + primary resection (n = 18) | No resection at all (n = 75) (SSA; PRRT; chemotherapy; everolimus or sunitinib) |
| Citterio et al. [21] | IT | Retrospective | 139 | ≤20 mitoses/10 high power field (HPF) and Ki-67 labelling index ≤ 20% at either the primary or metastatic sites; Hormone-secreting status associated with a distinct clinical syndrome (functioning NETs); Performance status (PS) 0–1 at presentation, according to the ECOG § | N/A | LM resection (n = 36) (32 were after primary resection) | No resection at all (n = 103) (SSA n = 95, SSA + chemo n = 30, SSA + everolimus n = 14, TACE or RFA + systemic and/or surgical treatment * n = 25) |
| Du et al. [24] | CN | Retrospective | 130 | LM from NET. | N/A | Radical resection of primary tumour (n = 42) | No resection at all (n = 56) (TACE (16/18 also received an RFA) n = 18, systemic chemotherapy n = 9, SSA n = 12, no treatment n = 17) |
| LM + primary resection (R0) n = 26, LM resection (R0) n = 6 | |||||||
| Primary + LM resection n = 26, primary resection n = 42, LM resection n = 6 | Chemotherapy (n = 21) chemotherapy (fluorouracil and/or epirubicin and/or doxorubicin and/or etoposide and/or cisplatin, etc.) n = 9, SSA n = 12) | ||||||
| TACE (n = 18) (16 also received a RFA) | |||||||
| Bertani et al. [17] | IT | Retrospective | 121 | Patients with synchronous and unresectable pNET LM. | N/A | Resection of primary tumour (n = 62) (n = 59 also received PRRT) | No resection at all (n = 59) (PRRT n = 55, SSA n = 29) |
| Boyar et al. [18] | NO | Retrospective | 114 | Patients with (WHO 2010) grade 1 and grade 2 tumours. | N/A | Resection of primary tumour with curative intent (n = 46) | No resection at all (n = 51) (streptozotocin + 5-fluorouracil/doxorubicin; SSA; IFN; embolization; PRRT; M-tor inhibitor) |
| Chamberlain et al. [19] | US | Retrospective | 85 | Patients treated for hepatic NET metastases. | The absence of identifiable liver disease, pathologic review at MSKCC revealing a non-NET or high-grade NET, or a patient decision to seek care elsewhere. | Segmentectomy or enucleation n = 12, lobectomy n = 3, extended resection n = 19 ‡ | Chemotherapy (n = 18) (streptozocin+ 5-FU; streptozocin + doxorubicin; 5-FU + leucovorin or cisplatin + etoposide) |
| HAE, with polyvinyl alcohol particles (n = 33) | |||||||
| Musunuru et al. [25] | US | Retrospective | 48 | Patients with liver-only metastatic neuroendocrine tumours. | N/A | Anatomical liver resection n = 6, ablation n = 4, resection and ablation n = 3 | Chemotherapy (n = 17) (observation, octreotide, and/or systemic chemotherapy) |
| Embolization (n = 18) | |||||||
| Chen et al. [20] | US | Retrospective | 38 | Patients treated for hepatic NET metastases. | Patients with evidence of extrahepatic disease or unresected known primary tumour. | LM resection (n = 15) (12 were combined with primary resection) | No resection at all (n = 23) (chemoembolization n = 5, chemotherapy and radiation n = 6, chemotherapy only n = 3, radiation only n = 2, no therapy n = 7) |
| Dousset et al. [23] | FR | Retrospective | 34 | Patients with metastatic endocrine tumours with bilobar metastases. | N/A | Curative intent resection n = 12 Palliative intent n = 5 † | Chemotherapy (n = 8) (streptozotocin + fluorouracil n = 4, chemoembolization n = 4) |
| LTx (n = 9) | |||||||
| Coppa et al. [22] | IT | Retrospective | 29 | LM from NET, confirmed histological diagnosis. | Non-carcinoid primary tumours, tumours with systemic venous drainage. | Hepatic resection with curative intent (n = 20) | LTx (n = 9) |
| Study | No. Patients (n) | Sex (n, %) | Age (Years) | Primary Tumour Location | LM Size in cm (Median, Range) | Non-Functional NETs (n, %) | Resection of Primary Tumour (n, %) | Resectable/Unresectable LM | Uni-/Bilobar Metastases | Extrahepatic Disease (n, %) | WHO 2010 Grade | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Pancreas (n, %) | Small Bowel (n, %) | Other/Unknown (n, %) | ||||||||||
