Prognostic Impact of Low Skeletal Muscle Mass on Major Adverse Cardiovascular Events in Coronary Artery Disease: A Propensity Score-Matched Analysis of a Single Center All-Comer Cohort

 , , and
, , and
Abstract
:
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Patient Management, Data Collection, and Clinical Follow-up
2.3. Study Outcomes and Definition
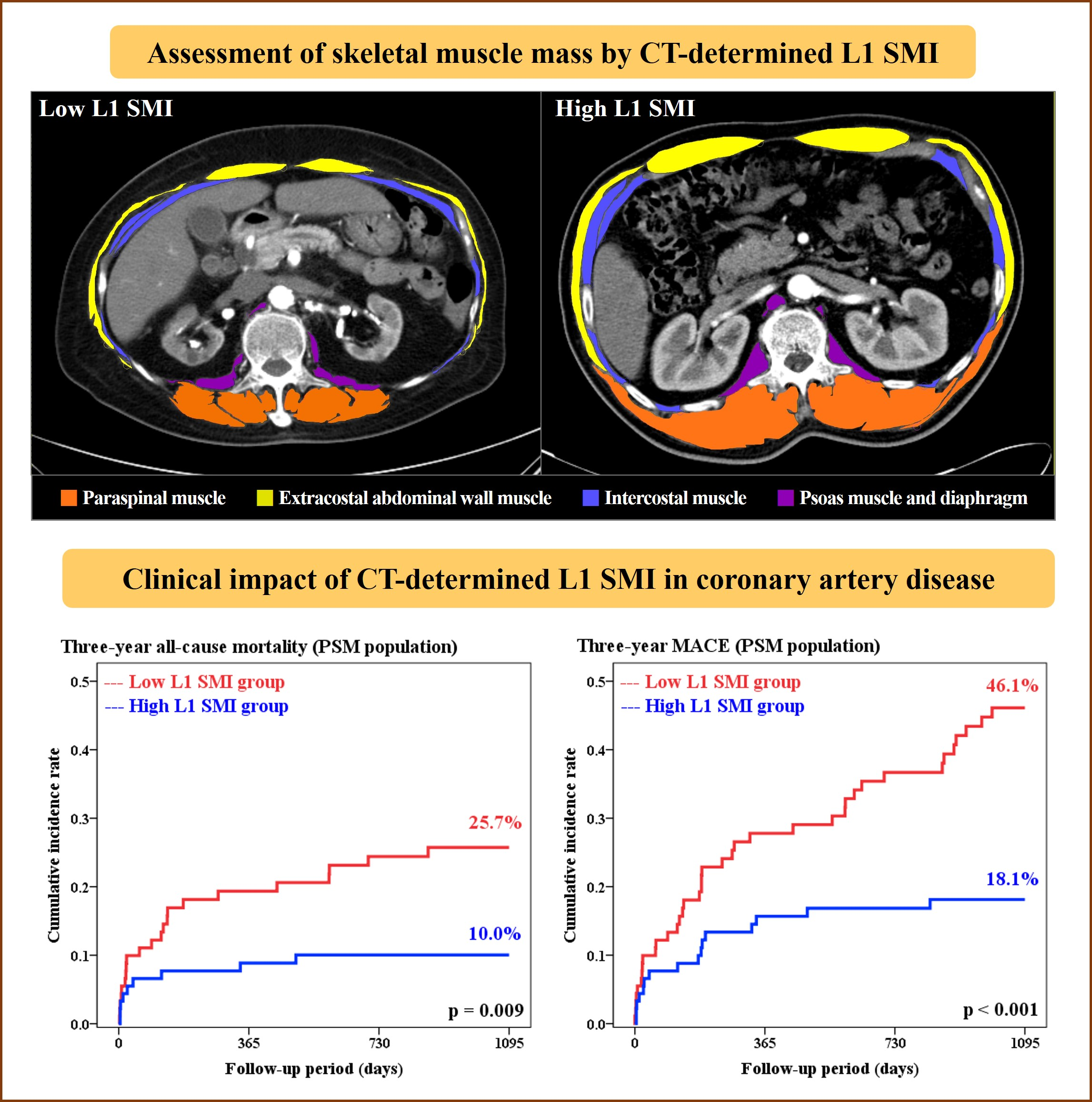
2.4. Definition of Low SMM and Method of SMM Assessment
2.5. Statistical Analysis
3. Results
3.1. CT Measurement of L1 SMI and Reference Values for Defining Low SMM
3.2. Baseline Characteristics and Procedural Profiles
3.3. Clinical Outcomes According to the Presence of Low L1 SMI
3.4. Multivariate Analysis for the Prognostic Impact of Low L1 SMI
3.5. Propensity Score-Matched Analysis
3.6. Clinical Outcomes Based on the Presence of Frailty
3.7. Detailed Characteristics of Patients Excluded at Initial Enrollment
4. Discussion
4.1. Novelty of the Present Study
4.2. Assessment of SMM by L1 SMI as a Promising Marker of Prognosis and Comorbidity
4.3. Mechanisms Linking Sarcopenia to Its Prognostic Value
4.4. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Morley, J.E.; Baumgartner, R.N.; Roubenoff, R.; Mayer, J.; Nair, K.S. Sarcopenia. J. Lab. Clin. Med. 2001, 137, 231–243. [Google Scholar] [CrossRef]
- Janssen, I.; Heymsfield, S.B.; Ross, R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J. Am. Geriatr. Soc. 2002, 50, 889–896. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2018. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Atkins, J.L.; Whincup, P.H.; Morris, R.W.; Lennon, L.T.; Papacosta, O.; Wannamethee, S.G. Sarcopenic obesity and risk of cardiovascular disease and mortality: A population-based cohort study of older men. J. Am. Geriatr. Soc. 2014, 62, 253–260. [Google Scholar] [CrossRef]
- Roubenoff, R.; Parise, H.; Payette, H.A.; Abad, L.W.; D’Agostino, R.; Jacques, P.F.; Wilson, P.W.; Dinarello, C.A.; Harris, T.B. Cytokines, insulin-like growth factor 1, sarcopenia, and mortality in very old community-dwelling men and women: The Framingham Heart Study. Am. J. Med. 2003, 115, 429–435. [Google Scholar] [CrossRef]
