Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. In Vitro Carbamoylation of Lipids
2.3. In Vitro Oxidation
2.4. Precipitation Procedure
2.5. ATR-FTIR Analysis
2.6. Routine Laboratory Measurements
2.7. Statistics
3. Results
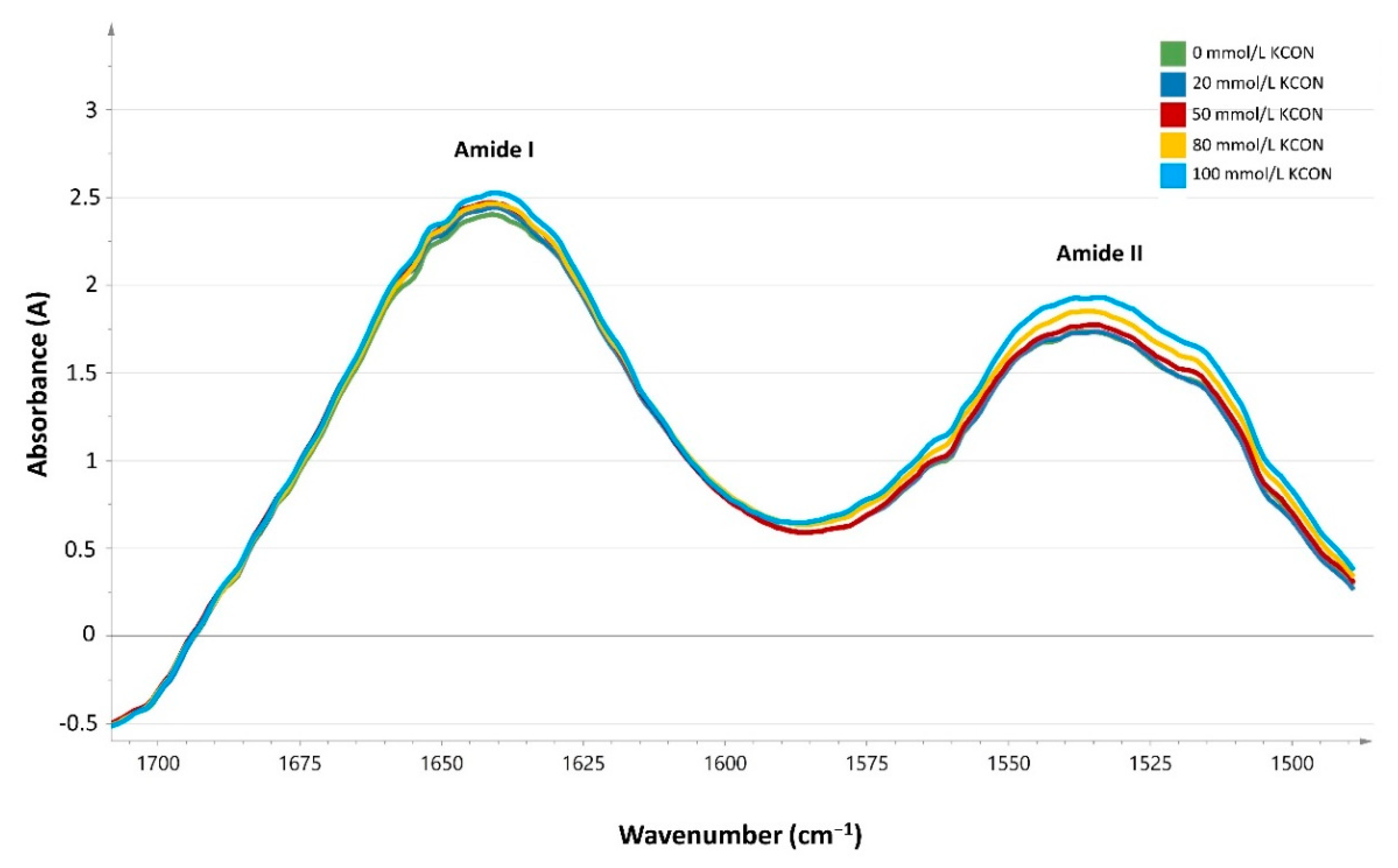
3.1. In Vitro Carbamoylation
3.2. In Vivo Samples
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jaisson, S.; Pietrement, C.; Gillery, P. Carbamylation-derived products: Bioactive compounds and potential biomarkers in chronic renal failure and atherosclerosis. Clin. Chem. 2011, 57, 1499–1505. [Google Scholar] [CrossRef]
- Delanghe, S.; Delanghe, J.R.; Speeckaert, R.; Van Biesen, W.; Speeckaert, M.M. Mechanisms and consequences of carbamoylation. Nat. Rev. Nephrol. 2017, 13, 580–593. [Google Scholar] [CrossRef]
- Wang, Z.; Nicholls, S.J.; Rodriguez, E.R.; Kummu, O.; Hörkkö, S.; Barnard, J.; Reynolds, W.F.; Topol, E.J.; DiDonato, J.A.; Hazen, S.L. Protein carbamylation links inflammation, smoking, uremia and atherogenesis. Nat. Med. 2007, 13, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, L.; Lundquist, P.; Kagedal, B.; Larsson, R. Plasma cyanate concentrations in chronic renal failure. Clin. Chem. 1996, 42, 482–483. [Google Scholar]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Speer, T.; Owala, F.O.; Holy, E.W.; Zewinger, S.; Frenzel, F.L.; Stähli, B.E.; Razavi, M.; Triem, S.; Cvija, H.; Rohrer, L.; et al. Carbamylated low-density lipoprotein induces endothelial dysfunction. Eur. Heart J. 2014, 35, 3021–3032. [Google Scholar] [CrossRef] [Green Version]
- Vaziri, N.D. Causes of dysregulation of lipid metabolism in chronic renal failure. Semin. Dial. 2009, 22, 644–651. [Google Scholar] [CrossRef]
- Holy, E.W.; Akhmedov, A.; Speer, T.; Camici, G.G.; Zewinger, S.; Bonetti, N.; Beer, J.H.; Lüscher, T.F.; Tanner, F.C. Carbamylated low-density lipoproteins induce a prothrombotic state via LOX-1: Impact on arterial thrombus formation in vivo. J. Am. Coll. Cardiol. 2016, 68, 1664–1676. [Google Scholar] [CrossRef]
- Apostolov, E.O.; Shah, S.V.; Ok, E.; Basnakian, A.G. Carbamylated low-density lipoprotein induces monocyte adhesion to endothelial cells through intercellular adhesion molecule-1 and vascular cell adhesion molecule-1. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 826–832. [Google Scholar] [CrossRef]