| Watzka et al. [27] | 204 | 111 (54) | 93 (46) | 58 ± 15 (60) * | 58 (28) | 73 (36) | 73 (36) | N/A | 123 (60) | 165 (81) | Mixed | N/A | N/A | All |
| Partelli et al. [26] | 166 | 92 (55) | 74 (45) | N/A ‡ | 166 | 0 | 0 | LM resection 0.8 cm (0.3–1.7 cm); no resection at all 3.4 cm (1–7 cm) † | 152 (92) | 91 (55) | Resectable | Both | N/A | All |
| Citterio et al. [21] | 139 | 67 (48) | 72 (52) | 56 (51–55) † | 36 (26) | 66 (47) | 37 (27) | N/A | 0 | 93 (67) | Mixed | N/A | N/A | 1–2 |
| Du et al. [24] | 130 | 69 (53) | 61 (47) | 49.0 ± 12.1 (N/A) * | 85 (65) | 7 [5] | 38 (30) | Mean 4.1 cm (range 3–15 cm) | 100 (77) | 68 (52) | Mixed | N/A | N/A | All |
| Bertani et al. [17] | 121 | 66 (55) | 58 (45) | 54.6 ± 12.6 (54.5) * | 121 (100) | 0 | 0 | N/A | 29 (24) | 63 (52) | Unresectable | N/A | 28 (23) | All |
| Boyar et al. [18] | 114 | 61 (54) | 83 (46) | 57 (32–83) † | 111 (97) | 0 | 3 [3] | N/A | 89 (78) | 46 (40) | Mixed | N/A | 51 (45) | 1–2 |
| Chamberlain et al. [19] | 85 | 37 (44) | 48 (56) | 52 (20–79) † | 42 (49) | 0 | 43 (51) | N/A | 49 (58) | 36 (42) | Mixed | Both | 45 (53) | 1–2 |
| Musunuru et al. [25] | 48 | 30 (63) | 18 (37) | N/A | 15 (31) | 0 | 33 (69) | Embolization 8.9 ± 6.1 cm; chemotherapy 3.7 ± 2.9 cm; any resection 4.5 ± 2.3 cm * | N/A | 12 (25) | Unclear | Both | 0 | N/A |
| Chen et al. [20] | 38 | 24 (63) | 14 (37) | N/A ‡ | 11 (29) | 9 (24) | 18 (47) | N/A | 9 (24) | 12 (32) | Mixed | Bilobar | 0 | N/A |
| Dousset et al. [23] | 34 | 18 (53) | 17 (47) | 49.5 (29–76) † | 17 (50) | 9 (26) | 8 (24) | N/A | 5 (15) | 21 (62) | Mixed | Bilobar | 0 | N/A |
| Coppa 2001 et al. [22] | 29 | 13 (45) | 16 (55) | N/A ‡ | 0 | 0 | 29§ | N/A | N/A | 11 (38) | Mixed | N/A | 0 | N/A |
| Bias Due to Confounding | Bias in Selection of Participants into the Study | Bias in Classification of Interventions | Bias Due to Deviations from Intended Interventions | Bias Due to Missing Data | Bias in Measurement of Outcomes | Bias in Selection of the Reported Result | Overall Bias | |
|---|---|---|---|---|---|---|---|---|
| Chamberlain et al. [19] | - | +/- | + | + | +/- | +/- | +/- | - |
| Coppa et al. [22] | - | +/- | + | + | +/- | +/- | +/- | - |
| Du et al. [24] | - | +/- | + | + | +/- | +/- | +/- | - |
| Musunuru et al. [25] | - | +/- | + | + | +/- | +/- | +/- | - |
| Boyar et al. [18] | - | +/- | +/- | + | +/- | +/- | +/- | - |
| Bertani et al. [17] | - | +/- | + | +/- | +/- | +/- | +/- | - |
| Chen et al. [20] | - | +/- | + | +/- | +/- | +/- | +/- | - |
| Citterio et al. [21] | - | +/- | + | +/- | +/- | +/- | +/- | - |
| Partelli et al. [26] | - | +/- | + | +/- | +/- | +/- | +/- | - |
| Watzka et al. [27] | - | +/- | + | +/- | +/- | +/- | +/- | - |
| Dousset et al. [23] | - | +/- | +/- | +/- | +/- | +/- | +/- | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaçmaz, E.; Heidsma, C.M.; Besselink, M.G.H.; Dreijerink, K.M.A.; Klümpen, H.-J.; Nieveen van Dijkum, E.J.M.; Engelsman, A.F. Treatment of Liver Metastases from Midgut Neuroendocrine Tumours: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 403. https://doi.org/10.3390/jcm8030403
Kaçmaz E, Heidsma CM, Besselink MGH, Dreijerink KMA, Klümpen H-J, Nieveen van Dijkum EJM, Engelsman AF. Treatment of Liver Metastases from Midgut Neuroendocrine Tumours: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(3):403. https://doi.org/10.3390/jcm8030403
Chicago/Turabian StyleKaçmaz, Enes, Charlotte M. Heidsma, Marc G. H. Besselink, Koen M. A. Dreijerink, Heinz-Josef Klümpen, Elisabeth J. M. Nieveen van Dijkum, and Anton F. Engelsman. 2019. "Treatment of Liver Metastases from Midgut Neuroendocrine Tumours: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 3: 403. https://doi.org/10.3390/jcm8030403
APA StyleKaçmaz, E., Heidsma, C. M., Besselink, M. G. H., Dreijerink, K. M. A., Klümpen, H. -J., Nieveen van Dijkum, E. J. M., & Engelsman, A. F. (2019). Treatment of Liver Metastases from Midgut Neuroendocrine Tumours: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 8(3), 403. https://doi.org/10.3390/jcm8030403