Relevance of Preoperative Hyperbilirubinemia in Patients Undergoing Hepatobiliary Resection for Hilar Cholangiocarcinoma

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Khan, S.A.; Davidson, B.R.; Goldin, R.D.; Heaton, N.; Karani, J.; Pereira, S.P.; Rosenberg, W.M.; Tait, P.; Taylor-Robinson, S.D.; Thillainayagam, A.V.; et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: An update. Gut 2012, 61, 1657–1669. [Google Scholar] [CrossRef]
- Esnaola, N.F.; Meyer, J.E.; Karachristos, A.; Maranki, J.L.; Camp, E.R.; Denlinger, C.S. Evaluation and management of intrahepatic and extrahepatic cholangiocarcinoma. Cancer 2016, 122, 1349–1369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, J.Q.; Cai, S.W.; Cong, W.M.; Chen, M.S.; Chen, P.; Chen, X.P.; Chen, Y.L.; Chen, Y.F.; Dai, C.L.; Huang, Q.; et al. Diagnosis and treatment of cholangiocarcinoma: A consensus from surgical specialists of China. J. Huazhong Univ. Sci. Technol. Med. Sci. 2014, 34, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Poruk, K.E.; Pawlik, T.M.; Weiss, M.J. Perioperative Management of Hilar Cholangiocarcinoma. J. Gastrointest. Surg. 2015, 19, 1889–1899. [Google Scholar] [CrossRef] [Green Version]
- Su, C.H.; Tsay, S.H.; Wu, C.C.; Shyr, Y.M.; King, K.L.; Lee, C.H.; Lui, W.Y.; Liu, T.J.; Peng, F.K. Factors influencing postoperative morbidity, mortality, and survival after resection for hilar cholangiocarcinoma. Ann. Surg. 1996, 223, 384–394. [Google Scholar] [CrossRef]
- Liu, F.; Li, Y.; Wei, Y.; Li, B. Preoperative biliary drainage before resection for hilar cholangiocarcinoma: Whether or not? A systematic review. Dig. Dis. Sci. 2011, 56, 663–672. [Google Scholar] [CrossRef]
- Iacono, C.; Ruzzenente, A.; Campagnaro, T.; Bortolasi, L.; Valdegamberi, A.; Guglielmi, A. Role of preoperative biliary drainage in jaundiced patients who are candidates for pancreatoduodenectomy or hepatic resection: Highlights and drawbacks. Ann. Surg. 2013, 257, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.J.; Nunes, Q.M.; Huang, W.; Pathak, S.; Wei, A.L.; Tan, C.L.; Liu, X.B. Preoperative biliary drainage in patients with hilar cholangiocarcinoma undergoing major hepatectomy. World J. Gastroenterol. 2013, 19, 8731–8739. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Tsuchikawa, T.; Okamura, K.; Nakamura, T.; Tamoto, E.; Noji, T.; Asano, T.; Amano, T.; Shichinohe, T.; Hirano, S. Risk factors for a high Comprehensive Complication Index score after major hepatectomy for biliary cancer: A study of 229 patients at a single institution. HPB (Oxford) 2016, 18, 735–741. [Google Scholar] [CrossRef]