- Apostolov, E.O.; Ray, D.; Alobuia, W.M.; Mikhailova, M.V.; Wang, X.; Basnakian, A.G.; Shah, S.V. Endonuclease G mediates endothelial cell death induced by carbamylated LDL. Am. J. Physiol. Heart Circ. Physiol. 2011, 300, H1997–H2004. [Google Scholar] [CrossRef] [Green Version]
- Asci, G.; Basci, A.; Shah, S.V.; Basnakian, A.; Toz, H.; Ozkahya, M.; Duman, S.; Ok, E. Carbamylated low-density lipoprotein induces proliferation and increases adhesion molecule expression of human coronary artery smooth muscle cells. Nephrology (Carlton) 2008, 13, 480–486. [Google Scholar] [CrossRef]
- Apostolov, E.O.; Shah, S.V.; Ok, E.; Basnakian, A.G. Quantification of carbamylated LDL in human sera by a new sandwich ELISA. Clin. Chem. 2005, 51, 719–728. [Google Scholar] [CrossRef]
- Apostolov, E.O.; Ray, D.; Savenka, A.V.; Shah, S.V.; Basnakian, A.G. Chronic uremia stimulates LDL carbamylation and atherosclerosis. J. Am. Soc. Nephrol. 2010, 21, 1852–1857. [Google Scholar] [CrossRef]
- Holzer, M.; Gauster, M.; Pfeifer, T.; Wadsack, C.; Fauler, G.; Stiegler, P.; Koefeler, H.; Beubler, E.; Schuligoi, R.; Heinemann, A.; et al. Protein carbamylation renders high-density lipoprotein dysfunctional. Antioxid. Redox Signal. 2011, 14, 2337–2346. [Google Scholar] [CrossRef]
- Krilov, D.; Balarin, M.; Kosovic, M.; Gamulin, O.; Brnjas-Kraljevic, J. FT-IR spectroscopy of lipoproteins—A comparative study, Spectrochim. Acta A Mol. Biomol. Spectrosc. 2009, 74, 701–706. [Google Scholar] [CrossRef]
- Coffey, M.D.; Coe, R.A.; Colles, S.M.; Chisolm, G.M. In vitro cell injury by oxidized low density lipoprotein involves lipid hydroperoxide-induced formation of alkoxyl, lipid, and peroxyl radicals. J. Clin. Investig. 1995, 96, 1866–1873. [Google Scholar] [CrossRef] [PubMed]
- Burstein, M.; Scholnick, H.R.; Morfin, R. Rapid method for the isolation of lipoproteins from human serum by precipitation with polyanions. J. Lipid Res. 1970, 11, 583–595. [Google Scholar]
- Roche Diagnostics, Cobas 8000 Modular Series: Intelligent Lab Power (2013). Available online: http://www.cobas.be (accessed on 30 May 2019).
- Fink, P.; Roemer, M.; Haeckel, R.; Fateh-Moghadam, A.; Delanghe, J.; Gressner, A.M.; Dubs, R.W. Measurement of proteins with the Behring nephelometer. A multicenter evaluation. J. Clin. Chem. Clin. Biochem. 1989, 27, 261–276. [Google Scholar]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [PubMed]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Barth, A. Infrared spectroscopy of proteins. Biochim. Biophys. Acta 2007, 1767, 1073–1101. [Google Scholar] [CrossRef] [Green Version]