- Ko, B.J.; Chang, Y.; Jung, H.S.; Yun, K.E.; Kim, C.W.; Park, H.S.; Chung, E.C.; Shin, H.; Ryu, S. Relationship Between Low Relative Muscle Mass and Coronary Artery Calcification in Healthy Adults. Arterioscler. Thrombosis Vasc. Boil. 2016, 36, 1016–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, S.O.; Rhee, S.Y.; Chon, S.; Hwang, Y.C.; Jeong, I.K.; Oh, S.; Ahn, K.J.; Chung, H.Y.; Woo, J.T.; Kim, S.W.; et al. Sarcopenia is independently associated with cardiovascular disease in older Korean adults: The Korea National Health and Nutrition Examination Survey (KNHANES) from 2009. PLoS ONE 2013, 8, e60119. [Google Scholar] [CrossRef] [PubMed]
- Nichols, S.; O’Doherty, A.F.; Taylor, C.; Clark, A.L.; Carroll, S.; Ingle, L. Low skeletal muscle mass is associated with low aerobic capacity and increased mortality risk in patients with coronary heart disease—A CARE CR study. Clin. Physiol. Funct. Imaging 2018. [Google Scholar] [CrossRef] [PubMed]
- Mok, M.; Allende, R.; Leipsic, J.; Altisent, O.A.; Del Trigo, M.; Campelo-Parada, F.; DeLarochelliere, R.; Dumont, E.; Doyle, D.; Cote, M.; et al. Prognostic Value of Fat Mass and Skeletal Muscle Mass Determined by Computed Tomography in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 117, 828–833. [Google Scholar] [CrossRef]
- Garg, L.; Agrawal, S.; Pew, T.; Hanzel, G.S.; Abbas, A.E.; Gallagher, M.J.; Shannon, F.L.; Hanson, I.D. Psoas Muscle Area as a Predictor of Outcomes in Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2017, 119, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Drudi, L.M.; Phung, K.; Ades, M.; Zuckerman, J.; Mullie, L.; Steinmetz, O.K.; Obrand, D.I.; Afilalo, J. Psoas Muscle Area Predicts All-Cause Mortality After Endovascular and Open Aortic Aneurysm Repair. Eur. J. Vasc. Endovasc. Surg. 2016, 52, 764–769. [Google Scholar] [CrossRef]
- Hale, A.L.; Twomey, K.; Ewing, J.A.; Langan, E.M., 3rd; Cull, D.L.; Gray, B.H. Impact of sarcopenia on long-term mortality following endovascular aneurysm repair. Vasc. Med. 2016, 21, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, D.H.; Kim, C.; Lee, N.; Wolfe, L.; Pfeifer, J.; Amendola, M. Sarcopenia predicts poor long-term survival in patients undergoing endovascular aortic aneurysm repair. J. Vasc. Surg. 2018, 67, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Juszczak, M.T.; Taib, B.; Rai, J.; Iazzolino, L.; Carroll, N.; Antoniou, G.A.; Neequaye, S.; Torella, F. Total psoas area predicts medium-term mortality after lower limb revascularization. J. Vasc. Surg. 2018, 68, 1114–1125.e1. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, Y.; Matsumoto, T.; Inoue, K.; Matsuda, D.; Yoshiga, R.; Yoshiya, K.; Furuyama, T.; Maehara, Y. Sarcopenia is a risk factor for cardiovascular events experienced by patients with critical limb ischemia. J. Vasc. Surg. 2017, 65, 1390–1397. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.J.; Faxon, D.P.; Gunnar, R.M.; Kennedy, J.W.; King, S.B., 3rd; Loop, F.D.; Peterson, K.L.; Reeves, T.J.; Williams, D.O.; Winters, W.L., Jr.; et al. Guidelines for percutaneous transluminal coronary angioplasty. A report of the American College of Cardiology/American Heart Association Task Force on Assessment of Diagnostic and Therapeutic Cardiovascular Procedures (Subcommittee on Percutaneous Transluminal Coronary Angioplasty). Circulation 1988, 78, 486–502. [Google Scholar] [PubMed]
- Rockwood, K.; Song, X.; MacKnight, C.; Bergman, H.; Hogan, D.B.; McDowell, I.; Mitnitski, A. A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cutlip, D.E.; Windecker, S.; Mehran, R.; Boam, A.; Cohen, D.J.; van Es, G.A.; Steg, P.G.; Morel, M.A.; Mauri, L.; Vranckx, P.; et al. Clinical end points in coronary stent trials: A case for standardized definitions. Circulation 2007, 115, 2344–2351. [Google Scholar] [CrossRef]
- Mitsiopoulos, N.; Baumgartner, R.N.; Heymsfield, S.B.; Lyons, W.; Gallagher, D.; Ross, R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. 1998, 85, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef]
- Derstine, B.A.; Holcombe, S.A.; Ross, B.E.; Wang, N.C.; Su, G.L.; Wang, S.C. Skeletal muscle cutoff values for sarcopenia diagnosis using T10 to L5 measurements in a healthy US population. Sci. Rep. 2018, 8, 11369. [Google Scholar] [CrossRef]
- Rush, E.C.; Goedecke, J.H.; Jennings, C.; Micklesfield, L.; Dugas, L.; Lambert, E.V.; Plank, L.D. BMI, fat and muscle differences in urban women of five ethnicities from two countries. Int. J. Obes. 2007, 31, 1232–1239. [Google Scholar] [CrossRef]
- Recio-Boiles, A.; Galeas, J.N.; Goldwasser, B.; Sanchez, K.; Man, L.M.W.; Gentzler, R.D.; Gildersleeve, J.; Hollen, P.J.; Gralla, R.J. Enhancing evaluation of sarcopenia in patients with non-small cell lung cancer (NSCLC) by assessing skeletal muscle index (SMI) at the first lumbar (L1) level on routine chest computed tomography (CT). Support. Care Cancer 2018, 26, 2353–2359. [Google Scholar] [CrossRef]