- Nanashima, A.; Abo, T.; Hamasaki, K.; Wakata, K.; Kunizaki, M.; Tou, K.; Takeshita, H.; Hidaka, S.; Sawai, T.; Tsuchiya, T.; et al. Predictors of intraoperative blood loss in patients undergoing hepatectomy. Surg. Today 2013, 43, 485–493. [Google Scholar] [CrossRef]
- Farges, O.; Regimbeau, J.M.; Fuks, D.; Le Treut, Y.P.; Cherqui, D.; Bachellier, P.; Mabrut, J.Y.; Adham, M.; Pruvot, F.R.; Gigot, J.F. Multicentre European study of preoperative biliary drainage for hilar cholangiocarcinoma. Br. J. Surg. 2013, 100, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Mansour, J.C.; Aloia, T.A.; Crane, C.H.; Heimbach, J.K.; Nagino, M.; Vauthey, J.N. Hilar cholangiocarcinoma: Expert consensus statement. HPB (Oxford) 2015, 17, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Figueras, J.; Llado, L.; Valls, C.; Serrano, T.; Ramos, E.; Fabregat, J.; Rafecas, A.; Torras, J.; Jaurrieta, E. Changing strategies in diagnosis and management of hilar cholangiocarcinoma. Liver Transplant. 2000, 6, 786–794. [Google Scholar] [CrossRef]
- Kimura, N.; Young, A.L.; Toyoki, Y.; Wyatt, J.I.; Toogood, G.J.; Hidalgo, E.; Prasad, K.R.; Kudo, D.; Ishido, K.; Hakamada, K.; et al. Radical operation for hilar cholangiocarcinoma in comparable Eastern and Western centers: Outcome analysis and prognostic factors. Surgery 2017, 162, 500–514. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.A.; Barkun, J.; de Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; de Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo classification of surgical complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed]
- Jarnagin, W.R.; Gonen, M.; Fong, Y.; DeMatteo, R.P.; Ben-Porat, L.; Little, S.; Corvera, C.; Weber, S.; Blumgart, L.H. Improvement in perioperative outcome after hepatic resection: Analysis of 1803 consecutive cases over the past decade. Ann. Surg. 2002, 236, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Belghiti, J.; Hiramatsu, K.; Benoist, S.; Massault, P.; Sauvanet, A.; Farges, O. Seven hundred forty-seven hepatectomies in the 1990s: An update to evaluate the actual risk of liver resection. J. Am. Coll. Surg. 2000, 191, 38–46. [Google Scholar] [CrossRef]
- Miyagawa, S.; Makuuchi, M.; Kawasaki, S.; Kakazu, T. Criteria for safe hepatic resection. Am. J. Surg. 1995, 169, 589–594. [Google Scholar] [CrossRef]