- Oberg, K.A.; Ruysschaert, J.M.; Goormaghtigh, E. The optimization of protein secondary structure determination with infrared and circular dichroism spectra. Eur. J. Biochem. 2004, 271, 2937–2948. [Google Scholar] [CrossRef] [Green Version]
- Fernandez-Higuero, J.A.; Salvador, A.M.; Martin, C.; Milicua, J.C.; Arrondo, J.L. Human LDL structural diversity studied by IR spectroscopy. PLoS ONE 2014, 9, e92426. [Google Scholar] [CrossRef]
- Liu, K.Z.; Man, A.; Dembinski, T.C.; Shaw, R.A. Quantification of serum apolipoprotein B by infrared spectroscopy. Anal. Bioanal. Chem. 2007, 387, 1809–1814. [Google Scholar] [CrossRef]
- Berg, A.H.; Drechsler, C.; Wenger, J.; Buccafusca, R.; Hod, T.; Kalim, S.; Ramma, W.; Parikh, S.M.; Steen, H.; Friedman, D.J.; et al. Carbamylation of serum albumin as a risk factor for mortality in patients with kidney failure. Sci. Transl. Med. 2013, 5, 175ra29. [Google Scholar] [CrossRef]
- Gorisse, L.; Pietrement, C.; Vuiblet, V.; Schmelzer, C.E.; Köhler, M.; Duca, L.; Debelle, L.; Fornès, P.; Jaisson, S.; Gillery, P. Protein carbamylation is a hallmark of aging. Proc. Natl. Acad. Sci. USA 2016, 113, 1191–1196. [Google Scholar] [CrossRef]
- Nicolas, C.; Jaisson, S.; Gorisse, L.; Tessier, F.J.; Niquet-Leridon, C.; Jacolot, P.; Pietrement, C.; Gillery, P. Carbamylation is a competitor of glycation for protein modification in vivo. Diabetes Metab. 2018, 44, 160–167. [Google Scholar] [CrossRef]
- Coopman, R.; Van de Vyver, T.; Kishabongo, A.S.; Katchunga, P.; Van Aken, E.H.; Cikomola, J.; Monteyne, T.; Speeckaert, M.M.; Delanghe, J.R. Glycation in human fingernail clippings using ATR-FTIR spectrometry, a new marker for the diagnosis and monitoring of diabetes mellitus. Clin. Biochem. 2017, 50, 62–67. [Google Scholar] [CrossRef]
- Steinbrecher, U.P. Oxidation of human low density lipoprotein results in derivatization of lysine residues of apolipoprotein B by lipid peroxide decomposition products. J. Biol. Chem. 1987, 262, 3603–3608. [Google Scholar]
- De Bruyne, S.; Speeckaert, M.M.; Delanghe, J.R. Applications of mid-infrared spectroscopy in the clinical laboratory setting. Crit. Rev. Clin. Lab. Sci. 2018, 55, 1–20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Healthy Subjects | CKD Stage 3, 4 or 5 | CKD Stage 5d | p | |