- Campos, A.M.; Moura, F.A.; Santos, S.N.; Freitas, W.M.; Sposito, A.C. Sarcopenia, but not excess weight or increased caloric intake, is associated with coronary subclinical atherosclerosis in the very elderly. Atherosclerosis 2017, 258, 138–144. [Google Scholar] [CrossRef]
- Tibuakuu, M.; Zhao, D.; Saxena, A.; Brown, T.T.; Jacobson, L.P.; Palella, F.J., Jr.; Witt, M.D.; Koletar, S.L.; Margolick, J.B.; Guallar, E.; et al. Low thigh muscle mass is associated with coronary artery stenosis among HIV-infected and HIV-uninfected men: The Multicenter AIDS Cohort Study (MACS). J. Cardiovasc. Comput. Tomogr. 2018, 12, 131–138. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Corriere, M.; Ferrucci, L. Age-related and disease-related muscle loss: The effect of diabetes, obesity, and other diseases. Lancet Diabetes Endocrinol. 2014, 2, 819–829. [Google Scholar] [CrossRef]
- Bone, A.E.; Hepgul, N.; Kon, S.; Maddocks, M. Sarcopenia and frailty in chronic respiratory disease. Chronic Respir. Dis. 2017, 14, 85–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.N.; Choi, K.M. The implications of sarcopenia and sarcopenic obesity on cardiometabolic disease. J. Cell. Biochem. 2015, 116, 1171–1178. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Rihal, C.S.; Lennon, R.J.; Spertus, J.A.; Nair, K.S.; Roger, V.L. Influence of frailty and health status on outcomes in patients with coronary disease undergoing percutaneous revascularization. Circ. Cardiovasc. Qual. Outcomes 2011, 4, 496–502. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Cesari, M.; Landi, F.; Vellas, B.; Bernabei, R.; Marzetti, E. Sarcopenia and Physical Frailty: Two Sides of the Same Coin. Front. Aging Neurosci. 2014, 6. [Google Scholar] [CrossRef] [Green Version]
- Bernabeu-Wittel, M.; Gonzalez-Molina, A.; Fernandez-Ojeda, R.; Diez-Manglano, J.; Salgado, F.; Soto-Martin, M.; Muniesa, M.; Ollero-Baturone, M.; Gomez-Salgado, J. Impact of Sarcopenia and Frailty in a Multicenter Cohort of Polypathological Patients. J. Clin. Med. 2019, 8, 535. [Google Scholar] [CrossRef]