- Ribero, D.; Zimmitti, G.; Aloia, T.A.; Shindoh, J.; Fabio, F.; Amisano, M.; Passot, G.; Ferrero, A.; Vauthey, J.N. Preoperative Cholangitis and Future Liver Remnant Volume Determine the Risk of Liver Failure in Patients Undergoing Resection for Hilar Cholangiocarcinoma. J. Am. Coll. Surg. 2016, 223, 87–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemming, A.W.; Reed, A.I.; Fujita, S.; Foley, D.P.; Howard, R.J. Surgical Management of Hilar Cholangiocarcinoma. Ann. Surg. 2005, 241, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Ferrero, A.; Lo Tesoriere, R.; Vigano, L.; Caggiano, L.; Sgotto, E.; Capussotti, L. Preoperative biliary drainage increases infectious complications after hepatectomy for proximal bile duct tumor obstruction. World J. Surg. 2009, 33, 318–325. [Google Scholar] [CrossRef]
- Cai, Y.; Tang, Q.; Xiong, X.; Li, F.; Ye, H.; Song, P.; Cheng, N. Preoperative biliary drainage versus direct surgery for perihilar cholangiocarcinoma: A retrospective study at a single center. Biosci. Trends 2017, 11, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Cannon, R.M.; Brock, G.; Buell, J.F. Surgical resection for hilar cholangiocarcinoma: Experience improves resectability. HPB (Oxford) 2012, 14, 142–149. [Google Scholar] [CrossRef] [PubMed]
- Sano, T.; Shimada, K.; Sakamoto, Y.; Yamamoto, J.; Yamasaki, S.; Kosuge, T. One hundred two consecutive hepatobiliary resections for perihilar cholangiocarcinoma with zero mortality. Ann. Surg. 2006, 244, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Yu, W.F. Obstructive jaundice and perioperative management. Acta Anaesthesiol. Taiwan 2014, 52, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Baron, D.M.; Hochrieser, H.; Posch, M.; Metnitz, B.; Rhodes, A.; Moreno, R.P.; Pearse, R.M.; Metnitz, P.; European Surgical Outcomes Study (EuSOS) group for Trials Groups of European Society of Intensive Care Medicine; European Society of Anaesthesiology. Preoperative anaemia is associated with poor clinical outcome in non-cardiac surgery patients. Br. J. Anaesth. 2014, 113, 416–423. [Google Scholar] [CrossRef] [Green Version]
- Tee, M.C.; Shubert, C.R.; Ubl, D.S.; Habermann, E.B.; Nagorney, D.M.; Que, F.G. Preoperative anemia is associated with increased use of hospital resources in patients undergoing elective hepatectomy. Surgery 2015, 158, 1027–1038. [Google Scholar] [CrossRef]