|---|---|---|---|---|
| N | 45 | 37 | 47 | |
| Median age (years) | 28 (24–33) | 70 (56–75) | 67 (56–75) | <0.0001 |
| % diabetes mellitus | 0 | 30 | 32 | |
| Urea (mmol/L) | 8.9 (7.8–9.9) | 25.0 (18.7–37.5) | 32.8 (28.5–40.1) | <0.0001 |
| Creatinine (µmol/L) | 72.5 (62.8–80.0) | 160.9 (138.6–243.8) | 627.6 (474.7–774.4) | <0.0001 |
| eGFR (mL/min/1.73 m2) | >90 | 31.0 ± 13.6 | <15 | <0.0001 |
| Albumin (g/L) | 47.3 (45.0–50.0) | 42.2 (40.3–44.5) | 40.0 (36.2–42.9) | <0.0001 |
| Total cholesterol (mmol/L) | 4.8 (4.3–5.5) | 4.7 (3.7–5.5) | 4.3 (3.7–5.8) | NS |
| HDL cholesterol (mmol/L) | 1.6 (1.3–2.0) | 1.3 (1.0–1.6) | 1.1 (0.9–1.5) | <0.0001 |
| LDL cholesterol (mmol/L) | 2.7 (2.3–3.1) | 2.3 (1.8–3.1) | 2.4 (1.7–3.2) | NS |
| Triglycerides (mmol/L) | 1.0 (0.8–1.3) | 1.7 (1.1–2.3) | 1.4 (1.1–2.4) | =0.0002 |
| Apolipoprotein B (g/L) | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | 0.8 (0.7–0.9) | NS |
| Variable | β (Standard Error) | p | |
|---|---|---|---|
| Amide II/amide I AUC ratio, r2 = 0.54, p < 0.001 | Triglycerides (mmol/L) | −0.001819 (0.001367) | 0.1858 |
| Apolipoprotein B (g/L) | −0.0306 (0.006277) | <0.0001 | |
| Creatinine (µmol/L) | −0.00001067 (0.000006989) | 0.1293 | |
| Urea (mmol/L) | −0.0006622 (0.0001436) | <0.0001 | |
| Age (years) | −0.0002128 (0.00008219) | 0.0108 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Delanghe, S.E.; De Bruyne, S.; De Baene, L.; Van Biesen, W.; Speeckaert, M.M.; Delanghe, J.R. Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy. J. Clin. Med. 2019, 8, 774. https://doi.org/10.3390/jcm8060774
Delanghe SE, De Bruyne S, De Baene L, Van Biesen W, Speeckaert MM, Delanghe JR. Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy. Journal of Clinical Medicine. 2019; 8(6):774. https://doi.org/10.3390/jcm8060774
Chicago/Turabian StyleDelanghe, Sigurd E., Sander De Bruyne, Linde De Baene, Wim Van Biesen, Marijn M. Speeckaert, and Joris R. Delanghe. 2019. "Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy" Journal of Clinical Medicine 8, no. 6: 774. https://doi.org/10.3390/jcm8060774
APA StyleDelanghe, S. E., De Bruyne, S., De Baene, L., Van Biesen, W., Speeckaert, M. M., & Delanghe, J. R. (2019). Estimating the Level of Carbamoylated Plasma Non-High-Density Lipoproteins Using Infrared Spectroscopy. Journal of Clinical Medicine, 8(6), 774. https://doi.org/10.3390/jcm8060774