- Sayer, A.A.; Robinson, S.M.; Patel, H.P.; Shavlakadze, T.; Cooper, C.; Grounds, M.D. New horizons in the pathogenesis, diagnosis and management of sarcopenia. Age Ageing 2013, 42, 145–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, S.C., Jr.; Benjamin, E.J.; Bonow, R.O.; Braun, L.T.; Creager, M.A.; Franklin, B.A.; Gibbons, R.J.; Grundy, S.M.; Hiratzka, L.F.; Jones, D.W.; et al. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients with Coronary and other Atherosclerotic Vascular Disease: 2011 update: A guideline from the American Heart Association and American College of Cardiology Foundation. Circulation 2011, 124, 2458–2473. [Google Scholar] [CrossRef]
- Anderson, L.; Oldridge, N.; Thompson, D.R.; Zwisler, A.D.; Rees, K.; Martin, N.; Taylor, R.S. Exercise-Based Cardiac Rehabilitation for Coronary Heart Disease: Cochrane Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2016, 67, 1–12. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.T.; Corra, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Overall Population | PSM Population | |||||||
|---|---|---|---|---|---|---|---|---|
| Low L1 SMI (n = 141) | High L1 SMI (n = 334) | p-Value | S.diff | Low L1 SMI (n = 91) | High L1 SMI (n = 91) | p-Value | S.diff | |
| Age (years) | 70.4 ± 11.0 | 64.0 ± 9.2 | <0.001 | −0.65 | 68.7 ± 11.5 | 67.1 ± 8.7 | 0.26 | −0.17 |
| Sex (men) | 100 (70.9) | 230 (68.8) | 0.66 | −0.05 | 66 (72.5) | 65 (71.4) | 0.87 | −0.03 |
| BMI (kg/m2) | 21.6 ± 2.6 | 24.9 ± 2.9 | <0.001 | 1.16 | 22.8 ± 2.3 | 23.0 ± 2.6 | 0.47 | 0.11 |
| Clinical presentation | ||||||||
| Myocardial infarction | 46 (32.6) | 97 (29.0) | 0.44 | −0.09 | 29 (31.8) | 28 (30.7) | 0.87 | −0.03 |
| Unstable angina | 36 (25.5) | 110 (32.9) | 0.11 | 0.20 | 24 (26.3) | 29 (31.8) | 0.42 | 0.15 |
| Stable angina | 48 (34.0) | 115 (34.4) | 0.94 | 0.01 | 30 (32.9) | 29 (31.8) | 0.87 | −0.03 |
| Past medical history | ||||||||
| Previous CAD | 4 (2.8) | 6 (1.7) | 0.49 | −0.26 | 2 (2.1) | 0 (0.0) | 0.50 | 0.10 |
| Hypertension | 85 (60.2) | 223 (66.7) | 0.18 | 0.16 | 59 (64.8) | 53 (58.2) | 0.36 | −0.15 |
| Diabetes | 68 (48.2) | 145 (43.4) | 0.34 | −0.11 | 43 (47.2) | 46 (50.5) | 0.66 | 0.07 |
| Dyslipidemia | 18 (12.7) | 65 (19.4) | 0.08 | 0.28 | 14 (15.3) | 15 (16.4) | 0.84 | 0.05 |
| Cerebrovascular accident | 12 (8.5) | 28 (8.3) | 0.96 | −0.01 | 9 (9.8) | 5 (5.4) | 0.41 | −0.35 |
| Peripheral artery disease | 29 (20.5) | 51 (15.2) | 0.16 | −0.20 | 20 (21.9) | 16 (17.5) | 0.46 | −0.15 |
| Previous malignancy | 13 (9.2) | 19 (5.6) | 0.16 | −0.29 | 6 (6.5) | 6 (6.5) | >0.99 | <0.001 |
| Current smoker | 48 (34.0) | 115 (34.4) | 0.94 | 0.01 | 34 (37.3) | 36 (39.5) | 0.76 | 0.05 |