- Tohme, S.; Varley, P.R.; Landsittel, D.P.; Chidi, A.P.; Tsung, A. Preoperative anemia and postoperative outcomes after hepatectomy. HPB (Oxford) 2016, 18, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, T.J.; Yopp, A.; Qin, Y.; Zhao, B.; Guo, P.; Liu, F.; Schwartz, L.H.; Allen, P.; DAngelica, M.; Fong, Y.; et al. Role of preoperative biliary drainage of liver remnant prior to extended liver resection for hilar cholangiocarcinoma. HPB (Oxford) 2009, 11, 445–451. [Google Scholar] [CrossRef] [Green Version]
- Squires, M.H., 3rd; Lad, N.L.; Fisher, S.B.; Kooby, D.A.; Weber, S.M.; Brinkman, A.; Scoggins, C.R.; Egger, M.E.; Cardona, K.; Cho, C.S.; et al. The effect of preoperative renal insufficiency on postoperative outcomes after major hepatectomy: A multi-institutional analysis of 1170 patients. J. Am. Coll. Surg. 2014, 219, 914–922. [Google Scholar] [CrossRef]
- Buettner, S.; Margonis, G.A.; Kim, Y.; Gani, F.; Ethun, C.G.; Poultsides, G.; Tran, T.; Idrees, K.; Isom, C.A.; Fields, R.C.; et al. Conditional probability of long-term survival after resection of hilar cholangiocarcinoma. HPB (Oxford) 2016, 18, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.J.; Mao, H.; Shrestha, A.; Tan, Y.Q.; Ma, W.J.; Yang, Q.; Wang, J.K.; Cheng, N.S.; Li, F.Y. Prognostic factors and long-term outcomes of hilar cholangiocarcinoma: A single-institution experience in China. World J. Gastroenterol. 2016, 22, 2601–2610. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | Number with Percentage and Median with Interquartile Range (IQR) | |||
|---|---|---|---|---|
| Studied Group (n = 81) | Patients with Preoperative Biliary Drainage (n = 58) | Patients without Preoperative Biliary Drainage (n = 23) | p | |
| Age | 60 (54–65) | 60.0 (55.0–67.0) | 56.0 (48.0–65.0) | 0.181 |
| Patient sex | ||||
| Female | 34 (42.0%) | 24 (41.4%) | 10 (43.5%) | 0.999 |
| Male | 47 (58.0%) | 34 (58.6%) | 13 (56.5%) | |
| Bilirubin concentration (mg/dL) | 2.44 (1.00–9.78) | 2.14 (0.93–4.90) | 9.64 (1.10–19.67) | 0.028 |
| AST activity (U/L) | 66 (46–106) | 72 (48–106) | 59.5 (46–95) | 0.406 |
| ALT activity (U/L) | 81 (51–106) | 85 (51–110) | 68.5 (58–85) | 0.208 |
| GGTP activity (U/L) | 352 (156–592) | 441 (210–643) | 176 (105–298) | 0.006 |
| Creatinine concentration (mg/dL) | 0.77 (0.70–0.91) | 0.77 (0.69–0.88) | 0.78 (0.72–1.07) | 0.535 |
| INR | 1.00 (0.95–1.08) | 0.99 (0.96–1.07) | 1.03 (0.93–1.11) | 0.562 |
| Protein concentration (g/dL) | 6.80 (6.35–7.35) | 6.90 (6.40–7.50) | 6.80 (6.30–7.00) | 0.358 |
| Albumin concentration (g/dL) | 3.60 (3.20–3.90) | 3.50 (3.05–3.90) | 3.70 (3.50–3.80) | 0.263 |
| Urea concentration (mg/dL) | 28.0 (22.0–36.0) | 27.5 (21.0–36.5) | 28.0 (22.0–32.0) | 0.916 |
| Hemoglobin concentration (g/dL) | 12.45 (11.5–13.28) | 12.3 (11.3–13.3) | 12.7 (12.3–13.1) | 0.124 |
| White Blood Cells (103/µL) | 7.04 (5.90–8.59) | 7.04 (6.30–8.41) | 6.80 (5.55–9.00) | 0.579 |
| Platelets (103/µL ) | 263.5 (213.0–326.0) | 253.5 (206–349) | 274 (227–308) | 0.953 |
| Ca19–9 (U/mL) | 155.1 (43.1–421.6) | 167.9 (53.4–562.0) | 113.6 (26.9–222.0) | 0.245 |
| CEA (ng/mL) | 1.95 (1.22–2.80) | 2.0 (1.2–3.0) | 1.8 (1.3–2.4) | 0.678 |
| TNM tumor staging III or higher | 18 (22.2%) | 14 (28.6%) | 4 (21.1%) | 0.760 |
| Liver resection type | ||||
| Right or extended right | 36 (44.4%) | 32 (55.2%) | 4 (17.4%) | 0.003 |
| Left | 45 (55.6%) | 26 (44.8%) | 19 (82.6%) | |
| Packed red blood cells transfusion | 0 (0–2) | 0 (0–2) | 2 (0–2) | 0.384 |
| Fresh frozen plasma transfusion | 0 (0–2) | 0 (0–2) | 2 (0–3) | 0.106 |
| Operative time (hours) | 7.0 (5.8–7.9) | 6.5 (5.3–7.8) | 7.5 (7.0–8.3) | 0.025 |
| Positive bile culture | 46 (56.8%) | 43 (74.1%) | 3 (13.0%) | <0.001 |
| Postoperative Complications | Way of Treatment | Number of Patients with This Complication |
|---|---|---|
| Biliary leak | Endoscopic retrograde cholangiopancreatography | 1 |
| Reoperation | 1 | |
| Percutaneous drainage | 1 | |
| Bleeding | Reoperation | 5 |
| Rectus abdominal muscle bleeding | Wound revision | 1 |
| Wound infection, difficulty with drain removal | Minilaparotomy, wound revision | 1 |
| Abdominal abscess | Percutaneous drainage | 1 |
| Reoperation | 2 | |
| Intraabdominal infection | Reoperation | 1 |
| Wound dehiscence | Wound revision | 3 |
| Gastrointestinal tract bleeding | Gastroscopy | 3 |
| Pleural effusion | Pleurocentesis | 3 |
| Renal failure | Dialysis | 3 |
| Liver failure | Albumin dialysis | 2 |
| Without albumin dialysis | 6 | |
| Respiratory failure | Artificial ventilation | 2 |
| Heart failure | Pharmacological treatment | 2 |
| Multiple organ dysfunction syndrome as a result of choking | Pharmacological treatment, artificial ventilation | 1 |
| Death | 9 |
| Factors | Outcome Measure | |||||
|---|---|---|---|---|---|---|
| Postoperative Mortality | Postoperative Severe Complications | |||||
| OR | 95% CI | p | OR | 95% CI | p | |
| Age | 1.04 | 0.95–1.13 | 0.404 | 1.06 | 1.00–1.13 | 0.063 |
| Patient sex (Male) | 1.51 | 0.35–6.53 | 0.579 | 2.64 | 0.91–7.66 | 0.073 |
| Preoperative biliary drainage | 3.52 | 0.42–29.87 | 0.249 | 1.18 | 0.40–3.49 | 0.772 |
| Bilirubin concentration (mg/dL) | 1.14 | 1.05–1.24 | 0.003 | 1.08 | 1.01–1.15 | 0.018 |
| AST activity (U/L) | 1.97 | 0.63–6.19 | 0.245 | 0.96 | 0.35–2.62 | 0.941 |