| Frailty (CFS ≥5) | 47 (33.3) | 74 (22.1) | 0.011 | −0.31 | 30 (32.9) | 23 (25.2) | 0.25 | −0.21 |
| Mild to moderate (CFS 5–6) | 35 (24.8) | 70 (20.9) | 21 (23.0) | 22 (24.1) | ||||
| Severe (CFS 7) | 12 (8.5) | 4 (1.1) | 9 (9.8) | 1 (1.0) | ||||
| Laboratory data | ||||||||
| Total cholesterol (mmol/L) | 3.88 (3.18–4.64) | 4.20 (3.49–5.12) | 0.004 | 0.13 | 3.88 (3.41–4.63) | 4.03 (3.23–4.71) | 0.90 | 0.01 |
| LDLc (mmol/L) | 2.34 (1.77–3.10) | 2.64 (1.99–3.36) | 0.034 | 0.10 | 2.35 (1.89–3.09) | 2.37 (1.77–3.00) | 0.78 | 0.02 |
| hs-CRP (mg/L) | 7.0 (1.0–17.0) | 2.0 (1.0–8.5) | 0.006 | −0.13 | 6.0 (1.0–15.5) | 4.0 (1.0–17.5) | 0.80 | −0.02 |
| HbA1c (%) | 6.41 ± 1.47 | 6.56 ± 1.77 | 0.40 | 0.09 | 6.31 ± 1.60 | 6.61 ± 1.79 | 0.24 | 0.18 |
| CrCl (mL/min) | 60.4 ± 29.4 | 79.4 ± 30.6 | <0.001 | 0.63 | 66.1 ± 30.9 | 71.3 ± 27.1 | 0.23 | 0.18 |
| LVEF (%) | 50.6 ± 11.4 | 54.2 ± 9.6 | 0.001 | 0.35 | 51.2 ± 11.3 | 51.6 ± 12.9 | 0.85 | 0.03 |
| CT scan profiles | ||||||||
| Average days from PCI to CT scan | −2.5 ± 11.6 | −3.7 ± 11.8 | 0.30 | −0.10 | −4.0 ± 10.8 | −4.0 ± 10.5 | 0.96 | −0.01 |
| L1 SMA (cm2) | 66.92 ± 15.86 | 96.49 ± 21.84 | <0.001 | 1.46 | 70.18 ± 16.06 | 90.30 ± 17.17 | <0.001 | 1.21 |
| Male | 74.07 ± 12.61 | 107.37 ± 16.22 | <0.001 | 2.18 | 77.60 ± 11.65 | 98.43 ± 11.58 | <0.001 | 1.79 |
| Female | 49.49 ± 6.90 | 72.45 ± 10.45 | <0.001 | 2.45 | 50.60 ± 7.00 | 69.98 ± 10.82 | <0.001 | 2.13 |
| L1 SMI (cm2/m2) | 25.14 ± 4.066 | 36.18 ± 5.864 | <0.001 | 2.05 | 26.03 ± 4.03 | 33.95 ± 4.52 | <0.001 | 1.85 |
| Male | 26.52 ± 3.74 | 38.36 ± 5.24 | <0.001 | 2.39 | 27.49 ± 3.45 | 35.54 ± 3.77 | <0.001 | 2.23 |
| Female | 21.77 ± 2.64 | 31.36 ± 4.02 | <0.001 | 2.60 | 22.19 ± 2.74 | 29.99 ± 3.81 | <0.001 | 2.35 |
| Post-PCI medications | ||||||||
| Aspirin | 127 (90.0) | 309 (92.5) | 0.38 | 0.17 | 82 (90.1) | 81 (89.0) | 0.81 | 0.05 |
| Clopidogrel | 116 (82.2) | 301 (90.1) | 0.017 | 0.37 | 77 (84.6) | 76 (83.5) | 0.84 | −0.05 |
| Beta-blocker | 70 (49.6) | 159 (47.6) | 0.68 | −0.05 | 45 (49.4) | 44 (48.3) | 0.89 | 0.05 |
| Calcium channel blocker | 49 (34.7) | 101 (30.2) | 0.33 | −0.11 | 31 (34.0) | 24 (26.3) | 0.26 | −0.20 |
| ACE-inhibitors and ARBs | 81 (57.4) | 215 (64.3) | 0.16 | 0.16 | 52 (57.1) | 54 (59.3) | 0.76 | 0.05 |
| Statins | 102 (72.3) | 280 (83.8) | 0.004 | 0.38 | 68 (74.7) | 67 (73.6) | 0.87 | −0.03 |
| Procedural profiles | ||||||||
| Number of treated lesions | 1.8 ± 1.1 | 1.7 ± 1.0 | 0.17 | −0.14 | 1.7 ± 1.0 | 1.7 ± 1.1 | 0.89 | −0.02 |
| Number of treated vessels | 1.3 ± 0.6 | 1.3 ± 0.5 | 0.35 | −0.10 | 1.3 ± 0.5 | 1.3 ± 0.5 | 0.89 | −0.02 |
| Treated vessels | ||||||||
| Left main | 7 (4.9) | 10 (2.9) | 0.29 | −0.29 | 3 (3.2) | 2 (2.1) | >0.99 | −0.23 |
| LAD | 87 (61.7) | 191 (57.1) | 0.36 | −0.10 | 53 (58.2) | 52 (57.1) | 0.88 | −0.03 |
| LCX | 38 (26.9) | 96 (28.7) | 0.69 | 0.05 | 19 (20.8) | 24 (26.3) | 0.38 | 0.17 |
| RCA | 57 (40.4) | 124 (37.1) | 0.50 | −0.08 | 40 (43.9) | 36 (39.5) | 0.55 | −0.10 |
| Type B2C lesions | 132 (93.6) | 315 (94.3) | 0.77 | 0.07 | 87 (95.6) | 84 (92.3) | 0.54 | −0.33 |
| Multivessel disease | 37 (26.2) | 80 (23.9) | 0.60 | −0.07 | 21 (23.0) | 22 (24.1) | 0.86 | 0.03 |
| Number of inserted stents | 1.77 ± 0.98 | 1.65 ± 0.92 | 0.21 | −0.13 | 1.67 ± 0.91 | 1.65 ± 0.95 | 0.87 | −0.02 |
| Average stent diameter (mm) | 2.91 ± 0.37 | 3.00 ± 0.44 | 0.032 | 0.21 | 2.92 ± 0.39 | 2.96 ± 0.46 | 0.50 | 0.10 |
| Total stent length (mm) | 41.8 ± 26.7 | 39.1 ± 26.7 | 0.32 | −0.10 | 39.8 ± 26.1 | 39.4 ± 25.8 | 0.90 | −0.02 |
| Bare metal stents | 4 (2.8) | 6 (1.7) | 0.49 | −0.26 | 2 (2.1) | 2 (2.1) | >0.99 | <0.001 |
| Drug-eluting stents | 139 (98.5) | 329 (98.5) | 0.95 | −0.03 | 91 (100.0) | 89 (97.8) | 0.50 | 0.10 |
| 1st generation | 29 (20.5) | 64 (19.1) | 0.72 | −0.05 | 19 (20.8) | 16 (17.5) | 0.57 | −0.12 |
| 2nd generation | 110 (78.0) | 265 (79.3) | 0.75 | 0.04 | 72 (79.1) | 73 (80.2) | 0.85 | 0.04 |
| Overall Population | PSM Population | |||||
|---|---|---|---|---|---|---|
| Low L1 SMI (n = 141) | High L1 SMI (n = 334) | Log-Rank p-Value | Low L1 SMI (n = 91) | High L1 SMI (n = 91) | Log-Rank p-Value | |
| All-cause mortality | 31 (23.7) | 19 (5.9) | <0.001 | 22 (25.7) | 9 (10.0) | 0.009 |
| Cardiovascular | 10 (8.4) | 7 (2.2) | 0.004 | 7 (9.1) | 5 (5.6) | 0.47 |
| Non-cardiovascular | 21 (16.6) | 12 (3.8) | <0.001 | 15 (18.3) | 4 (4.7) | 0.006 |
| Non-fatal MI | 11 (9.6) | 6 (1.9) | <0.001 | 8 (10.4) | 2 (2.4) | 0.037 |
| ST-elevation MI | 6 (5.0) | 3 (1.0) | 0.008 | 4 (5.2) | 1 (1.3) | 0.14 |
| Non-ST-elevation MI | 5 (4.7) | 3 (0.9) | 0.022 | 4 (5.4) | 1 (1.1) | 0.14 |
| Repeat revascularization | 23 (25.0) | 23 (7.9) | <0.001 | 16 (26.2) | 8 (10.0) | 0.025 |