| ALT activity (U/L) | 0.86 | 0.21–3.54 | 0.837 | 0.75 | 0.27–2.08 | 0.580 |
| GGTP activity (U/L) | 1.12 | 1.00–1.26 | 0.051 | 1.07 | 0.97–1.18 | 0.203 |
| Creatinine concentration (mg/dL) | 17.96 | 0.70–461.37 | 0.081 | 57.56 | 4.06–815.9 | 0.003 |
| INR | 9.33 | 0.08–1106.33 | 0.359 | 35.45 | 0.69–1827.7 | 0.076 |
| Protein concentration (g/dL) | 1.07 | 0.42–2.76 | 0.887 | 1.39 | 0.74–2.62 | 0.310 |
| Albumin concentration (g/dL) | 0.11 | 0.03–0.47 | 0.003 | 0.49 | 0.20–1.24 | 0.133 |
| Urea concentration (mg/dL) | 1.04 | 0.99–1.09 | 0.103 | 1.05 | 1.01–1,10 | 0.028 |
| Hemoglobin concentration (g/dL) | 0.27 | 0.13–0.56 | <0.001 | 0.65 | 0.45–0.93 | 0.019 |
| White Blood Cells (103/µL) | 1.02 | 0.72–1.43 | 0.922 | 1.04 | 0.82–1.32 | 0.770 |
| Platelets (103/µL ) | 0.91 | 0.45–1.85 | 0.790 | 0.84 | 0.51–1.39 | 0.501 |
| TNM tumor staging III or higher | 0.43 | 0.05–3.85 | 0.452 | 1.29 | 0.40–4.09 | 0.671 |
| Right or extended right hemihepatectomy | 12.6 | 1.49–106.02 | 0.020 | 1.98 | 0.74–5.26 | 0.172 |
| Packed red blood cells transfusion | 1.68 | 1.11–2.53 | 0.013 | 1.11 | 0.84–1.48 | 0.467 |
| Fresh frozen plasma transfusion | 1.34 | 0.99–1.82 | 0.057 | 1.08 | 0.84–1.38 | 0.549 |
| Operative time (hours) | 0.97 | 0.61–1.53 | 0.892 | 1.04 | 0.76–1.41 | 0.822 |
| Positive bile culture | 0.95 | 0.23–3.81 | 0.937 | 1.26 | 0.47–3.38 | 0.641 |
| Postoperative Mortality | |||
| Group of Patients | OR | 95% CI | p |
| Patients with preoperative albumin concentration ≤3.6 g/dL | 1.14 | 1.02–1.26 | 0.019 |
| Patients with preoperative hemoglobin concentration ≤12.45 g/dL | 1.13 | 1.03–1.25 | 0.014 |
| Patients with preoperative biliary drainage | 1.22 | 1.08-138 | 0.002 |
| Patients after right or extended right hemihepatectomy | 1.23 | 1.07–1.42 | 0.004 |
| Postoperative Severe Complications | |||
| Group of Patients | OR | 95% CI | p |
| Patients with preoperative creatinine concentration ≥0.77 mg/dL | 1.10 | 1.01–1.19 | 0.032 |
| Patients with preoperative urea concentration ≥28 mg/dL | 1.13 | 1.02–1.24 | 0.026 |
| Patients with preoperative biliary drainage | 1.10 | 1.00–1.21 | 0.042 |
| Patients after right or extended right hemihepatectomy | 1.15 | 1.02–1.29 | 0.020 |
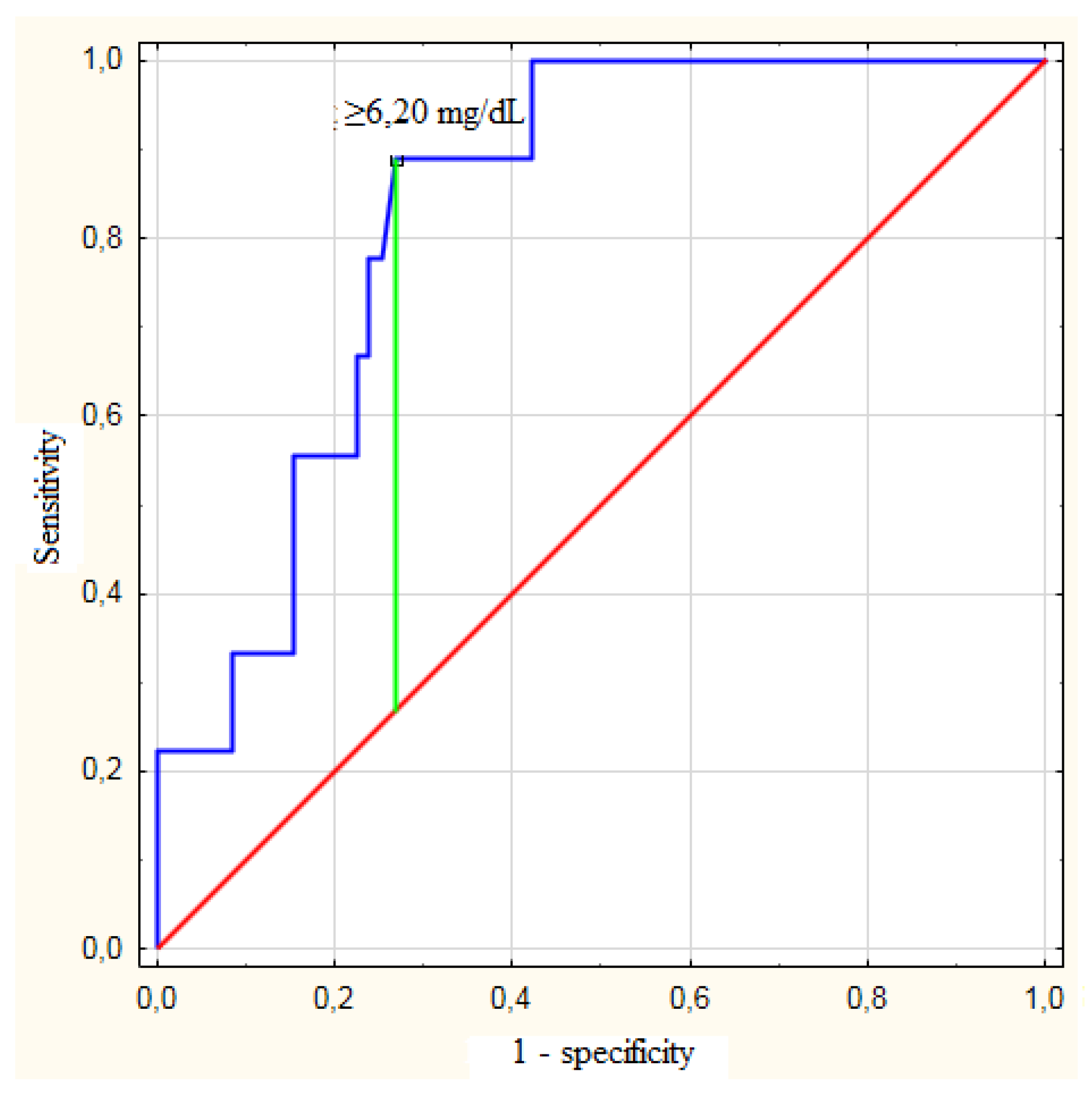
| Postoperative Mortality | ||||||
| Patients | Optimal Cut-Off | C-Statistic (95% CI) | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
| All patients | ≥6.20 mg/dL | 0.829 (0.723–0.934) | 88.9% | 73.2% | 29.6% | 98.1% |