| TVR | 18 (19.3) | 18 (6.1) | <0.001 | 13 (21.1) | 7 (8.9) | 0.06 |
| Non-TVR | 8 (8.6) | 7 (2.5) | 0.011 | 6 (9.6) | 1 (1.2) | 0.032 |
| MACE | 49 (39.6) | 37 (11.8) | <0.001 | 38 (46.1) | 16 (18.1) | <0.001 |
| 3-Year All-Cause Mortality | 3-Year MACE | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Model 1 * | ||||
| Low L1 SMI | 4.34 (2.45–7.69) | <0.001 | 3.82 (2.54–5.74) | <0.001 |
| Model 2 † | ||||
| Low L1 SMI | 3.74 (1.89–7.41) | <0.001 | 4.51 (2.76–7.38) | <0.001 |
| Model 3 ‡ | ||||
| Low L1 SMI | 3.69 (1.81–7.52) | <0.001 | 3.77 (2.27–6.27) | <0.001 |
| Model 4 § | ||||
| Low L1 SMI | 4.07 (1.95–8.45) | <0.001 | 3.76 (2.27–6.23) | <0.001 |
| Model 5 || (PSM analysis) | ||||
| Low L1 SMI | 2.68 (1.23–5.83) | 0.013 | 2.80 (1.56–5.03) | 0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, D.O.; Park, S.Y.; Choi, B.G.; Na, J.O.; Choi, C.U.; Kim, E.J.; Rha, S.-W.; Park, C.G.; Hong, S.-J.; Seo, H.S. Prognostic Impact of Low Skeletal Muscle Mass on Major Adverse Cardiovascular Events in Coronary Artery Disease: A Propensity Score-Matched Analysis of a Single Center All-Comer Cohort. J. Clin. Med. 2019, 8, 712. https://doi.org/10.3390/jcm8050712
Kang DO, Park SY, Choi BG, Na JO, Choi CU, Kim EJ, Rha S-W, Park CG, Hong S-J, Seo HS. Prognostic Impact of Low Skeletal Muscle Mass on Major Adverse Cardiovascular Events in Coronary Artery Disease: A Propensity Score-Matched Analysis of a Single Center All-Comer Cohort. Journal of Clinical Medicine. 2019; 8(5):712. https://doi.org/10.3390/jcm8050712
Chicago/Turabian StyleKang, Dong Oh, So Yeon Park, Byoung Geol Choi, Jin Oh Na, Cheol Ung Choi, Eung Ju Kim, Seung-Woon Rha, Chang Gyu Park, Suk-Joo Hong, and Hong Seog Seo. 2019. "Prognostic Impact of Low Skeletal Muscle Mass on Major Adverse Cardiovascular Events in Coronary Artery Disease: A Propensity Score-Matched Analysis of a Single Center All-Comer Cohort" Journal of Clinical Medicine 8, no. 5: 712. https://doi.org/10.3390/jcm8050712
APA StyleKang, D. O., Park, S. Y., Choi, B. G., Na, J. O., Choi, C. U., Kim, E. J., Rha, S.-W., Park, C. G., Hong, S.-J., & Seo, H. S. (2019). Prognostic Impact of Low Skeletal Muscle Mass on Major Adverse Cardiovascular Events in Coronary Artery Disease: A Propensity Score-Matched Analysis of a Single Center All-Comer Cohort. Journal of Clinical Medicine, 8(5), 712. https://doi.org/10.3390/jcm8050712