| Patients with preoperative albumin concentration ≤3.6 g/dL | ≥6.20 mg/dL | 0.788 (0.624–0.952) | 87.5% | 64.3% | 41.2% | 94.7% |
| Patients with preoperative hemoglobin concentration ≤12.45 g/dL | ≥6.20 mg/dL | 0.797 (0.650–0.945) | 88.9% | 71.0% | 47.1% | 95.7% |
| Patients with preoperative biliary drainage | ≥6.20 mg/dL | 0.891 (0.800–0.982) | 87.5% | 86.0% | 50.0% | 97.7% |
| Patients after right or extended right hemihepatectomy | ≥2.73 mg/dL | 0.933 (0.853–1.000) | 100.0% | 78.6% | 57.1% | 100.0% |
| Postoperative Severe Complications | ||||||
| Patients | Optimal Cut-Off | C-Statistic (95% CI) | Sensitivity | Specificity | Positive Predictive Value | Negative Predictive Value |
| All patients | ≥2.48 mg/dL | 0.662 (0.526–0.799) | 73.9% | 59.6% | 42.5% | 85.0% |
| Patients with preoperative creatinine concentration ≥0.77 mg/dL | ≥6.20 mg/dL | 0.724 (0.559–0.888) | 64.7% | 84.0% | 73.3% | 72.8% |
| Patients with preoperative urea concentration ≥28 mg/dL | ≥6.20 mg/dL | 0.741 (0.576–0.906) | 57.1% | 85.2% | 66.7% | 79.3% |
| Patients with preoperative biliary drainage | ≥2.48 mg/dL | 0.685 (0.530–0.840) | 70.6% | 68.3% | 48.0% | 84.8% |
| Patients after right or extended right hemihepatectomy | ≥2.48 mg/dL | 0.764 (0.585–0.944) | 76.9% | 78.3% | 66.7% | 85.7% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wronka, K.M.; Grąt, M.; Stypułkowski, J.; Bik, E.; Patkowski, W.; Krawczyk, M.; Zieniewicz, K. Relevance of Preoperative Hyperbilirubinemia in Patients Undergoing Hepatobiliary Resection for Hilar Cholangiocarcinoma. J. Clin. Med. 2019, 8, 458. https://doi.org/10.3390/jcm8040458
Wronka KM, Grąt M, Stypułkowski J, Bik E, Patkowski W, Krawczyk M, Zieniewicz K. Relevance of Preoperative Hyperbilirubinemia in Patients Undergoing Hepatobiliary Resection for Hilar Cholangiocarcinoma. Journal of Clinical Medicine. 2019; 8(4):458. https://doi.org/10.3390/jcm8040458
Chicago/Turabian StyleWronka, Karolina Maria, Michał Grąt, Jan Stypułkowski, Emil Bik, Waldemar Patkowski, Marek Krawczyk, and Krzysztof Zieniewicz. 2019. "Relevance of Preoperative Hyperbilirubinemia in Patients Undergoing Hepatobiliary Resection for Hilar Cholangiocarcinoma" Journal of Clinical Medicine 8, no. 4: 458. https://doi.org/10.3390/jcm8040458
APA StyleWronka, K. M., Grąt, M., Stypułkowski, J., Bik, E., Patkowski, W., Krawczyk, M., & Zieniewicz, K. (2019). Relevance of Preoperative Hyperbilirubinemia in Patients Undergoing Hepatobiliary Resection for Hilar Cholangiocarcinoma. Journal of Clinical Medicine, 8(4), 458. https://doi.org/10.3390/jcm8040458